
Abstract
This study examines the health of elderly Korean Canadians in home care and investigates the risk factors for caregiver distress of families caring for their elderly relatives. Korean Canadians, Chinese Canadians, and other Canadian home care clients were compared using the Resident Assessment Instrument–Home Care (RAI-HC). The assessments were done as a part of normal clinical practice between January 2002 and December 2010 within Ontario. A sample of 58,557 home care clients was analyzed using descriptive statistics and chi-square analysis at the bivariate level and multiple logistic regression models. The major finding of the present study is that Korean clients had higher physical impairments and higher prevalence of major chronic diseases, but they were less likely to receive personal support or nursing services. Moreover, the results provide clear evidence of the importance of language barriers for all linguistic minorities, including Korean Canadians.
Introduction
Immigration in Canada
Changes in immigration laws in 1966 led to a substantial rise in the number of Asian immigrants to Canada (A. H. Kim, 2008). About 3.7% of the total Canadian population is Chinese immigrants (Statistics Canada, 2007). Korean immigrants came to Canada in increasing numbers over the past two decades, and they now represent 0.3% of the total Canadian population. However, the size of the Korean Canadian population is increasing faster with a growth rate of 53%, compared to 19% growth in the Chinese Canadian population and only 4% growth for the general population between 1996 and 2001 (A. H. Kim, 2008; M. Kwak & Hiebert, 2010; Statistics Canada, 2007).
In Ontario, 90% of Korean Canadians and Chinese Canadians reside in four of the fourteen health regions within the province: Mississauga Halton, Toronto Central, Central, and Central East (Ontario Association of Community Care Access Centers, 2010). These regions have clusters of Chinese or Korean neighborhoods providing access to informal support networks with shared cultural heritages. However, formal service providers may also provide culture-specific services (e.g., Chinese- and Korean-speaking care coordinators). In other regions of Ontario, these useful services may not be readily available.
Acculturation
Immigrants become more acculturated to a host culture over time, but only when it occurs at young age (Cheung, Chudek, & Heine, 2011). Better language acquisition among young immigrants is an important contributor to this adaptation (Hakuta, Bialystok, & Wiley, 2003). Conversely, immigration later in life is stressful because of cultural adjustments and language barriers that are likely to be more severe (Mui, 1996, 2001). Challenges such as discrimination, communication difficulties, lack of social resources, and feelings of detachment in the society may affect adaptation to the host environment (Bernstein, Park, Shin, Cho, & Park, 2011; Kiefer, Kum, & Choi, 1985; Lai & Chau, 2007; Mui, 2001). Elderly Asian immigrants often lack information and preparation to adjust to the major changes in cultural norms and social conditions (Mui, 1996, 2001). About 6% of Korean immigrants and 10% of Chinese immigrants are aged above 65 (Statistics Canada, 2006, 2007). Thus, elderly immigrants are a minority within a minority, making them a vulnerable and understudied group (Ma, Chu, & Tsou, 2002).
Cultural Values
The traditional Korean culture, similar to Chinese culture, places family as a focal point of social organization and encourages family well-being and interdependence (Lai, 2007). Korean culture, based on familism, is strongly kinship-oriented and discourages individual needs and desires (Chun, Knight, & Youn, 2007; J. Kim & Lee, 2003). The core value of family obligation involves the Confucian tradition of filial piety (Hanzawa et al., 2010; A. H. Kim, 2010; Roh, 2010), which emphasizes that children must respect and give thoughtful attention to their elders for giving birth and rearing them into adulthood (Han, Choi, Kim, Lee, & Kim, 2008; A. H. Kim, 2010; J. Kim & Lee, 2003; Lai, 2007). Thus, institutionalization or receiving external health or social services may be viewed negatively in this culture (A. H. Kim, 2010, G. Kwak & Lai, 2012). These social values promote an intense moral obligation to support aged parents. In addition, Asian culture values stoicism and patience, which encourages keeping feelings in rather than expressing them and experiencing sorrow silently (Pang, 1995).
Cultural Values and Immigration
Immigrants experience cultural changes as a result of the process of acculturation or the interaction between the original and the new culture (Berry, 2006; W. Kim, 2002). Western culture, unlike Korean culture, emphasizes individualistic lifestyles and values independence and personal freedom (Choi, 1993; Hanson, Sauer, & Seelbach, 1983; Y. Lee, 1995; Spence, 1985). Some North American studies suggest that a continuation of traditional Korean values after immigration encourages families to care for and live with their aged parents (Jun, 2005; A. H. Kim, 2010; Park, 2012; Yoo, 2014; Yoo & Kim, 2010). However, there is also evidence of changes in values toward a greater focus on independence, autonomy, and youth (Wong, Yoo, & Stewart, 2006; Yoo, 2014). The likelihood of this change is affected by the age at immigration, the length of exposure to lifestyles of other cultures, and education levels (Hyun, 2001). As more adult children integrate into Western society, one might expect the use of formal health care services such as home care to increase among older Koreans.
Despite these changes, there is clear evidence that family members still provide substantial levels of support to elderly family members living with them to avoid reliance on outside assistance (A. H. Kim, 2010, G. Kwak & Lai, 2012; M. Lee, Yoon, & Kropf, 2007). Family members caring for older adults may experience caregiver distress in the form of physical, psychological, emotional, social, and financial stress (A. H. Kim, 2010; G. Kwak & Lai, 2012; Lai, 2008; H. Lee & Singh, 2010). The likelihood of caregiver distress has been shown to be related to cognitive and functional status of the elderly (Chang & Horrocks, 2006; S. Kim et al., 2006; Lim, Son, Song, & Beattie, 2008).
Many studies, regarding the gender differences, cultural predictors, use of formal services, and service barriers, have been conducted on Chinese Canadian caregivers (Chappell & Kusch, 2007; Chappell & Funk, 2011; Ho, Friedland, Rappolt, & Noh, 2003; Lai, 2007, 2008, 2009a, 2009b; Lai & Leonenko, 2007; Lai, Luk, & Andruske, 2007; Lai & Surood, 2010; J. Lee & Bell, 2011). However, only a limited number of studies are available for Korean Canadian caregivers. A few studies investigate living arrangements and social support for older Korean immigrants (A. H. Kim, 2010; G. Kwak, 2010; G. Kwak & Lai, 2012), and one thesis exists on Korean informal caregiver distress in Canada (Jun, 2005).
Research Questions
The Andersen–Newman behavioral model of use of health services postulates that culture and ethnicity is one of the predisposing factors that can affect health service use (Andersen, 1995). Thus, the traditional culture and the process of acculturation would be expected to have important implications for the use of health services by Korean immigrants. The key questions of interest in the present study are whether Korean Canadian home care clients differ in their levels of need, access to services, and rates of caregiver distress compared with Chinese Canadians and the general population of home care clients.
Although the present study will not test for the causal pathways between access to health service and cultural values, it will provide the most detailed Canadian data available to date on characteristics associated with differences in service use and caregiver distress among the two main subpopulations of Asian Canadians.
Chinese Canadian clients were selected as a comparison group because they have some similarities to Koreans in terms of norms related to filial piety, community orientation, and religious/cultural heritage. However, there are also important differences between these groups that suggest they should not be combined a priori as a homogeneous cultural minority (e.g., recency of migration, size of diaspora in Canada).
Method
Sample
This study was based on secondary analyses of de-identified data for all long-stay home care clients assessed as part of normal clinical practice by health professionals in 14 Ontario Community Care Access Centers (CCAC) using the Resident Assessment Instrument–Home Care (RAI-HC; Canadian Institute for Health Information, 2014b). CCAC are single entry point agencies funded by the Ontario Ministry of Health and Long-Term Care that evaluate the need for and provide access to the care that vulnerable persons need in home and community settings. RAI-HC assessments examined here were completed between January 2002 and December 2010. Personal identifiers, such as name and health card number, were stripped from the record or encrypted in a way that would prevent identification prior to the transmission of the data to the research group, and unique client identifiers were given by the Ontario Association of CCAC. For all CCAC clients, assessments were performed by trained health professionals (e.g., care coordinators and nurses) as part of the standard clinical practice done on admission and thereafter every 6 months or on significant clinical change. Missing data were generally not a major concern given that the assessment is a mandatory requirement and the data were used by multiple stakeholders who require complete data.
The study sample was drawn from the population of all long-stay home care clients admitted during the study period (N = 705,922). Using a variable for primary language, it was possible to identify clients whose primary language was Korean (1,017) or Chinese (11,508). All clients from both groups were retained for the present study to maximize the power to detect differences for each subgroup compared with the general population. However, given that the other home care clients included almost 690,000 cases, a subset was randomly selected to yield a comparison group of 46,032 clients who had a primary language other than Chinese or Korean. A guideline of 4 times greater than the largest subgroup (Chinese Canadians) was used to set the sample size for the comparison group, which is consistent with methods used in the case-control literature (Grimes & Schulz, 2005).
Data Source
RAI-HC is a person-centered assessment system developed for use with adults in home and community-based settings that has been shown to have good reliability and validity (Hirdes, Ljunggren et al., 2008; Landi et al., 2000; Morris, Carpenter, Berg, & Jones, 1997). The instrument focuses on the person’s functioning and quality of life by assessing needs, strengths, and preferences in a broad range of domains consisting of more than 300 items.
Two RAI-HC items were used to define caregiver distress: “A caregiver is unable to continue in caring activities, e.g., decline in the health of the caregiver makes it difficult to continue,” and “Primary caregiver expresses feelings of distress, anger, or depression.” The presence of either of these indicators was considered indicative of potential distress. Although the first indicator may be caused by other factors (e.g., aging of the caregiver), it will also include health declines associated with caregiver burden. These items on caregiver distress have been used previously to develop the Method for Assigning Priority Levels (MAPLe) decision support algorithm for prioritization of home care clients’ access to community and facility-based health services (Hirdes, Poss, & Curtin-Telegdi, 2008).
Ethnicity was obtained from the RAI-HC assessment item on preferred language. Care coordinators completing the assessment used standard language codes provided by the Canadian Institute for Health Information as part of the Home Care Reporting System technical specification (Canadian Institute for Health Information, 2014a). In addition, the “need for an interpreter” item was assessed directly based on the client’s or caregiver’s response; hence, it was not inferred from the client’s ethnicity.
The items describing the profile of health and health service use for Korean Canadians, Chinese Canadians, and other Canadians were chosen based on a paper by Hirdes, Mitchell, Maxwell, and White (2011). These items are commonly used to describe health status and health service use.
Several summary scales can be derived from RAI-HC assessments to described a client’s health and functional status. The Activities of Daily Living Hierarchy (ADLH) Scale measures physical disability, with scores ranging from 0 (no impairment) to 6 (total dependence) by considering performance in early loss (e.g., dressing) to late loss (e.g., eating) ADLs (Landi et al., 2000; Morris, Fries, & Morris, 1999; Morris et al., 1997). The Changes in Health, End-stage disease and Signs and Symptoms (CHESS) Scale identifies individuals at risk of serious health decline, with scores ranging from 0 (not at all unstable) to 5 (highly unstable; Armstrong, Stolee, Hirdes, & Poss, 2010; Hirdes, Frijters, & Teare, 2003). The Cognitive Performance Scale (CPS) is based on memory impairment, level of consciousness, and executive function, with scores ranging from 0 (intact) to 6 (very severe impairment; Landi et al., 2000; Morris et al., 1994). The Depression Rating Scale (DRS) screens for depressive symptoms with values ranging from 0 (no depressive symptoms) to 14 (severe depressive symptoms; Burrows, Morris, Simon, Hirdes, & Phillips, 2000; Szczerbińska, Hirdes, & Zyczkowska, 2011). The Instrumental ADL capacity (IADL) Scale, which ranges from 0 to 6, considers meal preparation, ordinary housework, and phone use, with higher scores indicating greater difficulty in IADL (Morris, Carpenter, Berg, & Jones, 2000). The interRAI Pain Scale uses frequency and intensity of pain to create a score from 0 to 3 (Fries, Simon, Morris, Flodstrom, & Bookstein, 2001). Finally, the Method for Assigning Priority Levels (MAPLe) decision support algorithm ranges from low to very high with higher scores indicating greater needs. MAPLe has been shown to predict nursing home placement, caregiver distress, and ratings that the “client would be better off in other living environment” in many different international jurisdictions (Hirdes, Poss et al., 2008). MAPLe has also been validated as a predictor of institutionalization from acute hospital settings (Noro et al., 2011). Hence, all scales used in the present analyses have good reliability and validity, and are positively associated with impairment (Morris et al., 1999; Morris et al., 1997; Hirdes, Ljunggren et al., 2008; Landi et al., 2000). Studies with interRAI instruments in Asian countries have also reported similar results (see, for example, Chi, 2011; Chi, Chou, Kwan, Lam, & Lam, 2006; Chou & Chi, 2008; Kang, Lee, Kim, Park, & Yoon, 2008; Kwan, Chi, Lam, Lam, & Chou, 2000).
Scores on the summary scales were divided into different categories using cutoffs previously used by Hirdes et al. (2011). These scale cutoffs were specified prior to examining caregiver distress.
RAI-HC has been mandated for use in eight Canadian provinces and territories (Canadian Home Care Association, 2008). It has been used extensively in other countries including Denmark, Finland, Iceland, Norway, Sweden, Czech Republic, France, Germany, Italy, the Netherlands, and England (see, for example, Carpenter et al., 2004; Sørbye et al., 2009). In addition to its clinical applications for care planning and outcome measurement, RAI-HC can also be used for case-mix classification (Björkgren, Fries, & Shugarman, 2000; Poss, Hirdes, Fries, McKillop, & Chase, 2008) and quality measurement (Bos et al., 2007; Dalby, Hirdes, & Fries, 2005; Hirdes et al., 2004).
Ethics Clearance
Ethics clearance for secondary analysis of the data was obtained through the University of Waterloo, Office of Human Research.
Statistical Analysis
To provide a descriptive profile of the health of elderly Korean Canadians in home care, data were analyzed first to obtain percentage and frequency distributions. Bivariate differences in socio-demographic, clinical, caregiving, and health service use characteristics by ethnicity were evaluated with chi-square analysis using a two-tailed test with an alpha level of .05. In addition, temporal effects were examined using 2002 as a reference year, but no significant differences were found over time in the key dependent variable of interest (caregiver distress).
The bivariate analyses reported in Tables 1 to 4 were used to identify how the three cultural groups differed with respect to important clinical and service use variables. The MAPLe algorithm in Table 5 provides a risk adjustment variable that incorporates most of the important clinical scales and items referred to in the earlier tables.
Percentage of Home Care Clients With Selected Socio-Demographic, Diagnostic, and Health Characteristics by Ethnicity, Ontario, 2002-2010.
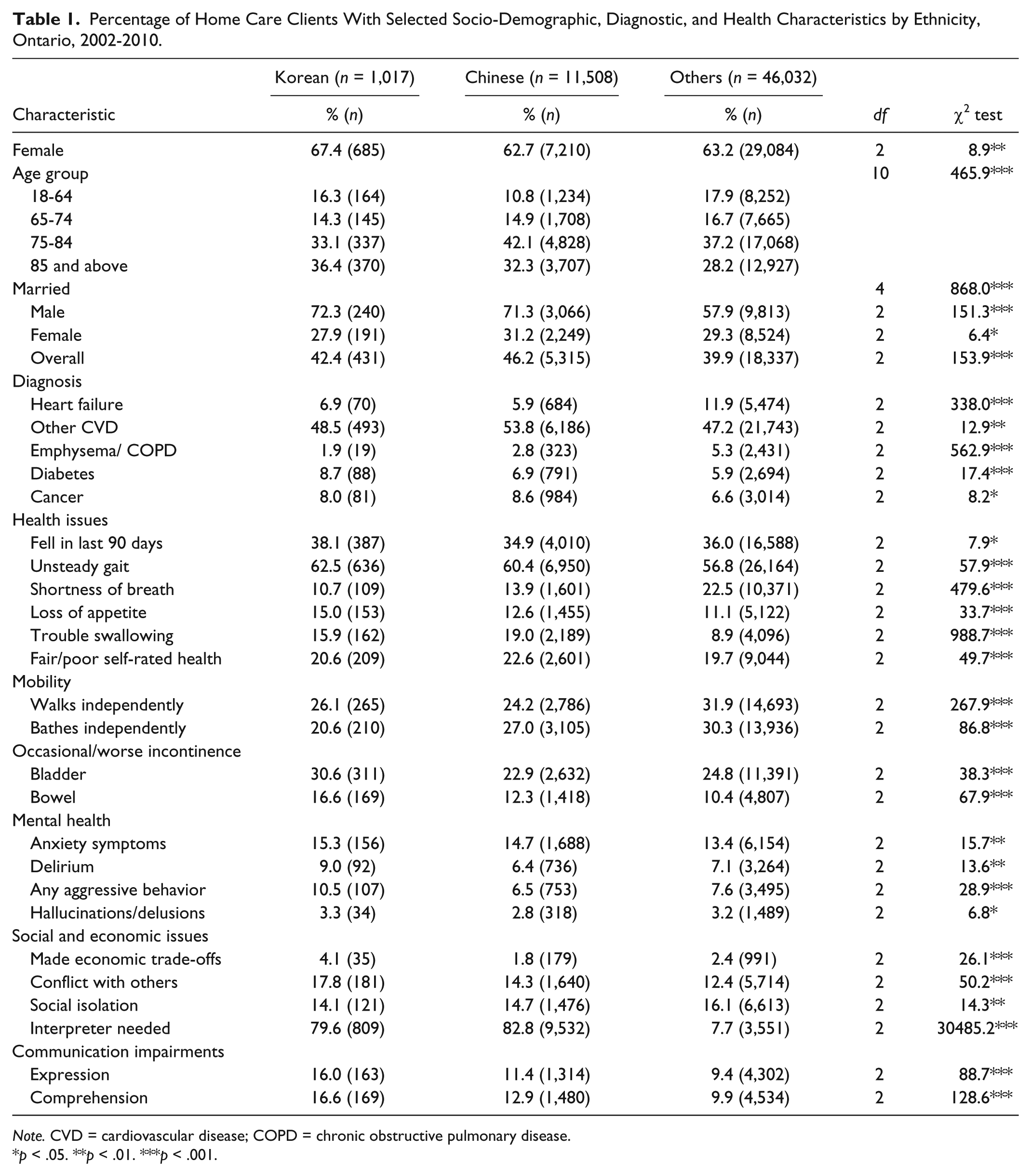
Note. CVD = cardiovascular disease; COPD = chronic obstructive pulmonary disease.
p < .05. **p < .01. ***p < .001.
Percentage Distribution of Selected Informal Caregiving Variables by Ethnicity, Ontario, 2002-2010.

p < .05. **p < .01. ***p < .001.
Distribution of Clinical Scale Scores Among Ethnicity, Ontario, 2002-2010.

Note. ADL = Activities of Daily Living; CHESS = Changes in Health, End-stage disease and Signs and Symptoms; IADL = Instrumental Activities of Daily Living; MAPLe = Method for Assigning Priority Levels.
p < .05. **p < .01. ***p < .001.
Percentage of Home Care Clients Receiving Selected Resources, Health Services, and Interventions by Ethnicity, Ontario, 2002-2010.
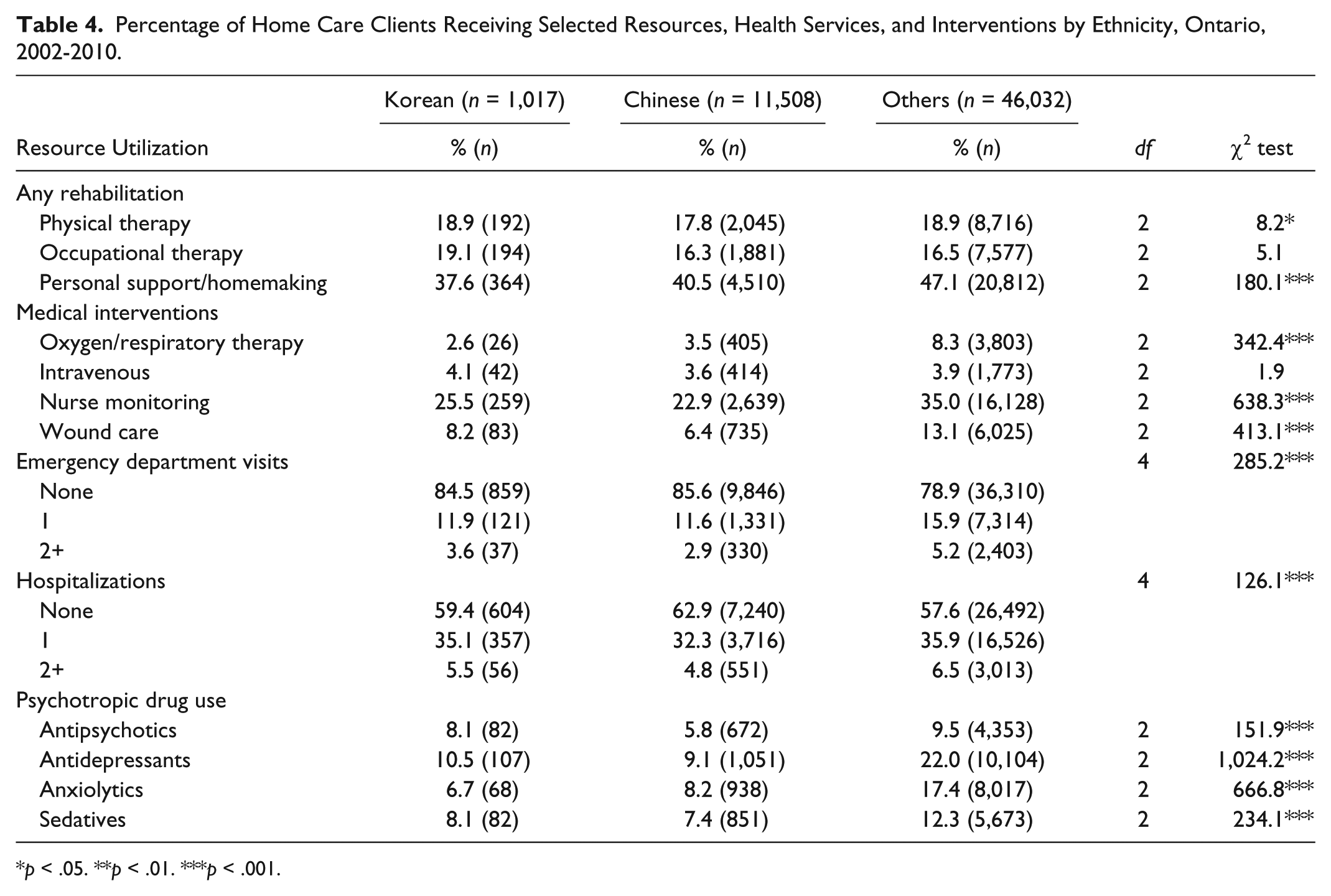
p < .05. **p < .01. ***p < .001.
Alternative Multiple Logistic Regression Models for the Effects of Ethnicity and Interpreter Needed on Caregiver Distress, Ontario, 2002-2010.

Note. MAPLe = Method for Assigning Priority Levels; OR = odds ratio; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
To investigate the risk factors for caregiver distress, crude and adjusted odds ratios (OR) and their 95% confidence intervals (CI) for caregiver distress were obtained from multiple logistic regression models. Summary scales were treated as continuous variables when tested in models. All statistical analyses were performed using SAS software (Version 9.4).
Results
Table 1 shows the percentage of home care clients with selected socio-demographic, diagnostic, and health characteristics by language group. In this and subsequent tables, the large sample sizes result in relatively modest differences being statistically significant, although they may sometimes not be clinically significant. Therefore, the emphasis here is placed on the larger differences that are clinically significant and have relevance for policy or clinical practice. In terms of overall characteristics, the Korean Canadians, Chinese Canadians, and other Canadian home care clients had a comparable age distribution. However, Korean Canadian clients had a somewhat higher percentage of women, and Korean Canadian and Chinese Canadian males were substantially more likely to be married than other male home care clients. The distributions of medical diagnoses were relatively comparable across the three groups, except Korean Canadian and Chinese Canadian clients had notably lower rates of heart failure than other clients. On the other hand, Chinese Canadian clients had the highest rates of other cardiovascular diseases (53.8%, p < .01). Korean Canadian clients had slightly higher rates of falls in last 90 days (38.1%, p < .05) and higher rates of unsteady gait (62.5%, p < .001) compared with the other groups. In addition, Korean Canadian and Chinese Canadian clients were less likely to walk or bathe independently compared with other clients. Loss of appetite (15%, p < .001) was most common in the Korean Canadian clients, and trouble swallowing was about double the rate in Korean Canadians (15.9%) and Chinese Canadians (19%) compared with other home care clients (8.9%, p < 0.001). Moreover, Korean Canadian clients had the highest rates of mental health symptoms such as anxiety symptoms, delirium, any aggressive behavior, and hallucinations or delusions. The rates of expressive and receptive deficits in communication were also highest in Korean Canadian clients.
Three indicators were used to assess social variables: “Made economic trade-offs,” “Conflict with others,” and “Social isolation.” Korean Canadian clients were about twice as likely to make economic trade-offs among purchasing food, medication, housing, and necessary medical care compared with the other two groups. In addition, rates of social isolation were comparable among the three groups, but “conflict with others” was most common in the Korean Canadian clients. The most dramatic difference across groups was the need for translation, where about 80% of Korean Canadians and Chinese Canadians needed an interpreter compared with only 8% of other home care clients (p < .0001).
Table 2 provides the distribution of selected informal caregiving variables by language group. The rates of caregiver distress were highest in the Korean Canadian clients (25.9%) and lowest in the other clients (17.3%, p < .001). Korean Canadians and Chinese Canadians were much less likely to live alone or to live only with their spouse compared with other clients. On the other hand, both minority groups were about twice as likely as other home care clients to either “live with their spouse and child” or “live with their child only.” Similarly, Korean Canadian and Chinese Canadian clients were also much more likely to live with their primary and secondary caregivers than other clients. Both the primary and secondary caregivers were more likely to be a child than in other home care clients; however, they were also substantially less likely to have caregivers who were other relatives or friend/neighbors.
Table 3 provides the distribution of various clinical algorithms and scale scores by ethnicity. Although the three groups had similar distributions for pain, health instability (measured by the CHESS Scale), and depressive symptoms, there were clear differences with respect to cognitive and functional status. Korean Canadian clients had the highest percentage with a CPS score greater than 3 (20.7%, p < .001), indicating a moderate or worse impairment in cognition. With respect to ADL impairment, they had about twice the proportion of moderate or worse functional status compared with other home care clients (about 18% compared with 10%, respectively, p < .001). Similarly, Korean Canadian and Chinese Canadian home care clients’ IADL capacity scale scores indicated higher rates of impairment in instrumental activities than other clients. These differences are also reflected in the MAPLe algorithm, which is a composite measure combining factors such as ADL impairment, cognition, falls, IADL, and behavior. Korean Canadians had the largest proportion in the two highest MAPLe categories (43.4%, p < .001) compared with Chinese Canadian and other clients.
Table 4 provides the percentage of home care clients receiving selected health services and clinical interventions by ethnicity. A somewhat higher percentage of Korean Canadian clients received occupational therapy (19.1%, p < .05), but they were less likely to receive personal support or homemaking services (37.6%, p < .001) compared with Chinese Canadian and other clients. There were only modest differences between groups in emergency visits and hospitalizations; however, Korean Canadian and Chinese Canadian clients were much less likely to receive medical interventions such as oxygen therapy, nurse monitoring, and wound care. In addition, both groups had a much lower rate of use of psychotropic medications (except antipsychotics) than other home care clients.
Table 5 presents the results for various multiple logistic regression models investigating the associations of ethnicity and the need for an interpreter with caregiver distress. The models also adjust for other factors that may be associated with caregiver distress including MAPLe, age, sex, marital status, and receipt of personal support services. When their main effects are considered alone, the language variable was significantly associated with caregiver distress with or without the adjustments for other covariates (Korean Canadian unadjusted OR = 1.67, 95% CI = [1.45, 1.93]; adjusted OR = 1.40, 95% CI = [1.19, 1.64]; Chinese Canadian unadjusted OR = 1.45, 95% CI = [1.38, 1.52]; adjusted OR = 1.28, 95% CI = [1.22, 1.36]). When the reference group was changed to be Chinese Canadians rather than the general home care population, the CI for Korean Canadian clients overlapped with 1.00 slightly, and the p value was .07, indicating that the difference between the two Asian groups did not quite meet the 0.05 level of significance, although both clearly had higher rates of distress than the general home care population.
The need for an interpreter was also significantly associated with caregiver distress with or without adjustments for other covariates (unadjusted OR = 1.67, 95% CI = [1.60, 1.75]; adjusted OR = 1.41, 95% CI = [1.34, 1.48]). However, when both variables were introduced as covariates in the caregiver distress model, the language variable was no longer significant but the interpreter needed variable remained significant (unadjusted OR = 1.69, 95% CI = [1.58, 1.80]; adjusted OR = 1.40, 95% CI = [1.30, 1.51]). Language barriers were significant irrespective of order of entry to the model, and statistical tests of collinearity indicated that this was not a major concern for these variables. Indeed, given that ethnicity and need for an interpreter are not indicators of the same underlying concept, they should not be considered to be multicollinear items.
The analysis shows that it is the language barrier and not “Chinese-ness or Korean-ness” that is a key factor associated with caregiver distress. Interactions between ethnicity and the need for an interpreter were also tested. These interactions were found to be significant, and the adjusted ORs are shown in Figure 1. For all three different ethnic clients, the need for an interpreter was associated with a higher level of caregiver distress. For those who do not need an interpreter, Korean Canadian clients had somewhat lower odds of distress and Chinese Canadians had higher odds of distress compared with the general population of home care clients. On the other hand, the odds of caregiver distress were highest among Korean Canadian clients requiring an interpreter.
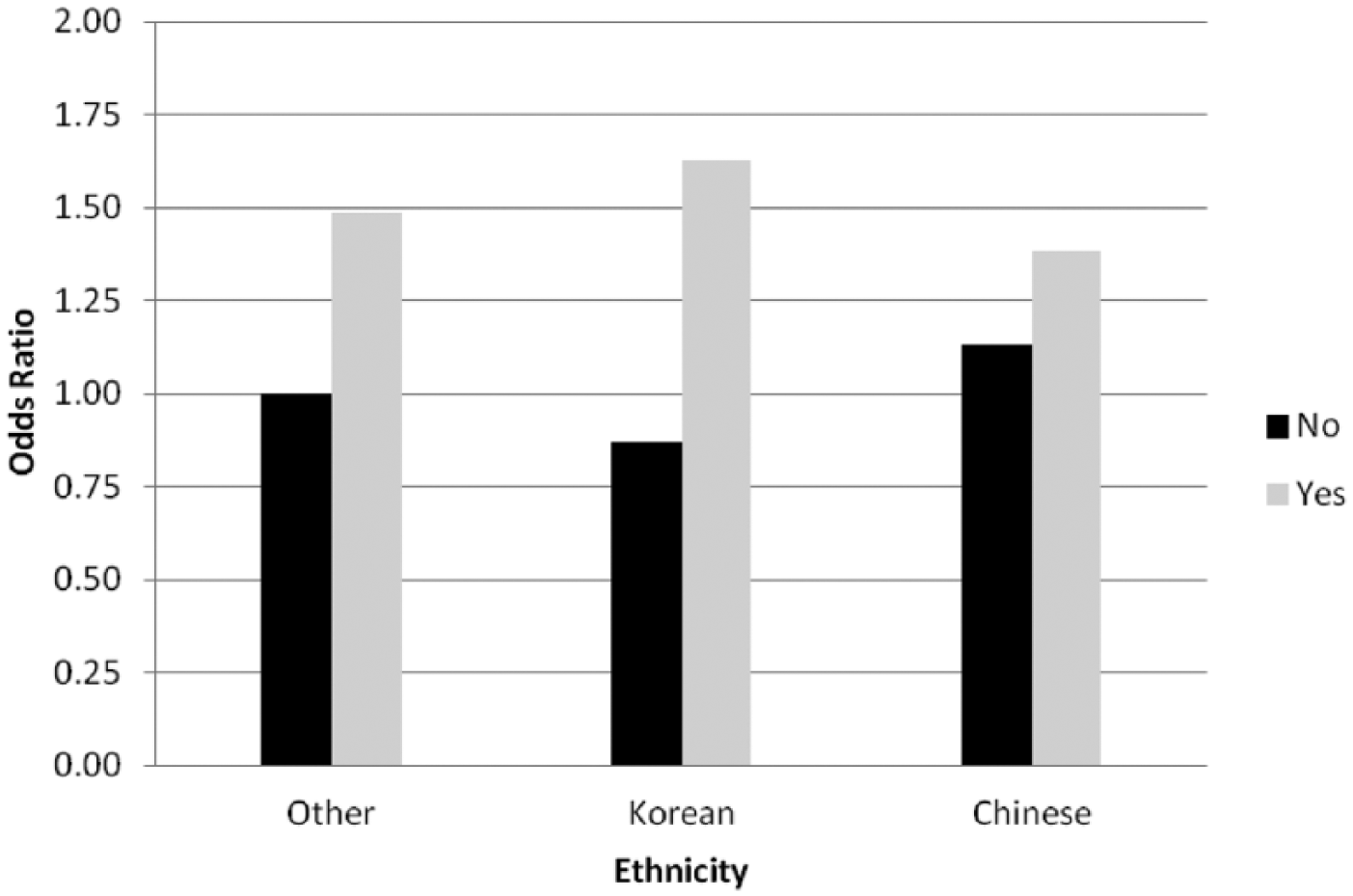
Adjusted odd ratios for caregiver distress by ethnicity and need for an interpreter (Yes/No), Ontario, 2002-2010.
Figure 2 shows the rates of caregiver distress by MAPLe priority levels and cultural groups. For all three groups, MAPLe is clearly associated with an increased rate of caregiver distress. In addition, the rates of distress are higher within MAPLe levels for the Korean Canadian and Chinese Canadian clients, but they do not appear to differ substantially from each other (although both have higher rates within MAPLe levels than their counterparts in the general population).

Percentage of home care clients with a distressed caregiver by ethnicity and MAPLe level, Ontario, 2002-2010.
Discussion
An important finding of the present study is that Korean Canadian clients had higher levels of need for home care services based on indicators such as falls, unsteady gait, mobility impairment, incontinence, and mental health symptoms. Korean Canadian clients also had a higher incidence of major chronic diseases, including diabetes, cancer, and other cardiovascular diseases. They also had notably higher levels of functional and cognitive impairments than other home care clients. Despite their higher need for support services, Korean Canadians were less likely to receive personal supports/homemaking and home nursing. These results suggest the possibility that they begin to receive help from formal services too late, and consequently, their caregivers experience high levels of distress. It is also clear that language barriers are a major risk factor to elevated distress in both cultural groups examined here.
As one might expect based on Confucian values, higher percentages of children took care of and lived with the Korean Canadian and Chinese Canadian clients compared with the general home care population. These living arrangements may have allowed for the exchange of intergenerational support (e.g., grandparents may have provided child care in the home to allow both parents to work). Prior support by grandparents may therefore be repaid by assistance from their children as they become frailer in later life. However, with increased female labor force participation, it may be stressful for employed adult children in multigenerational households to provide care to both their children and elderly parents.
Korean Canadian and Chinese Canadian clients were less likely to have emergency visits and hospitalizations. These lower rates may mean that they are being managed well at home. On the other hand, these findings may also demonstrate the stoicism that delays seeking help for pain or discomfort caused by health conditions. It is also possible that Eastern medicines and therapies might be used instead of conventional health care services. Finally, some elders may avoid visits to emergency departments because of language barriers that discourage the service use.
It is also clear from this study that there were high rates of informal caregiver distress in these groups, indicating that these caregivers are not impervious to the challenges of supporting relatives with heavy care needs. Korean Canadian clients had the highest unadjusted rate of caregiver distress among these ethnic clients, a finding that is consistent with those reported by other studies (E. E. Lee & Farran, 2004). This difference was due, at least in part, to the substantially higher levels of impairments evident in the Korean Canadian clients. However, compared with the general population, rates of caregiver distress were higher in both cultural groups after adjusting for need and socio-demographic factors.
The present results also point to the critical importance of language barriers for home care clients and their caregivers. Other studies have reported that language barriers were the most frequently experienced and the most common adaptation difficulties among immigrants (Koh & Bell, 1987; Mui, 1996; Wong, Yoo, & Stewart, 2005). The present results demonstrate that these difficulties carry over to the experience of informal caregivers. In fact, the multivariable logistic regression analyses indicated that the significance of ethnic differences disappears when the need for an interpreter is included. Thus, targeting language barriers can be a start in reducing distress experienced by home care clients and caregivers from cultural minorities. However, if these needs are not properly met or managed, they can lead to social isolations and other barriers in living in the community. Consequently, addressing language issues is a fundamental requirement for any home care agency serving clients in a multicultural society.
One of the objectives of this study was to investigate the risk factors for caregiver distress of families caring for the elderly members. After controlling for clinical indicators of need, the main risk factor that affected caregiver distress was the need for an interpreter for the clients. Lack of language support such as translation services can be discriminatory to minority groups who do not speak the official language of the dominant culture. The failure of government to provide such services can exacerbate health outcomes in these populations (Woloshin, Bickell, Schwartz, Gany, & Welch, 1995). Language barriers can influence understanding and absorption of information leading to social isolation and causing psychosocial distress and health declines in the elderly individuals who immigrated later in life (Colenda & Smith, 1993; M. S. Lee, 1989; Lai & Surood, 2010; Mui, 2001). Moreover, language barriers impair social function, a problem that may in turn lower self-esteem, a sense of security and control, access to important information, ability to make friends, and participate in the community (Antle, 2004).
The findings related to the MAPLe algorithm are also of interest because they demonstrate that it continues to be a predictor of caregiver distress within cultural groups. Therefore, home care agencies serving diverse populations may be reassured that the algorithm indicates need for services to be provided in a manner that is not culturally constrained. The higher levels of distress within MAPLe levels among Korean Canadian and Chinese Canadian clients were no longer significant after adjusting for the need for an interpreter. This suggests that home care agencies should provide services that target the dimensions of need operationalized by the MAPLe algorithm, and they must do so in a manner that is sensitive to cultural and linguistic considerations.
For multicultural societies, it is essential to account for linguistic diversity as part of health and social service delivery. Cultural competence should be a basic requirement for home care workers and other health care providers, but practical provisions to deal with language barriers are also fundamental considerations. Language barriers may pose important problems for issues such as health literacy, awareness of service options, self-determination, self-esteem, and compliance with treatment regimens (Damron-Rodriguez, Wallace, & Kington, 1995; Woloshin et al., 1995).
Finally, it is important to underline that language barriers are important considerations not only for Korean Canadian and Chinese Canadian clients, but also for other linguistic minorities. The increased distress associated with the need for an interpreter was also evident within the comparison group of other home care clients. Hence, this is not a problem unique to Canadians of Asian origin. However, there are only a limited number of governmental language training programs that target older immigrants in Canada (Immigrant Settlement & Integration Services, 2010). Thus, governments should provide supports to reach out to isolated minority populations of older adults to prevent further deterioration of their health, enhance their quality of life, and support caregivers, making a valuable social and economic contribution to society.
Limitations
The cross-sectional nature of the data set used here limits one’s ability to make causal inferences in these findings, but the multidimensional nature of the RAI-HC assessment permitted adjustments for many different potential confounders. Second, there may be errors involved in the ascertainment of clinical characteristics such as depressive symptoms or caregiver distress, which in turn may have weakened some associations of interest. However, Chi (2011) argued that the interRAI instruments are well-suited for cross-cultural assessment of the needs of older adults. Third, fluency in other languages was not considered because only the primary language was assessed in the RAI-HC. Fourth, the ascertainment of caregiver distress was a binary variable, so the subjective severity of the distress cannot be determined beyond its presence or absence. However, other articles have used the same variable to examine caregiver distress (Hirdes, Freeman, Smith, & Stolee, 2012; Hirdes, Poss, & Curtin-Telegdi, 2008). Fifth, the immigrant sample being investigated involved only those who were part of long-stay home care programs. Thus, the results may not be generalizable to community-dwelling Korean Canadian and Chinese Canadian older adults not receiving formal home care services.
Despite these limitations, the present study suggests that Korean Canadian home care clients have higher impairments, but receive fewer services than other clients. Korean Canadians are one of the most rapidly increasing immigrant populations in Canada. Therefore, the need to respond to the systematic barriers identified here will likely grow over time.
Footnotes
Acknowledgements
J. H. holds the Home Care Research and Knowledge Exchange Chair funded by the Ontario Ministry of Health and Long-Term Care.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.