
Abstract
The objective of the present study was to investigate the difference in the level of self-esteem among patients with psychiatric disorders and normal controls. After a detailed literature review, it was hypothesized that there would be a significant difference in the level of self-esteem among patients with psychiatric disorders and normal controls. The sample of the present study consisted of 260 participants, who were further divided into two groups: clinical group (n = 140) and normal controls (n = 120). The age range of the participants in both the samples were 18 to 25 years (with the mean age of 22.14 years for psychiatric patients and 21.18 years for normal controls), and they belonged to middle socioeconomic status. The clinical group consisted of diagnosed psychiatric patients according to Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR) criteria and further divided into four subgroups, including patients of (a) schizophrenia (n = 40), (b) major depressive disorder (n = 40), (c) obsessive-compulsive disorder (n = 40), and (d) opioid dependence disorder (n = 20). The semi-structured interview form of Institute of Clinical Psychology, University of Karachi, and Rosenberg Self-Esteem Scale were used. Descriptive Statistics and one-way ANOVA were applied to analyze and interpret the data in statistical terminology. Results indicate significant differences among patients with psychiatric disorders and normal controls on the variable of self-esteem (F = 30.513, df = 4, 255, p< .05). The finding has implications for clinical interventions and also suggests avenues for future research.
Introduction
Self-esteem is defined as the individual’s assessment of self-worth (Rosenberg, 1965) and is affected both by our ideas about how we are measuring up to our own standards (i.e., primarily internal) and by our ability to control our sense of self in interactions with others (i.e., primarily external); both these processes have important repercussions on our feelings about ourselves (Bordens & Horowitz, 2008). People with high self-esteem regard themselves highly and are generally pleased with who they are (Bordens & Horowitz, 2008). They tend to have positive, well-anchored, and secure feelings of self-worth and are satisfied with themselves (Kernis, 2000). They are better at making new friends, at communicating about themselves, at providing emotional support to others, and at resolving interpersonal conflicts (Buhrmester, Furman, Wittenberg, & Reis, 1988). In contrast, feelings of failure, incompetence, and worthlessness are common characteristics of people with low self-esteem (Bordens & Horowitz, 2008). People with low self-esteem evaluate themselves negatively, which increases the proneness toward feelings of being weak, helpless, hopeless, frightened, vulnerable, fragile, incomplete, worthless, and inadequate. Consciously or unconsciously low self-esteem causes patients or others to hate and reject themselves, which may be expressed in direct or indirect ways (Stuart & Sundeen, 1987).
The past few decades have seen an increase in the research on self-esteem deficits and their debilitating effects among psychiatric patients. Research on self-esteem deficit and its paralyzing effects among psychiatric populations has already provided a great deal of insight into this phenomenon. According to O’Brien, Bartoletti, and Leitzel (2006), among patients with psychiatric disorders or mental illnesses, low self-esteem is either a diagnostic criterion or an associated feature of nearly two dozen mental disorders in Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000). Research evidence recognizes low self-esteem to occur in several psychiatric disorders, particularly major depressive disorders, dysthymic disorder, anxiety disorders, eating disorders, sexual dysfunction, and personality disorders (Leary & MacDonald, 2003), schizophrenia (Lysaker, Roe, & Yanos, 2007; Gureje, Harvey, & Herrman, 2004), obsessive-compulsive disorder (Fava, Savron, Rafanelli, Grandi, & Canestrari, 1996; Stumpf & Parker, 2000), and opioid dependence disorder (Frances & Franklin, 1988) in young adults. This fundamental importance of self-esteem in the course of various disorders is still inviting the attention of researchers due to its significance and implications.
There is also a controversy that swirls around the relative impact of self-esteem and psychiatric illnesses on each other. Some researchers argue that self-esteem deficit makes individuals vulnerable to psychiatric illnesses (see Khanam, Rizwan, & Bilal, 2008), and some suggest that psychiatric illnesses lessen one’s level of self-esteem (see Steinhausen, 2005), while others argue that there is a vicious cycle between low self-esteem and psychiatric illnesses (see Silverstone & Salsali, 2003). The present study is an effort to highlight the relative presence of self-esteem deficits in psychiatric patients compared with normal controls. This comparative analysis is not only limited to a specific diagnostic classification and its controls; instead, it considers a number of diagnostic groups under this analysis, which adds to its significance and makes it distinctive to previous studies. The inclusion of multiple groups (i.e., participants from patients of schizophrenia, major depressive disorder, obsessive-compulsive disorder, and opioid dependence disorder) not only makes the study sample more representative of the psychiatric population, but also makes intergroup comparisons possible, which add to the study’s credibility. On the basis of literature, it was hypothesized that there would be a significant difference in the level of self-esteem among patients with psychiatric disorders and normal controls.
Method
Sample
The sample of this study consisted of 260 participants, including (a) clinical group, and (b) normal controls group (For demographics see Table 3 & 4). The clinical group consisted of 140 participants, who had been taking treatment for their mental health problems from outpatient clinics of different psychiatric and psychological settings within urban areas of Karachi, Pakistan. They were diagnosed psychiatric patients according to DSM-IV-TR; APA, 2000) criteria, including patients of (a) schizophrenia (n = 40), (b) major depressive disorder (n = 40), (c) obsessive-compulsive disorder (n = 40), and (d) opioid dependence disorder (n = 20). The participants of the opioid dependence disorder group were comprised of males only because of the unavailability of females with opioid dependence disorder in outpatient clinical setups in Karachi.
Normal controls consisted of 120 participants who themselves or their first-degree relatives had never experienced any kind of psychological problem that demanded clinical attention or consultancy from mental health professionals. Participants for the control group were drawn from different institutions and organizations in Karachi.
The ages of the participants in both samples ranged from 18 to 25 years, with a mean age of 22 years for psychiatric patients and 21 years for normal controls (see Table 1 & 2). The entire sample was drawn from the middle socioeconomic class, and the minimum education level was Middle (eighth grade).
Measures
Semi-structured interview form
The semi-structured interview form is a qualitative tool designed by the Institute of Clinical Psychology (ICP), University of Karachi, to use in Out patient Department(OPD). It consisted of items focusing on an individual’s demographic information, presenting problems, history of problem, medical history, family history, educational history, social and occupational history, recreational activities, sexual history, mental state examination, extrasensory perceptions, belief system, affective state, anxieties, gender identity problems, psychosomatic complaints, addiction problems, family psychopathology, personality traits, motivation, and behavior during interview. It is not a standardized measure, but a practice tool to get qualitative information from patients, and it usually takes 20 to 30 minutes to be administered.
Rosenberg Self-Esteem Scale (RSES)
The RSES (Rosenberg, 1965) is a 10-item scale that was originally designed to measure global self-esteem. It uses the 4-point Likert-type response format: strongly agree, agree, disagree, and strongly disagree. The scores can range from 0 to 30, with the higher scores indicating a high level of self-esteem and lower scores indicating a low level of self-esteem. In the present study, a translated version (in Urdu) of the RSES (Sardar, 1998) was used. Cronbach’s alpha was found to be .71 for the clinical sample and .75 for the normal controls, which indicates adequate internal consistency of the Urdu RSES.
Research procedure
This research was conducted after approval of research review board in ICP, University of Karachi. The sample for the clinical group was recruited from different psychiatric departments and mental health clinics within urban areas of Karachi. A letter of consent describing the research project was provided to authorities of selected organizations. After getting permission from authorities, the psychiatric patients were approached individually with the help of their respective psychiatrists and psychologists who had already been treating them. The initial few minutes were spent putting the patients at ease, and then the purpose of the study was briefed and discussed in very general terms. The researcher assured the confidentiality of the participant’s personal information and responses. The formal consent was taken from patients through a consent form, and only those patients who gave consent to participate were included in the sample. First, the researcher conducted a detailed diagnostic interview and recorded all necessary information about each participant’s illness on the Semi-Structured Interview Form, which was utilized to confirm the diagnosis made by the respective psychiatrist/psychologist according to the diagnostic criteria of DSM-IV-TR(APA, 2000). The participants’ final diagnosis was determined by a consensus meeting between the researcher, respective psychiatrist/psychologist, and an expert clinician’s opinion.
Finally, the RSES was administered to assess the psychiatric patients’ level of self-esteem. Participants were allowed to ask questions if they had any difficulty in following instructions and understanding the statements. At the end of the administration of research measures, psychiatric patients and concerned authorities were thanked for their cooperation and time.
The sample for normal controls was drawn from different institutions and organizations in Karachi. The same procedure that was applied to the clinical group was followed for the normal controls. They were individually interviewed to assess them as controls for the study (e.g., age, marital status, education), and they were requested to respond on the RSES. During the process of study, the researcher adhered to four key ethical principles: respect for the person’s rights and dignity, responsibility, and integrity.
Statistical analysis
After scoring, the research data were analyzed to interpret them in statistical terminology. Data were initially compiled into a Microsoft Excel spreadsheet and then analyzed on Statistical Package for Social Sciences (SPSS, V-13.0) software. To test the hypotheses of the present study, one-way ANOVA was computed.
Results
Descriptive Statistics for Age of Clinical Group and Normal Controls.

Note. This table indicates the mean scores and standard deviations for age of male and female participants belonging to both clinical group and normal controls.
Descriptive Statistics for Age of Various Subgroups Within Clinical Group.

Note. This table indicates the mean scores and standard deviations for age of male and female participants belonging to all clinical groups. MDD = major depressive disorder; OCD = obsessive-compulsive disorder; ODD = opioid dependence disorder.
Summary of Demographic Characteristics of Clinical Group and Normal Controls.

Note. This table presents frequencies and percentages of both clinical and normal controls groups. The information is presented according to their gender, family structure, and marital status.
Summary of Demographic Characteristics of Subgroups Within Clinical Group.
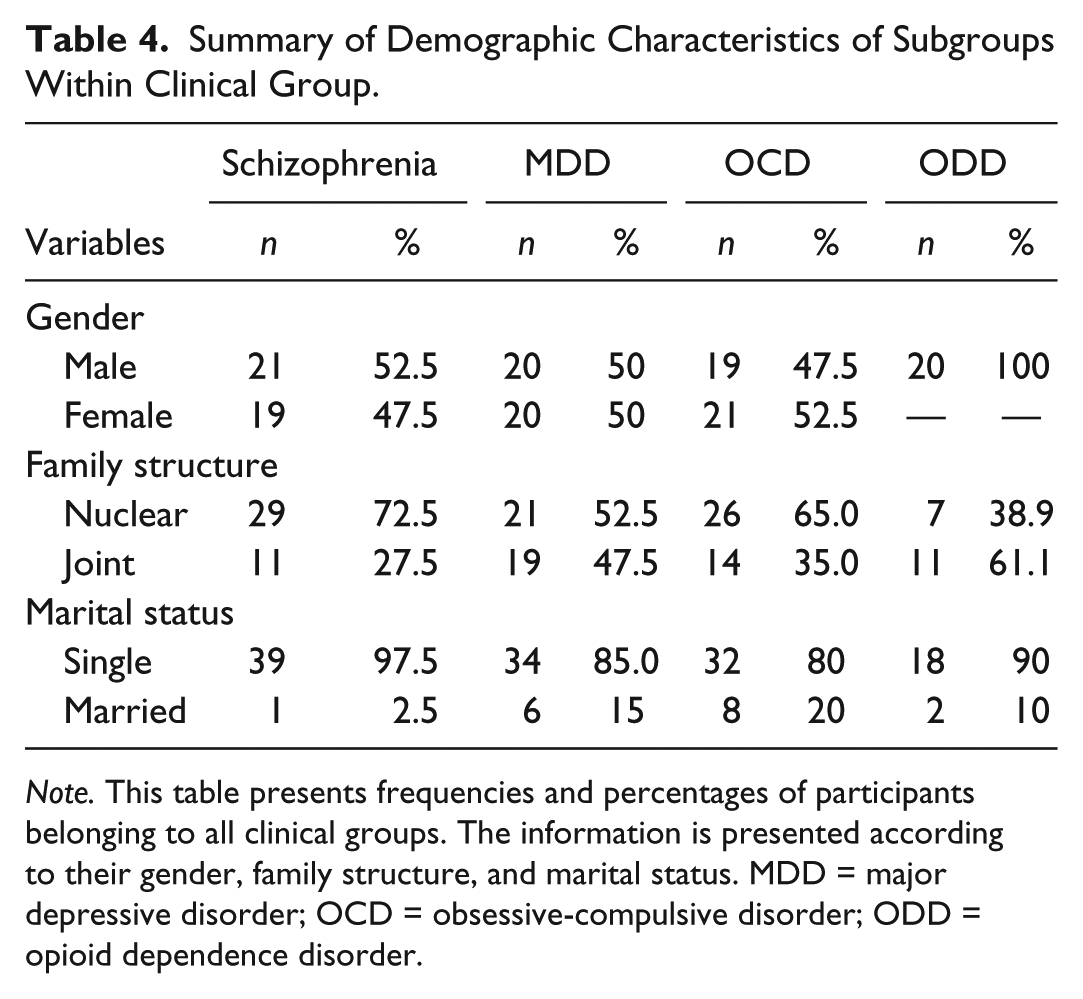
Note. This table presents frequencies and percentages of participants belonging to all clinical groups. The information is presented according to their gender, family structure, and marital status. MDD = major depressive disorder; OCD = obsessive-compulsive disorder; ODD = opioid dependence disorder.
Summary of ANOVA for the Variable of Self-Esteem Among Clinical Group and Normal Controls (N = 260).

Note. This table shows that the clinical group (patients of schizophrenia, major depressive disorder, obsessive-compulsive disorder, and opioid dependence disorder) scored significantly lower on the variable of self-esteem as compared with normal controls (F = 30.513, df = 4, 255, p< .05).
Post Hoc Tukey’s HSD Analysis Among Normal Controls and Various Subgroups of Clinical Group for Self-Esteem.
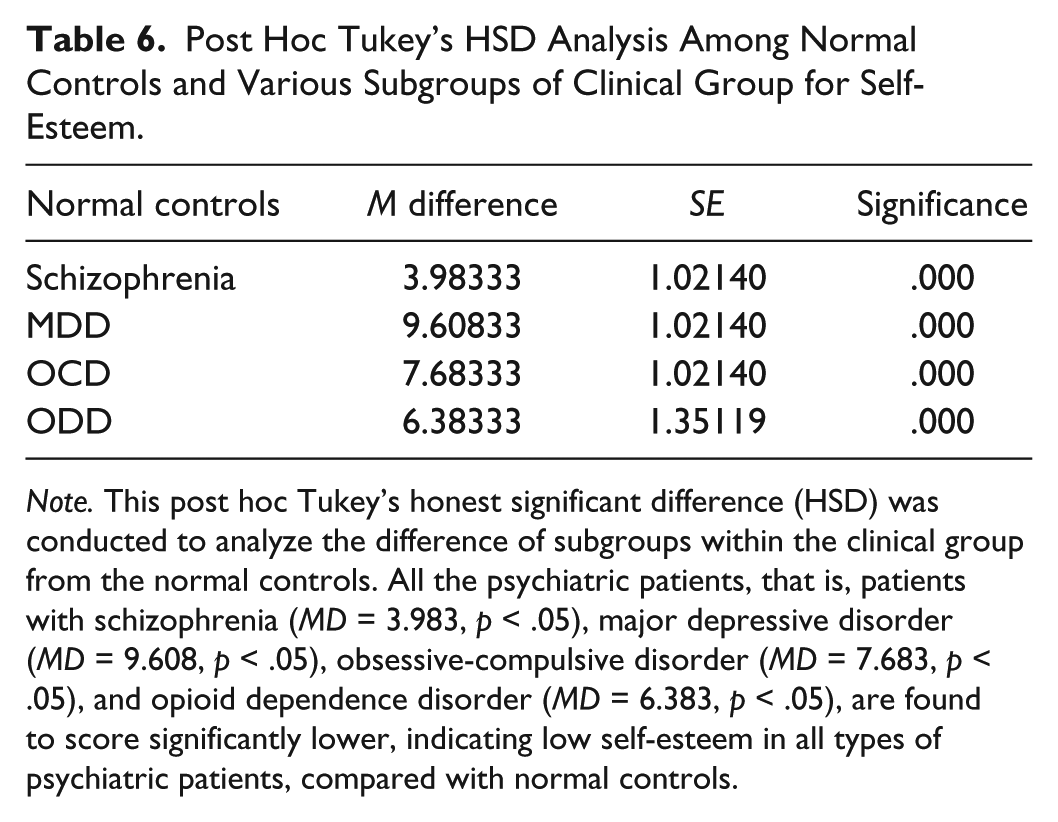
Note. This post hoc Tukey’s honest significant difference (HSD) was conducted to analyze the difference of subgroups within the clinical group from the normal controls. All the psychiatric patients, that is, patients with schizophrenia (MD = 3.983, p < .05), major depressive disorder (MD = 9.608, p < .05), obsessive-compulsive disorder (MD = 7.683, p < .05), and opioid dependence disorder (MD = 6.383, p < .05), are found to score significantly lower, indicating low self-esteem in all types of psychiatric patients, compared with normal controls.
Discussion
As we hypothesized that “there would be a significant difference in the level of self-esteem among patients with psychiatric disorders and normal controls,” the results from a statistical analysis of the data show that the clinical group (patients of schizophrenia, major depressive disorder, obsessive-compulsive disorder, and opioid dependence disorder) scored significantly lower on the variable of self-esteem as compared with normal controls (F = 30.513, df = 4, 255, p < .05;Table 5). These findings are consistent with the formulated hypothesis and validate the previous studies (e.g., Butler, Hokanson, & Flynn, 1994; Ehntholt, Salkovskis, & Rimes, 1999; Gureje et al., 2004; Hansson et al., 1999; Rashid, 2007; Roe, 2003; Salsali & Silverstone, 2003; Silverstone & Salsali 2003) that have reported low levels of self-esteem in psychiatric patients compared with normal controls. Furthermore, post hoc Tukey’s honest significant difference (HSD) test was conducted to analyze the difference of subgroups within the clinical group from normal controls (Table 6). All the psychiatric patients, that is, patients of schizophrenia (MD = 3.983, p< .05), major depressive disorder (MD = 9.608, p< .05), obsessive-compulsive disorder (MD = 7.683, p< .05), and opioid dependence disorder (MD = 6.383, p < .05), are found to score significantly lower, indicating low self-esteem in all types of psychiatric patients, compared with normal controls in this study.
The value we assign to ourselves is generally based on five factors—two physical and three psychological. The physical factors that determine our self-esteem are our appearance (the way we look) and our physical abilities. The psychological determinants of self-esteem are how well we do (our perceived intelligence), how confident we are in social situations, and how we regard ourselves (Rice, 1987). However, Strickland (2001) described that psychologists who write about self-esteem generally discuss it in terms of two key components: the feeling of being loved or lovable and accepted by others and a sense of competence and mastery in performing tasks and solving problems independently. In psychiatric patients, generally both components (i.e., feeling of being loved or lovable and accepted by others) are impaired and manifest as deficiency of self-esteem. As Berk, Macneil, Castle, and Berk (2008) described, that insight into reality that one has a severe mental illness may be associated with a fall in self-esteem and demoralization. He further extended that diagnosis by saying that denial may be a way of protecting oneself from the cognitive dissonance experienced when trying to integrate the idea of a stigmatized illness with one’s usual self-concept. This might also be a reason for patients with psychiatric disorders to, when they become aware of their illness, spontaneously respond to their illness with denial; and that when they accept their illness, they become prone to negatively evaluate themselves. As Sanyal (2008) suggested, psychiatric patients can believe that they are less smart than other people, and this can adversely affect their self-esteem and reinforce isolation. In this way, people with psychiatric illnesses do not trust themselves; they view themselves as awful people who are poor in all aspects of life compared with others. They not only perceive that they lack confidence in themselves and their ability to control their lives but also that they are socially inapt. Thus, their psychiatric disorder limits their coping mechanisms, and impairs their problem-solving and decision-making skills. Consequently, they disregard themselves, and their self-esteem is further lowered.
Another reason for the low level of self-esteem among psychiatric patients as compared with normal controls is the role of stigmatization. Several researchers have put forward that in psychiatric patients, the stigmatization of suffering from a severe psychiatric disorder creates typical self-esteem–destructive ideas and low self-esteem (e.g., Berge & Ranney, 2005; Blankertz, 2001; Kahng & Mowbray, 2005; H. Stuart & Sartorius, 2005). Patients with psychiatric disorders are not generally accepted in society as well as by their families and are frequently criticized. They are usually labeled as insane, mad, mental, psycho, useless, burden, and so on, which leads to feelings of inadequacy, a general sense of worthlessness, and inferiority, which in turn contributes to a low level of self-esteem. Link and Phelan (1999) illustrated that the stigma of mental illness carries not only negative moral connotations (e.g., “lazy”) but also results in social marginalization, isolation, withdrawal, a devalued sense of self, and lower self-esteem for those diagnosed with a mental disorder. Lysaker, Tsai, Yanos, and Roe (2008) suggested that the experience of greater levels of stigma was generally related to poorer self-esteem. This could be further explained that the quality of feedback received by others significantly affects one’s level of self-esteem, as Leary et al. (2003) posited. They noted that approval and disapproval from environment clearly affects self-esteem. Sullivan (1953) also put forward that self-esteem is shaped by individuals’ appraisals of how they are perceived by significant others, and specifically that negative feedback is detrimental to self-esteem. Thus, culturally defined stigmas affect patients’ self-esteem by developing in them a sense of segregation and discrimination and inducing feelings of humility, worthlessness, and shame, which in turn may also adversely affect the course of their illness by causing further deterioration. The evidence obtained in this study points to the importance of self-esteem in planning the remedies and therapeutic interventions for those experiencing mental illness challenges.
This study has certain limitations. First, the sample consisted of young adult patients with middle socioeconomic status who fall into only four diagnostic categories, including schizophrenia, major depressive disorder, obsessive-compulsive disorder, and opioid dependence disorder, so that a generalization of the results to the entire psychiatric population is not applicable. The second limitation is the use of the subjective measure of Urdu self-esteem and an unstandardized semi-structured interview form. In Pakistan, both of these forms have never been tested for their psychometric characteristics. Future research should therefore utilize a sample from varied age groups and different diagnostic groups and should also focus on the biological, sociological, and psychological moderator or mediator mechanism underlying self-esteem changes following the onset of psychiatric illnesses.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.