
Abstract
Participants (6 male, 4 female) on a methadone maintenance program completed a Think-Aloud procedure while viewing two stereotypical picture sets depicting opiate-dependent and mainstream lifestyles. Discourse analysis indicated that participants used two different discourses: a stereotype-affirming defensive discourse, which involved affirming the negative and positive stereotypes regarding opiate-dependent and mainstream lifestyles, and a stereotype-refuting defensive discourse, which involved refuting negative opiate-dependent stereotypes while constructing mainstream lifestyles and members negatively. We argue that both discourses fit within a grander discourse concerning normalization with participants’ speech functioning to defend them from being negatively stereotyped by making them “normal” members of society.
Introduction
Opiate-dependent people are stigmatized members of society: They have been demonized by politicians, the law, and the press (Buchanan & Young, 2000; Elliott & Chapman, 2000) and are labeled as “dangerous,” “anti-social,” “unassertive,” and “dirty” by the general public (Finnigan, 1996; Sheard & Tompkins, 2008). This can push people who are dependent on opiates away from mainstream society, as well as make recovery more difficult by hampering their reintegration into the mainstream (e.g., drug offences make it more difficult to become employed). Opiate users may also internalize negative stereotypes, losing self-confidence and feeling “discarded and isolated from mainstream society” (Buchanan & Young, 2000, p. 414). Indeed, many studies report opiate users’ feelings of social exclusion as well as a yearning to have a “normal” life (Andersson, Nilsson, & Tunving, 1983; Nettleton, Neale, & Pickering, 2011).
The nature of addiction can also push one away from a mainstream lifestyle. For example, although economic disadvantage is not as associated with heroin initiation as the stereotype purports (Seddon, 2008), poverty can become a serious problem if one becomes dependent, which may then lead on to other stigmatized social issues; homelessness, physical/mental illness, and criminality are all more prevalent among opiate-dependent people (Sheard & Tompkins, 2008). Being part of mainstream society is also about having relationships with others who are part of the mainstream, yet people who become dependent on opiates increasingly withdraw from non-using friends and family (Best, Manning, & Strang, 2007). Finally, the opiate-dependent community has its own language, shared understandings of needs, and shared experiences that make it more comfortable around like members (Anderson & Levy, 2003), which opiate users may contrast against the identity and pressures of the mainstream (Best et al., 2007).
While there is ample literature concerning how proponents of mainstream society view opiate-dependent people, there is minimal literature regarding how people who are dependent on opiates view or construct their own lifestyles, and none that explicitly and purposefully look at how opiate-dependent people view or construct a mainstream lifestyle or mainstream members. There are several reasons, however, that an opiate-dependent persons’ relationship with, and constructions of, mainstream and opiate-dependent lifestyles may be important. For example, De Maeyer, Vanderplasschen, and Broekaert (2009) found that the two most important notions in quality of life from the perspective of someone who is dependent on opiates are personal relationships and social inclusion, which were severely hindered by being outside of the mainstream society. In Best, Ghufran, Day, Ray, and Loaring (2008), the most commonly expressed reason for wanting to be abstinent was becoming “tired of the lifestyle,” and the strongest cited factor for achieving abstinence was moving away from drug-using friends. Furthermore, mainstream services designed to help people become free of opiates are often found to be stigmatizing and shaming to service users, effecting continued participation (Gourlay, Ricciardelli, & Ridge, 2005; Radcliffe & Stevens, 2008). Finally, Nettleton et al. (2011) and Taïeb, Révah-Lévy, Moro, and Baubet (2008) found that people who recover often see themselves as “damaged” and seek to establish “acceptable” (mainstream) identities.
Given the present discussion, the aim of this study is to explore how people who are dependent on opiates but are on a methadone maintenance program talk about and construct mainstream and opiate-dependent lifestyles in reaction to mainstream and opiate-dependent stereotypes. But first, it is worth considering participants’ positions in the study; they have taken steps to become free of illegal opiates via methadone maintenance and attending key worker meetings regarding health, employment, housing, and criminal justice. Thus, participants are under explicit surveillance from a mainstream institution and their help-seeking actions implicitly or explicitly represent a shift toward mainstream society.
Method
Design
The study is qualitative, using a “Think-Aloud” procedure with some verbal prompts to gain audio data. The order in which the opiate-dependent and mainstream picture sets were shown was counterbalanced.
Sample
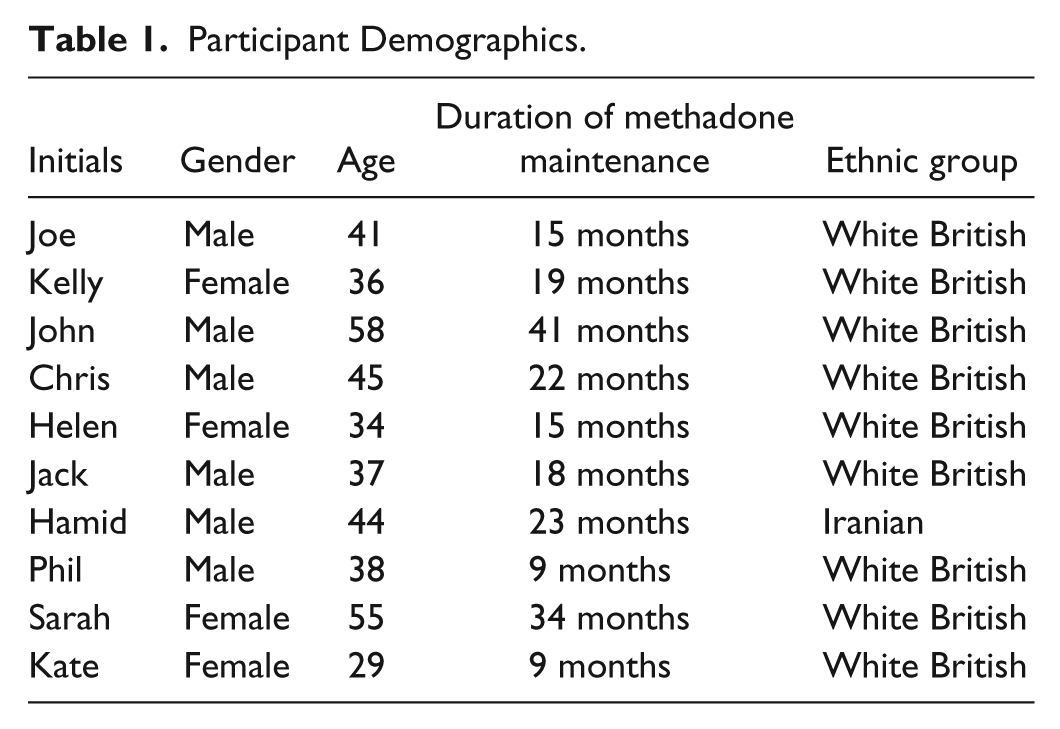
This opportunistic sample consisted of six males and four females, aged 30 to 58 years, all of whom were White British apart from one male who was Iranian. All participants were on a methadone program at a harm minimization charity for drug-dependency (where A.M. had volunteered for 9 months), primarily opiates, in outer London. Although no participants claimed to still be using opiates, this cannot be ruled out, and some participants said they were using other illegal drugs (e.g., marijuana) and/or alcohol. Participant demographics are shown in Table 1. All participants have been given a pseudonym.
Participant Demographics.
Measures
The Think-Aloud procedure involved talking as much as possible in reaction to the images presented. After the participant had stopped talking for a significant amount of time (approximately 15 s), the researcher prompted the participant to talk about a picture they had not yet discussed or if the participant had talked about all of the pictures, then the researcher used a pre-developed prompt or one based on what they had said during the procedure.
The reason for employing the Think-Aloud method was to reduce overly thought responses and facilitate a stream of consciousness (Aanstoos, 1983) in the hope of better replicating more passive, everyday situations where one is on a more reactionary, pre-conscious level.
Procedure
Participants completed the procedure in a small room at a drugs charity they attended almost every day as part of a methadone maintenance program. The researcher explained to participants the Think-Aloud procedure and that they would be shown stereotypical images of opiate-dependent and mainstream lifestyles, stressing that there were no right or wrong answers, as the procedure simply requires talking about what comes to mind when viewing the pictures, and that there are no “tricks.” The first set of images was then revealed (which were pinned onto a board at random, apart from the central image which was always either the picture of heroin or the pint of beer depending on the lifestyle that was being represented). After clarifying each picture (e.g., saying the picture of the squat was not just a run-down house, etc.), the participant was asked to begin, the microphone was switched on, and the researcher then sat behind them. After viewing the first picture set (for 10-15 min), the next image board was set up, the images were explained, and then the participants were asked to “think aloud” about them as well.
Pictures
There were eight pictures in each of the two picture sets. One picture set was selected to represent a stereotypical mainstream lifestyle, and consisted of a family meal, a typical semidetached house, a woman shopping, a pint of beer, commuters getting on the tube to work, four friends laughing, a heterosexual couple, and a credit card. The other picture set was selected to represent a stereotypical opiate-dependent lifestyle, and consisted of a block of council estate flats, a woman shoplifting, a mother with two young children (one White, one mixed race), a heterosexual couple, a homeless man with a dog and a cup, a 10 pound note, a large pile of brown heroin, and a squat with some young people sitting.
The ideas for images were chosen in collaboration with people who are or have been dependent on opiates. Care was taken not to make the stereotypical opiate-dependent lifestyle pictures too extreme to constrict the participants’ constructions.
Data Analysis
The analysis is placed within the traditions of Potter and Wetherell’s (1987) model of discourse analysis which emphasizes the action orientation of talk, considers discourse as “doing,” and focuses on the ways in which participants use discursive resources and manage issues of interest and stake. In addition, the analysis was informed by the principles of Billig’s (1987) rhetorical psychology. Rhetorical psychology draws on the long-standing history of the study of rhetoric and places the ways in which people speak or write within a notion of argument and ideology and highlights their cultural context at any given time. Accordingly, using both these perspectives reflects a methodological position whereby the language people use can be read to explore the positions they are taking within their given social context.
Results and Discussion
Overall, two discourses could be seen within the data relating either to affirming or refuting stereotypes; these discourses fit within a grander discourse concerning normalization. These will be briefly described before being detailed further.
Stereotype-Affirming Defensive Discourse
Of 10 participants, 4 (Kelly, Sarah, Hamid, and Helen) had an overwhelmingly stereotype-affirming defensive discourse. On the whole, this involved supporting negative stereotypes regarding an opiate-dependent lifestyle and positive stereotypes regarding a mainstream lifestyle, while keeping oneself from being labeled a stereotypical “junkie.” Given participants were recruited because they were on a methadone program, by affirming the negative opiate-dependent stereotypes and separating themselves from those stereotypes, participants placed themselves in a more positive light; by affirming positive mainstream stereotypes participants could speak of their “new life” in a positive way, as well as once again place themselves outside of a negative opiate-dependent stereotype by allowing referral to “normal,” positive aspects of a mainstream lifestyle they kept during the time they used opiates. Thus, one can see how affirmation of the stereotypes can serve to defend the participant’s image; however, when “affirming participants” were unable to separate themselves from a negative stereotype, their language then often served to make them blameless, again defending their image.
Stereotype-Refuting Defensive Discourse
Of 10 participants, 3 (Joe, Chris, and Kate) had an overwhelmingly stereotype-refuting defensive discourse. Essentially, this involved challenging the stereotypes and re-organizing the realities presented to make them more equal and overlain. By talking about the mainstream negatively, participants positioned their current and/or old lifestyles as a more equitable alternative, as opposed to a sharp drop in status. “Refuting” could also challenge the stereotypes by widening the boundaries of the presented conception of mainstream and opiate-dependent lifestyles, deconstructing them such that the categories became convoluted. The reconstruction of stereotypes did not go so far as to present opiate use positively, or whatever lifestyle or activities surrounded opiate use for the particular participant, but talking about it negatively seemed to be avoided; instead analogies were often drawn, for example, by comparing opiate use with alcohol. Like the “affirming” discourse, the “refuting” discourse can be seen as protecting the participant’s image. Again, actions could be constructed as more blameless if “refuting” was a restricted option.
Three participants did not have a mainly “refuting” or “affirming” defensive discourse. Of these, two participants (Jack and John) had a more “affirming” discourse concerning mainstream stereotypes and more of a “refuting” discourse concerning opiate-dependent stereotypes, though not as strongly as the mainly “refuting” participants. The last participant (Phil) did not say much and the procedure was short as he had a very strong emotional reaction to the “alcohol” image; therefore, not enough text is present to make a judgment regarding overall discourses.
Normalizing Defensive Discourse
The “affirming” and “refuting” discourses in essence serve the same defensive function—that of normalization. The “refuting” discourse worked on more of a group level, challenging the construction of normality presented by the stereotypical images, for example, by blurring the boundaries between mainstream and opiate-dependent groups and lifestyles or by constructing the mainstream negatively, making the lifestyles more equivalent. If we think of the stereotypical lifestyles as two separate, hierarchical boxes, the “refuting” discourse works by bringing the mainstream box down in line with the opiate-dependent box and expanding the borders so they overlap. The “affirming” discourse worked on a more personal level: Instead of challenging the presentation of group stereotypes, it served to place participants outside of the opiate-dependent stereotype, often as an exception during the years when they used. If we again think of the lifestyles as hierarchical boxes, the “affirming” discourse largely left the boxes where they were and placed participants outside, somewhere in-between. As mentioned, making oneself blameless was another strategy used by participants; this fit into the normalization discourse as it served to signal that the participant was not a bad person, but rather that their actions were understandable and normal given their circumstances.
The two subdiscourses—stereotype-affirming defensive discourse and refuting defensive—will now be described in greater depth in relation to the process of normalization.
Stereotype-affirming defensive discourse
As part of the basis of an “affirming” discourse, a mainstream lifestyle was labeled as normal and attractive. Indeed, within an “affirming” discourse, participants, aside from the topics of alcohol and stigmatization, had no criticism of the mainstream and only talked about it in an aspirational way, for example, having steady employment, family meals, shopping for the week instead of a day, and so on:
could be anywhere, looks quite nice, hmm I’d like to live there, yeah, nice little garden, yeah, quaint . . . family having dinner, hmm, yeah, I’d pictured myself happy like this once. (John) Right, these are just part of a normal life. (Kelly)
Consequently, the mainstream was constructed as a positive lifestyle, especially in terms of community:
but everything’s building up nicely, I got a fam- a new baby on the way, and everything seems to be good, you know, I do miss friendship, like I say I’m building up on friends but to be honest, a lot of my time on my own, cause I isolated myself so much, and work, I’ve lost jobs, you know, really good jobs. (Helen)
As exampled in the above quote, the positives of a stereotypically mainstream lifestyle were often contrasted against the negatives of their own, previous opiate-dependent lifestyle—a lifestyle and drug that was constructed entirely negatively:
the lifestyle gets you down, everywhere, always ‘round the corner, and it just takes you places before you know it. (Sarah) this stuff is, is evil and it will make people, the nicest people do the horrible-est things. (Helen)
Indeed, opiates were portrayed as a drug that “spirals” one “out of control” (Helen). These particular constructions also mitigate participants from possible attacks on their character, given opiates can make the “nicest people” commit horrible acts and take people places without their knowing. Mitigating responsibility was a feature of “affirming defensive” discourses in terms of opiates, parental responsibilities, and crime; one participant employed a medical discourse when talking about her opiate dependency:
you know I’ve never met anybody like me, who was taking drugs, everybody was so greedy, “yeah I’ll have that and all this pills and whatever,” no I didn’t use like that, I just used to stop being sick. (Kelly)
Here the participants’ drug-use was presented as more of a necessity, in contrast to the “greedy” stereotype (a presentation that will also be seen in “affirming” participants’ criminal activities). Thus, by constructing an opiate-dependent lifestyle in a stereotypically negative way, participants can boost their image by comparison—“I wasn’t that bad”—as well as distancing themselves from the “opiate-dependent group” in general. Furthermore, participants talked about their opiate use in the past tense, positioning them outside of the associated lifestyle.
Negative stereotyping was not limited to the lifestyle or drug however, but extended to opiate users as well. This provided another opportunity to contrast their more “normal” and “positive” opiate-dependency with that of the stereotype:
my only saving grace is that I still got my looks and all my teeth (laughs), you know, most people they’re, they’re absolutely, torn apart by this drug. (Helen) they’re stoned, they can’t do anything, just get money for drugs, I, I had a job for most of the time, umm before I got sick, but that wasn’t related to umm, to heroin. (Sarah)
“Affirming” participants consistently placed themselves in the mainstream prior to drug dependency—further normalizing themselves in contrast to the opiate-dependent stereotype:
these photos represent to me, of what I’ve had, umm, before I heavily got involved with drugs, I had my relationship, I had my set of friends, I had my own house, umm, my own business. (Hamid)
In this quote, we get an indication of how opiates were constructed as a causal factor in negative life outcomes, something consistently emphasized within an “affirming” discourse.
In terms of whether “affirming” participants positioned themselves as having more of an “opiate-dependent” or “mainstream” identity in the present, it was variable as participants tended to switch depending on the context.
Still, when it came to an opiate-dependent lifestyle, it was spoken of in the past tense. Given participants’ history with opiate use and their affirmation of negative opiate-dependent stereotypes, it is not surprising “affirming” accounts referenced shame and guilt at their past:
I was always ashamed, always feeling guilty because of my kids, you know, and the friends I had left, they knew but, they didn’t know, not all of what I was doing. (Sarah)
Emphasizing guilt helps portray participants as more human than the opiate-dependent stereotype and helps inoculate them from potential attacks on their character. Relatedly, some participants also spoke about pretending to be normal during times of opiate use:
we were pretending to live a, nice, life, but you know behind doors it was domestic violence, stealing, crack. (Kelly)
Parenthood was quite a prominent theme for each of the three “affirming” women, and appeared to represent an important battleground for protecting their image. For Kelly, her keeping and looking after her children was the most prominent tool used in distancing herself from the “junkie” stereotype:
they don’t see their kids, ok so they might go visit once a year but they’ve definitely been taking it off whether it’s, I don’t know I can’t imagine how, I mean, I don’t know, I don’t understand why you can’t look after them though. (Kelly)
For Helen, it was a different story:
really I should have been thinking about my children and how to get them back, I didn’t lose them, I handed them to my father, voluntary, I had a break-down, so, but that was due to other things going on. (Helen)
Stealing was another contentious issue. Shoplifting was spontaneously admitted to by three of the four participants with a mainly “affirming” discourse and one with a mixed discourse, but none of the three “refuting” participants. However, these admissions fit within the “affirming defensive” discourse by contrasting their stealing—only occasional, little, and necessary—with the general, over-the-top stealing of a typical “junkie”:
well I got charged for both offences and I got put on tag, and really and truly I wasn’t a heavy shop lifter, I wasn’t someone out there earning money for drugs or really or going at it every day like some, other guys I know. (Helen)
Again, “affirming” participants presented themselves as “not-as-bad,” affirming the stereotype to their advantage. Three of the four participants also positioned their stealing within a more valiant or blameless frame by describing how they had to steal for their kids, even when the money was directly or indirectly for drugs, and two participants said they stole because they needed to eat:
but it’s usually just because I’ve been stoned and I need to eat, that’s mostly it, but umm, or it’s been a couple of times where I’ve nicked a couple of presents ‘cause it’s my daughter’s birthday or something, so I can spend the money on drugs but I’ve never nicked solely to buy drugs, never. (Jack)
Methadone, within the “affirming” discourse, was constructed as a positive intervention, one that would help with preventing a return to a previously chaotic life:
I’m leading that life now because I’m on the methadone. (Kelly)
Alcohol, on the other hand, was in fact labeled by all but two participants, across discourses, as a drug as bad as, or worse than, opiates:
in my actual experience of drugs, alcohol is probably about the worst drug going, when it comes to how it changes peoples personalities. (John)
This negative construction of alcohol, along with the construction for mainstream members who drink, enabled participants to present their addiction in a more positive light. By bringing alcohol into a similar arena to opiates and making their use comparable, participants also de-mythologize opiate use and opiate users. The use of alcohol as analogous to opiates could be considered a “refuting” tactic, but still fit into the “affirming” discourse with its higher function of normalization. “Affirming” accounts may also have benefited from a flavor of refuting in terms of allowing participants to be more balanced in their highly positive presentation of mainstream life, while simultaneously protecting their image.
There was one more topic where “affirming” discourses aimed some criticism at the mainstream, and that was related to stigmatization:
to just treat them like a human being, would, would really make a difference, cause that’s what people want, they just want to be spoken to normally, treated with respect, unless they’ve given them a reason, to dislike them. (Helen)
Like alcohol, commentary regarding stigmatization fit into an “affirming” discourse via its higher function of normalization—indeed the above quote explicitly relates stigmatization to not being treated normally. Criticism of the mainstream was also unproblematic for participants with a mainly “affirming” discourse because they would talk about past stigmatization, keeping them from presently being labeled negatively due to opiate dependency, but also removing them from the mainstream at the point where it is being criticized—though the “affirming” discourse by its nature involved the stigmatization of people who are dependent on opiates, producing hypocrisy when taken as a whole.
Refuting defensive
In general, participants with a mainly “refuting” discourse spoke negatively about mainstream lifestyles, with two of the three mainly “refuting” participants having nothing positive to say whatsoever:
looks like a typical wage slave environment, everything there is, to do with money and, earning it basically, apart from what would appear to be students rather than friends, but all the other pictures are basically, sheep going to work on the underground, which I did for years before I wised, wised up, the nice semi-detached house with the nice mortgage on it, which they’ll never probably never own. (Chris) and what, sitting ‘round the table not talking, being married and not having, having any fun or what, the couple, look how pissed they look. (Kate)
Here we can see the construction of mainstream lifestyles as money-oriented and monotonous. The contrast to the “affirming” discourse is stark; whereas “affirmers” saw a “happy couple” (Kelly), “a good healthy relationship” (Hamid), or a “lovely family” (Sarah), “refuters” talked about the same pictures negatively. However, mainstream lifestyles were at the same time talked about as normal, especially by Joe who was less directly critical of mainstream lifestyles: Instead of making mainstream lifestyle components more negative, he focused on making opiate-dependent and mainstream lifestyle components more equivalent and comparable:
That’s a normal house, a semi-detached three-bedroom house, that’s normal but it’s normal living on an estate as well . . . um, them two lovers, are like the lovers in the last one to me, no difference. (Joe)
As indicated hereinbefore, the process of normalization in the “refuting” discourse, as with its defensive function, is more explicit and direct than the “affirming” discourse. Furthermore, this normalization extended to the types of people who used opiates as well as opiate use itself, with all three of the “refuting” participants using doctors as an example:
the ones who come down here (drugs charity) might do but in life you get doctors on drugs, everything don’t you, they can write their own scripts out, you get politicians, everyone on drugs, you just don’t see them ‘cause they got money to go to a private doctor. (Joe) you’d be amazed at the number of doctors that, secretly addicted to opiates, thousands of doctors a year get put away to dry out, from opiate, addiction, but they’re not on the streets, they’re not on that board, their life is quietly brushed under the carpet, nobody wants to see it proved that people can live a normal lifestyle, and use opiates. (Chris)
In addition to illustrating high-status groups using opiates, serving to limit the types of inferences one might make from knowing someone is/was dependent on opiates, Joe’s quote has other normalizing—defensive functions—he uses an extreme case formulation when stating “everyone on drugs” and compares the clients of the drugs charity, who he says might fit the stereotype, to opiate-dependent people one would find in “life,” making the stereotypical clients seem not real and minimizing their representation of the group. Chris’s quote is interesting in the way it introduces conspiratorial tones, criticizing the mainstream who “brush” normal opiate-dependent lives “under the carpet.” Furthermore, arguing a counter position is made more difficult because challenging him would place one with the conspirators or the ignorant who do not want “to see it proved that people can live a normal lifestyle, and use opiates.” Notice here, also, the construction of heroin as a drug which can be controlled, a drug that does not take everything from you one by one. A final touch in the quotes was the effect of constructing non-stereotypical opiate users as people whom one does not see, either because they have money for a private doctor or because they are deliberately hidden; again, this makes their positions more incontestable. This worked especially because the “refuting” discourses were bolstered by participants’ appeals to special in-group knowledge; in other words, “refuting” discourses, which by their nature involved countering common ideas, required participants to make themselves the experts on the topic and the mainstream ignorant of reality (this was not a feature of “affirming” discourses, possibly because “affirmers” distanced themselves from an opiate-dependent identity):
they read a book, go to Cambridge and think they know something about heroin but unless you’ve been there, unless you’ve been there you have no fucking clue, so how do, do they, know me, they don’t. (Kate)
With the “refuting” discourse, participants tended to talk about groups as opposed to individuals, and spoke very little about themselves and the particulars of their own life. As such, “refuting” participants did not talk about guilt, shame, personal crimes, or about what they have lost because of opiate dependency. Indeed, for the “refuting” discourse, it would not be beneficial to give evidence reinforcing negative opiate-dependent stereotypes, and because participants presented opiate users as heterogeneous, speaking at a group level ensures that any negative conjecture is placed within the category of stereotyping and stigmatization. Focus at the group level also meant “refuting” participants did not talk about their “old selves” as illegal opiate users, as the “affirmers” did—in fact, they rarely talked about their own opiate use at all. Indeed, if the “refuting” discourse worked by challenging and convoluting the distinction between opiate-dependent and mainstream lifestyles, there is less appeal to a before and after, especially a negative old self and positive new self; the effect of this is to reinforce, or at least not clash with, the construction of people who are opiate dependent as normal people who happen to use opiates. One consequence of all this is that the “refuting” discourse rarely implicates opiates as a causal factor in negative consequences, instead attention is deflected:
that shoplifter . . . could be stealing for drugs but could just be for some money, most people steal for alcohol. (Kate)
Not surprisingly then, “refuting” participants did not say that the stereotypical opiate-dependent images were a good representation of opiate dependency:
right, in all your pictures, uhh, you’re portraying a heroin user as a down and out, socially maladjusted, emotionally disturbed, individual or individuals, you don’t portray, the whole picture of heroin addiction or addiction in general. (Chris) . . . yeah they represent . . . apart from the one in the middle (picture of heroin) they could all be anything, any lifestyle can’t they . . . take the drug one out the middle and all the rest could be a normal lifestyle. (Joe)
Here we see two very different ways to “refute” the stereotypes: Chris describes the pictures as extreme and unrepresentative, while Joe describes them as so normal they could be part of “any lifestyle.” Either way the effect is the same, whether a part of a more mainstream or opiate-dependent lifestyle, you are normal. Defining normality was particularly present in Joe’s account, who redefined the boundaries of normality several times depending on context, but near the end defined each picture as normal (e.g., the squat, shoplifting, heroin use, homelessness), even if he could not describe them as mainstream:
it’s normal, but it’s not mainstream . . . yeah only two represent that to me, that was the drugs obviously and the man (homeless man), well it represents more alcoholism. (Joe)
“Refuting” participants, by making opiate-dependent people more heterogeneous than the stereotype and widening the catchment area of normality presented in the pictures, position themselves as normal and mainstream, often explicitly, without having to reference specifics of their life:
how I live is part of mainstream society as far as I’m concerned, I don’t try to exile myself from mainstream society, that’s mainstream society saying I’m not like you. (Chris)
However, when criticizing the mainstream, “refuting” participants, much like “affirming” participants, remain positioned outside of the mainstream:
sometimes I feel sorry for them, they got a lot of stress on their boat ain’t they, got to pay the mortgage and all that. (Joe)
As mentioned, the “refuting” discourse did not refute so much that opiates became a positive experience or drug, but it was normalized. Furthermore, negative talk about opiates, rife in “affirming” accounts, was not talked about much; when opiates were talked about negatively, it was more innocuous than “affirming” accounts (e.g., “physically addictive” (Chris) as opposed to “evil” (Helen)) and was most often counterbalanced with an analogy:
heroin has never really been proved, to kill except in overdoes quantities, which is the same in everything, water will kill you in overdoes quantities. (Chris)
Methadone, however, was spoken of very negatively, again contrasting the “affirming” discourse:
methadone’s worse, it’s addictive, it gets you down, has side effects, withdrawals, umm, and, and the only reason that we get it is ‘cause they won’t give us gear to get us off it. (Kate)
Placing responsibility of addiction on factors other than oneself was less of a feature in “refuting” discourses, in part because the discourse was at a less personal, group level. Therefore, responsibility, when laid down, was often put at the feet of mainstream society as opposed to individuals such as partners or family, as in the “affirming” accounts:
people have been shoveled onto these council estates, society produces these problems, you shovel a whole bunch of people who are all addicted to the same substance in one little same area. (Chris) they make it illegal, yeah, illegal, and then arrest us ‘cause we need it, then when people try to get a job they can’t, have to steal yeah, tell people to get better then say sorry, you have to come here every day at three. (Kate)
Hypocrisy was almost inevitable when refuting the stereotypes and it was perhaps the most difficult in these moments where mainstream society’s part in opiate dependency was being described. For example, Chris portrayed a picture of people living on council estates as “all” addicted to opiates, and Kate portrayed heroin as a drug that is needed and leads to stealing, in sharp contrast to their previous statements. Kate’s comments regarding having to get her methadone script every day during working hours represents another layer to the negativity directed toward methadone as a solution to opiate dependency. The quotes, in fact, can be taken as commentary on stigmatization, something that the “affirming” and “refuting” discourses had in common along with the rhetoric regarding the status of alcohol—in fact, sometimes these concepts combined:
a heroin’s addict a heroin’s addict umm, it’s acceptable to be an alcoholic but it’s not acceptable to be a heroin addict, but umm, I, both cost the same, how many heroin addicts would we have and how many alcohol addicts? Remove the stigma which one’s more dangerous? (Chris)
Conclusion
The present study therefore aimed to explore how people who are currently dependent on opiates conceptualize mainstream and opiate-dependent lifestyles using a Think-Aloud procedure. From the analysis, two discourses could be seen within the data relating either to affirming or refuting stereotypes which can be understood with a grander discourse concerning normalization. In particular, some participants illustrated an affirmation of mainstream and opiate-dependent stereotypes, which appeared to defend the participant’s notion of self, making them blameless and defending their image. In contrast, some showed a refuting defensive discourse which involved re-organizing and challenging the realities presented by the stereotypes. These “affirming” and “refuting” discourses in essence served the same defensive function—that of normalization, however, while the “refuting” discourse worked on more of a group level, for example, by blurring the boundaries between mainstream and opiate-dependent lifestyles, the “affirming” discourse worked on a more personal level by placing the individual outside of the opiate-dependent stereotype.
Mostly, then, data indicate that people with an opiate-dependency have a need to be seen as, and treated as, an individual, three-dimensional human and not as a grossly negative stereotype. This need could be triggered whenever mainstream versus opiate-dependent identities or stereotypes become salient. These results have implications for the ways in which this population could be approached and illustrate possible barriers and facilitators for uptake and involvement in rehabilitation. First, in terms of how this population could be approached, the results from the present study indicate that what these clients actually say may not be a direct reflection of what they think but more an illustration of a presentation of their self which is defending against existing stereotypes. When deciding to engage with a drug program, these identities may become particularly salient as they are being confronted with the norms of mainstream society. Therefore, the ways in which clients in the drug service relate their life circumstances and how they would like to move forward may not present true and concrete versions of reality, but rather their constructions may be borne out of need to be seen as a normal individual. Accordingly, those working with this client group should be aware of this need to be defensive and attempt to offer a supportive, empathetic, and non-judgmental relationship to help lower such defenses so that more productive work can take place.
Second, in terms of potential barriers to the uptake and engagement with support, the results also highlight some implications for practice. In particular, the “refuting” discourse involved minimizing the negative consequences of opiate dependency, while emphasizing the negative consequences of mainstream life; specifically, methadone was labeled negatively and opiates were constructed as a more controllable drug. This construction may make it more likely that clients slip back into an opiate-dependent lifestyle, or even less likely to enter treatment in the first place. Similarly, the “refuting” “slave wage” construction of mainstream reality may signify that attaining secure employment is less likely. Therefore, those working with this client group need to be prepared to challenge this “refuting” discourse, while recognizing the need for normalization. However, this will not be an easy task given the level of functions that this discourse serves.
Third, it is possible that the “affirming” discourse may signify positive outcomes in terms of abstinence and integration into mainstream society with an associated better quality of life. Therefore, it may be beneficial to vocalize agreement with mainstream stereotypes for the purpose of interacting with mainstream members and institutions as it does not cause tension or upset the status quo and will be less likely to be interpreted as defensive.
There are several limitations to this study which need to be considered. First, participants were on a methadone maintenance program and so the discourses produced, and their hypothesized consequences, may not generalize to those who are not seeking treatment or indeed to other people on a methadone maintenance program, given the sample size. Also, the potential consequences of the discourses are just that—hypothesized. Future research, preferably quantitative, is needed to establish whether there are any significant consequences and to suggest helpful solutions.
To conclude, the results from the present study indicate that participants dependent on opiates relate to stereotypes of mainstream and opiate-dependent lifestyles in ways that normalize their past and current positions in society. Accordingly, whether they refute or affirm the stereotypes presented, they do so in ways to protect and defend against their notions of selves. Most treatment programs for opiate dependency offer a solution to any client’s behavior by encouraging a shift away from the opiate lifestyle toward a more mainstream way of living. The results from the present study not only provide insights into how those with opiate dependency conceptualize these two lifestyles but also highlight potential barriers and facilitators that need to be addressed if this shift in behavior is to occur. In particular, the results highlight a need to understand the defensive nature of the rhetoric used and that while affirming discourses may facilitate recovery refuting discourses could act as a barrier.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.