
Abstract
The purpose of this study was to examine the relationship between the Japanese version of the Developmental Coordination Disorder Questionnaire (DCDQ-J) and the Social Responsiveness Scale (SRS) in Japanese children with autism spectrum disorders (ASD). The participants were 19 children with ASD. The DCDQ-J is a parent questionnaire that can assess the degree of motor skill impairments, and the SRS assesses the severity of social impairments. To check the criterion-related validity of the DCDQ-J in children with ASD, the Japanese version of the Movement Assessment Battery for Children-2 (MABC2-J) was also conducted. The total score of the DCDQ-J was significantly negatively correlated with the SRS score in the same way as the MABC2-J total score. These results indicate that the severity of social impairments in children with ASD is related not only to the child’s fundamental motor abilities but also to practical motor skills in everyday life.
Introduction
In recent years, empirical studies have revealed the existence of motor skill impairments in children with autism spectrum disorders (ASD), using standardized assessment batteries such as the Movement Assessment Battery for Children (MABC; Henderson & Sugden, 1992). The MABC and its 2nd edition, MABC2 (Henderson, Sugden, & Barnett, 2007), are standard tests used worldwide to identify developmental coordination disorders (DCD; Blank, Smits-Engelsman, Polatajko, Wilson, & European Academy for Childhood Disability, 2012). In general, children with ASD between the ages of 6 and 15 years showed a lower total standard score with this test, indicating that their general level of motor skill was significantly lower than that of typically developing children (Green et al., 2002; Green et al., 2009; Hilton et al., 2007; Hirata et al., 2014; Miyahara et al., 1997; Whyatt & Craig, 2012).
Furthermore, some studies investigated the relationship between individual differences in MABC performance and social impairment in children with ASD. Hilton et al. (2007) conducted the MABC for children with Asperger syndrome (AS) and typical children aged 6 to 12 years, and their severity of social impairments was also assessed by the Social Responsiveness Scale (SRS; Constantino & Gruber, 2005), the internationally accepted parent report questionnaire of social impairments in children. The results indicated that the MABC total standard score was interrelated with the SRS score among the two groups. In recent years, Hirata et al. (2014) conducted the Japanese versions of the MABC2 (MABC2-J) and the SRS (Kamio et al., 2013) only for children with ASD aged 7 to 15 years who were without severe intellectual impairments, and the relationship between each measure was investigated. The results from the MABC2-J indicated that difficulties with manual dexterity (MD) were the most frequently occurring problems in children with ASD. The SRS score also strongly interrelated with each MABC2 standard score. The results of these two studies using either the MABC or MABC2 and the SRS indicate the possibility that motor skill impairments are interrelated with social impairments in children with ASD. Hirata et al. suggested the possibility that the same neurological dysfunction such as cerebellar dysfunction might explain the motor–social link in children with ASD. Dyck, Piek, Hay, and Hallmayer (2007) and Hilton, Zhang, White, Klohr, and Constantino (2012) both reported similar results, although they used different measures of motor and social abilities. Dyck et al. assessed several abilities in children with ASD aged 4 to 13 years, and investigated the relationship between their motor and social abilities. The measures used in their study were the McCarron assessment of neuromuscular development, which could objectively assess the child’s fine and gross motor ability (McCarron, 1997), and the Autism Diagnostic Interview (ADI; Lord, Rutter, & Le Couteur, 1994), which is the internationally accepted semi-structured interview for parents designed to evaluate the child’s qualitative impairments in reciprocal social interaction. The results indicate that scores of each measure were interrelated, and Dyck et al. suggested the possibility that the process underlying motor coordination is a core deficit in children with ASD. Hilton et al. objectively assessed the motor abilities of children with ASD aged 4 to 20 years using the Bruininks-Oseretsky Test of Motor Proficiency, 2nd edition (BOT-2; Bruininks & Bruininks, 2005), and the severity of social impairments were evaluated by the SRS. The BOT-2 scores were interrelated with the SRS score, and Hilton et al. suggested the possibility that motor impairment constitutes a core component of ASD in the same manner as postulated by Dyck et al.
In light of the studies mentioned above, it may be safely assumed that motor skill impairments and social impairments are interrelated in children with ASD. To date, however, few attempts have been made to investigate such a relationship. von Hofsten and Rosander (2012) argued that the comorbidity of motor skill impairments and social impairments indicates the possibility of a common brain dysfunction in the background of motor and social abilities in children with ASD. Thus, an examination of the relationship between motor skill impairments and social impairments may provide further understanding and new insight into the underlying neural mechanism of ASD. In this study, we investigated the relationship between motor skill impairments and social impairments in Japanese children with ASD, using a new scale, that is, the Japanese version of the Developmental Coordination Disorder Questionnaire-2007 (DCDQ-J; Nakai et al., 2011).
Many authors agree that motor skill assessments, such as the MABC2, are time consuming and expensive, and that parent questionnaires may form an efficient alternative for screening large numbers of individuals for DCD (Civetta & Hillier, 2008). The original version of DCDQ was developed by Wilson, Kaplan, Crawford, Campbell, and Dewey (2000) and revised in 2007 (DCDQ-2007; Wilson et al., 2009). The DCDQ-2007 has been reported as a reliable and suitable measure for identifying children with motor skill impairments, and a strong relationship between the DCDQ-2007 total score and MABC2 total standard score was found in typical children or children with motor difficulties (Pannekoek, Rigoli, Piek, & Barrett, 2012; Wilson et al., 2009). The DCDQ has already been translated into many languages, and the European Academy for Childhood Disability (EACD) guideline recommends it as the best evaluated questionnaire (Blank et al., 2012). However, there are very few studies that used the DCDQ-2007 for children with ASD (i.e., Hilton et al., 2012; Miyachi et al., 2014). Previous studies revealed that DCDQ-2007 scores were interrelated with BOT-2 scores (Hilton et al., 2012) and the severity of stereotyped behavior (Miyachi et al., 2014) in children with ASD. To our knowledge, the relationship between DCDQ-2007 and SRS in children with ASD has not been investigated. In children without ASD, the DCDQ-2007 and the MABC2 can assess relatively similar motor ability, but each measure also evaluates different aspects of motor ability (Wilson et al., 2009). The MABC2 is designed to assess Criterion A of the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) criteria for DCD, and the DCDQ-2007 is designed to assess Criterion B of the DSM-IV-TR. In other words, the MABC2 is used for objective assessment of a child’s fundamental motor abilities in a clinical setting, whereas the DCDQ-2007 is used for subjective assessment of a child’s motor abilities in broader settings such as his or her natural environment in daily living. If the DCDQ-2007 score were interrelated with the SRS score in children with ASD in the same way as the MABC2, evidence of the motor–social link in children with ASD would become more robust. In this study, we tried to clarify this point using the Japanese version of the DCDQ-2007 (DCDQ-J; Nakai et al., 2011). However, the criterion-related validity of the DCDQ-J, such as its relationship with MABC2-J, has not yet been well investigated. Thus, we investigated the relationship between DCDQ-J and MABC2-J in Japanese children with ASD. In a previous study, Green et al. (2009) investigated the degree of motor skill impairments in children with ASD using the MABC and DCDQ. Their results indicated that motor skill impairments are common in children with ASD, and the DCDQ performed moderately well as a screen for possible motor difficulties. However, in the study of Green et al., children with moderate intellectual impairments were also included. For them, their low performance on the MABC may have been due to their difficulties in understanding and following instructions. Based on this possibility, only participants without additional intellectual difficulties were included in this study.
To summarize, the purpose of this study was to examine the relationship between DCDQ-J and SRS in children with ASD who were without intellectual disabilities. To check the criterion-related validity of the DCDQ-J in children with ASD, the MABC2-J was also conducted. This type of research will increase our understanding of children with ASD and contribute toward developing an assessment method for children with ASD.
Method
Participants
We recruited children with ASD from elementary and junior high schools in the neighborhood of Tokyo Gakugei University (Koganei City, Tokyo) who met the following conditions. First, children were diagnosed by child psychiatrists as having Pervasive Developmental Disorder (PDD) based on the DSM-IV-TR criteria. Second, children were confirmed to be free from severe sensory, neurological, or muscular impairments such as blindness, low vision, deafness, and cerebral palsy. Third, to control for underlying intellectual effects, such as difficulties in understanding and following instructions, the children were confirmed not to have severe intellectual difficulties by their parents. Ultimately, 19 children with ASD (17 males, 2 females) participated. Their chronological ages (CAs) ranged from 7 to 15 years. We measured the participants’ IQs by the Wechsler Intelligence Scale, Japanese version (Japanese WISC-4 Publication Committee, 2010), which is a standardized and commonly used test in Japan. All 19 children were included in this study because their full IQs ranged from 75 to 124. It appeared that they did not have additional intellectual difficulties. Among participants, 3 were diagnosed with AS, 3 with high-functioning autism (HFA), and 13 were with PDD-not otherwise specified (NOS).
The DCDQ-J
The DCDQ-J (Nakai et al., 2011), a 15-item questionnaire, is a parent’s and/or teacher’s reported measure of a child’s motor skill characteristics in ordinary settings. In this study, the mothers evaluated their own children. The DCDQ-J provides raw scores for three sub-scales of motor skill: Control During Movement (CDM), Fine Motor/Handwriting (FM), and General Coordination (GC), as well as the total score calculated by combining these scores. Each item was rated on a 5-point scale, and lower scores indicated greater difficulties with motor skills. The DCDQ-2007 provides a cutoff point of the total score to identify motor difficulties. However, the DCDQ-J as yet does not have such a cutoff point. Thus, in this study, we used the cutoff point of the DCDQ-2007 (Wilson et al., 2009).
The MABC2-J
The MABC2-J (Henderson et al., 2007), now in development, was used to assess motor skill impairment. This test can assess children aged 3 to 16 years, and consists of eight sub-tests, which make up a total motor score and three sub-component scores: MD, aiming and catching (AC), and balance (BAL). The structural validity of MABC2 was confirmed using confirmatory factor analysis (Schulz, Henderson, Sugden, & Barnett, 2011). A norm attached to the test manual was used when total raw scores were converted to total standard scores (M = 10, SD = 3) and percentiles. Lower standard scores indicate greater severity of motor skill impairments.
The Japanese Version of the SRS
The Japanese version of the SRS (Constantino & Gruber, 2005; Kamio et al., 2013) was used to quantitatively assess the severity of social impairments. The SRS, a 65-item questionnaire, is a parent- and/or teacher-reported measure of a child’s social impairments in ordinary social settings. In this study, the mothers evaluated their own children. Each item was rated on a 4-point scale, and the norm attached to the original test manual was used when raw scores were converted to a total T score (M = 50, SD = 10). Higher scores indicated greater severity of social impairments. To check the accuracy of ASD diagnosis, we classified the participants’ level of social impairments based on SRS scores according to the SRS manual. Impairment levels were from the “severe range (76 ≤ T, n = 10),” to the “mild-to-moderate range (60 ≤ T ≤ 75, n = 9).” Children in the “severe range” and “mild-to-moderate range” met the DSM criteria for PDD.
Procedure
Ethical approval for the study was obtained from the Research Ethics Board of Tokyo Gakugei University. Consent for participation in this study was obtained from the participant’s parents, and the children were under no obligation to take part in the tests. Each participant was assessed in two sessions. The MABC2-J was administered to the children in the first session and the Wechsler Intelligence Scale to the second. These sessions were conducted in a private room in Tokyo Gakugei University. While the children performed tasks from the MABC2-J, their mothers completed the SRS and DCDQ-J in another room. The Japanese version of the Wechsler Intelligence Scale for Children (4th ed.; WISC-IV) was conducted on another day.
Statistical Analysis
SPSS software (Version 22.0; SPSS, Inc., 2013) was used for statistical analysis. All the measured values (Table 1) were tested for deviation from normality. The tests revealed that not all the measures were normally distributed. Thus, nonparametric analyses were used in this study. Spearman’s rank correlation was used to analyze the relationship between the measures. In this study, we used a group with relatively heterogeneous CA and IQ ranges, and examined rank correlations between measured values and participant’s CA or IQ. All the measured values were not significantly and strongly correlated with participant’s CA and IQ. Thus, we did not use participant’s CA and IQ as a covariate in any statistical analysis. To check the criterion-related validity of DCDQ-J, we also investigated the relationship between the cutoff points of the MABC2-J and DCDQ-J. In this study, the MABC2-J was used as a criterion measure. According to many previous studies (Pannekoek et al., 2012; Wilson et al., 2009), the 15th percentile of the MABC2-J total score was used as the cutoff point for identifying motor difficulties.
Participant Characteristics (n = 19).

Note. CA = chronological age; IQ = intelligence quotient; SRS = Social Responsiveness Scale; DCDQ = Developmental Coordination Disorder Questionnaire; MABC2 = Movement Assessment Battery for Children-2.
Results
Table 1 presents the characteristics of the participants such as CA, IQ, SRS T score, DCDQ-J scores, and MABC2-J total standard score.
We classified the DCDQ-J total raw score into two groups: “definite motor difficulties” and “no motor difficulties” by using the cutoff point of DCDQ-2007 (Wilson et al., 2009). All participants were classified into the “definite motor difficulties” group. We also classified the percentile of the MABC2-J total standard score into two groups according to many previous studies: “definite motor difficulties (below the 15th percentile)”’ and “no motor difficulties (above the 16th percentile).” Forty-seven percent of the children with ASD scored below the 15th percentile in their total standard score. Table 2 shows the relationship between each category. We calculated each case for factors of discrimination accuracy, such as sensitivity and specificity. The sensitivity of the cutoff point of the DCDQ-J raw total score was 100%, while the specificity was 0% as a consequence of the number of true negatives being 0.
Relationship Between Each Category of DCDQ-J and MABC2-J.
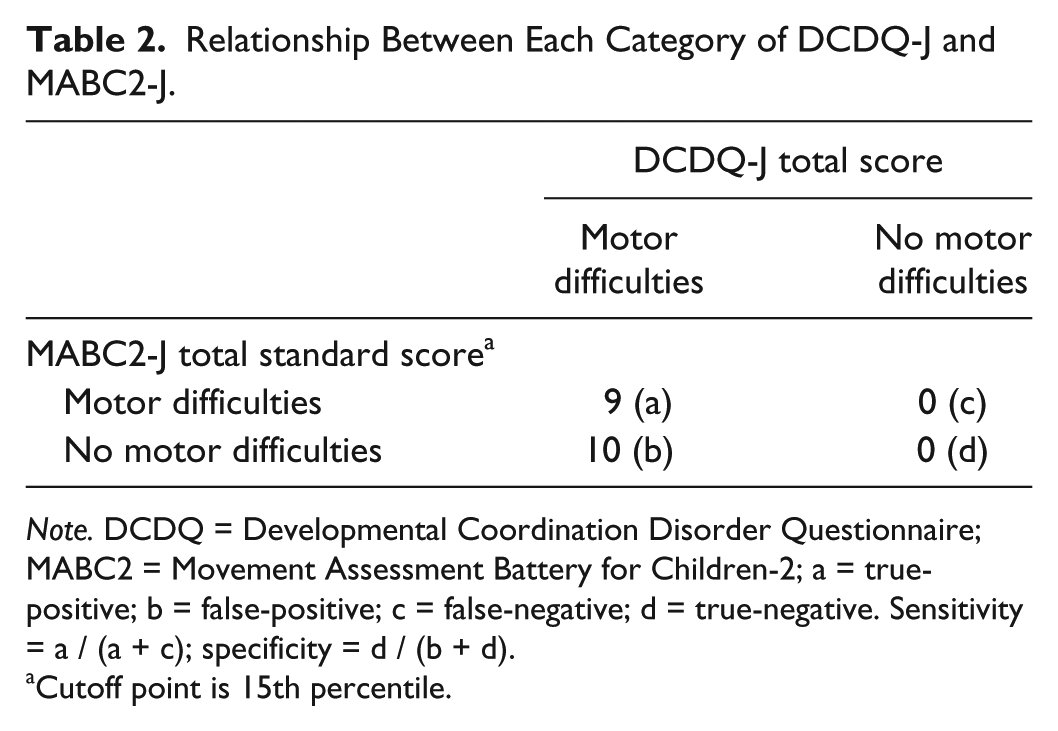
Note. DCDQ = Developmental Coordination Disorder Questionnaire; MABC2 = Movement Assessment Battery for Children-2; a = true-positive; b = false-positive; c = false-negative; d = true-negative. Sensitivity = a / (a + c); specificity = d / (b + d).
Cutoff point is 15th percentile.
Next, we calculated the Spearman’s rank correlations between measures. Table 3 shows the results. The DCDQ-J total score was significantly correlated negatively with the SRS T score (rs = −.72, p < .01), that is, the lower the DCDQ-J total score, the higher the SRS T score. However, the DCDQ-J total score was significantly correlated positively with the MABC2-J total standard score (rs = .74, p < .01). The MABC2-J total standard score was significantly correlated negatively with the SRS T score (rs = −.51, p < .05). We also calculated the Spearman’s rank correlations between the SRS T score and each sub-scale of DCDQ-J. Correlations between SRS and DCDQ-J sub-scales ranged from −.54 to −.64, and all the coefficients were statistically significant.
Spearman’s Rank Correlations Between Motor Skill and SRS.
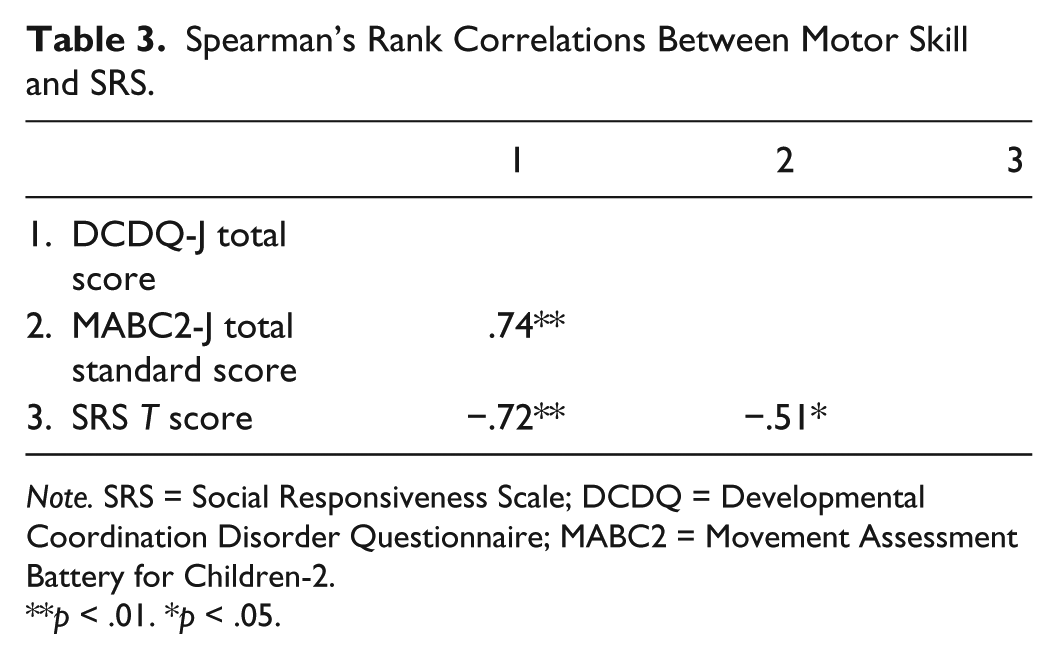
Note. SRS = Social Responsiveness Scale; DCDQ = Developmental Coordination Disorder Questionnaire; MABC2 = Movement Assessment Battery for Children-2.
p < .01. *p < .05.
Discussion
Relationship Between DCDQ-J and SRS
In this study, we evaluated the degree of motor skill impairments in Japanese children with ASD using the DCDQ-J, and examined the relationship between the DCDQ-J and SRS. According to previous studies using the DCDQ or DCDQ-2007 (Green et al., 2009; Hilton et al., 2012; Miyachi et al., 2014), the DCDQ-J total score indicated that motor skill impairments are common in children with ASD. It should also be emphasized that the DCDQ-J scores were interrelated with the SRS scores, that is, the more severe the motor skill impairments, the more severe the social impairments. These results are in agreement with Hirata et al. (2014) who used the MABC2-J for Japanese children with ASD. The DCDQ-2007 and the MABC2 are used worldwide as standard motor tests for identifying DCD. As mentioned in the “Introduction,” the DCDQ-2007 and the MABC2 can assess relatively similar motor ability, but each measure also evaluates different aspects of motor ability (Wilson et al., 2009). The MABC2 is used for objective assessment of a child’s fundamental motor abilities in a clinical setting, whereas the DCDQ-2007 is used for subjective assessment of a child’s motor abilities in broader settings such as his or her natural environment in daily living. The resulting DCDQ-J score was strongly interrelated with the SRS score in the same way as the MABC2-J score, which means that the severity of social impairments in children with ASD is related not only to the child’s fundamental motor abilities but also to practical motor abilities in everyday life. It seems that this result provides further support for the motor–social link in children with ASD. In this study, three sub-scales in the DCDQ-J were related at the same degree with SRS score. However, Hirata et al. reported that the severity of social impairments was most strongly interrelated with the manual dexterity score of the MABC2-J. We should therefore consider the heterogeneity of motor skill impairments in children with ASD. Hirata et al. also pointed out the possibility that several groups with different motor skill impairments may exist among children with ASD. However, we could not reach a robust conclusion because the participant group was too small. In a future study, we should resolve this methodological problem and try to check these hypotheses with a large number of participants.
The association between motor skill impairments and social impairments in persons with ASD is a current hot topic. Several researchers have found that performance in motor tasks and tasks that evaluated social impairments were linked in children with ASD (Dyck et al., 2007; Hilton et al., 2007; Hilton et al., 2012; Hirata et al., 2014; MacDonald, Lord, & Ulrich, 2013). However, the question of why motor skill and social impairments are interrelated in children with ASD remains unanswered. From a neurological perspective (Hilton et al., 2007; von Hofsten & Rosander, 2012), comorbidity of motor skill impairments and social impairments in children with ASD indicates the possibility of a common brain dysfunction. Some authors have pointed out the possibility that cerebellar dysfunction could explain why individual differences in motor control were strongly interrelated with social impairments in children with ASD (Hirata et al., 2014; Papadopoulos et al., 2012). In current neuroscience studies, the cerebellum is considered to play an important role not only in the control of skilled movement but also in the individual’s interaction with others in social settings (Ito, 2008; Vakalopoulos, 2013). Cerebellar abnormality in autism, for example, has been consistently shown from neuroimaging studies (Courchensne, Hesselink, Jernigan, & Yeung-Courchensne, 1987). For future research, investigation of the cerebellum’s role in various psychological domains in children with ASD is warranted. Developmental perspective also seems to be important. Bhat, Landa, and Galloway (2011) suggested the possibility that small differences in early motor development are among the essential factors that affect early social development of toddlers with ASD. As a result, motor skill and social impairments were considered to still be interrelated in older children with ASD. MacDonald, Lord, and Ulrich (2014) recently reported that motor skill impairments were interrelated with social impairments in young children with ASD aged 14 to 33 months. To reveal the manifestation process of the motor–social link in children with ASD, a longitudinal investigation focused on the motor development of ASD is necessary.
Relationship Between DCDQ-J and MABC2-J
This is the first study to examine the relationship between DCDQ-J and MABC2-J in Japanese children with ASD. The correlation between the DCDQ-J total score and the MABC2-J total standard score was statically significant in children with ASD. Thus, it seems possible that the DCDQ-J can be used as a quantitative measure of the severity of motor skill impairments for Japanese children with ASD. With respect to discrimination accuracy, Pannekoek et al. (2012) have already found incomplete agreement in the classification of motor difficulties by the MABC2 and the DCDQ-2007. A similar result was also obtained in this study. Considering that the two motor measures used in this study assessed overlapping but distinct constructs, it is not surprising that a discrepancy between the cutoff points of the MABC2-J and DCDQ-J occurred. However, we should note that the number of true negatives was 0. Considering that the DCDQ-2007 tends to be used for the initial screening for DCD, sensitivity seems to be more important than specificity (Wilson et al., 2009). It may be said that the DCDQ-J has a role as a screening tool for DCD because the number of false negatives was also 0. Furthermore, the degree of motor skill impairments of the false-positive group might be so low as to not have a diagnosis of DCD. Atypical or insufficient movement characteristics of children with ASD were often reported (i.e., Mari, Castiello, Marks, Marraffa, & Prior, 2003; Rinehart et al., 2006). It is necessary to check the degree of motor skill impairments of children with ASD from some point of view other than DCD. In a future study, we plan to conduct a similar investigation for more children with or without ASD, and examine the criterion-related validity of the DCDQ-J.
Limitations
There are many limitations in this study. The small number of participants limits its generalizability. The lack of Japanese standardizations of the MABC2-J and other behavioral measures of social functioning in ASD are additional limitations. These methodological problems are issues that can be addressed in future studies.
Footnotes
Acknowledgements
The authors are grateful to the children and parents who participated.
Authors’ Note
Shogo Hirata and Akio Nakai contributed equally to the study. The research use in Japan and the development of the Japanese version of the MABC2 are based on a contract between Akio Nakai and Pearson Education Limited, with the great support of Prof. Sheila E. Henderson, David A. Sugden, and Anna Barnett.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was supported in part by the Japan Society for the Promotion of Science and Research Grant from the Ministry of Health, Labour, and Welfare, Japan.