
Abstract
The major subject matter of the proposed article is the gap between global value of health and its practical implementation in the form of actual daily practices. The article addresses the concept of health in contemporary society and claims healthy lifestyle ideology to be the essence of contemporary health culture. Thus, this ideology is discussed as a basic framework proposed by the modern discourse with respect to body practices management as it builds up its logic of practice. Meanwhile, health-oriented lifestyle is considered to be a practical logic derived out of it. The author shows that there are four types of interconnection between the logical practice and the practice of logic, whereas health-oriented lifestyle is one of them. The article aims to demonstrate that health-oriented lifestyle concept in its visionary ideal form is quite far from being a practical guide for daily human behavior. Human beings are not ready to fight all their affections although they know much and sometimes they feel they can do much. This means that the basic ground for an evident discord between the high value of health and its practical incorporation into daily activities of concrete individuals lies in the field of physicality matters and civilization’s disability to manage them.
The Constitution of the World Health Organization (WHO, 1946) states, “The enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being without distinction of race, religion, political belief, economic or social condition.”(p. 1) Based on this statement, health may be attributed to a range of underlying human values. And, indeed, it can be treated as a basic resource whose quality determines the usefulness of human life and the nature of individual’s participation in social life. But when we take into account the sociocultural side of health phenomenon, it becomes clear that at different stages of social development there were different health discourses, or historically variable types of health culture. The defining set of health factors, health definition itself, as well as the general value of health had been changing over the pass of epochs. Throughout civilizing process, the idea of health as a completely deterministic external condition (health as a faith) changed by the vision of health as a result of each individual’s personal choice. Initially, the responsibility for health fell on various natural and supernatural forces of exogenous nature; however, modern society tends to blame individuals and their lifestyles for what is happening with their health. For instance, according to a modern point of view, individual health is by 60% dependent on the lifestyle (Lalonde, 1981). Figure 1 illustrates this vision with respect to health risk factors admitted by the WHO.

The risk transition: Over time, major risks to health shift from traditional risks (e.g., inadequate nutrition or unsafe water and sanitation) to modern risks (e.g., overweight and obesity; World Health Organization, 2009).
Admittedly, modern people by themselves tend to assume that they really do influence on the way their lives go. For instance, the latest available European Value Study (EVS) data show that more than 58% of people gave the Score 7, 8, 9, or 10 when answering the question “How much control over your life?” where 0 meant “none at all” and 10 stood for “a great deal” (European Value Study Wave 4 Data, 2008).
Moreover, contemporary health discourse tends to position health as a great value in its temporal sense that makes health valuable as a thing in itself. Whereas globally accepted definition of health is extensively generalized, 1 health gains the status of the highest point of human well-being and self-realization.
Thereby, the concept of health, as problematized in frames of contemporary cultural discourse, is closely related to the notion of lifestyle. Notwithstanding the fact that the value of health can be treated as somewhat significant in any kind of society, and some researchers even tend to treat health “as natural, absolute and perpetual life value” (Shapovalova, 2007), considerable discrepancy between the global value of health and its practical incorporation into daily activities in the form of an important lifestyle element can be observed. The purpose of this article is to analyze the nature of this inconsistency and to develop a solid explanation for its viability. At that, the logic of our cogitations will be as follows. First of all, we are going to distinguish between healthy lifestyle ideology and health-oriented lifestyle by means of using the concepts “the logic of practice” and “the practical logic” of health culture in contemporary society. Then, we are going to appeal to some empirical evidence to demonstrate how these concepts reveal themselves in real life. For healthy lifestyle ideology of contemporary society, we will address to the latest available European Social Survey (ESS) data, and for health-oriented lifestyles (or their opposites), we will turn to WHO Reports. Thus, we intend to show how ideology is constructed to make people adhere to healthy lifestyle principles and what is the problem of its transformation into health-oriented day-to-day activities.
So, the logic of practice is understood as the condition of operation and the principle of structuring for practical logic, while practical logic, in its turn, enables the actors to perceive the logics of practice, to judge, and to act (Schäfer, 2009). As far as lifestyles are sets of practices and attitudes that make sense in certain contexts (Chaney, 1996), we are going to discuss the context of healthy lifestyle and after that, the lifestyle itself. With respect to our subject area, the healthy lifestyle ideology will stand for the logic of practice, whereas health-oriented lifestyle will represent the practical logic.
Generally, the major distinction between healthy lifestyle ideology and health-oriented lifestyle is quite transparent—that is, the distinction between the idea and its practical embodiment. Nevertheless, it is important to provide more sophisticated and deep-root explanation for differentiation between these concepts. Lifestyle points at steady forms of personal behavior that are the result of free choice making in frames of field-dictated limits; it is the personal way to solve social system antagonisms (Beck, 1992). Lifestyle represents an absolutely modern form of status differentiation, which implies that status is derived not from the occupation or a certain set of individual privileges but from the way these privileges and resources are used individually. Many people, in particular, choose their occupation and the way of its organization based on its compatibility with their personal lifestyle values (Chaney, 1996). Thus, we can assume that individual choice is a very important aspect in conceptual reflection of lifestyle as a notion. Using Ionin’s (2000) expression, “the style can exclusively be present only where the choice is present” (p. 195). Consequently, the social role, or the free behavior choice pattern, is the lifestyle’s molecule. The style is a typical choice in frames of possible. As we already made it clear, we are going to analyze the healthy lifestyle as the logic of practice and a certain ideological field that offers its consumers a set of principles and directions toward practical actions with respect to their body and health. Let us consider it closer.
Healthy Lifestyle Ideology: Politics, Market, and Branding
First of all, it should be mentioned that healthy lifestyle ideology in its general global meaning is indeed formed under the dictation of real medical statistics: In contemporary world, the main mortality factors are disorders associated with the way people live their lives. Thus, according to WHO data, 10 major mortality factors among world population are (WHO Official Site, n.d.; see Figure 2). 2

The leading causes of death in 2008.
We can distinctly see that so-called “civilization diseases” (chronic and degenerative disorders) start to fulfill the top places among human death factors. These diseases increasingly depend on the lifestyle that one chooses, and on the quality of one’s life as well as on one’s ability to use the available resources of own body strategically and demonstrate self-reliable orientation toward health during one’s personal lifestyle.
In general, healthy lifestyle criteria are quite simple and exhaustive: The list of indicators to assess the level of personal deduction for everyday health care includes dietary inclinations, physical activity, and unhealthy habits (Kіnger, 2005). In addition, workplace conditions, public and domestic violence, reproductive behavior, and so on can be taken into account (Huss-Ashmore et al., 1992). These are the basic healthy lifestyle principles, which can be found throughout the whole space of social interactions—from school and university textbooks (in Valeology, Principles of personal and social safety, etc.) to political programs.
Healthy Way of Life As a Matter of Social Politics
The issue of health as a matter of state politics (biopolitics) can be effectively illustrated by means of Foucault’s principle of state power efficacy, which is based on simultaneous generalization and individualization. It turns out that, in general, health is a personal decision of an individual, and at the same time, it is the question of national importance. Thus, we can observe panopticon effect in action, when control over the members of society is very successfully implemented in a latent way, and to a large extent they act as controllers. At the end of the day, the health care system becomes a religion of modern society. Through the establishment of “uncertain normality” discourse, only few can be treated as healthy, and everyone, in fact, becomes a potential patient, which means entering the field of control, risk assessment, and external (state) intervention (Kevin, 2007). Some researchers go even further by stating that public health policy is actually a program of social control packaged in a wrapper of healthy lifestyle idea promotion. The idea here is in an unprecedented self-control at the cost of provoking public excitement increasing resulting as an effective system of individual behavior regulation (Fitzpatrick, 2001). They even talk about contemporary death of humane medicine and the rise of coercive healthism (Fitzpatrick, 2001).
It is important to state that we are not giving here any assessments of healthy lifestyle ideology as a political issue. We are rather trying to find its place in frames of political system. It is obvious that healthy lifestyle ideology does not exist as an independent database of health state factors and ways to maintain good health. It rather finds direct expression in state national legislation promoting everyday health-focused behaviors among general public. For instance, Article 32 of the Law of Ukraine “Basic Law of Ukraine on Health Care” proclaims the following: The State shall promote the establishment of healthy way of living by means of spreading scientific knowledge about health, medical, environmental and physical education organization, implementation of activities aimed at improving hygienic culture, creating the necessary conditions, including medical monitoring of physical training, recreation and tourism, development of medical and athletic facilities, dispensaries, recreation centres and other health facilities to combat health habits which are harmful for human, establishing a system of socio-economic incentives for individuals adopting healthy lifestyle. Ukraine has made public policy limiting smoking and alcohol consumption.
Ukrainian legislation, in general, requires from its citizens taking care of their personal health: The Article 11 of the Law of Ukraine on Health contains the following clause: “Citizens of Ukraine ought to take care of their health.” The question of real force of this clause is just another one, as it is clear that no one (at least for now) recovers fines and puts behind bars for overeating, lack of sleep, or lack of physical activity. However, in some countries, the attempts to introduce a practice of tax on unhealthy lifestyles already have been made. Italian Health Ministry wants to introduce a tax on soft drinks and alcohol (O’Leary, 2012)—several countries, including Hungary and Denmark, have implemented nominal “fat taxes” on unhealthy foods; France has an extra tax on sweetened drinks; Peru plans to implement a junk food tax in coming months (Koebler, 2012); and Arizona authorities want to tax smokers and obese people (Forer, 2011). Monique Currie, the deputy director of the state Medicaid office in Arizona and one of the advocates of this initiative, said as follows: If you do not want to change your life and take responsibility for your health, which ultimately leads to public spending, then you will have to participate in co-financing. You must take responsibility for the fact that your smoking costs us a round sum.
Moreover, WHO, as it is stated in the latest Watch Report on the 65th World Health Assembly, should provide technical support and expert advice to member states on the implementation of fiscal, legislative and regulatory measures to improve food and nutrition. This should involve technical support to finance ministries on the administration of national food tax and regulatory systems and administration, as well as the production of manuals and toolkits. (WHO Watch Report on the 65th World Health Assembly, 2012, p.14)
At this point, as we already mentioned, we are going to refrain from evaluating political programs and social policies with regard to health behavior promotion at whole. In the long run, our task here is to show the key role played by the healthy lifestyle phenomenon in modern sociocultural discourse at the level of political organization.
Healthy Way of Life As a Matter of Market Strategy and Branding
In frames of market economy, we can consider health and healthy lifestyle as power brands and elements of an exceptional new philosophy that is sometimes called “wellness philosophy.” According to expert estimations, the healthy lifestyle industry, which recently was just at the level of infancy, promises to be a new billionary industry the next decade. Today, the wellness market is compared with the high-tech sector in terms of capital turnover. The worldwide annual turnover in the industry, according to the analysis of the famous American businessman and economist Paul Zane Pilzer, is about 425 billion U.S. dollars. The researcher notes that in 2000, Wellness industry in America has already been the one with sales up to 200 billion U.S. dollars, and about a half of that amount was spent on sports clubs and 70 billion U.S. dollars on vitamins and minerals (Pilzer, 2001).
Indeed, today’s society market can be the first to react on public needs for meeting the aspirations to lead a healthy lifestyle. It makes a huge amount of package offers that can provide a person with a possibility to buy healthy (organic) food, visit gyms, health clubs, beauty salons, spas, and so on. The proportion of people willing to make substantial investments in their health grows very fast. According to the German economic research institution “Global Insight,” 47% of people aged from 20 to 30 suggest that they actively use the means to maintain personal health (Bayram, 2008, p. 28).
Thus, the market eagerly turns the idea of healthy lifestyle into the industry of savory versions, a plethora of public and commercial broadcasting programs (and books) designed to make science, technology, or philosophy of health accessible to the “average man” (Allen & Anderson, 1994, p. 4). That is an easy way to make healthy lifestyle a fashionable and stylish trend. In modern world, everyone is in rush for health. The notion of healthy lifestyle has already gained the archetypical traits. Advertising companies use this widely to make different products more attractive to public. Table 1 shows the list of slogans, used in advertisements presented all over the world All of them tend to dramatize the health phenomenon.
List of slogans used in advertisements.
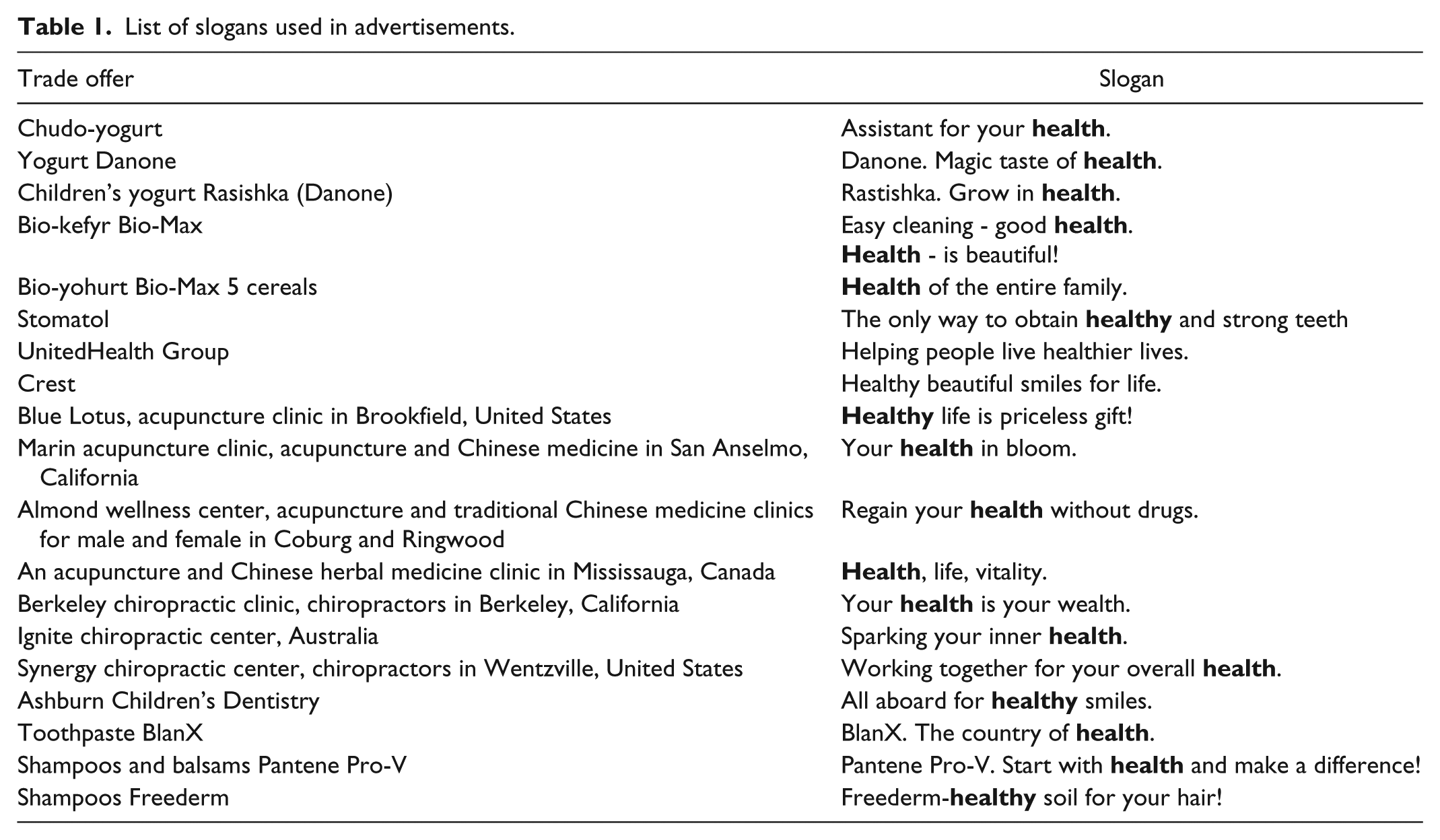
To that we can also add that even such unhealthily viewed brands as Coca-Cola are trying to join the ranks of healthy lifestyle ideology. In the 1980s, Coca-Cola used the advertising slogan “Have a Coke and a Smile” to boost sales. These days, it is more like “Have a Coke and Hit the Gym.” And the head honchos at Coke have revamped the brand’s advertising, with a focus on how to incorporate Coca-Cola products into a healthy lifestyle (Breene, 2013).
Health-Oriented Lifestyle
So, we have shown that healthy lifestyle is an ideology that is the general logic of practice open for various kinds of practical embodiment. Now we can go further to the analysis of the practical logic itself. The interconnection between the logic of practice and the practical logic is such that the first serves as the source for knowledge and means necessary for the second. Hence, we have purposefully split the concepts of healthy lifestyle and health-oriented lifestyle. Healthy lifestyle is seen by us as a kind of cliché that can hide or mask various aspects of health as a sociocultural phenomenon. Meanwhile health-oriented lifestyle is the practical implementation of healthy lifestyle idea in a specific biographical situation.
First of all, when talking about health-oriented lifestyle, we should mention the aspect of personal choice embedded into actions that constitute it. This leads us to recognizing it in frames of intentionality, meaning that health-oriented action can be broadly defined as the intentional and reflective activity that has been consciously thought out and aimed at a specific target (Verlen, 2001). Here, of course, we are talking about health as such a target. Taking this intentionality aspect into consideration, we may typify health-oriented lifestyle as a recommended act (as opposed to those allowed and forbidden; Sorokin, 1992). Indeed, health orientation in everyday practices is often viewed as a kind of above-normal activity that is not usually demanded, being although highly desirable. Such behavior is certainly being endorsed by different means and, moreover, may be seen as a feat. An individual showing intentional focus of his or her lifestyle on health may be perceived as being largely self-limiting, abstaining from various “unhealthy temptations” and getting a reward for it in a form of certain positive image in public eyes. Health-oriented lifestyle choice entails a number of “awards” on its bearer. Except the health itself, an individual following healthy lifestyle is seen as a model of organization, discipline, purposefulness, responsibility, strong will, and even more. He or she is capable of making an effort, consciously “signing” under the constant hard work on himself or herself.
Our understanding of the sense hidden under the concept of health-oriented lifestyle can be widened by means of involving some ideas initially proposed by Habermas in frames of his social action theory. Thus, according to him, there are four types of social action: strategic (utilitarian), normative (similar to Weber’s value-rational action), dramatic, and communicative action (Habermas, 1984). If we analyze the various types of relation to health and corresponding actions determined by it, we can talk about the following. Strategic behavior toward health stands for the egocentric not too far-sighted actions of individuals aimed at getting fast results (when people become concerned about health in terms of short-term profit which is, in fact, a symptomatic treatment not reaching the essentially of the problem). To some extent, this type of action is purely technical and temporary, not related to an attempt to implement a comprehensive revision of the general life strategy behavior; when health is really threatened, the person is ready to take care of it in a disciplined and responsible manner. However, when health is normal, the need for daily (prophylactic) reproduction of health depreciates sharply, health resources start to be confined, yielding in a hierarchy of motives to other factors such as getting pleasure, building a successful career, and so on. Normative action reflects noninternalized attitudes, which means that under other social circumstances, such as the absence of coercion or other external influence, a person would not adhere to certain principles of a healthy lifestyle. A striking example of such kind of activity is the way of life of many children and teenagers. Until they are under elder control, they are normally fed, they follow optimal sleep and rest regime, and generally do not resort to bad habits, but in case of the absence of control they willingly violate basic principles of a healthy lifestyle. Such kind of behavior is inherently infantile as it desperately lacks self-reflection. This means that a person imitates a lifestyle imposed on him or her by someone else and, accordingly, would not necessarily adhere to it in other context. Dramatic action, in this context, expresses human desire of self-representation, the will to be in the center of the most fashionable trends with regard to a healthy lifestyle (fashion for physical activity, organic food, natural personal hygiene and household products, etc.). The actual health-oriented lifestyle, to our opinion, is the one representing communicative activity that is the one associated with a high level of self-reflection and long-term prospect; lifestyle-oriented health, in other words, is a lifelong strategy. Depending on the length of individual’s life perspective in relation to own health, and also on the type of emotional commitment, all types of actions can be placed on an integrated axis of coordinate (Figure 3).

Types of actions.
The visionary aspect of health-oriented lifestyle can be brightly illustrated by Piaget theory of cognitive development. Health-oriented lifestyle may be regarded to as a kind of final stage (the highest point) of individual development representing a well-established striving to a steady state of dynamic equilibrium. At the “sensorimotor” stage, a person learns to read the signals of own body, and during this period, the main type of activity is strategic that is reducing unpleasant (painful) sensations and maximizing of pleasures. “Preoperative stage” corresponds to normative behavior. At this stage, a person has to take certain patterns of behavior for granted not passing them through his or her own conscious mind. “Operational stage” turns on self-reflection process in a person, but it does not awaken awareness of the importance of certain actions in the long-term prospect. And finally, on the “stage of formal operations,” a person develops the rational structure of thinking. It provides an individual with an opportunity to understand the symbolic value, use abstract strategies to understand the hidden meanings, and make general conclusions in the context of the development strategy of his or her own life in terms of health.
Thus, we are talking about health-oriented lifestyle as a daily production of individuals’ health. This means that virtually any everyday person’s activity is being correlated with its possible impact on health. That is what may be referred to as self-sufficient type of health orientation (Bredikhina, 2006), when a person operates with a sufficient knowledge about health and actively implements the principles of healthy lifestyle ideology in his or her everyday practices. Self-sufficiency in health orientation is the grounding foundation of health-oriented lifestyle formation. Its basic principle is preventive character of actions related to health. That is reflected in the idea of a strategic management of health as a finite resource accompanied with individual orientation toward long-term outlook and total correlation between all the aspects of vitality and possible health risks.
Another important dimension of health-oriented lifestyle is the matter of conscious lifestyle choice. Otherwise, the whole idea would be a substitute, mere fashion following, a forced temporary measure, a compromise with oneself on the basis of self-deception, and so on. Actually, we are talking about the health-oriented lifestyle choice as “the heroic pass,” provided with a high level of awareness and responsibility, as well as making a constant daily choice while fighting with two basic neurotic obsessions of mankind that are laziness and fear (Kozlovskij, 2011).
Admittedly, health-oriented lifestyle, generally speaking, is not a very enjoyable way of existence, which is not surprising, as “any kind of awareness multiplies suffering” (Kozlovskij, 2011). It is much easier to go with the flow, putting the whole set of responsibility for one’s own health on poor heredity, environmental pollution, and bad health care and living conditions, promoting the enjoyment motto, “We all are going to be there sooner or later.” Opposed to that, adherence to health-oriented lifestyle is about self-improvement and self-commitment; thus, it demands a huge set of efforts. This involves investment of time as well as socially constructed forms of attraction with all the conjugated limitations, self-denial, and self-sacrifice (Bourdieu, 2002).
Doubtlessly, that is what constitutes the ideal (visionary) practical logic. It is hardly that much commonplace when we shift our attention to empirical reality. The latest usually dazzles with a vast range of destructive practices of all kinds and forms—from poor eating habits to high levels of alcohol and drugs consumption. The following data (see Figure 4) show some figures on prevalence of these unhealthy activities and their consequences worldwide (WHO Statistics, 2013).
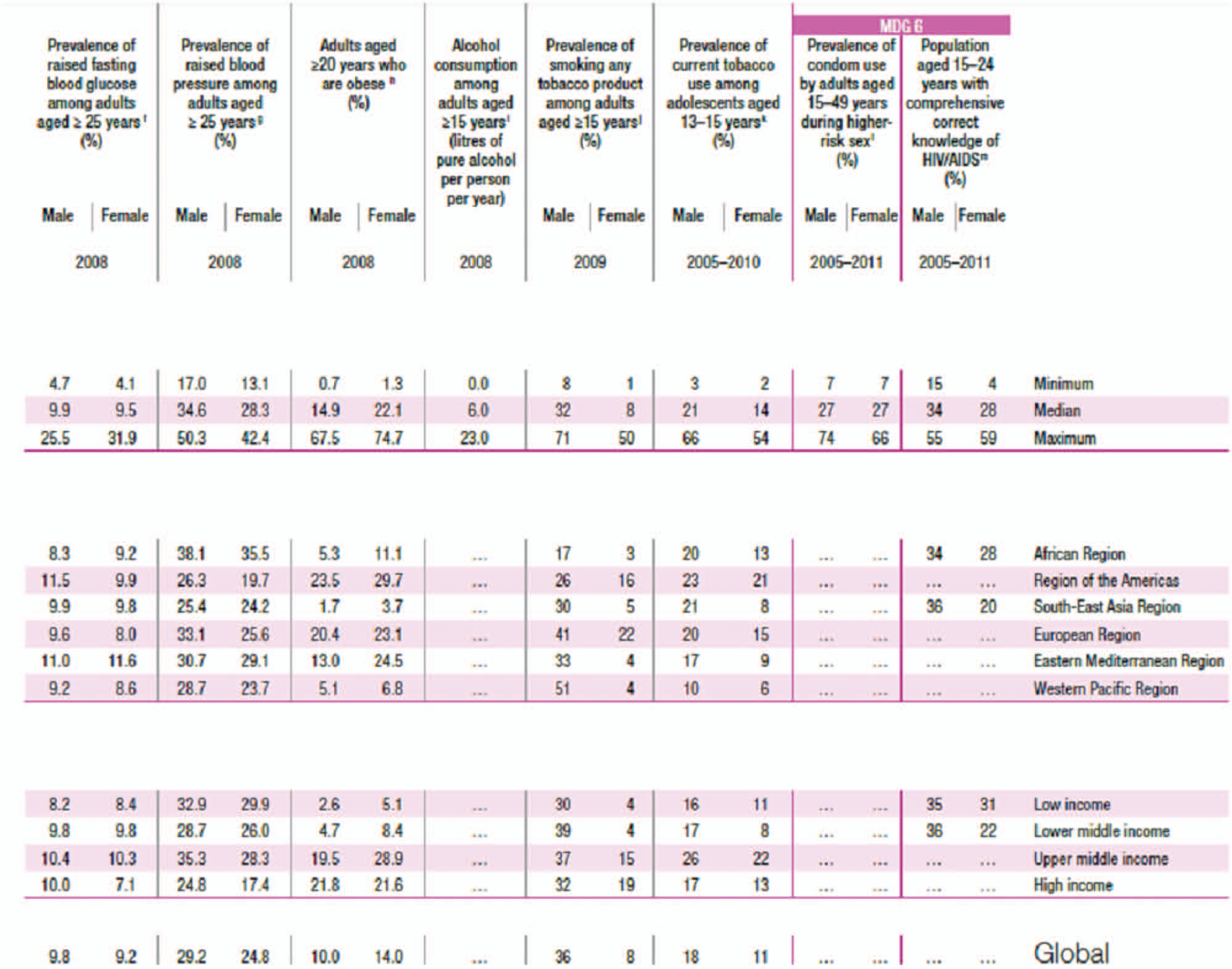
Risk factors (WHO Statistics, 2013, p.117).
And here is WHO projection on what is going to happen if people continue to live like they do now (Figure 5).
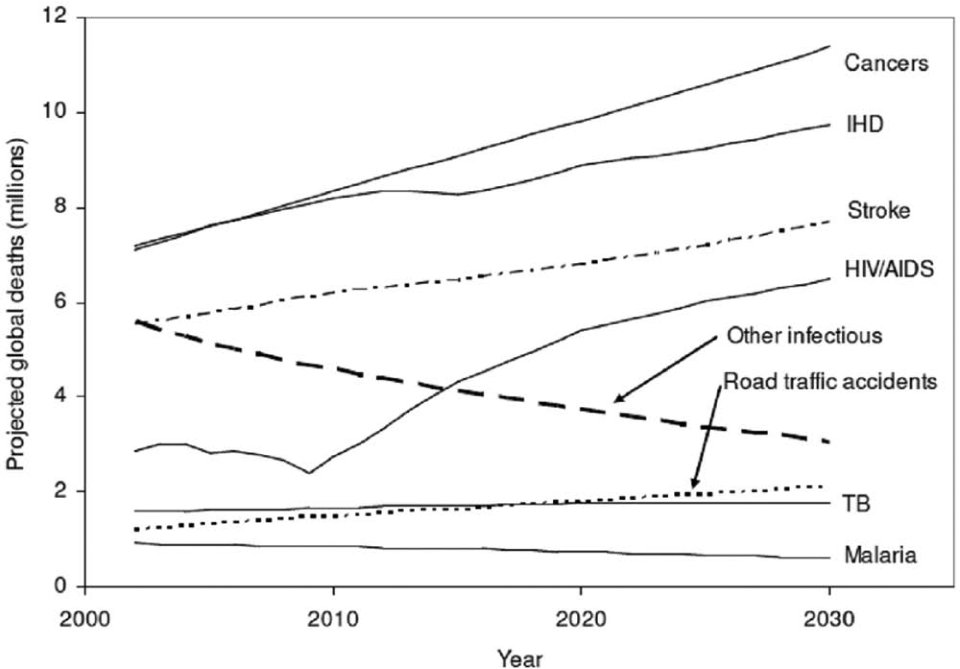
Projected trends in total deaths for selected causes, baseline world scenario for 2002-2030 (Mathers & Loncar, 2005).
We can see that the interconnection between the logical practice and the practice of logic is quite compound. Here, we were talking about four types of that interconnection, namely, strategic, normative, dramatic, and communicative types of health orientations. We also stated that only the latest can be seen as pure health-oriented lifestyle. So here we are getting close to the question why this visionary highly valuable and truly beneficial strategy for organizing life does not become a commonplace reality for majority of individuals. We believe here that the main reason for that is rooted deep into cultural codes of Western civilization. According to Elias (2000), civilizing process is about moving toward greater suppressing and controlling of the affective side of human identity. Still, the problem is that notwithstanding all the civilizational efforts to bring the physicality under control, the body keeps dictating its own rules: All kinds of dependences, emotional or physical, mild and severe, are manifest illustrations for this. Thus, civilization progress, being significantly successful in bringing more instruments for rational control and providing mass population with the necessary knowledge and means for control over physicality, has to face that the latter still is too strong. After all, physicality is much more “experienced” in comparison with “modern ratio.” The thing is that body is a field for direct implementation of any general healthy lifestyle ideological principles. And the problem hidden beneath that is body’s own rules of functioning that often lead a person toward gaining momentary pleasures without assuming his or her later consequences. Thus, people really have a high value of health and they usually understand the set of basic principles of healthy lifestyle but they still WANT to get pleasure. Although there was no target international research that could corroborate this thesis, we can demonstrate the ambivalence between cultural and affective by means of existent ESS data (Figure 6).

Human values block from the ESS5 (2010) Edition 3.0 data (European Social Survey Round 5 Data, 2010).
We can see here that those culturally driven values (like importance to follow traditions and customs, to follow the rules, to behave properly) do not confront with the value of freedom and craving for hedonistic values (like importance to seek fun and pleasure, try different things, and have a good time).
Thus, even within the social sciences, one should consider the physicality in the sense that, despite the general civilization tends to “curbing affections” (Elias, 2000), the body continues to dictate its own terms and conditions, often not even allowing the consciousness to enter the decision-making process.
To summarize, we can conclude that healthy lifestyle ideology, which is embodied in politics and economy, is not that easily transformed into health-oriented lifestyle. Eventually, we have ascertained that a lifelong adherence to health-oriented lifestyle is really challenging and hard, which can be an additional reason why a wide range of destructive practices are there in the place. However, the main reason, as we put it, lies in the milieu of civilization’s incapacity to curb physicality and its affections. As long as civilization largely puts this responsibility on personal choice and lifestyle decisions, individuals find themselves stuck between integrated knowledge about health and healthy lifestyle and their emotional strivings and desires for obtaining pleasure (which too often, although not necessarily always, tend to be not that healthy). Taking the fact that short-term gains tend to prevail over long-term benefits into consideration, the body usually wins. Moreover, we pointed out that there is a certain underrepresentation of physicality matters (as determinants of human behavior) in social sciences and in modern health discourse at large. The thing is that civilization, despite its general tendency to fight for human health, simply cannot afford raising individuals who would be deeply concentrated on filling their bodies with mindfulness in frames of communicative health-oriented lifestyles. At long last such people would rather be ascetics than social beings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.