
Abstract
Evidence does not support the use of restraint and seclusion (RS) to contain patients on psychiatric inpatient units, yet these practices continue to be used and defended. Use of RS often results in serious injuries to patients and psychiatric health care workers. Media exposure and legal challenges have led to negative opinions about RS but not their elimination. Substance Abuse and Mental Health Services Administration set a firm goal to permanently eliminate the use of RS, emphasizing that such practices are non-therapeutic. There is agreement that prevention is central to eliminating RS. The aims of this grounded theory study were to understand the contextual processes in preventing RS and the facilitators and barriers to prevention practice. Barriers include lack of resources at the micro-level, mismanaged messages at the institutional level, and, at the policy level, belief that all simply need a “change of heart.” Participants in this study did not think that they had adequate staffing, facilities, or education to prevent RS. Most were unaware of RS prevention policies.
The psychiatric literature is replete with experiences of persons who have been placed in restraints and seclusions on inpatient psychiatric units. Persons exposed to these practices express a range of negative responses from terror or rage, to feeling stripped of their humanity and overpowered (Hamrin, Iennaco, & Olsen, 2009; Kontio et al., 2012; Lebel, 2011; Shattell, Andes, & Thomas, 2008). There is no evidence that the use of restraint and seclusion (RS) offers an effective treatment strategy for psychiatric health care workers to manage persons hospitalized with severe mental illness (Muralidharan & Fenton, 2006). Sailas and Fenton (2012) conclude that no recommendation can be made about the effectiveness, benefit, or harmfulness of RS use based on randomized controlled studies, and the use of RS should be minimized because narrative studies have described adverse physical and psychological harm to patients and staff. Fatalities and serious injuries to patients and nursing staff continue to be attributed to the ongoing use of RS (Ferreira, 2010; Norwood et al., 2011). The human, institutional, and economic costs associated with RS are sizable and have not been adequately measured.
Literature Review
Definitions of RS use are imprecise and how interventions are translated into practice is not universally understood. Some classify RS as treatment failure, whereas others view RS as effective tools for averting injuries during crises and emergency situations (Geller & Glazer, 2012). These practices include various physical holds, leather straps, bed nets, restraint beds, and isolation rooms. The Centers for Medicare and Medicaid Services (2006) define restraint as “any manual method, physical or mechanical device, material, or equipment that immobilizes or reduces the ability of a patient to move his or her arms, legs, body, or head freely” and seclusion as the “involuntary confinement of a patient alone in a room or area which the patient is physically prevented from leaving” (p. 71380).
It was estimated that the U.S. Mental Health System spends more than US$375 million yearly on the consequences of conflict and containment on inpatient psychiatric settings (Flood, Bowers, & Parkin, 2008). As the cost of psychiatric care has shifted largely from the states to the jointly funded federal-state governmental program of Medicaid, the distribution of quality psychiatric care and inpatient work environments has not been adequately tracked or evaluated (Hanrahan, Aiken, McClaine, & Hanlon, 2010). States cut US$1.6 billion in non-Medicaid mental health spending from 2009 to 2011. As a result of these cuts, inpatient mental health care is shifting to community hospitals, which rely substantially on Medicaid for payment (Honberg, Diehl, Kimball, Gruttadaro, & Fitzpatrick, 2011). Tovino (2007) hypothesized that the use of RS originates in the wider, more global systemic problems of psychiatric care, finance, and treatment. Despite widespread interest in the phenomenon, knowledge deficits related to processes that produce change or reductions in RS use remain static. Translation of best practice has been slow, complicated by the complex and uncontrollable environmental variables inherent in RS use on inpatient psychiatric units (Johnson, 2010). Public policies play a critical, but often overlooked role in improving bedside practices and fidelity of public health interventions that lead to improved outcomes across all health care treatment settings (Mirvis, 2009). Ideally, inpatient psychiatric settings provide a safe, structured environment, and nursing care around the clock for persons who are in need of this level of treatment (Varcarolis, 2013).
Violence in health care is a serious international challenge, and in mental health settings violence is considered endemic (Lebel, 2011). Lebel (2011) characterizes violence as “the portal” to RS use, while, conversely, RS use contributes to workplace violence. This tri-directional cycle of violence occurs on the individual (practice), institutional (management), and regulatory (public policy) levels. Krug, Mercy, Dahlberg, and Zwi (2002) argue that violence prevention is within the realm of public health, not only because of the enormous effect violence has on health and health care services but also due to the roles public policy and regulation can play in mitigating the consequences. Social values influencing whether interpersonal violence is endorsed or frowned upon are expressed in the social and economic policies that preserve socioeconomic inequality and cultural norms, such as those associated with male dominance over women, parental dominance over children, and the acceptance of violence as a way to deal with conflict. For all types of violence, prevention efforts need to be tailored to social, cultural, and economic contexts (Krug et al., 2002). Institutional values play a key role in the ways in which psychiatric health care workers and patients treat one another interpersonally, and influence the everyday social norms and attitudes of the treatment environment.
Substance Abuse and Mental Health Services Administration (SAMHSA) set a firm goal to permanently eliminate the use of RS, emphasizing that such practices are non-therapeutic. Findings contained in a SAMHSA (2010) meta-analysis suggest that next step to implementing evidence-based best practices involves understanding the contextual factors that contribute to an organization’s capacity to implement prevention strategies. More recently, SAMHSA’s National Registry of Evidence-Based Programs and Practices determined that the clinical model called Six Core Strategies to Prevent Conflict and Violence: Reducing the Use of Seclusion and Restraint scored an overall rating of 2.8 on the readiness for implementation scale, reflecting a value just below being adequate for dissemination. Reviewers found the availability of implementation materials and availability of training and support resources to be lacking (Huckshorn, 2012). This study contributed to the RS prevention science by identifying contextual variables that modulate facilitators and barriers to RS prevention practices, and by discovering new gaps in the translation of national policy and evidence-based best practices.
Aims
The purpose of this grounded theory method (GTM; Charmaz, 2006) study was to understand the complex processes that psychiatric health care workers engage in to prevent the use of RS within the multidimensional context of the inpatient psychiatric unit. For this research, psychiatric health care workers were defined as registered nurses (RNs), licensed practical nurses (LPNs), nurse managers (NMs), medical doctors (MDs), nurse practitioners (NPs), mental health counselors (MHCs), administrators (ADMs), activity therapists (ATs), and policy makers (PMs). PMs with expertise in RS prevention were also included. Exploring processes involved in preventing the use of RS in the psychiatrically hospitalized population of the Southeastern United States from the standpoints of psychiatric health care workers, along with significant gray literature (information contained in government, academic, or business reports that lie outside the domains of published books and journals) and policy texts, provided information about a region that is mostly overlooked in the literature. Specific aims of this GTM study were to
understand contextual processes in preventing RS,
determine how resources are used or not in eliminating the use of RS,
explore the role of prevention policies, and
describe the facilitators and barriers to prevention practice.
For the science of RS prevention, SAMHSA (2010) identified understanding the contextual factors determining an organization’s capacity to implement effective strategies as a crucial next step toward elimination.
Method
Theoretical Framework
This study was founded on Bourdieu’s (1977) critical theory of practice. Bourdieu (1977) emphasizes that mastery of the symbolism of social interaction, and the language and actions of practical, everyday know-how, occurs through a continuous decoding of the perceived, but not consciously noticed rules and structures of everyday life and practice. Bourdieu’s (1977) dynamic heuristics of practice, habitus, and field directed the development of micro-, meso-, and macro-analysis. The study involved semi-structured interviews with 21 participants, and a specific grounded theory process used was that of (Bryant & Charmaz, 2007; Charmaz, 2006; Charmaz, 2011).
Human Subjects
Prior to recruitment, the study protocol was approved by the Institutional Review Board at the University of Tennessee, Knoxville, TN. Before each interview, elements of informed consent (IC) were explained and the participant’s level of understanding was assessed. After the oral explanation, participants read and signed the IC statement and received a copy. Data were collected from September 2011 through March 2012. There were no adverse events during the study related to rights of participants in research. Participants’ identities were protected and names were altered on all research data. Researchers and transcribers signed confidentiality forms.
Data Collection
The logic of GTM guided the system of data collection (Charmaz, 2006). For Charmaz (2005), consequences of knowledge made available and practices engaged in are “made real in collective and individual life” (p. 514). Participants from various health care professions, psychiatric facilities, and Southeastern states were sought to provide a rich data source. Interviews were conducted with ADMs, PMs, and frontline psychiatric care providers. Codes and categories emerged during the data gathering and concurrent analysis processes.
Interviews
Time and place were determined by the participant. Interviews were conducted in library rooms and other private areas, away from the inpatient environment to ensure confidentiality. Participants were not paid for the interview time itself but received a US$25 gift card. All psychiatric health care workers were required to have been employed by a psychiatric health care facility in the Southeastern United States within the past 5 years, as the regulations governing the use of RS in psychiatric hospitals in the United States were set forth by the Centers for Medicare and Medicaid Services (2006) in the Final Rule (42 Code of Federal Regulations [CFR] Part 482). Participants were asked to fill out a demographic form and a 16-item Life Events Checklist (LEC) following the interview. Interviews lasted 30 to 120 min and were audio recorded with permission, then transcribed verbatim.
Participants were asked, “Tell me about a time when you saw a patient who could potentially be restrained or secluded. What did you or other staff members do to prevent it?” Subsequent questions and discussion related to the use of resources, the awareness of prevention policies, and the facilitators and barriers to prevention practice.
Policies and laws at the state and national levels were examined to construct a more accurate account of the phenomenon and to interpret contextually how policies affect or do not affect practice. Categories of knowledge generated from the individual (micro), institutional (meso), and organizational (macro) standpoints were compared. Contrasted, deconstructed, and reconstructed meanings from interview data were also compared with gray literature.
LEC
Understanding potential traumatizing effects of staff exposure to RS is critical to prevention practice (Stromberg, 2012). The LEC is a 16-item screening tool consisting of items that ask about exposure to 16 different potentially traumatic events known to produce post-traumatic stress disorder or other post-traumatic problems. The mean kappa coefficient for all LEC items is 0.61, and the retest correlation at 1 week is r = .82 (Gray, Litz, Hsu, & Lombardo, 2004). The rationale for LEC use was the importance of traumatic exposure to RS use and the subsequent psychiatric health care workers’ effectiveness with patients, and the association between workplace violence and RS use. It was administered after the interviews.
Participants
The study participants included eight RNs, one LPN, one NM, one MD, two NPs, three MHCs, two ADMs, one AT, and two PMs. A total of 21 participants were interviewed from the states of Virginia, North Carolina, Florida, Tennessee, and the District of Columbia. The majority 81% were from Tennessee. Participants were recruited from community contacts, educational conferences, and professional organizations. Flyers were distributed and participants were contacted via phone and email.
Sixteen participants were female and five were male. The mean age was 47 years, ranging from 23 to 65 years. Seventeen were older than 35 years. One participant was African American. This was an educated group with 16 having earned at least a baccalaureate. Two had high school diplomas, one had a technical school certification, two had associate’s degrees, five had master’s degrees, and three held doctorates.
Data Analysis
Prior research showed that there were differing levels of awareness regarding how to successfully prevent and eliminate RS, and that prevention policies regulating RS use differ drastically among states and facilities. Data gathering and analysis focused on creating a theoretical representation of how psychiatric health care workers prevent and eliminate RS from various individual, institutional, and organizational standpoints. As data gathering and analysis continued, questions about policy and resources emerged. ADMs and PMs were recruited. According to Charmaz (2006), GTM works best when the grounded theorist collects and analyzes the data, ensuring that nuances of meaning, structure, and process are explored concurrently. Data analysis was ongoing with the assistance of the University of Tennessee (Knoxville), College of Nursing Grounded Theory Research Group.
Theoretical sampling at all phases aided clarification of categories and concepts (Charmaz, 2005). After completing five interviews, data were coded and analyzed (Charmaz, 2006). Participants offering a more diverse account of the phenomenon of RS prevention, such as those working in different types of health care organizations, were recruited. This data gathering led to a systematic exploration of RS prevention policies and how they are implemented by psychiatric health care workers from several institutions in a locale.
Theoretical sampling included the use of policy and regulatory texts, along with interviews of PMs at the state and federal levels. Theoretical sensitivity called for a more organic, emergent process of data collection. This heterogeneous sample improved the understanding of process categories from the individual (micro), institutional (meso), and organizational (macro) levels.
Categories related to RS prevention practice were developed. Coding included identification of the language of action related to the practice of RS prevention. As categories developed, focused coding was used to find the broader categories summarizing detailed processes described by participants. Many of these practice actions could not be explained without examining how they fit together with other categories (Saldana, 2009). The completed theory must give a concise understanding of a social world, confronting problems and processes within it (Charmaz, 2005). Trustworthiness improved via consulting the University of Tennessee (Knoxville) Phenomenology Research Group. The University of Tennessee (Knoxville) Grounded Theory Research Group assisted in the ongoing analysis process and helped determine data saturation. Constant comparison was used to explore categories as they related to individual, institutional, and organizational levels (Charmaz, 2006).
As collection and analysis progressed, policy implications at the state and federal levels were explored to interpret how policies affect or do not affect practice. Categories generated from individual (micro), institutional (meso), and organizational (macro) standpoints were developed systematically, and formed a theoretical analysis of the phenomenon that fit with Bourdieu’s theory of practice (Bourdieu, 1977). NVivo qualitative data analysis software, QSR International Pty Ltd. Version 9, 2010, was used to assist with organizing and coding the transcribed interviews and policy texts, as well as establishing an audit trail. Initial models for theory development and concept analysis were prepared using this program.
Findings
Findings are organized at the micro-, meso-, and macro-levels corresponding to Bourdieu’s triune analytics, arranged from individual, institutional, and organizational perspectives.
Micro
On an individual level, facilitators to prevention practice included personal characteristics such as being respectful, staying calm, and caring about patients. Barriers were conversely identified as being prideful, jumping the gun, and not understanding mental illness. The individual strengths identified by participants related to personal attributes of the staff included believing that RS prevention and elimination is possible, using humor and focusing on self. Individual weaknesses attributed to staff consisted of characteristics such as being burnt out, lacking patience, having no confidence or being fearful, and behaviors such as rigidly enforcing rules, being prideful, exhibiting intolerance, disrespecting patients, or insisting on maintaining control.
Knowing or not knowing what works
The established civil rights of psychiatrically hospitalized persons include the principle that patients have the right to experience the least restrictive means of treatment. On the surface, this concept appears straightforward. In practice, “distinguishing among these interventions on the basis of restrictiveness proves to be a purely subjective exercise fraught with personal bias” (Sadock & Sadock, 2007, p. 1376). While definitions are blurry, processes determining the least restrictive interventions are abstruse. The majority of participants answered the opening interview question using normalized psychiatric treatment language such as de-escalating, redirecting, distracting, talking, removing stimuli, self-regulating, and listening.
First, I try to go and talk to the patient and see what’s going on, see what their needs are. Maybe if something’s bothering them, or just try to talk and listen. If the patient starts to get aggressive, then we have an alarm that we can hit for the other staff to come. (Male, MHC)
Participants expressed tension between knowing what to do to prevent RS yet always being ready to do it. Four participants stated unprompted that they would not work in a facility where the use of RS was not an accepted option.
Reading the signs
Almost all participants referred to some way of observing or reading changes that signaled the emergence of a volatile situation, potentially resulting in RS use. However, not all participants believed that RS prevention and elimination is possible.
Participants described the signs they look for in patients having a hard time, cueing staff members that there is potential for RS: A change, not quite calm, but not yet escalated: a change in tone of voice. Maybe they are responding to internal stimuli, sometimes they just get a stare, like they are seeing something that is not part of what’s there or they see right through me. Maybe they have just thrown a hot drink. Pacing, that’s a big one. (Female, RN) I’m looking at their facial expressions, their tone of voice, looking at the escalating kind of things that are going on, their body movements, just trying to read them that way. Does it look like they’re going to come at me and hit me? Or does it look like they are open to talking? Do I need to come closer or back away? (Female, RN)
Kontio et al. (2012) suggest that psychotic behavior is the Number 1 reason RS are used, whether the behavior is aggressive or not. According to Sadock and Sadock (2007), in conditions such as acute schizophrenia, severe agitation occurs due to frightening hallucinations and delusions which are made more complicated by a sense of paranoia, which in turn is made worse when the trauma of RS use is added. Exhibiting symptoms is a way patients attract attention, letting psychiatric health care workers know that they are struggling emotionally or losing touch with outside reality.
One participant described reading the signs as a form of gambling, with knowledge of the patient as the unknown card.
For boys who we kind of knew were posturing, we would challenge them. I’ve got in people’s faces and said, “Go ahead. Carry out your threat!” I was gambling and guessing based on my relationship with them. I’m looking for tension in the shoulders, the shoulders hunched up, fists clenched, tone of voice, volume of voice, yelling, the language; are they cursing versus are they just kind of speaking more normally or pacing, shadow boxing, feet boxing, punching the air, kicking things on the ground, stomping. (Male, MHC)
Participants talked about de-escalation training as being helpful. Some had negative reactions to their coworkers use of RS, rather than knowingly using skills learned in de-escalation trainings to prevent RS. Reading the signs also pertained to coworkers who add to the tension in a pre-crisis situation, increasing the probability of RS use occurring with a patient which eventually leads to more work for the staff.
Their [staff] pride gets in the way. And those are the restraints that make me sick, the ones that occur because of staff. (Male, MHC) I feel like sometimes it’s [RS] used as a punishment. Like, [whispers: No one will know what I’m saying right?]. Because afterwards it’s, “Ok, they won’t mess with us again. They won’t do that again” but you know, “put them in a bed net and we won’t have this problem again.” So I think it’s used as a punishment instead of de-escalating a person, which is what the intent of it [de-escalation training] is. To keep them safe. To keep us safe. There’s a perception that it is less work to do a restraint or seclusion, even though it is a lot of extra paperwork. (Female, RN)
Psychiatric health care workers who are educated to read the signs, with persons who are at risk of becoming aggressive and know how to prevent RS use, are less apt to become victims of patient assaults (Schwecke, 2007).
There was a staff member that got hurt, busted her ear. She worked at a prison, and she said, “If I could have just done this hold [demonstrating], I could have stopped everything. It would have worked alright! It wouldn’t have involved so many people.” We can only do approved holds. There was a basket hold and then the one where you grab around, but it just depends on the size of the person. There’s a new hold that we’re doing where patients lay on their back, arms out, and then someone curls around the person’s thighs. I could not get my arms around a girl’s thighs! That hold is just horrible. Plus, your face is right there. It’s just—that hold, is just—and the guys have to put their knees between the person’s elbow [laughs]. But, in the meantime, there’s a lot of chaos and these things are hard to do. (Female, MHC)
Knowing how to prevent RS use can be confusing when the emphasis is placed on how to use RS instead. Stromberg (2012) suggested that traditional “de-escalation” trainings are insufficient to change the kind of normative culture of care where the use of RS is commonplace.
Facing challenging moments without resources
The vast majority, 19 participants, did not feel that they had the resources to prevent RS use. Staff shortages, along with a lack of education and time, and feeling de-valued by their institutions were often cited as problems endemic to the workplace. This was described by health care workers as receiving low pay and not having the resources to do a good job. The physical environment, architectural layout, staff time, staffing patterns, institutional culture, and unit space were found to be deficient.
The staff were upset, so the patients pick up on that. No matter how hard they [staff] try to hide it, they [patients] pick up on it, and are a bit more on edge. In my case, the layout of the building and staff not being able to see me or what was going on was the reason the assault happened. It could have been lethal. (Male, MHC) This staff person has been hit more than once. I’ve seen the way this staff has talked to patients and approached patients. Maybe that could have been prevented. I don’t think he got enough training, because his preceptorship lasted just a few days. I really don’t think they’re [administration] allowing new staff to work with someone long enough. (Female, RN) If there is a unit that ought to be aesthetically pleasing, positive, therapeutic, it’s ours, but it’s not. It looks like a broken down motel. (Male, MD)
Seeing others hurt, experiencing fear
Patients experiencing fear are often met by health care workers who are also afraid. Fear has been identified as a challenging barrier to transforming psychiatric health care workers’ orientations to more recovery-oriented paradigms (Ashcraft & Anthony, 2008). Almost all the participants had seen patients or other staff members injured during a restraint or seclusion. Seventeen participants reported on the LEC that they had themselves been the victim of a physical assault; for example, being attacked, hit, slapped, kicked, or beaten up at some point in their lifetime. Two participants had firsthand knowledge of patient deaths from asphyxiation that were the result of using some type of restraint.
Several participants revealed that they had family members who had been hospitalized on psychiatric units and felt that they had a stake in improving the experiences of patients and families on these units. However, the lack of knowledgeable staff, resources, time, and support from ADMs left these participants often at odds with their respective institutions values and priorities when it came to issues of quality of patient care and value-based priorities.
Meso
Facilitators to RS prevention identified at the institutional level were meeting people where they are and attending to safety risks. Participants viewed education, leadership, administrative support, and appropriate staffing to be the value-based priorities that facilitated RS prevention. Obstacles included the perception of scant resources allocated to specific RS prevention practices, staff not being listened to or included in policy-making processes or decision-making; and fearing loss of employment.
Being unaware of prevention policy
More than half, 16 participants were unaware of any RS prevention policies. All participants knew of some policies related to how to use RS, but few had specific knowledge of institutional prevention policies. The discussions on policies often centered on policies that were “passed down” to psychiatric health care workers from their administration, or from state and federal PMs. Four participants had participated in the creation of prevention policies.
There are the cattle prods of Joint Commission and CMS, cattle prods are extremely strong, if you are in administration in a psychiatric facility. I will say that our leadership, the administrators of the hospital and other people were all very focused on restraint and seclusion. These were things that were recorded at every leadership meeting, probably monthly. We had extensive data. We wanted to be on the cutting edge of every new practice or strategy that could happen. It was an absolutely strong focus at the hospital. Now, whether that translated into much better results, I don’t know right this minute. (Female, ADM) The message my staff get from me is that restraints are considered failure in treatment. So, if you’re using restraint, there’s a failure in treatment. When we talk about restraints or using restrictive interventions, we talk about what we could have done differently. Could we have maybe got somebody that knows the patient better to talk with them beforehand, did the patient meet the criteria for seclusion? So why did the patient go into restraint, rather than seclusion? Seclusion is least restrictive. (Female, ADM)
Findings at the meso-level demonstrate that the policy of RS elimination originates at the federal level. Material contained in the Seclusion and Restraint: National Action Plan (SAMHSA, 2008) is mismanaged at the intersectional, institutional level, while participants described a wide range of misinformation used to justify unclear outcomes. For example, ADMs expressed being pushed into compliance by utilizing data without fully comprehending the contextual nuances that underpin prevention practice and demonstrated misunderstandings about the use of the least restrictive interventions. If policies are not well understood at the institutional level, implementation on the practice level is near impossible.
Macro
According to Tovino (2007), high-quality psychiatric health care treatment is not distributed evenly, and problems related to access and finance figure prominently. Policy translation and implementation are contingent upon what has value to the society at large, the legislative bodies, the regulatory agencies, the institutional cultures, and the professional standards of those engaged in psychiatric practice. People have better or worse mental health depending on where they live and how their communities are structured and organized (McKenzie & Harpham, 2006).
Leveling the playing field
Federal PMs expressed lofty goals and ideals in contrast to frontline psychiatric health care workers. Trauma-informed care was identified as a way to respectfully approach patients and staff to level the playing field.
So it has to be trauma informed care for everyone, you know, to level the playing field. Trauma informed care is really about being respectful, respectful to everyone including staff. I mean it has to be the direct care staff, you know, that’s who needs it most in the industry. (Female, PM) Seclusion and restraint, first off, are non-evidence-based, historical interventions that more mimic assault than they do any kind of clinical therapy. There is no evidence for it that they have any therapeutic benefit. They generally should only be used as safety measures of last resort in the face of imminent danger, but over the last fifty, sixty, seventy years they’ve become way overused. They were always fairly unregulated and have caused not only a lot of emotional trauma to both the people being restrained and secluded but also to the staff being asked to do it. They’ve also caused many accidents, serious injuries and a multitude of deaths. (Female, PM) Because as far as private hospitals here, they don’t think we have any business in their business. So it’s going to be interesting. But with the USDOJ kind of quietly in the background, and the fact that these private hospitals are living on Medicaid clients, I’m going to try and do it. We’re going to fix our regulations this next year. (Female, PM)
Regulation was identified by one participant as the only viable route to RS prevention and elimination. Providing health care workers with adequate support and resources to prevent RS should be a condition for facilities receiving Medicare and Medicaid payments.
Bourdieusian Analysis and Core Categories
Because the micro- (practice), meso- (habitus), and macro- (field) levels were analyzed, three major themes constitute the core categories of the theory (see Figure 1). The following analysis is a sequential synthesis of these multilevel findings in more abstract and theoretical terms. These are detailed below. This includes an appraisal of how thoroughly federal policy has influenced the creation of institutional cultures of RS prevention practice and non-violence in the field of practice, which are identified as essential to RS prevention ideology, and how fully psychiatric health care workers have been involved in implementing evidence-based best practices with fidelity (Lebel, 2011).
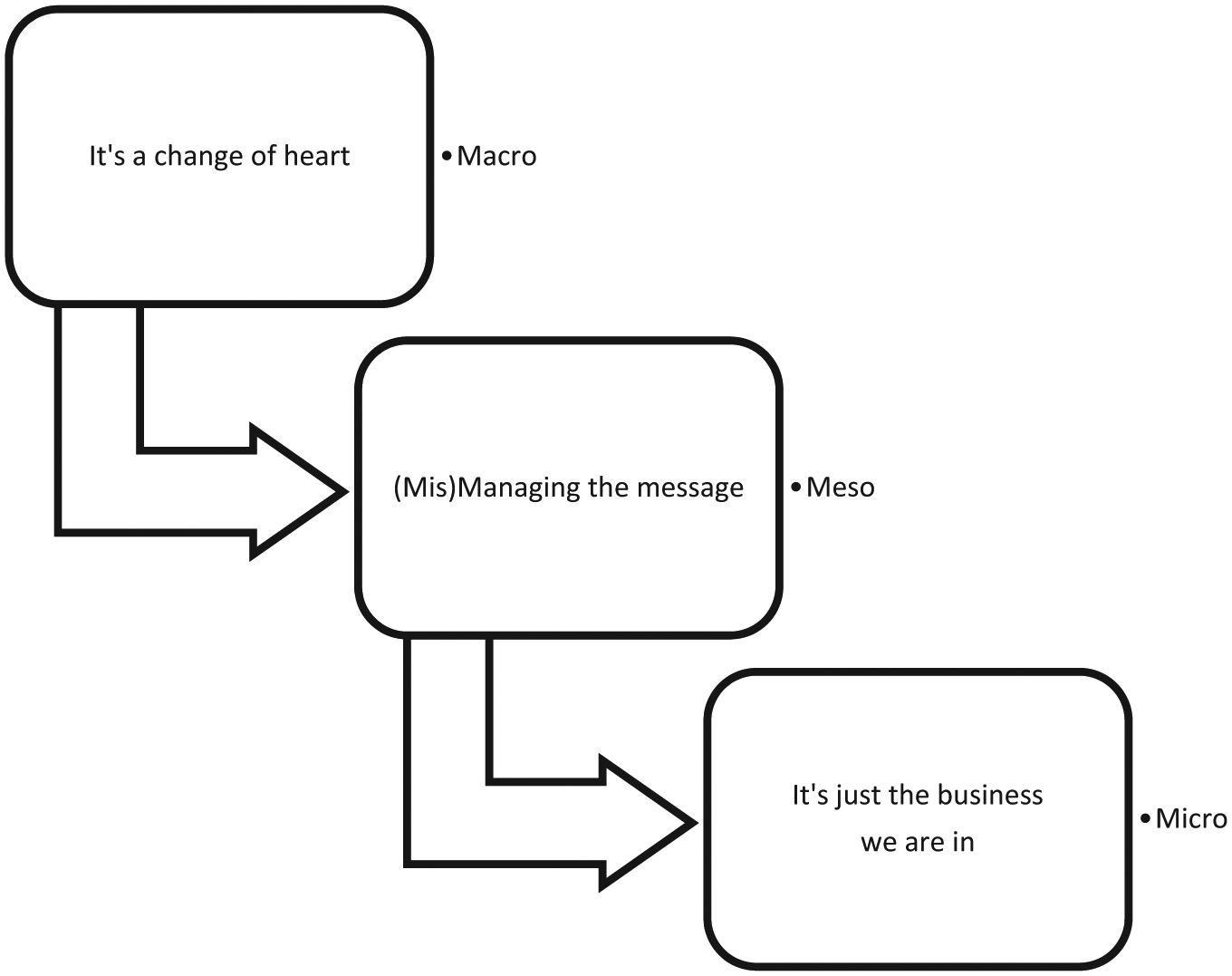
Core categories: Preventing the use of restraint and seclusion.
It’s Just the Business We Are in
On the individual practice level, there are unseen consequences to the violent encounters experienced by psychiatric health care workers in environments where the use of RS is commonly practiced. Health care workers distance themselves and react without thinking in response to repeated exposure to violent and traumatic events. These workers create personal meanings based on an evaluation of the level of threat, harm, or challenge experienced; and, by an evaluation of their perceived options and abilities to mitigate the effects of the potentially traumatic situation (Van der Kolk, 1996). Carlsson, Dahlberg, Lutzen, and Nystrom (2004) suggested that the way the psychiatric health care worker copes with and handles his or her sense of fear is a decisive factor in how a potentially violent encounter will progress. Emotional disconnection or distancing is a predictable response to prolonged stress or fears. This occurs physiologically, with the down-regulation of corticotropin-releasing hormone, decreased adrenocorticotropin-releasing hormone, and increasing levels of testosterone and estrogen. Successive and repeated stressors can have cumulative physiological and psychological effects causing the experiences of hopelessness in these trauma-exposed individuals responsible for caring for this vulnerable population (McFarlane & De Girolamo, 1996). According to Carlsson et al. (2004), this repeated level of fear can lead the psychiatric health care worker into a state of chaos, where uncertainty and anxiety dominate, contributing to the business as usual status quo: acting without thinking.
As coding progressed, an in vivo category reemerged that crystallized the theoretical analysis pertaining to individual practice. Examining these reemerging codes and categories related to resources such as staffing patterns, time, and space, the in vivo quote, “It’s just the business we are in,” summed up the tensions between and among (a) the belief in and the knowledge of the possibility of prevention practice actions and (b) the acceptance of structurally defined and objectively imposed limitations on prevention practice.
The in vivo quote, “It’s just the business we are in,” points to the objective meaning that this business of RS prevention has for participants. The more psychiatric health care workers incorporate the language of economics and the metaphor of business, and accept the hegemonic forces of the market, the less time and other resources are perceived to be available to make moral decisions about the human beings in their care. The more the business model is emphasized in practice, with a focus on its limited resources, whether it be real or perceived, the more psychiatric health care workers think they must act out of necessity, rather than acting out of a sense of moral freedom, or duty to care for their patients. The following participant quote depicts what it means to be in the business we are in: We don’t have the space [to prevent RS], and I think administration gets frustrated with that too. You know, dealing with a building that really just, that needs, we need, I mean it’s awful. It’s painfully obvious. I even know that engineering gets frustrated trying to keep up. You know, it’s just the business we are in, but it takes a lot [money] to get a new building. (Female, NM)
In attempting to reconcile, literally and physically, what gets in the way of RS prevention practice, this participant brings up the building she works in. Not only does she reveal her frustration about the space, she alludes to this lack of resource as being “painfully obvious.” Looking to the future, she does not have confidence that there will be enough resources allocated to fix the dilapidated building in which she works, because it will take a lot of money. Everyone is frustrated trying to keep up with the physical and structural deterioration of the building. The aging, outdated building takes on symbolic meaning and delivers a message that is unmistakable. It is asking too much to prevent RS use when the structures around you and your coworkers are decaying. Fatalistically, she declared, “It’s just the business we are in.” In other words, it cannot or will not be changed by those in higher positions in the organization.
Mismanaging the Message
On the institutional level, definitions of RS are not uniform across psychiatric facilities and ADMs are not well versed in the most up-to-date best practices. Another participant did not believe that there are adequate supplies needed for her to engage patients in meaningful activities because she works in mental health. Thus, working in mental health means there is a natural consequence of going without the resources you need. At this institutional level, RS prevention is not well understood or valued as a determining factor in creating an ethic of care. While finances are perceived to be scarce, the messages passed down to frontline workers are confusing and paradoxical, especially when it comes to providing enough resources to maintain an ethic of care on psychiatric units, including adequate staffing.
The business of RS prevention includes the way psychiatric health care workers see RS prevention practice in relation to psychiatric patients, the way the message of RS prevention practice gets managed structurally in institutions, and the way federal-level policy is interpreted. Participants felt constrained by their environments, further limiting their ability to experience their work or RS prevention as important or worthy of investment. Psychiatrically hospitalized people and the health care workers caring for them are at the mercy of the profits of market forces, which ultimately determine how RS prevention or use is practiced. Psychiatric health care workers often receive mixed messages from leaders: Do not use RS, but however, do it with the inadequate resources you have in terms of buildings, staffing, and assistance.
It’s a Change of Heart
In direct contrast to mid-level ADMs and frontline workers, top-level PMs did not see RS prevention as a costly undertaking. In practice, psychiatric health care workers expressed despair describing their surroundings and lack of support and resources. At the institutional level, there was a mismanaging of the message of RS prevention. PMs at the top of the field considered RS prevention nothing more than a “change of heart.”
It doesn’t really cost any extra money. It’s a cultural and attitudinal shift, it’s a change of heart. It doesn’t cost anything. It’s a culture. What we do is free, there is no dollar sign attached. Not only that, to tell you the truth, it would be more cost efficient [to prevent RS]. I mean look what happens with worker’s compensation, or staff injuries or calling out [sick]. When you have restraints and seclusions it’s as traumatizing to the staff as it is the patients who are being restrained. So I would have to say that the staff, even if they are not bleeding, what happens to them psychologically? Because they are in an environment where—what they are doing to people all the time affects them. That’s the long term effects of violence. There is nothing therapeutic about that. (Female, PM)
The messages of violence prevention and trauma-informed care are espoused in the ideological spin off. However, as the macro message starts in the heart and soul of culture, where the less visible structures organize practice, it ends up in the mundane world of business as the message increases in dross and loses meaning.
While examining meanings, it was important to first see the social in the individual. What people do and think, and how they interact at the individual and local levels, informs their everyday ideologies and determines their paths of participation in the social world (Charmaz, 2006). These psychiatric ideologies are translated through action into the world of practice where these ideas are produced and reproduced. The language of psychiatric care processes takes on the vernacular of business as usual.
The first research question examined practice norms and actions that psychiatric health care workers perform in their social worlds to prevent RS use. On the surface, this is a simple question. However, what participants reveal about how they view their practice environments, their coworkers, and their workplace hierarchies shed more light on what is missing for them in their practice worlds than what steps they take to prevent RS use. Difficult and complex patient care decisions concerning RS use are made without support, in chaotic environments where participants feel rushed to act out of a habit of necessity, acquiesced to, and justified by a lack of adequate resources. This reveals a notable gap in the translation of best practices in the area of RS prevention on inpatient psychiatric units. The messages of trauma-informed, patient-centered, strength-based, and family-centered care in the facilitation of quality preventive care and treatment are not being adequately translated into practice. There is a disconnection between the ideal types of care promoted by SAMHSA and real-time practice. Access to quality care and how care is financed figure prominently in this equation (Tovino, 2007).
Conclusion
The connections among the micro-, meso-, and macro-level analysis, in concert with the relational characteristics of practice (individual), habitus (organizational), and field (policy), form a complex web of facilitators and barriers influencing RS prevention practice (see Figure 2). At each level of analysis, the core categories are at cross purposes, while espousing intent to prevent RS use. Concepts, meanings, and ideologies are put in motion, reproduced and made to work in the social world of psychiatric RS prevention and use (Bourdieu & Wacquant, 1992). This was a descriptive study conducted in one region of the United States, and results may not be transferable to other regions.

Representation of macro-, meso-, and micro-analysis related to core categories.
Implications
According to these participants, psychiatric health care workers are not always prepared to prevent RS due to multiple barriers, including a lack of resources, time, space, and education, and (mis)managed policy implementation. Environments of care are poorly designed. Few strategies for improvement are given. Only one participant, who worked in an adolescent facility, described any state-level regulations or oversight from any state agency. The following describes some possible solutions to these practice-level barriers.
Policy and Procedure
Involving psychiatric health care workers in the crafting of RS prevention policy is one low-cost, high-impact intervention that has the potential to increase both patient satisfaction with psychiatric care and staff members’ satisfaction with their job-lives. Opportunities for nurses, MHCs, and other direct care staff to offer suggestions and to work interprofessionally on quality improvement projects create positive relationships that change culture. By engaging direct care workers in creative projects, organizations invite budgetary savings related to the use of RS, worker’s compensation, liability, and staff turnover (Lebel, 2011). Investing in this simple intervention makes sense, while raising the consciousness of psychiatric workers by helping them reorganize their priorities to align more closely with the RS prevention agenda, rather than with the objective finality and economic fatalism invoked by the business model. However, without the cooperation of state-level regulators, insisting on this level of quality control, business as usual will predominate.
Trauma-Informed Care
Trauma-informed care involves a reorganization of ideology, a paradigmatic shift in thinking that can only occur by changing the structures of care and caring, both visible and invisible. This involves translating the message that RS use is traumatizing to both patients and psychiatric health care staff, including understanding the roles that violence and victimization play in the lives of psychiatrically hospitalized persons. This challenges the business as usual model of psychiatric care by transforming the power dynamics among staff and patients into a more collaborative model of cooperation, rather than forced compliance. Trauma-informed care includes the psychiatric health care workers in the equation by helping them examine their own vicarious traumas related to violence on inpatient units (Stromberg, 2012). According to the LEC, 80% of these participants have been victims of physical assault, and almost all have seen other staff members or patients injured during a RS.
Specific Mandates
There are clear and purposeful actions that the psychiatric health care professions are well situated to carry out, in relation to the business of preventing RS use. First, the information and research forming the growing evidence base that RS use is dangerous and ineffective needs to be compiled and widely disseminated through education, and applied in practice. Second, research is needed to develop a body of alternative intervention strategies to counter the effects of the language of business deployed in psychiatric care. Third, nursing and other disciplines have a duty to join together and support scholarship that reinforces the ethical argument against the business model of mental health care that supports the continued use of RS as a valid treatment intervention. This includes advocating for this vulnerable population of hospitalized persons at the community, state, and federal levels to assure that they are being cared for in the most humane and least restrictive manner possible. The prevention of violence in mental health treatment and the promotion of healing environments are public health priorities. This amounts to more than just the business we are in.
Footnotes
Acknowledgements
I would like to acknowledge my dissertation committee (Sandra Thomas, Marian Roman, Paul Erwin), the phenomenology research group, and the grounded theory research group at the University of Tennessee, Knoxville. Special thanks to my dissertation chair and co-author, Joanne M. Hall and Jan Brown, leader of the college of nursing grounded research group.
Authors’ Note
Kelly Carlson is now at Dr. Lillian R. Goodman Department of Nursing, Worcester State University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This research was funded in part by a leadership award from Sigma Theta Tau, Gamma Chi chapter.