
Abstract
This study tested a 10-year longitudinal model examining the role of adolescent attachment, adult romantic attachment, and emotion regulation strategies on adult symptoms of psychopathology. Fifty individuals completed a measure of attachment security to parents and peers at age 14, measures of romantic attachment and emotion regulation at age 22, and a measure of psychopathology at age 24. Results revealed that attachment insecurity to parents in adolescence was associated with greater symptoms of psychopathology in adulthood, and emotion-focused strategies partially mediated this association. Anxious romantic attachment was also related to psychopathology, an association that was fully mediated by emotion-focused strategies. The long-term mechanism involved in the association between earlier attachment and future adaptation will be discussed.
In the last decade, research supporting associations between adolescent and adult attachment models, general psychosocial adaptation, and disposition to distress in nonclinical samples has flourished (Fortuna & Roisman, 2008; Mallinckrodt & Wei, 2005). Specifically, attachment insecurity in both adolescence and adulthood has been concurrently linked to symptoms of psychopathology. However, few studies have examined longitudinal models linking these variables (Lee & Hankin, 2009), thus limiting our understanding of the developmental precursors to adult adaptation. This study thus tested the long-term influence of attachment insecurity toward parents and peers in adolescence and toward romantic partners in young adulthood on the development of adult psychopathology. Furthermore, although theoretical models indicate that associations between earlier attachment models and later adaptation lie in the specific emotion regulation strategies adopted by individuals to deal with distress (Carlson & Sroufe, 1995; Chaplin & Cole, 2005; DeKlyen & Greenberg, 2008), this assumption has yet to be empirically tested. Accordingly, the main objective of this study was to investigate associations between attachment insecurity in adolescence and young adulthood and global symptoms of psychopathology in later adulthood. We further tested the role of emotion regulation strategies as mediators of these longitudinal associations.
Attachment Theory: Childhood, Adolescence, and Young Adulthood
According to attachment theory, internal working models developed in response to the quality of repeated attachment-related parent–child interactions influence the child’s expectations and beliefs about the self, others, and the environment (Bolwby, 1988; Bretherton, 1987; Main, Kaplan, & Cassidy, 1985). The classic work of Ainsworth (Ainsworth, Blehar, Waters, & Wall, 1978) identified three attachment categories: secure, insecure-avoidant, and insecure-ambivalent, based on child separation–reunion behavior with the primary caregiver. Children who have experienced interactions with a sensitive caregiver who consistently responds to their attachment needs are more likely to develop a secure attachment model consisting of self-representations of competency and perceptions of others as dependable and available in times of need (Bretherton, 1987).
Children with an insecure-avoidant attachment relationship with their primary caregiver have learned that expressing distress or the need for proximity in stressful situations is likely to evoke rejection from their caregiver. To protect themselves from this possible rejection, avoidant children inhibit attachment-related behaviors, such as the expression of negative emotions and proximity seeking (Main & Cassidy, 1988). Based on their experiences, avoidant children may view others as untrustworthy and develop positive but unrealistic self-perceptions, with an excessive focus on their ability to overcome difficult situations on their own. Insecure-ambivalent children, however, have experienced inconsistent or unpredictable caregiving, leading them to worry about the availability of their attachment figure to respond to their manifestations of distress. In response to their caregiving experiences, ambivalent children learn to exaggerate and intensify distress signals to maintain parental proximity (Main & Cassidy, 1988). Accordingly, these children may develop self-perceptions as being helpless and unlovable, and view others as being unreliable.
Main and Solomon (1990) later identified a fourth attachment pattern, which they called insecure-disorganized. Disorganized child attachment is believed to develop in the presence of frightening or frightened parental behavior (Madigan, Moran, Schuengel, Otten, & Pederson, 2007). According to Main and Hesse (1990), disorganized children are caught at the heart of an important dilemma in which their source of comfort also represents their source of fear. Consequently, these children show confused and contradictory withdrawal and approach behaviors toward their attachment figure when distressed. Children with disorganized attachment describe themselves the most negatively of all the attachment groups, show the highest level of affect dysregulation, and lack organized and coherent attachment strategies for seeking parental proximity in times of distress (Main & Solomon, 1990).
Similar systems exist for classifying adolescent attachment models, using both categorical and continuous dimensions of security (see Main & Goldwyn, 1985, for details on the Adult Attachment Interview), while others rely solely on continuous scales of security (e.g., Armsden & Greenberg, 1987). Accordingly, a more secure adolescent is likely to be involved in a goal-corrected parent–teen relationship, which allows for increased independence from parents to attain normative age-appropriate social goals (e.g., development of social relationships with peers, greater exploration of a larger environment, etc.) while still maintaining contact with parents through open communication (Allen, 2008; Armsden & Greenberg, 1987; Kobak & Duemmler, 1994). However, greater adolescent attachment insecurity toward parents, in general, is marked by feelings of resentment and alienation, as well as emotional detachment (Armsden & Greenberg, 1987).
Although parents remain the adolescent’s primary attachment figure, close peers increasingly fulfill certain attachment needs during this crucial developmental period (Allen, 2008; Armsden & Greenberg, 1987; Zeifman & Hazan, 2008). In line with this idea, Zeifman and Hazan (2008), who investigated participants’ (aged 6 to 17) preferred attachment figure relating to the four components of attachment (i.e., proximity seeking, safe haven, separation distress, and secure base), reported that nearly all sample participants preferred spending time with peers over parents. Moreover, between the ages of 8 and 14, participants increasingly preferred receiving comfort and emotional support from peers, although parents remained the primary sources of separation distress and bases of security. By late adolescence, the authors noted that romantic partners were identified as the overall preferred attachment figures. During late adolescence and early adulthood, there is thus a subsequent restructuring of the attachment hierarchy with romantic partners becoming the most sought-out attachment figures (Hazan & Shaver, 1987; Zeifman & Hazan, 2008).
Adult romantic attachment can be measured along two orthogonal dimensions, which assess feelings and thoughts toward romantic partners in general, that is, avoidance of intimacy and anxiety over abandonment (Brennan, Clark, & Shaver, 1998). Avoidantly attached individuals generally distrust their romantic partners and are uncomfortable with intimacy, whereas anxiously attached individuals are preoccupied by thoughts of abandonment by their partners. Taken together, parents, peers, and romantic partners represent important attachment figures at specific phases of development.
Attachment and Psychopathology
In addition to influencing one’s perceptions of self and others, internal working models of early attachment relationships influence the individuals’ resilience and vulnerability to stressful life events, consequently affecting their well-being and mental health (Bolwby, 1988). Insecure adult attachment models have been found to be associated with more inflexible perceptions of self (Lopez, 1996), as well as more negative and distorted views and expectations of others (Mikulincer & Shaver, 2008). Based on these distorted cognitive models, individuals may perceive and experience difficult and stressful events in a more negative manner (e.g., anger, hurt, disappointment, sadness, jealousy, helplessness), potentially exacerbating their experience of distress (Collins, 1996). In line with this idea, attachment security during childhood, adolescence, and young adulthood has been shown to be a protective factor against psychopathology and related symptoms such as anxiety, depression, dissociation, and antisocial behaviors (Davila, Ramsay, Stroud, & Steinberg, 2005; Dozier, Stovall-McClough, & Albus, 2008). In contrast, internalized representations of self and others developed in response to insensitive caregiving are thought to increase the risk of developmental maladaptation across the life span (DeKlyen & Greenberg, 2008; Moss, Bureau, St-Laurent, & Tarabulsy, 2011). Therefore, although attachment insecurity is not considered a disorder in and of itself, it is viewed as an important risk factor for adult psychopathology, including symptoms of anxiety, depression, dissociation, and antisocial behaviors (Bolwby, 1988; Davila et al., 2005; Dozier et al., 2008).
Adolescence is a particularly interesting developmental phase to study with respect to attachment insecurity and psychopathology given that, as previously stated, different attachment figures (i.e., parents and peers) play an active role in the teen’s life (Armsden & Greenberg, 1987; Zeifman & Hazan, 2008). Concurrent and prospective studies with adolescent samples have already linked attachment insecurity to higher instances of depression and behavior problems (Laible, Carlo, & Raffaelli, 2000; Lee & Hankin, 2009). For example, Lee and Hankin (2009) found that both anxious and avoidant attachment orientations to parents and close peers in adolescence predicted prospective increases in depressive and anxiety symptoms over a 5-month period. However, this study was limited in that it did not assess the independent contribution of attachment security to parents and peers, but rather used a global attachment score. In two other studies that included independent parent and peer scores, both attachment relationships were found to be concurrently associated with psychopathology: General insecurity was associated with greater depression and anxiety (Muris, Meesters, van Melick, & Zwambag, 2001), whereas security was related to greater overall adjustment (i.e., greater sympathy and lower aggression and depression; Laible et al., 2000) in adolescence. In these two studies, the contribution of attachment to parents and to peers in relation to psychopathology was similar. However, in a study by Wilkinson and Walford (2001), the authors found that only adolescent attachment security to parents, not to peers, was related to lower distress. Taken together, study findings are somewhat inconsistent with respect to the distinct influence of attachment insecurity to parents and peers on the development of symptoms of psychopathology. Moreover, given the cross-sectional nature of these studies, our understanding of the longitudinal influence of these specific relationships on later adult psychopathology is limited.
Associations between greater attachment insecurity in adulthood and general psychopathology have also been investigated, although findings differ across studies. Some studies report that both the anxious and avoidant attachment orientations are positively correlated with internalizing, externalizing, and overall symptom severity (Fortuna & Roisman, 2008; Mallinckrodt & Wei, 2005). Others find stronger associations with symptoms of psychopathology for the anxious dimension than for the avoidant, particularly when internalizing symptoms (i.e., anxiety, depression) are measured as outcomes (Brenning, Soenens, Braet, & Bosmans, 2011; Lopez, Mauricio, Gormley, Simko, & Berger, 2001; Mikulincer & Shaver, 2007).
In summary, at both adolescence and adulthood, attachment insecurity has been linked to various symptoms of psychopathology. However, no study to date has examined associations across these two developmental periods. Moreover, there are inconsistencies in the adolescent literature concerning the relative influence of attachment to parents versus peers and, in the adult literature, of anxious versus avoidant orientations on outcome measures. In addition, most studies have focused on the association between attachment and symptoms of depression and anxiety (Lee & Hankin, 2009; Lopez et al., 2001; Muris et al., 2001), despite the fact that the assessment of global symptoms of psychopathology, versus specific disorders, may be particularly appropriate when studying nonclinical populations.
Attachment, Emotion Regulation Strategies, and Psychopathology
Attachment theory provides a strong framework for understanding associations between the quality of primary caregiver–child relationships and mental and psychological well-being over time. Within this framework, it would seem that emotion regulation strategies represent important contributors to this association. Specifically, based on attachment theory, the parent–child relationship influences the development of emotion regulation strategies thought to be important for later adult adaptation (Bowlby, 1982; DeKlyen & Greenberg, 2008). According to Thompson (1994), “Emotion regulation consists of the extrinsic and intrinsic processes responsible for monitoring, evaluating, and modifying emotional reactions, especially their intensive and temporal features, to accomplish one’s goals” (p. 28-29). Based on attachment theory, individuals adopt specific emotion regulation strategies to accomplish their goal of dealing with distress that is in accordance with their internal working model of attachment (Mikulincer & Shaver, 2007, 2008). When faced with distress or stressful situations, individuals will rely on these strategies to regulate their emotions, thoughts, and behaviors. For example, individuals with an avoidant attachment are more likely to use deactivating strategies to deal with stress-related situations, which include denial of emotion-related thoughts and information, as well as suppression of emotional expressivity (Kobak, Cole, Ferenz-Gillies, Fleming, & Gamble, 1993; Mikulincer & Shaver, 2007, 2008). Avoidant individuals adopt these strategies to maintain their attachment system deactivated because activation of this system would cause them to relive past or present experiences of distress in response to a distant and rejecting attachment figure (Mikulincer & Shaver, 2007). Fear, anxiety, anger, sadness, shame, guilt, and distress are especially inhibited as they relate to feelings of vulnerability, contradicting the avoidant individual’s self-perceptions of competency, superiority, and strength (Hesse, 1999). Although denial of emotional states and inhibition of emotional expressivity are adaptive for avoidant individuals in the short term, over time, they can potentially contribute to psychopathology, including anxiety disorders (Zeijlmans van Emmichoven, van IJzendoorn, de Ruiter, & Brosschot, 2003), eating disorders (Ward et al., 2001), and antisocial behaviors (Rosenstein & Horowitz, 1996), given that negative emotions are not openly communicated and accurately evaluated but are rather suppressed (Mikulincer & Shaver, 2007).
However, anxiously attached individuals are more inclined to use hyperactivating strategies, which include exaggeration of threats, over-dependence on the attachment figure, and hypervigilance to cues of danger and abandonment, when faced with stress-related situations (Mikulincer & Florian, 1995; Mikulincer & Shaver, 2007, 2008). Focusing on potentially negative cues and emotions causes these individuals to link negative experiences together so that one negative thought leads to a string of others (Mikulincer & Shaver, 2008). The anxiously attached individual is therefore caught in a vicious cycle whereby his or her attention to negative information leads to negative thoughts and ruminations, which in turn intensifies their feelings of anxiety, and thus their focus on potentially negative cues. Although the use of hyperactivating and emotion-focused strategies (e.g., self-blame, self-criticism, ruminations, focus on negative emotions, and feelings of helplessness) by anxiously attached individuals is somewhat effective for maintaining the attention of attachment figures, these strategies may serve to intensify negative feelings, such as anger, helplessness, and stress, which have been found to contribute to the development of symptoms of psychopathology, including depression and anxiety disorders (Cantazaro & Wei, 2010; Hankin & Abramson, 2001; Lopez et al., 2001).
Given that insecure attachment models have been shown to be related to symptoms of psychopathology, and that these models promote the use of specific emotion regulation strategies associated with qualitative differences in attachment relationships (e.g., avoidantly attached individuals avoid expressing their emotions at all cost, while anxiously attached individuals are intensively focused on their negative emotions), these strategies may be important mediating variables explaining the association between earlier attachment insecurity and adult functioning (Carlson & Sroufe, 1995; Chaplin & Cole, 2005; DeKlyen & Greenberg, 2008). In line with this idea, problematic strategies such as emotional reactivity and difficulties in identifying and communicating feelings (Lopez et al., 2001; Mallinckrodt & Wei, 2005; Wei, Heppner, & Mallinckrodt, 2003) have already been identified as mediators of the association between insecure attachment and psychopathology, particularly depression and anxiety. However, these studies are limited in that samples were restricted to specific populations (undergraduates) and relied on concurrent data only. For example, using a sample of undergraduates, Wei et al. (2003) found that the perceived ability to overcome difficulties fully mediated the association between attachment anxiety and psychological distress (including anxiety and depression symptoms), whereas it only partially mediated the relationship between avoidant attachment and distress. Similarly, Lopez et al. (2001) reported that ineffective strategies (i.e., strong emotional responses, impulsivity, and distortions) partially mediated the positive association between anxious attachment and distress (combined depression and anxiety), whereas avoidant attachment was not a predictor of distress. Overall, reviewed studies, although cross-sectional, indicate that the association between attachment insecurity and psychopathology is indirect and may be mediated by different emotion regulation strategies. Not only will we attempt to replicate these concurrent mediation models using longitudinal data, but we will also test these models using diverse measures of attachment throughout development (toward parents and peers in adolescence and toward romantic partners in young adulthood).
The Current Study
Despite the evidence for concurrent associations between insecure attachment and psychopathology at adolescence and young adulthood (Fortuna & Roisman, 2008; Lee & Hankin, 2009; Lopez et al., 2001; Mallinckrodt & Wei, 2005; Muris et al., 2001), to our knowledge, no study has tested a developmental model across these periods. In this study, attachment was evaluated at two different time points (Time 1: 14 years of age, and Time 2: 22 years of age) and in relation to three distinct attachment figures (Time 1: parents and peers; Time 2: romantic partners). Given that the sample was nonclinical, a global index of symptoms of psychopathology was used as the outcome variable. The use of a normative rather than clinical sample is better suited for assessing the potential long-term associations between earlier attachment and later psychopathology as the presence of other potential influential variables, such as low family socio-economic status, parental psychopathology, and/or substance abuse in high-risk samples, can make it difficult to tease apart the unique influence of early insecurity on later functioning.
The first objective of this study was to test a longitudinal model evaluating the relative contribution of attachment insecurity toward parents and peers during adolescence (Time 1), anxious and avoidant romantic attachment orientations in young adulthood (Time 2), and emotion regulation strategies in young adulthood (Time 2) to self-reported symptoms of psychopathology in adulthood (Time 3). Based on past empirical evidence (Lee & Hankin, 2009; Muris et al., 2001), we expected greater insecurity at both Time 1 and Time 2 to be associated with greater symptoms of psychopathology. In line with the findings of Wilkinson and Walford (2001), we also expected adolescent attachment to parents to be more strongly related to adult psychopathology than adolescent attachment to peers. This hypothesis is also supported by the theoretical assumption that internal working models are based more prominently on caregiving experiences with parents rather than peers (Bolwby, 1988).
Given that emotion regulation strategies have also been linked to psychopathology (Lopez et al., 2001; Mallinckrodt & Wei, 2005), we expected attachment-related emotion regulation strategies, specifically emotion-focused strategies and emotional expressivity, to be related to adult symptoms of psychopathology. More precisely, we predicted that greater use of emotion-focused strategies (i.e., self-blame, ruminations, focus on negative emotions) and lower emotional expressivity (i.e., tendency to outwardly display and communicate emotions) would be related to greater symptoms of psychopathology.
The second study objective was to test mediation models in which attachment orientations (in adolescence and adulthood) would be related to later adult psychopathology via the use of emotion regulation strategies. Specifically, we expected that greater insecurity to parents and peers would be associated with greater symptoms of psychopathology in adulthood via the use of greater emotion-focused strategies and lower emotional expressivity. Based on the hyperactivating and deactivating strategies of the anxious and avoidant attachment models, respectively, we also expected romantic attachment in adulthood to be related to greater symptoms of psychopathology via the use of emotion-focused strategies for the anxiously attached and via the use of lower emotional expressivity for the avoidantly attached.
Method
Participants
Participants were 50 young adults (33 women and 17 men;M age = 23.5, SD = .88) taking part in an ongoing longitudinal study of developmental adaptation as a function of the parent–child relationship (see Moss, Smolla, Cyr, Dubois-Comtois, Mazzarello, & Berthiaume, 2006). Participants were part of a larger community sample that had been initially recruited through various daycares in diverse socio-economic areas of Montreal, Canada. The original longitudinal study began when children were 4 years of age. The present study included data collected from adolescence, that is, when participants were 14, 22, and 24 years of age, respectively, referred to in this article as Time 1 (T1), Time 2 (T2), and Time 3 (T3).
At Time 1 (M age = 13.7 years, SD = .64, n = 79, 45 girls), 10% of families reported earning less than $20,000 (figures represent Canadian dollars), 37% between $20,000 and $50,000, and 53% reported earning $50,000 and above. Seventy percent of the participants’ mothers obtained college- or university-level training, and 32% of the sample adolescents were living in a mother-headed single-parent family. At Time 2 (M age = 21.5 years, SD = 0.81, n = 66, 43 young women), 50% of young adults reported earning less than $10,000, 45% between $10,000 and $30,000, and 5% reported earning $30,000 and above. Thirty-two percent of the participants had completed a high school degree, and the rest had some college- or university-level training. Seventy-three percent of the sample participants were still living with their families, whereas the rest where living on their own. At Time 3 (M age = 23.5 years, SD = .88, N = 50, 33 young women), 22% of young adults reported earning less than $10,000, 48% between $10,000 and $30,000, and 30% reported earning $30,000 and above. Twenty-five percent of the participants had completed a high school degree, and the rest had some college- or university-level training. Forty-two percent of the sample participants were still living with their families of origin, whereas the rest were living on their own.
At T1, the sample included 79 participants. From T1 to T2, 13 (16.5%) were lost to attrition: 5 never responded to repeated contacts initiated by the project staff, 2 no longer had valid phone numbers, 1 moved away, 4 refused to participate, and 1 accepted participation but did not show up to the laboratory visit. Out of the 66 participants who completed T2 measures, 10 participants had to be dropped from analyses due to incomplete attachment and emotion regulation data sets (no differences on socio-demographic variables were found between these 10 participants and the remaining 56). From T2 to T3, six participants were lost to attrition (never responded to repeated contacts initiated by the project staff). ANOVAs and chi-square analyses of socio-demographic variables (age, gender, and family income) and main variables (adolescent attachment to parents and peers at T1 and adult attachment and emotion regulation strategies at Time 2) comparing the final study sample of 50 participants with the 29 who were lost to attrition or dropped from Time 1 to Time 3 revealed no significant differences. Moreover, additional analysis (ANOVAs and chi-square) revealed no significant differences in age, gender, and family income at initial assessment (when children were 4 years of age; n = 186) between the 50 participants who remained in the longitudinal project and the 136 who were lost over 20 years.
Procedure
Time 1
An initial phone call informing participants of the adolescent phase of the longitudinal study was followed by a laboratory visit for each adolescent during which the Inventory of Parent and Peer Attachment (IPPA; Armsden & Greenberg, 1987) questionnaire was completed. Mothers of participants completed a socio-demographic questionnaire sent to them by mail.
Time 2
Participants were contacted by phone and invited to the first of two laboratory visits (approximately 1 month apart), during which a socio-demographic questionnaire and the Experiences in Close Relationships (ECR; Brennan et al., 1998) measure were completed. During the second laboratory visit, participants completed the two emotion regulation measures: the Coping Inventory for Stressful Situations (CISS; Endler & Parker, 1994) and the Emotional Expressivity Scale (EES; Kring, Smith, & Neale, 1994). The emotion-focused subscale of the CISS was chosen given its positive anticipated overlap with the hyperactivating strategy of anxiously attached individuals, while the EES was chosen for its negative anticipated association with the deactivating strategy of the avoidantly attached. Participants also completed a modified version of the Life Event Questionnaire (Norbeck, 1984) to account for the presence of stressful life events throughout development.
Time 3
Participants were contacted by phone and asked to complete questionnaires that would be sent to them by mail. These included a socio-demographic questionnaire, the Symptom Checklist 90–Revised (SCL-90-R; Derogatis, 1983), and a modified versions of the Life Event Questionnaire (Norbeck, 1984) to account for the presence of stressful life events since the last laboratory assessment.
Measures
Inventory of Parent and Peer Attachment (IPPA)
The IPPA (Armsden & Greenberg, 1987) is a 24-item self-reported questionnaire evaluating adolescents’ positive and negative perceptions of affective and cognitive dimensions of their relationships with their parents and peers (e.g., my parents/my friends accept me as I am; if my parents/friends know something is bothering me, they ask me about it). Participants rated each item on a 4-point scale ranging from 1 (“almost always true”) to 4 (“almost never true”). Ratings were then summed, generating two global indices of attachment insecurity: 1 for parents (12 items; alpha current study = .83) and the other for peers (12 items: alpha current study = .84). A high global score reflected a high level of attachment insecurity. The IPPA has excellent psychometric qualities (average internal consistency and test–retest reliability scores: .90) and is widely used within adolescent attachment research (see Allen, Porter, McFarland, McElhaney, & Marsh, 2007; Smith, Calam, & Bolton 2009; Tambelli, Laghi, Odorisio, & Notari, 2012).
Experiences in Close Relationships (ECR)
The self-reported ECR (Brennan et al., 1998) consists of 36 items, which measure romantic attachment along two dimensions: avoidance of intimacy (18 items: alpha current study = .90; for example, I prefer not to show a partner how I feel deep down) and anxiety over abandonment (18 items: alpha current study = .90; for example, I worry about being abandoned). Participants responded to each item using a 7-point scale from 1 (“strongly disagree”) to 7 (“strongly agree”), rating the extent to which each item is descriptive of how they usually feel and behave in romantic relationships. Ratings were then averaged to compute scores for each dimension. High scores reflected more anxious and avoidant attachment orientations. The ECR is well-validated and widely used within the adult attachment literature (for a review, see Mikulincer & Shaver, 2007; Chapter 10).
Coping Inventory for Stressful Situations (CISS)
The CISS (Endler & Parker, 1994) is a 48-item self-administered questionnaire, which assesses four strategies of coping styles: task-focused, emotion-focused, distraction, and social diversion. For the present study, only data obtained for the emotion-focused scale (16 items: alpha current study = .87) were included in the present study, as the others did not pertain to our research questions. Specifically, emotion-focused regulation refers to strategies that monitor emotional distress in response to a stressful situation (e.g., I blame myself for not knowing what to do; I focus on the insufficient resources at my disposal to deal with the problem; I get angry with myself; I get angry with others). Respondents rated each item on a 5-point scale ranging from 1 (“not at all”) to 5 (“very much”). Ratings were then summed to compute a total score. A high score reflected greater use of the strategy. The CISS has good internal consistency with alpha coefficients ranging from .76 to .91 (Endler & Parker, 1994). Furthermore, this measure is widely used as a measure of emotion regulation (see Benoit, Bouthillier, Moss, Rousseau, & Brunet, 2010; Mc Elroy & Hevey, 2014).
Emotional Expressivity Scale (EES)
The EES (Kring et al., 1994) is a 17-item self-report questionnaire measuring the extent to which people outwardly display their emotions (alpha current study = .93). Respondents rated each item (e.g., I display my emotions to other people; other people believe me to be very emotional) on a 6-point scale ranging from 1 (“strongly disagree”) to 6 (“strongly agree”). Ratings were then summed to compute a total score. A high score reflected greater emotional expressivity. Reliability studies (Kring et al., 1994) show the EES to be internally consistent with an alpha coefficient of .91. Kring et al. reported a 4-week test–retest correlation of .90. As a result, the EES has been used in numerous studies for assessing emotion regulation (see Benoit et al., 2010; Niles, Haltom, Mulvenna, Lieberman, & Stanton, 2014; Vogel, Wade, & Hackler, 2008).
The Symptom Checklist 90–Revised (SCL-90-R)
The SCL-90-R (Derogatis, 1983) is a psychiatric self-report inventory. The 90 items included in the questionnaire were scored on a 5-point scale from 0 (“not at all”) to 4 (“extremely”), indicating the rate of occurrence of the 90 symptoms in the last 7 days. Symptoms can be classified into nine dimensions including somatization, obsessive–compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. The questionnaire also generates a global severity score, representing the average rating for the 90 items (alpha current study = .96). This global score was used in the analyses as an index of general experience of symptoms of psychopathology (correlation coefficients among SCL-90-R scales in the current study ranging from .39 to .77). A high global score reflected more symptoms of psychopathology. This scale is particularly useful for nonclinical patients who may be less symptomatic of specific disorders. Accordingly, the measure had been validated with adult nonclinical patients (Derogatis, 1983), which represents the sample of the current article.
Stressful life events
A modified version of the Life Event Questionnaire (Norbeck, 1984) was created for the purpose of the current study (72 items at T2; 40 items at T3). Participants indicated whether or not they experienced the specified event, in what year, whether it was a positive or negative experience, and the amount of impact the event had on his or her life ranging from 0 (“no effect”) to 3 (“great effect”). The following events were retained for the purpose of the present study as these events can be expected to influence one’s experience of psychopathology: (a) sickness of a close friend, family member, and/or of the self, (b) death of a close friend or family member, (c) parental divorce or separation, (d) the experience of a break-up.
Socio-demographic questionnaire
This 10-item questionnaire was created by the research team to assess participants’ demographic information pertaining to the self and the family (e.g., age, gender, income, education).
Results
Preliminary Analyses
Preliminary correlation analyses performed to identify possible covariates such as age, years of education, and income level in relation to the global psychopathology index revealed no significant associations (rs between −.20 and −.17). Given past findings showing consistent associations between gender and the prevalence of symptoms of psychopathology (Barlow, 2002), a t-test was conducted to assess differences between men and women on the global psychopathology index. Results revealed no significant association between gender and psychopathology, t(48) = 1.24 n.s. Furthermore, to assess the possible influence of stressful life events on adult symptoms of psychopathology, a risk index was created based on the presence (1) or absence (0) of stressful life events as reported at T2 and T3 (events reported at T2 and T3 were summed). Correlation analyses revealed no significant associations (r = .25, p = .08) between risk and psychopathology. Therefore, socio-economic variables, gender, and risk were not controlled for in subsequent analyses.
Correlation analyses were then conducted between the independent (adolescent and young adult attachment, and emotion regulation strategies) and dependent (global index of psychopathology) variables. Table 1 presents correlation coefficients as well as means, standard deviations, and range for study variables. Results show insecure adolescent attachment toward parents, anxious romantic attachment, and emotion-focused regulation strategies to be positively related to adult symptoms of psychopathology. Adolescent attachment to peers, avoidant attachment, and emotional expressivity were not.
Descriptive Statistics and Correlations Between Study Variables (N = 50).
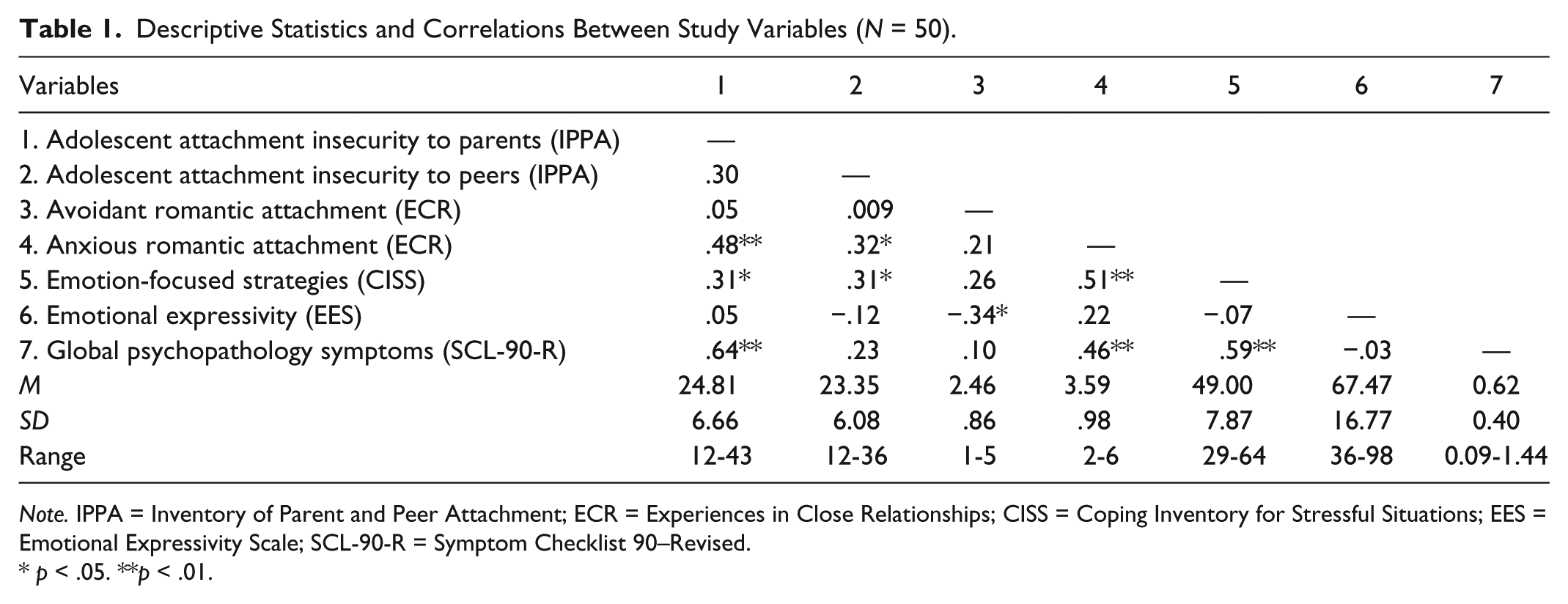
Note. IPPA = Inventory of Parent and Peer Attachment; ECR = Experiences in Close Relationships; CISS = Coping Inventory for Stressful Situations; EES = Emotional Expressivity Scale; SCL-90-R = Symptom Checklist 90–Revised.
p < .05. **p < .01.
Attachment and emotion regulation strategies as predictors of adult psychopathology
In line with our first hypothesis, we tested a complete longitudinal model to assess the long-term associations between adolescent and young adult attachment, emotion regulation strategies, and adult symptoms of psychopathology. A multiple regression analysis was therefore performed with adolescent attachment to parents and peers, anxious and avoidant romantic attachment orientations, emotion-focused regulation strategies, and emotional expressivity as predictors of global index of psychopathology. Results (see Table 2) revealed that adolescent attachment to parents and emotion-focused regulation strategies in young adulthood made a significant unique contribution to the prediction of adult psychopathology (explaining 19% and 14% of the variance, respectively), whereas adolescent attachment to peers, anxious and avoidant romantic attachment, and emotional expressivity did not.
Multiple Regression Model With Adolescent Attachment Insecurity to Parents and Peers, Anxious and Avoidant Romantic Attachment, Emotion-focused Regulation Strategies, and Emotional Expressivity as Predictors of Adult Symptoms of Psychopathology.
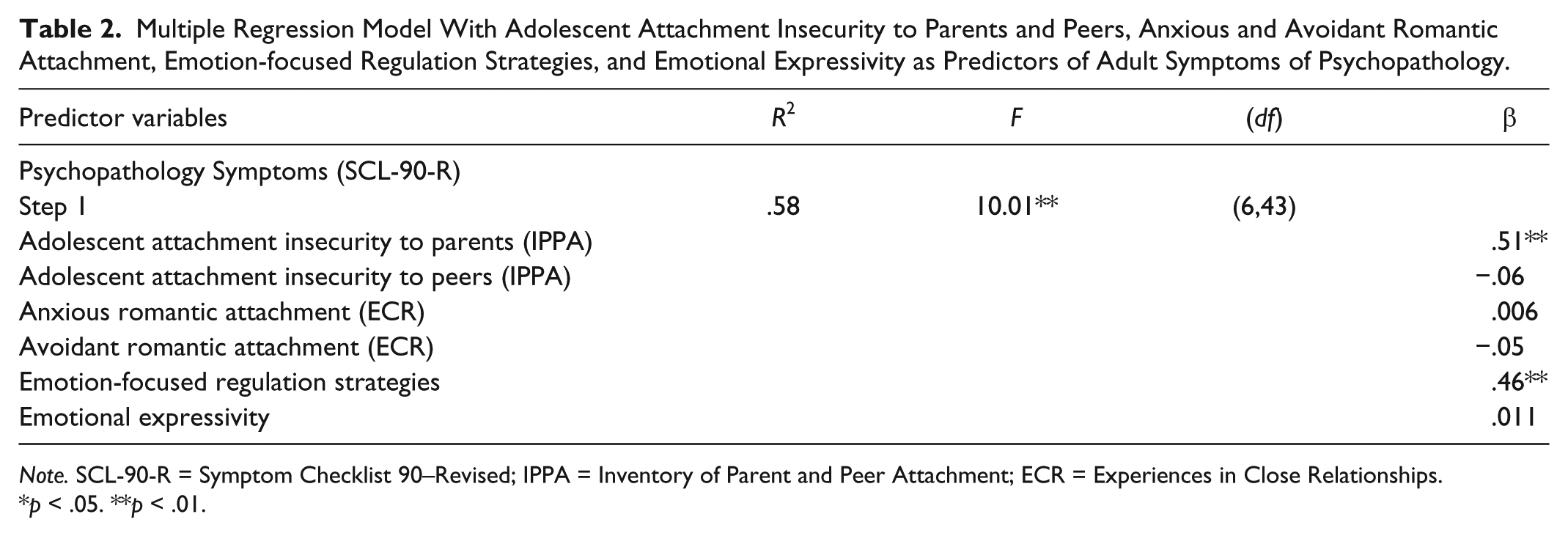
Note. SCL-90-R = Symptom Checklist 90–Revised; IPPA = Inventory of Parent and Peer Attachment; ECR = Experiences in Close Relationships.
p < .05. **p < .01.
Association between adolescent attachment to parents, emotion-focused strategies, and adult psychopathology
In line with our second objective and given the previously described significant findings, we next tested the role of emotion-focused regulation strategies as a mediator of the association between insecure adolescent attachment to parents and adult psychopathology. According to Baron and Kenny’s (1986) recommendations, all three conditions for testing such a model were met (see Figure 1): (a) The independent variable (adolescent attachment to parents) was related to the dependent variable (psychopathology), Path c: ΔR2 = .41, F(1, 48) = 32.69, p < .01, β = .64; (b) the independent variable was related to the mediator (emotion-focused strategies), Path a: ΔR2 = .10, F(1, 48) = 5.04, p < .01, β = .31; and (c) the mediator was related to the dependent variable, controlling for the independent variable, Path b: ΔR2 = .17, F(1, 47) = 19.24, p < .01, β = .44.

Mediation test between insecure adolescent attachment to parents and adult psychopathology via the use of emotion-focused strategies.
A final hierarchical regression with adult psychopathology symptoms as the dependent variable was then conducted with emotion-focused strategies entered in Step 1 and adolescent attachment insecurity to parents in Step 2. Results (see Table 3 and Figure 1) showed that, when taking into account the variance explained by emotion-focused strategies, adolescent attachment insecurity to parents remained a significant predictor of adult psychopathology, Path c’: ΔR2 = .23, F(1, 47) = 25.37, p < .01, d = .30. We further tested the significance of the mediated path using Preacher and Hayes’s (2004) bootstrapping methodology for indirect effects. This procedure is based on 1,000 bootstrap resamples to describe the confidence intervals (CIs) for indirect effects in a manner that makes no assumptions about the distribution of the indirect effects. Interpretation of the bootstrap data is accomplished by determining whether zero is contained within the 95% CI (thus revealing a lack of significance). Results revealed an indirect effect of .0080 and a bias-corrected bootstrap 95% CI [.0011, .0166], indicating a significant decrease in the effect of adolescent attachment to parents on adult psychopathology, through the use of emotion-focused strategies. The use of emotion-focused strategies is therefore considered to be a partial mediator of the association between adolescent attachment to parents and adult symptoms of psychopathology.
Hierarchical Regression Model With Adolescent Attachment Insecurity to Parents and Emotion-Focused Strategies in Young Adulthood as Predictors of Adult Symptoms of Psychopathology.

Note. SCL-90-R = Symptom Checklist 90–Revised; CISS = Coping Inventory for Stressful Situations; IPPA = Inventory of Parent and Peer Attachment.
p < .05. **p < .01.
Association between young adult anxious attachment, emotion-focused strategies, and adult psychopathology
Although anxious romantic attachment was not identified as a significant predictor in the tested longitudinal model described above, correlational analyses did reveal anxious romantic attachment to be positively linked to emotion-focused strategies and to symptoms of psychopathology. In line with our original hypothesis, we thus tested a model in which emotion-focused regulation strategies mediated the association between anxious attachment orientation in young adulthood and adult psychopathology. According to Baron and Kenny’s (1986) recommendations, all three conditions for testing such a model were met (see Figure 2): (a) The independent variable (anxious attachment) was related to the dependent variable (psychopathology), Path c: ΔR2 = .21, F(1, 48) = 12.94, p < .01, β = .46; (b) the independent variable was related to the mediator (emotion-focused strategies), Path a: ΔR2 = .26, F(1, 48) = 17.12, p < .01, β = .51; and (c) the mediator was related to the dependent variable, controlling for the independent variable, Path b: ΔR2 = .17, F(1, 47) = 13.05, p < .01, β = .48.
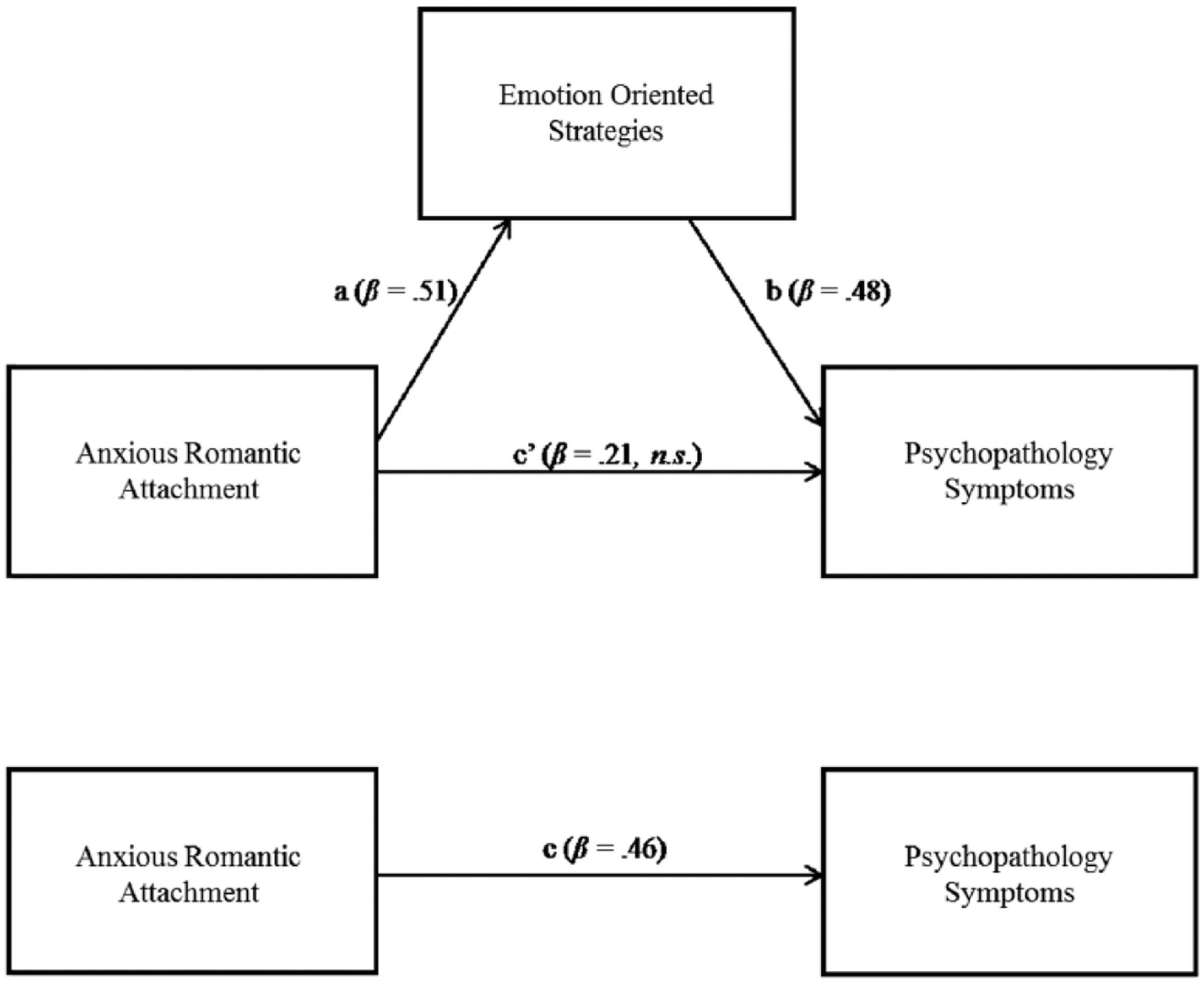
Mediation test between anxious romantic attachment in young adulthood and adult psychopathology via the use of emotion-focused strategies.
A final hierarchical regression with adult symptoms of psychopathology as the dependent variable was thus conducted with emotion-focused strategies entered in Step 1 and anxious attachment in Step 2. Results (see Table 4 and Figure 2) showed that, when taking into account the variance explained by emotion-focused strategies, anxious attachment was no longer significantly related to adult psychopathology, Path c’: ΔR2 = .03, F(1, 47) = 2.58, n.s. We further tested the significance of the mediated path using Preacher and Hayes’s (2004) bootstrapping methodology for indirect effects based on 1,000 bootstrap resamples. Results revealed an indirect effect of .0992 and a bias-corrected bootstrap 95% CI [.0350, .1771], indicating a significant decrease in the effect of anxious attachment on adult psychopathology. The use of emotion-focused strategies is therefore a complete mediator of the association between anxious attachment orientation in young adulthood and adult symptoms of psychopathology.
Hierarchical Regression Model With Anxious Romantic Attachment and Emotion-Focused Strategies in Young Adulthood as Predictors of Adult Symptoms of Psychopathology.

Note. SCL-90-R = Symptom Checklist 90–Revised; CISS = Coping Inventory for Stressful Situations; ECR = Experiences in Close Relationships.
p < .05. **p < .01.
Discussion
The overall objective of the present study was to (a) test a longitudinal model depicting the impact of attachment to parents and peers in adolescence and to romantic partners in young adulthood, on adult self-reported symptoms of psychopathology, and (b) test the theoretical assumption that specific emotion regulation strategies, that is, emotion-focused strategies and emotional expressivity, mediate associations between attachment insecurity (in adolescence and young adulthood) and adult symptoms of psychopathology. In doing so, our goal was to identify the mechanism through which earlier attachment relationships influenced the experience of adult symptoms of psychopathology. As expected, our results revealed that greater attachment insecurity toward parents in adolescence predicted greater symptoms of psychopathology in adulthood, 10 years later. Further analysis of this link revealed the partial mediating role of emotion-focused strategies. In addition, emotion-focused strategies fully mediated the positive association between anxious attachment in young adulthood and adult psychopathology. These findings and their implications are discussed in greater detail in the following sections.
Adolescent Attachment and Emotion-Focused Strategies as Predictors of Adult Symptoms of Psychopathology
Despite evidence suggesting concurrent associations between insecure attachment and psychopathology in adolescence (Laible et al., 2000; Lee & Hankin, 2009) and adulthood (Fortuna & Roisman, 2008; Lopez et al., 2001), the current study is the first to longitudinally investigate this relation across these two developmental periods (10-year lag). Specifically, we found greater parent–adolescent attachment insecurity to be associated with greater self-reported psychopathology in adulthood. Findings of this study therefore extend the existing concurrent literature by showing that attachment insecurity toward parents continues to be related to symptoms of psychopathology into the adult years. As expected, emotion-focused regulation strategies were also related to adult symptoms of psychopathology. We interpret these results as suggesting that, by resorting to emotion-focused strategies, including self-blame, ruminative thoughts, and feelings of helplessness in dealing with distress, negative emotions are not dealt with constructively. Rather than thinking of the problem in a more benign manner and finding appropriate solutions, individuals who use emotion-focused strategies become enveloped in the stressful situation, focused on the negative emotions associated with it, and overcome with feelings of helplessness (Mikulincer & Shaver, 2008). These strategies can thus serve to exacerbate one’s experience of negative emotions, contributing to the experience of symptoms of psychopathology in adulthood. Therefore, in accordance with our findings, emotion-focused strategies play a crucial and direct role in the presence of adult psychopathology.
We also found that, in addition to being related to adult symptoms of psychopathology 2 years later, emotion-focused strategies were also partial mediators of the association between insecure parent–adolescent attachment and adult symptoms of psychopathology. Our results are in line with those of previous studies showing that ineffective strategies mediate concurrent associations between insecure attachment and psychological distress (Lopez et al., 2001; Mallinckrodt & Wei, 2005). Nevertheless, emotion-focused strategies were only partial mediators, such that insecure attachment to parents in adolescence remained associated to adult psychopathology 10 years later. We interpret our results as providing evidence that internal working models associated with insecure attachment relationships toward parents predispose the individual to experience symptoms of psychopathology in adulthood (Davila et al., 2005; Dozier et al., 2008). Despite the fact that other attachment figures, namely, peers and romantic partners, may fulfill important attachment needs in later life (Allen, 2008), internal working models are primarily constructed from attachment-related experiences with parents in childhood and adolescence, when the individual is most vulnerable (Bowlby, 1982). These representational models form the basis for expectations and beliefs concerning the self and others as well as basic self-regulatory processes, which contribute to later symptoms of psychopathology (Bolwby, 1988; Main et al., 1985). During adolescence, in particular, when coping with developmental challenges are an inherent part of the parent–teen relationship, the quality of dyadic interactions may reinforce the teen’s internal working model regarding his or her ability to overcome difficult situations and the supportiveness and reliability of others (Dozier et al., 2008).
Anxious Romantic Attachment, Emotion-Focused Strategies, and Adult Psychopathology
Supported by results of past empirical studies, our initial findings suggested that anxious romantic attachment in young adulthood was related to greater self-reported symptoms of psychopathology, 2 years later (Fortuna & Roisman, 2008; Lopez et al., 2001; Mallinckrodt & Wei, 2005). Anxiously attached individuals are guided by negative working models of self and the world (Brennan et al., 1998; Collins & Read, 1990), that is, beliefs of being unworthy of receiving love and consistent support from their attachment figures. These individuals also fear partner abandonment and experience intense negative emotions in attachment-related contexts. Our results therefore suggest that these self-deprecating models may contribute to the experience of symptoms of psychopathology in adulthood.
However, our results further showed that anxious romantic attachment influenced the experience of symptoms of psychopathology via the use of emotion-focused strategies. Although we acknowledge that we did not control for earlier psychopathology, this study is nevertheless the first to demonstrate this indirect link using a 2-year delay, reinforcing the importance of the proposed model. These results are also in line with findings from previous studies (Cooper, Shaver, & Collins, 1998), suggesting that anxiously attached individuals may be caught in a vicious cycle whereby their negative views of self, coupled with their fears of partner abandonment, may lead them to be hypervigilant to negative cues and vulnerable to experiencing distress. To deal with these negative feelings, anxiously attached individuals may resort to emotion-focused strategies that include ruminations, self-blame, and feelings of helplessness in overcoming difficult situations alone (Mikulincer & Shaver, 2007, 2008), which can lead to greater feelings of distress and thus increases in self-reported symptoms of psychopathology over time.
Adolescent Attachment to Peers and Avoidant Attachment in Adulthood
In our study, adolescent attachment insecurity toward peers was unrelated to adult symptoms of psychopathology. Although this null finding may reflect a lack of power, it is concordant with that of Wilkinson and Walford (2001), who also failed to identify such an association using a concurrent design with a much larger sample (N = 404). This suggests that the concurrent association between attachment insecurity toward peers and symptoms of psychopathology demonstrated in a few studies (Laible et al., 2000; Lee & Hankin, 2009; Muris et al., 2001; Wilkinson, 2010) may not be maintained over time. Unlike attachment relationships with parents, which are enduring features of one’s life (Allen, 2008), attachment relationships with peers are more fleeting, with the formation of new friendships and the dissolution of others. Whereas adolescents’ friendships may contribute to alleviating or exacerbating symptoms of psychopathology in adolescence, this association is unlikely to carry over into adulthood. Additional studies with larger samples are thus necessary to provide support for the theoretical idea that the quality of attachment experiences with the most important caregiving figures, usually parents, is most predictive of the individual’s internal working model and future adaptation (Bretherton, 1987).
In line with the findings of Lopez et al. (2001), our results showed no relation between avoidant romantic attachment orientation in young adulthood and the global index of psychopathology. Past research has shown that avoidance is related to the development of symptoms of psychopathology only under extreme conditions of stress (Berant, Mikulincer, & Florian, 2001; Ein-Dor, Doron, Solomon, Mikulincer, & Shaver, 2010). Given our low-risk sample, the likelihood of our participants experiencing high levels of stress was limited, which may explain our nonsignificant findings. The lack of findings may also be attributed to under-reporting of symptoms of psychopathology by avoidantly attached individuals given their strategy of minimization of distress signals (Mikulincer & Shaver, 2007, 2008). Wei et al. (2003) suggested that these individuals may not report distress on simple measures with high face validity, as the one used in the present study. The authors found that when multiple measures of psychopathology were used, a positive association between avoidant attachment and psychological distress was more likely to be detected. Future studies using multiple measures of psychopathology are thus needed to clarify our lack of a significant association.
Emotional Expressivity and Symptoms of Psychopathology
Contrary to the expectation that a lack of emotional expressivity would be associated with greater symptoms of psychopathology 2 years later, the tendency to express emotions was unrelated to psychopathology in the present study. Again, these null findings may be attributed to the rather limited sample size of the current study. In fact, past studies have shown associations between lower emotional expressivity and greater prevalence of psychiatric disorders (i.e., alcohol and drug dependence, and depression; Corcos & Speranza, 2003), and higher emotional expressivity and fewer symptoms of psychological distress (Vogel et al., 2008). Using the same EES as the one used in the present study, Vogel et al. (2008) found that greater emotional expressivity was negatively associated with psychological distress when assessed concurrently in a large sample of undergraduate students. The authors proposed that highly distressed individuals may be less likely to openly express their emotions, given their expectation that communicating emotions may cause them to experience even greater unpleasant feelings (Vogel et al., 2008). In light of the results from the Vogel et al. study, and those of the present study, we suggest that, whereas emotional expressivity and psychopathology may be concurrently related, the tendency to express emotions may not buffer against future experience of symptoms of psychopathology. However, we interpret this null finding with caution given the restricted sample size of the current study.
Study Limitations
Several study limitations should be noted. First, owing to our limited sample size, the present study may have been under-powered, and thus, all null findings should be interpreted with caution. Moreover, we recognized the higher proportion of women in our sample such that study findings may be more applicable to women than men. Further studies with larger samples in which women and men are equally represented are necessary to confirm study results. Second, adolescent attachment security to parents and peers was assessed along a continuous dimension of insecurity, whereas adult attachment was assessed along the anxious and avoidant dimensions. Given this discrepancy, we were unable to assess the long-term association of anxious and avoidant attachment insecurity in adolescence and adulthood. A third limitation of the present study is that all study variables were self-reported, which may have engendered under-reporting of symptoms by avoidantly attached individuals and over-reporting by anxiously attached individuals. Moreover, individuals who endorsed emotion-focused regulation strategies may also have been more likely to over-report symptoms, given their focus on distress. Future studies should use various measures for assessing symptoms of psychopathology to correct for this possible bias. Last, given that we could not control for psychopathology symptoms in adolescence, we cannot rule out the possibility that self-reported symptoms in adulthood were persisting symptoms from the adolescent period. Replication studies of current findings should include an earlier measure of psychopathology to address this limitation. Nevertheless, our sample consisted of a normative population, reducing the likelihood that our results are an artifact of severe and persistent psychopathology.
Conclusion
In summary, findings from this study extend the investigation of adult adaptation by presenting new longitudinal associations spanning a 10-year period, that is, between the ages of 14 and 24. Specifically, results highlight the association between an insecure attachment to parents in adolescence and greater symptoms of psychopathology in adulthood. These results therefore make an important contribution to the existing attachment literature in showing, from a developmental perspective, that adolescents’ negative expectations and views within the context of an insecure relationship with parents are directly related to greater symptoms of psychopathology in adulthood, 10 years later. By identifying this developmental model, our results suggest that adolescent attachment to parents and the use of emotion-focused strategies in young adulthood may be important mechanisms to target in reducing symptoms of psychopathology in adulthood. For example, our findings directly support the theoretical framework of Emotion-Focused Couples Therapy (EFT; Johnson, 2004). This attachment-based intervention approach aims at improving couples’ negative interactions through changes in emotion regulation strategies. In a recent article by Dalgleish et al. (2014), the authors found that more anxiously attached individuals showed greater improvements in marital satisfaction following EFT. Accordingly, by providing anxiously attached individuals with more adaptive strategies for regulating their distress, these individuals are more likely to show increased psychosocial functioning. The results of the present article are also in line with the Attachment Based Family Therapy by Diamond, Siqueland, and Diamond (2003), which focuses on improving the quality of the parent–adolescent attachment relationship for depressed and suicidal adolescents. Taken together, based on our findings, prevention and intervention programs centered on fostering more secure parent–adolescent attachment relationships as well as more adaptive emotion regulation strategies in adulthood are crucial for thwarting or improving the experience of symptoms of psychopathology in the future. Nonetheless, the replication of our findings with larger samples using a pre/post-test experimental design is necessary to corroborate study conclusions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by the Social Sciences and Humanities Research Council of Canada (research grant) and the Fonds Québécois de Recherche sur la Société et la Culture (doctoral scholarship).