
Abstract
Lifestyle changes such as in physical exercise, social activity, and diet can mitigate cognitive decline and improve quality of life in caregivers and care recipients with cognitive impairment. However, caregiver perspectives on lifestyle change remain largely unexamined. This study compares perspectives among caregivers for those with dementia and those with mild cognitive impairment (MCI). Interviews were conducted with caregivers in two sites in China, and thematic similarities and differences were examined between the two groups. Caregivers from both groups identified exercise, social activity, and diet as healthy ways of life. Differences were found in approaching lifestyle change based on health of the care recipient. Caregivers for patients with dementia found more often that they had no time or possibility for change, while caregivers for individuals with MCI were more often hopeful about change.
Introduction
It is projected that more than 30% of the Chinese population will be age 60 or older—about 400 million people—by 2050, adding to a projected 2 billion age 60+ population worldwide (Banister, Bloom, & Rosenberg, 2010; Gu & Cai, 2009), making age-related diseases and conditions like cognitive impairment a priority in intervention-oriented research. Increasing attention has been paid to lifestyle behaviors, such as physical activity, social engagement, and diet in improving cognitive health. A growing body of evidence demonstrates the importance of physical activity (Angevaren, Aufdemkampe, Verhaar, Aleman, & Vanhees, 2008; Heyn, Abreu, & Ottenbacher, 2004; Lautenschlager et al., 2008; Lautenschlager, Cox, & Kurz, 2010) and social interactions (Bassuk, Glass, & Berkman, 1999; Seeman, Lusignolo, Albert, & Berkman, 2001) in mitigating the advancement of cognitive impairment. Physical activity also seems to provide mood benefits to individuals with mild cognitive impairment (MCI) and mild to moderate dementia (Olazarán et al., 2004).
Lifestyle-based interventions have also suggested the efficacy of such treatments for family members providing care, who play a critical role in the well-being of frail elders at home. An intervention using weekly, telephone-supervised, home-based physical activity regimens resulted in improvements in self-reported quality of sleep, blood pressure reactivity to a laboratory-based emotional challenge, and psychological distress (King, Baumann, O’Sullivan, Wilcox, & Castro, 2002). Other physical activity studies have found positive effects on caregiver sense of burden (Hirano et al., 2011), anxiety, depression, and perceived self-efficacy in controlling negative thoughts (Waelde, Thompson, & Gallagher-Thompson, 2004).
There is increasing evidence that behavioral interventions targeting care dyads can be successful. Including the caregiver as part of an intervention has the potential to offer distinct benefits for individuals with cognitive impairment as well as for the caregivers, from the perspectives of social interaction, observational learning, and social reinforcement (Kazdin & Nock, 2003; U.S. Department of Health and Human Services, 2010). A study using a tailored activity program involving long-term adherence to activities, such as making salads or listening to music, found significant reductions in behaviors, such as repetitive questioning and argumentative behaviors, and improvements in quality of life for persons with dementia (Gitlin et al., 2008). It also found objective burden, measured by caregiver estimate of time “on duty,” to be decreased by roughly 5 hr after 4 months on the intervention (Gitlin et al., 2008). Few studies have been conducted to examine the effect of lifestyle-based interventions on dementia care dyads in China. One study found that caregivers and care recipients with early-stage dementia benefited from physical exercise, with improved stress levels and relationship quality (Burgener, Marsh-Yant, & Nega, 2010).
In sum, there is consensus that physical activity and social interaction are effective ways of mitigating cognitive decline, improving mental health, and increasing subjective well-being for the cognitively impaired and their caregivers. However, though many studies examine patient perspectives on lifestyle change, the perspectives of caregivers in enacting lifestyle changes remain largely absent from the literature. As lay caregivers become integral in interventions for the cognitively impaired, understanding their preferences for and barriers to lifestyle change will shed light on whether they will accept and how well they will perform in behavioral interventions. Indeed, the efficacy of social and physical activity has been shown to be dependent on individual preference and other demographic factors, such as gender (Baker et al., 2010; Lichtenberg, Kemp-Havican, MacNeill, & Johnson, 2005). Consequently, assessing perspectives on lifestyle change from dementia caregivers is crucial to designing appropriate, effective, and acceptable behavioral interventions for care dyads. Given that frail elders are almost exclusively dependent on informal caregivers in the community setting, as well as an increasing number of elders with cognitive impairment, lifestyle intervention targeting caregivers and their care recipients is particularly important in China (Wu, Mao, & Zhong, 2009). Even small delays in the progression of cognitive decline by improving health of caregivers and care recipients may substantially lessen the impact of dementia on individuals and society.
Theoretical Frame
The transtheoretical or stages of change model (Prochaska & DiClemente, 1983) can serve as a useful model for interpreting perspectives on lifestyle change from these two groups of caregivers. The strength of the stages of change model lies in its avoidance of conceptualizing behavior change as a binary phenomenon, instead using empirical findings to attend to the temporal dimension of behavior change. This insight allows for a more nuanced understanding of how best to intervene in the “processes of change” such that individuals can progress through the stages (Prochaska & Velicer, 1997).
The transtheoretical construct typically follows six stages of change: precontemplation, contemplation, preparation, action, maintenance, and termination. Precontemplation represents a state in which an individual does not plan to take action in the future (sometimes defined as 6 months). These individuals may be underinformed or demoralized from past failures and thus do not think much about changing their behavior. In contemplation, individuals understand the benefits of lifestyle change but are also keenly aware of the challenges and downsides of change, and so remain ambivalent. Preparation marks an intention to change in the very near future (around 1 month), usually with plans to change. Action describes individuals who have recently begun to meet a criterion for behavior change. Maintenance marks a period where behavior change has been ongoing for some time, though the level of activity is not as high as in the action stage. Termination marks effortless maintenance of a particular lifestyle.
Though the stages of change model originated in smoking cessation (Prochaska & DiClemente, 1983) and has since been applied to the cessation of many negative and risky behaviors, it also holds relevance for positive behavior change such as physical exercise (Garber, Allsworth, Marcus, Hesser, & Lapane, 2007; Plotnikoff, Lippke, Johnson, & Courneya, 2010). In this article, we utilize the model’s descriptive constructs to emphasize the relationships that caregivers have with healthy lifestyles such as physical exercise, good diet, and social activity. Our definitions are the following: (a) the precontemplative stage is not perceiving lifestyle change as granting benefits, (b) the contemplative stage is perceiving benefits to lifestyle change but recognizing substantial barriers involved in change, and (c) the preparation stage is planning or foreseeing lifestyle changes.
This study presents caregivers’ key concerns about preserving cognitive and physical health. It compares views on lifestyle change and healthy ways of life for Chinese caregivers caring for individuals with dementia and those caring for individuals with MCI to address the existing gaps in the social science and behavioral literature. Compared with individuals with MCI, individuals with dementia are more impaired in instrumental activities of daily living and their caregivers are more likely to report depression and burden (Hinton, Haan, Geller, & Mungas, 2003; Leroi, McDonald, Pantula, & Harbishettar, 2012; Marshall et al., 2011). Because of these sources of difference in caregiving experience, we compare and contrast perceptions of lifestyle change in the two groups of caregivers, using the transtheoretical model to help reiterate and clarify these similarities and differences. The twofold goal of this study is to identify common influences on lifestyle change in caregivers for those with cognitive impairment in China and suggests reasons for which the perceptions of lifestyle change in the two groups may differ.
Method
A total of 36 caregivers were recruited from Chinese memory clinics in two cities, Wuhan and Beijing, in fall of 2009. Wuhan is the capital of Hubei province in central China, while Beijing, the national capital, lies on the northeastern coast. Both are major urban centers of China, but Beijing is one of the few leading cities in China in terms of finance, public services, infrastructure, and urban planning. Beijing has a population of about 20 million, while Wuhan has a population of about 10 million (Wuhan Statistical Bureau, 2011; National Bureau of Statistics of China, 2011).
After contacting caregivers referred by physicians in Zhongnan Hospital, a teaching hospital affiliated with Wuhan University, the study team recruited 21 participants (14 caregivers of persons with MCI and 7 caregivers of persons with dementia). In Beijing, caregivers who visited the memory clinic at the No. 6 Hospital, a teaching hospital with a focus on mental health at Beijing University, were approached by the study team, which included a psychiatrist and a nurse. A total of 25 caregivers (8 caregivers of persons with MCI and 17 caregivers of persons with dementia) agreed to participate in the study. Inclusion criteria for caregivers were that they were over 18 years of age and had been the primary caregiver for over 1 month. Exclusion criteria were whether they had dementia, a related disorder, or severe physical or mental disability. The protocol was approved by the Institutional Review Boards at both universities in China.
We conducted face-to-face, in-depth interviews with participants, sometimes with care recipients present. The interviews lasted 1 to 3 hr and were conducted in Chinese by two trained researchers who understood the local dialect. Informed consent was obtained and questionnaires completed. With participants’ permission, all interviews were audio recorded and transcribed. The transcriptions were compared with recordings by two research team members who understood the local dialect and translated into English by two research team members. Interview questions covered the explanatory model of the caregiver about either dementia or MCI (depending on the diagnosis of the frail elder), including etiology, symptomology, pathophysiology, course of illness, and treatment (Kleinman, Eisenberg, & Good, 1978). Questions also elicited caregivers’ health problems, and their thoughts on healthy lifestyles.
The present study looks at views on healthy lifestyles, focusing on the questions, “What are some ways of maintaining a healthy lifestyle and improving mental health”; “From your own experience, is physical exercise, healthy diet, or social activity most conducive to maintaining good health and mood”; “Which changes would be most willing to make to your lifestyle”; and “In order for you to improve your physical health or mood to better take care of the elderly, which of the following aspects would be most helpful?” Analysis of translated transcripts included coding line-by-line or paragraph-by-paragraph, and the emergence of main themes and subthemes were identified in a code matrix. Two different coders coded the same interview to ensure consensus. Descriptive statistics summarized demographic data, using statistical software (SPSS 20.0.0).
Results
Participant Characteristics
Demographic data for caregivers from Wuhan and Beijing are presented in Table 1. Though there were differences between caregivers for dementia patients and caregivers for individuals with MCI, there was no statistically significant difference across the two groups in terms of age, gender, marriage status, education level, work status, or income (p > .1 for all demographic categories). Roughly half of participants were male. Nearly all were married; most participants were spouses of the cognitively impaired individual. Most participants were retired or had been retired. Over four fifths of participants were high school graduates or higher and reported monthly retirement pay of over 1,500 renminbi (RMB, ~US $220 in 2009).
Sample Characteristics.
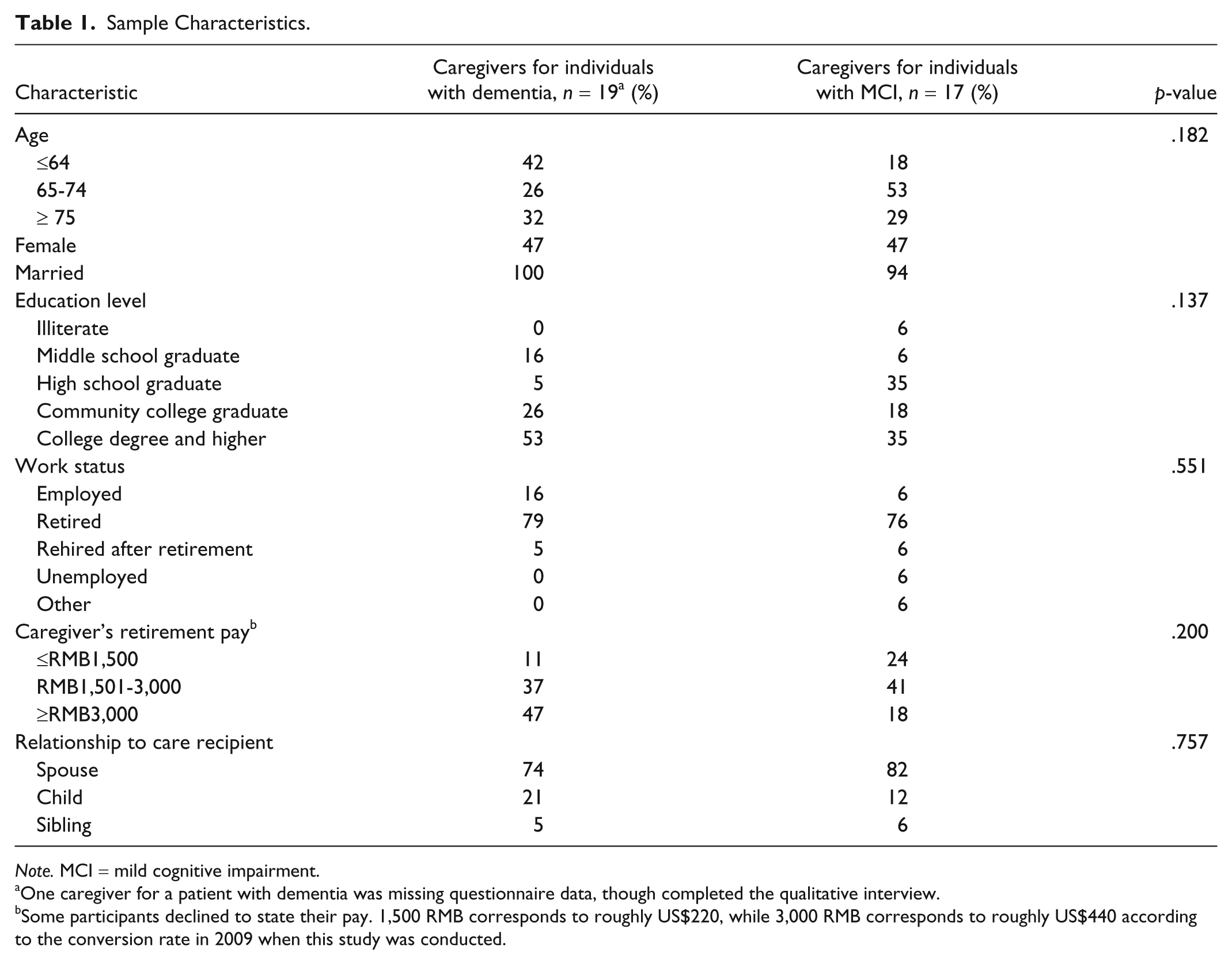
Note. MCI = mild cognitive impairment.
One caregiver for a patient with dementia was missing questionnaire data, though completed the qualitative interview.
Some participants declined to state their pay. 1,500 RMB corresponds to roughly US$220, while 3,000 RMB corresponds to roughly US$440 according to the conversion rate in 2009 when this study was conducted.
Major Themes
Caregivers for individuals with dementia and those with MCI expressed some similar and some divergent views on lifestyle changes. Views on lifestyle change that were similar across caregivers dealt with environmental barriers to lifestyle change and satisfaction with the current state of affairs. The views that differed between these two groups were grouped into three key themes—lack of time for change, no perceived possibility of change, and loss of daily activity skills. These themes are not completely separate; parts are subsumed in many of the responses given, but they have been separated here for analytic clarity.
Similarities in views
Ways of maintaining health
When asked whether physical exercise, social activity, and diet were relevant in maintaining a healthy lifestyle, caregivers agreed that some or all of them were relevant. For example, a caregiver for an individual with MCI from Wuhan said, “I do [know some ways of maintaining health], like to do more physical activity, exercise more, keep a mainly vegetarian diet, can’t eat too much meat and greasy food, or one will have poor health.” As the quoted caregiver shows, most caregivers mentioned multiple ways of maintaining a healthy lifestyle when they were prompted to do so.
Tallying codes from the qualitative interviews revealed that that over three fourths of caregivers agreed that physical exercise (taking walks, practicing Tai Chi, or dancing) was a way of maintaining health. Forty percent of caregivers for individuals with dementia regarded diet as important, while 71% of caregivers for individuals with MCI mentioned diet as a significant way of healthy living. Thirty percent of caregivers for individuals with dementia and half of caregivers for individuals with MCI regarded social activity as important for maintaining health. There were no statistically significant differences in the proportion of responses between the two groups of caregivers. Responses from the interviews related to diet, exercise, or social activity as ways of improving health are summarized as proportions in Table 2.
Perspectives on Types of Lifestyle Change.

Note: Table was compiled from coded responses to interview questions regarding their knowledge of ways of healthy life, the most conducive method to maintaining health and mood, and their views on potential lifestyle change. (p-value for χ2 for three categories = .574). MCI = mild cognitive impairment.
Aside from physical exercise, diet, and social activity, caregivers also spontaneously mentioned music and reading as ways of maintaining health in the interviews. Four caregivers (11%) mentioned listening to music, singing, or playing music as ways to improve or maintain health. Three caregivers (8%) mentioned reading, either online or in print, as ways of having a healthy lifestyle.
Environment
Living condition and comorbidities can be important for the prospect of lifestyle change. A caregiver for a care recipient with MCI in Wuhan, Mrs. A, expresses her disappointment: “Sometimes I want to exercise a little more, but I live on a high floor, and my lower back is not good, so I rarely go outdoors.”
A caregiver of a dementia patient, Mrs. B, acknowledges the personal importance of environment. Mrs. B stresses that “if there are beautiful natural surroundings, the air is good in a clean place, people’s feelings are better.”
Everything is good, there’s no need to change
10 of 37 caregivers (27%) stated that there was no need for change. Caregivers for patients with dementia and MCI determined that they did not want to change because they were satisfied with their current situation. For example, a caregiver for an MCI patient in Wuhan, Mr. C, says, “I have not fully considered changing my way of life. I feel the current situation is quite good.” At the same time, Mr. C mentioned the limitations of the efficacy of drugs earlier in his interview, and admits that the status of his wife, and therefore his way of life, “can only slowly improve.”
A caregiver for a dementia patient in Wuhan, Miss D, says, I feel that my arrangements are quite good, and don’t want to change anything; this disease does not have effective medications to begin with; passing the days like now is fine. Other people say that I care for him quite well.
Differing views between caregivers for individuals with dementia and those with MCI
No time for change
Caregivers for patients with dementia (3 of 19) described having no time as a major barrier to making changes to their lifestyle. Mrs. E from Beijing is a caregiver for her spouse, a patient with dementia, who relies on her to help him with some—but not all—daily tasks, such as preparing his medicine in the morning or accompanying him on walks. The couple also converse with each other in Russian to try to raise the care recipient’s cognitive level. Mrs. E feels that she is too preoccupied with her “family issues” to make significant changes to her way of life.
I want to change, but I think that because of my family issues I feel there is no time. Don’t have that energy.
What kinds of lifestyle changes are you willing to make?
Just, I should worry less about my family issues, and I should worry less about things in general. [. . .] Right now, there is difficulty. I just should care less about my family issues.
Due to her family issues, Mrs. E finds it difficult to add to or improve her daily routine with increased exercise, social activity, or even better sleeping habits. In fact, due to those family issues, Mrs. E admitted that her Russian sessions with her husband “do not go very smoothly. [. . .] If we persist for a period of time, if there is a family issue, then we can’t go on.” The sole way that Mrs. E finds to combat her problems is to “worry less.”
Family obligations that take precedence for caregivers are not limited to caring specifically for the care recipient. A caregiver from Wuhan worried that she might not have time for physical exercise after her children send her grandson to her home.
In contrast, Mr. F, a caregiver for an MCI patient in Beijing, was responsive to suggestions for lifestyle changes. No caregivers with MCI cited not having enough time as a barrier for adopting lifestyle changes. Whereas Mrs. E feels that she has no time for change, Mr. F concurs enthusiastically with prospects of lifestyle change for his wife. When asked about plans for the future, Mr. F says, After you are done seeing her, see if you guys have any measures. I hope that she can change some ways of life. For example, having fun is okay, but not too much fun. For example, often going out to play, taking walks, relax, interacting more, building some responsibility.
Mr. F in fact has a clear picture in mind for the improvements for him and his wife. His problems are not of time and energy, but persuading his wife to enact those changes with him. Mr. F’s wife often disagreed with him, interjecting and at one point saying she does “not like to listen to him say things.” She emphasized her past skills in cooking and working, contrasting this with his negligence toward the family while he served in the 39th Army. Mr. F concluded the interview by repeating what that he hoped “you guys” (the interviewers, representing medical expertise) could persuade her to change.
Possibility for change
Three caregivers for individuals with dementia stated that there was no possibility for change. One caregiver from Beijing expresses these considerations on her ability to change her lifestyle: There’s no way to change it. It can only be changed when I finally make the decision to send him to a residential care facility for elders. Even then I don’t have high regard for it. And it might not even be better than now, could even not be as good as now.
The above caregiver views the admission to a residential care facility as an eventuality, despite its inconvenience and strangeness. “I think that in the end we will go, but I think that we should postpone this as much as possible, you know?” Another caregiver for an individual with dementia, also living in Beijing, expressed similar worries.
How can I change my lifestyle? There’s no way to change it. Because she has a disease, I must care about it. This is for sure. If my burden can be relieved, that would be best. If not, then I will support myself. About it affecting my own health, I have anticipated it. This is also a worry. I anticipate that if she is there for a long time, my health right now is quite good, but it will decline. That is fate, nothing else.
She goes on to suggest that a full-time nurse working in her home could be a solution.
The notion that health and cognitive decline with aging is common was subscribed to by caregivers for dementia patients as well as individuals with MCI. However, these notions produced less worry among MCI caregivers; none of them said they could not change as opposed to the two caregivers above. A husband of a woman with MCI in Wuhan shows that despite maintaining traditional cultural approaches to aging, caregivers sought new ways to change. He says, “due to getting older. . .we’re now not as able as we’d like, so now it’s only possible to make improvements in diet; if we can get this kind of help it would be very good.” The son of a MCI care recipient in Wuhan, explicitly states that memory loss with age represents the “laws of nature,” and that the caregiver’s own age is related to his physical weakness, as sometimes, helping his father traverse the staircase becomes difficult. Despite this, he “hopes to improve diet, get professional guidance, and exercise more.”
Daily activity skills
Mr. G, a caregiver for his wife, suffering from mild dementia, expressed his limitations in changing his lifestyle with his wife. Though he thought that “a healthy diet and physical activity both count, my personal preference is for dietary knowledge, because I think that sometimes elderly people can’t stand physical activity and that kind of thing.”
Mrs. H’s articulations of the limitations on ways to change lifestyle offer a glimpse into how dementia affects her own life. Of her elderly mother suffering from moderate dementia and Parkinson’s symptoms, she says: A healthy diet, physical exercise, and social activities are all important, but because the elder is over 80, and what’s more, she’s lost her basic daily activity skills, and she cannot do physical exercise and social activities.
Whereas Mrs. H, whose mother suffered from dementia, explicitly stated her inability to do physical exercise and social activities, caregivers for those with MCI tended to not emphasize limitations. They spoke in terms of the positive potential of physical exercise and social activities. One caregiver for an individual with MCI said, “I think physical exercise helps the most to maintain good health. I exercise every day, I feel very confident of my own body.” Another caregiver says on the subject of exercise, “The most important thing is to persist; every day one must go out and exercise, and after a while my health will get better.” For both of these caregivers, exercise must be continual and regular to be effective. Exercise incorporated thus into one’s lifestyle can improve not only health but also confidence in the body, something many caregivers for those with dementia did not have.
The caregiver and son to a 79-year-old care recipient with MCI stresses the importance of social activity in life, saying “From my own experience, social activities can better promote maintaining good health and good mood [. . .] it is needed for work but also needed for everyday living.” Another caregiver to an MCI-afflicted individual maintains that “often going out, taking part in social activities, and socializing with people will make one feel very happy.”
Discussion
This study is one of the first to present Chinese dementia and MCI caregivers’ views toward lifestyle interventions to promote cognitive and physical health. Whereas some caregivers viewed their current lifestyle as adequate, many others found positive value in changing lifestyle. Caregivers identified diverse ways to live a healthy life, including social and physical activity, diet, music and dance, reading, and practicing a second language. Caregivers for patients with dementia and those for individuals with MCI had different approaches to making lifestyle changes; the former found that the burden of caregiving and their own declining health left them with no time or no possibility for change, while the latter were hopeful about making changes in the future despite their care recipients’ health problems. Perspectives on lifestyle change are affected by caregivers’ and care recipients’ environment, family dynamics, and health status.
Similarities in Views
The vast majority of caregivers for both those with MCI and those with dementia perceive some combination of physical exercise, social activity, and proper diet to be ways of maintaining a healthy lifestyle. Aside from these major categories, some caregivers also mentioned musical and reading activities as ways of improving mental health. Both groups of caregivers in this study seemed to prioritize physical exercise and diet in their perceptions on healthy ways of life.
Caregiver responses from both groups also suggested that environmental factors influence how care dyads practice healthy lifestyles. For one caregiver, clean and “beautiful natural surroundings” themselves could have therapeutic effects. On the other hand, living on a high floor prohibited another caregiver from regular physical exercise. Thus, environment can have important influences on the ability to practice a healthy lifestyle, independent of the stage of change a person is in. Living near a beautiful and clean river, for example, could facilitate a care dyad’s regular walks outside, but traversing flights of stairs can be the key factor preventing progression from the contemplative to the planning stage. Although no difference was found in the mentioning of environments across caregiver groups, individuals with dementia face a greater number of debilitating comorbidities compared with individuals with MCI (Plassman et al., 2011). Physical barriers such as staircases or distance can thus be a greater barrier in care dyads where one is suffering from dementia because it is less safe and more taxing for them to travel.
One final common theme between the two groups of caregivers is their satisfaction with their current situation. Miss D’s and Mr. C’s words suggest that one possibility for contentedness is that they view medicine as limited with regard to dementia treatment. Current understandings of dementia, its risk, and treatment are sparse. Though a society’s “medical imaginary” can render medicine in professional and popular conception as a “many-possibility enterprise,” caregivers in this study did not seem “susceptible to hope engendered by the cultural power of the medical imagination” (Good, 2001, p. 397). The perceived lack of treatment for dementia, in conjunction with the association of cognitive decline with normal aging in Chinese laypersons (Ikels, 2002), may have placed mental health improvement outside of the realm of biotechnological advancement and biomedical possibility. For this reason, they emphasized their acceptance of the present situation rather than looking toward a hopeful future.
In addition, this minority of caregivers from both groups may have deemed change unnecessary because our further analysis shows that they were already doing the social and physical activities they identified as healthy behaviors and did not need additional activity (data not shown). These caregivers did not view lifestyle change as necessary. In this sense, though they were precontemplative of additional lifestyle changes, many were already in the action or maintenance stages of healthy ways of life such as frequent exercise. Nonetheless, the data suggest that a minority of caregivers were not contemplative of additional lifestyle changes and could be suited for experiential processes for change, such as reevaluation of one’s situation, increasing choices for activity, and raising awareness of benefits. In addition, improving knowledge and awareness about available therapeutics for dementia could facilitate some caregivers toward contemplation by giving them hope.
Differences in Views
Despite similar views on the types of activities that would constitute a healthy lifestyle, the two groups of caregivers diverged on their perspectives on which kinds of lifestyle change would be viable for them. This study shows that the cognitive condition of care recipients matters in their caregivers’ perception of lifestyle change. Whereas roughly one third of caregivers for individuals with dementia spoke about lifestyle changes in terms of impossibility and limitation, caregivers for individuals with MCI approached lifestyle change in terms of their potential to maintain health and well-being.
Time was a more formidable constraint for some caregivers for individuals with dementia, but caregivers for those with MCI did not cite lack of time as an impediment to making changes in lifestyle. Caregivers for those with more advanced cognitive impairment must spend more time in caregiving tasks such as cooking or helping with activities of daily life, but the notion of lacking time was not strictly dependent on the burden of caregiving. Mrs. E, for example, considers her primary caregiving activity to be directly observing her husband taking his medications. Her husband, suffering from dementia, can wash up and use the restroom himself. However, she still feels that her “family issues,” her husband’s illness, prevents her from having enough time and energy to make changes. When she says she should “care less about [her] family issues,” the uncertain and unstable health condition of her husband is what prevents her from changing her sleeping and exercise habits, despite her wishes to do so.
The anthropologist Robert Murphy’s account of his journey with progressive paralysis (1987) shows that “uncertainty is a central feature of a chronic illness trajectory” (Becker & Kaufman, 1995, p. 165). He explains, “I gradually learned to live day by day” and hesitated before making plans more than one year long (Murphy, 1987, pp. 25-26). In this study, similarly, the caregiver voices the fundamental uncertainty of care recipients’ chronic illness. She cannot make plans or dedicate time to exercise not only because of caregiving activities but because her husband’s advancing health condition is too uncertain to do so.
All caregivers in this study recognized the inevitability of the declining trajectory of chronic illness and old age. For them, both were associated with decline in general and cognitive health. Caregivers for individuals with dementia seemed to take the inevitability of cognitive decline as something that lifestyle change can do nothing to ameliorate. Mr. F and other caregivers for individuals with MCI, on the other hand, emphasized benefits of physical exercise and social activity and mention their plans to change lifestyle. They saw value and potential in maintaining and even improving mood, confidence, and health. In other words, while caregivers for individuals with MCI also faced chronic illness, their voices were marked by hope, as well. This led to differences in their perception of lifestyle change and outlook toward institutional help, such as placement into a nursing home. These findings echo decision-making patterns of Chinese-American caregivers (Hicks & Lam, 1999), who negotiate the line between normal aging and dementia as they decided whether to place their loved ones in a nursing home.
The present physiological condition of care recipients was also important for caregivers’ responses. Whereas most caregivers for patients with MCI regarded exercise as an excellent way to stay in good shape, even if a caregiver for a patient with dementia (Mr. G) perceives physical activity and diet as part of a healthy lifestyle, he only realistically considers one. Caregivers such as Mrs. H or Mr. G acknowledge the importance of exercise and social activity but find that they can only change diet because their spouses’ limitations in daily activity skills prevent them from more active forms of lifestyle change.
The differences in perspectives on lifestyle change between the two groups of caregivers place them in two different stages of change. Caregivers for those with MCI had hopes and plans to enact lifestyle changes, showing that they are in the preparation stage. Some caregivers could give clear examples as to what kinds of change and talked about persisting in some activities, such as exercise. These individuals would benefit from programs that help transition into the action and maintenance stages, where active efforts are made to change. In the language of the stages of change model, behavioral processes—such as adding prompts for healthy behaviors, rewards for positive changes, and establishing helping relationships and social support—can be beneficial parts of a lifestyle change intervention for these caregivers.
However, caregivers for those with dementia were more likely to be in the contemplative or precontemplative stages. Evidence has shown that behavioral processes are only effective in the later stages of change (Marshall & Biddle, 2001). Prochaska and Velicer (1997) noted that precontemplative and contemplative individuals are “not ready for traditional action-oriented programs” (p. 39). Experiential processes may be effective; however, responses from caregivers in the present study show that experiential processes aimed at changing personal outlook and motivation will not necessarily help caregivers toward healthy lifestyle change. The reasons they cite, such as time constraints, difficulties with physical activity, and uncertainty inherent in chronic illness, lie outside of the personal sphere and may require changes in interpersonal and community contexts to alter health behaviors.
It is worth reiterating the extent to which caregivers spoke of their own lifestyle change in terms of the well-being of care recipients, which suggests that the suffering—forgetfulness, getting lost, losing skills, and other comorbidities—of MCI and dementia is interpersonal; it is social. Care recipients often spend all day solely in the company of their caregivers. As Kleinman (2010) writes, “social suffering conveys the idea that the pain and suffering of a disorder is not limited to the individual sufferer, but extends at times to the family and social network” (p. 1518). Becoming a caregiver can have negative effects on health lifestyle (Beesley, Price, Webb, & Australian Ovarian Cancer Study Group, Australian Ovarian Cancer Study—Quality of Life Study Investigators, 2010). This study illustrates that improving health is interpersonal, too, and shows the importance of addressing the health of caregivers as well as the care recipient. It also suggests that lifestyle change programs aimed at caregivers must consider the cognitive condition of their care recipients. Intervention design targeting caregivers and care recipients should consider family dynamics and changing family needs. One caregiver, for example, foresaw difficulty with exercise when her grandson arrived. Another caregiver highlighted his wife’s need to change “some ways of life,” insisting on changing her lifestyle. In this way, the dynamics of the care dyad itself (such as who is regarded to need lifestyle change most) and family dynamics outside of the care dyad (such as family responsibilities or involvement of other family members) could influence caregivers’ prospects for lifestyle change.
Because health condition, family and care dyad dynamics, and environment influence caregivers’ perspectives on lifestyle change, recruitment and implementation of lifestyle change programs must take these factors into account. The uncertainty of chronic illness and burden of caregiving limit the lifestyle change options of caregivers for patients with dementia.
The transtheoretical model has been critiqued for having arbitrary criteria for stages, omitting of external factors for change, and lacking predictive ability (Adams & White, 2005; Bandura, 1997; Prochaska, 2006; West, 2005). We recognize these limitations, and our findings suggest that progression along the stages of change may depend on changing external factors, such as environment and care recipient health condition, in addition to motivational and educational interventions. The stage constructs are used not as tools to validate stages or predict progress but rather as guidelines to elucidate differences between perspectives on lifestyle change from caregivers for cognitively impaired elderly. The data presented suggest that programs targeted toward care dyads with MCI and those with dementia may require quite different interventions, as caregivers for those with MCI could progress from the planning to action stage while caregivers for those with dementia would require progress from the contemplative or precontemplative to planning stage.
This study’s sample size prevents drawing generalizations about caregivers for those with MCI and those with dementia. In addition, clinic-based sampling could have resulted in sampling bias. However, the data illustrate diverse influences on experiences of caregiving and ability to change. Although we cannot conclude whether caregivers for individuals with dementia find change less accessible in general, their responses suggest an association by which the experience of caring for an individual with dementia can place them on a different stage of change. Further research with a larger sample of caregivers using survey interviews is necessary to determine if there is a significant difference between the perceptions of lifestyle change in the two groups. In addition, efficacy of interventions that are tailored to different groups of caregivers should be compared against the efficacy of nontailored interventions to begin assessing whether the differences identified in this study are actionable and provide significant improvements in intervention design.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant from the NIH Fogarty International Center/National Institute on Aging.