
Abstract
Little is known about the adult outcomes for children with an emotional/behavioral disorder (EBD). The present study examines the perspectives of 34 parents regarding the adult outcomes for their children who experienced emotional and behavioral problems in their youth. Participants completed an online survey containing questions about their child’s behavioral characteristics, educational experiences, and adjustment to adulthood as well as questions about the stress they experienced as a parent of a child with EBD. Both quantitative and qualitative measures were used to assess parents’ perceptions of factors affecting their child’s successful or unsuccessful adult outcomes. Remaining in school was related to positive adult outcomes, while exclusionary disciplinary experiences such as suspension and expulsion were related to negative adult outcomes. The relationship of results to the Individuals With Disabilities Education Improvement Act’s goals for adult functioning and implications for both parents and practitioners serving students with EBD are discussed.
Children and adolescents who greatly deviate from societal expectations for age appropriate behavior are part of every community. Such children may be considered to have an emotional or behavioral disorder, usually categorized either using the classification system of the schools or the mental health system. The Individuals With Disabilities Education Improvement Act (IDEIA), 2004, 20 U.S.C. § 1401 (3)(A)(i) defines emotional disturbance by both the presence of maladaptive behavior and negative educational impact as criteria. Descriptors of the disability include an inability to learn that cannot be explained by other factors; an inability to build satisfactory relationships with peers and teachers; inappropriate behavior or feelings under normal circumstances; a general pervasive mood of unhappiness or depression; and the tendency to develop physical symptoms or fears associated with school or personal problems, 34 C.F.R. § 300.8(c)(4)(i)(A-E). In order for a student to be found eligible for an Individualized Educational Plan (IEP), at least one of the indicators must be present, must be serious, extend over time, and have a negative impact on the child’s educational progress. In contrast, mental health professionals utilize the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) to classify children with mental disorders. The DSM-IV-TR system is multiaxial covering a broader range of diagnoses, including severity levels and etiology, than IDEIA. As schools and mental health organizations use different classification systems to identify children who need their respective services, it is therefore possible for children who have a DSM-IV-TR diagnosis to be found ineligible for school-based special education services due to the absence of a negative impact on educational progress. It is very difficult to separate the literature clearly based on the distinct but overlapping nosological systems. The relevant difference when discussing education outcomes is the IDEIA requirement that emotional or behavioral problems have a negative impact on educational achievement. While it is true that schools are bound by law to use the IDEIA definitions, it is also true that children with emotional problems not covered by IDEIA exist. For the purpose of this study, both children with emotional and behavioral disabilities classified by either IDEIA or the DSM series will be referred to as children with emotional and behavioral disorders (EBD).
Notwithstanding identification by IDEIA of some children and adolescents who have significant mental health concerns, there remain unmet needs of children and adolescents with behavior problems in schools who are either identified by DSM criteria alone or are not identified at all. The prevalence of mental health problems serious enough to warrant a DSM diagnosis in children and adolescents is 25% and between 3% and 17% actually are diagnosed as having a serious emotional disturbance (Costello, Egger, & Angold, 2005; Roberts, Roberts, & Wenyaw, 2009). However, less than 1% of the population of school-aged youth receive special education services for EBD (Planty et al., 2008).
It is the goal of all public education to promote the healthy social development and academic achievement of students so that children will grow into independent, productive, law-abiding, and contributing members of society (Brighouse, 2006; Public Schools of North Carolina State Board of Education, n.d.; Rothstein & Jacobsen, 2006, 2009). While families from diverse cultures and socioeconomic levels may interpret independence or economic productivity differently within their cultural context, broadly stated, all groups endorse transitioning from childhood dependence to assuming an adult role in the culture. These same goals for transition to adulthood have been recognized for children with disabilities, and these universal goals were made explicit in the most recent reauthorization of IDEIA. However, despite progress since the passage of initial federal special education legislation in 1975, students with disabilities have lagged behind typically developing peers in achieving adult independence. In recognition of this situation, Congressional findings in the preamble to the 2004 reauthorization of Individuals With Disabilities Education Act (IDEA) reaffirm and reinforce that the purpose of Special Education is to prepare students for “further education, employment, and independent living,” 20 U.S.C. § 1400(d)(1)(A). In addition, Congress noted that “providing effective transition services to promote successful post-school employment or education is an important measure of accountability for children with disabilities” 20 U.S.C. § 1400(c)(14).
Although these goals historically have been present in law, the 2004 reauthorization put particular emphasis on transition services to improve overall outcomes in these areas. Much previous research has focused on single outcome measures that report graduation rates (U. S. Department of Education, 2008) or employment outcomes (Zigmond, 2006), rather than multidimensional measures of adult functioning (K. H. Armstrong, Dedrick, & Greenbaum, 2003). The aforementioned research has led to a general consensus that outcomes for EBD students in young adulthood are not positive, confirming the necessity of Congressional intent to strengthen transition services to improve adult functioning in the community through postsecondary education, employment, and independent living.
Although disability legislation under IDEIA includes transition services for students with EBD by teaching skills needed for independent functioning in young adulthood, nevertheless, the educational experiences that these students receive often are negative. Since the passage of the Safe Schools Act of 1994 (20 U.S.C. 5961), exclusionary practices such as suspension and expulsion increasingly have been used as schools adopt “zero tolerance” approaches to discipline. Such practices have been found to be arbitrarily delivered in many cases and to be used disproportionately often for children with disabilities and minority students, particularly African American males (Aud, KewalRamani, & Frohlich, 2011; Skiba, 2002; Skiba, Eckes, & Brown, 2010; Skiba & Rausch, 2006). For example, 47% of students with EBD have been suspended or expelled in elementary or middle school, while 73% have been suspended or expelled in high school (SRI International, 2006; Wagner, Kutash, Duchnowski, Epstein, & Sumi, 2005). In comparison, in 2005, the U.S. expulsion rate for general education students in grades K-12 was estimated at 2.1 per 1,000 students (0.21%; Gilliam, 2005). Considering high school students alone, more recent data indicated the overall expulsion rate for general education students is approximately 3% (Stillwell, Sable, & Plotts, 2011) whereas for high school students with EBD, the rate is 73% (Wagner et al., 2006).
Students affected by these and other negative school experiences are more likely to drop out before comple- ting high school, and students with EBDs have been found to have the highest drop-out rate (55.9%) among stud- ents receiving special education or general education (U.S. Department of Education, 2003; U.S. Department of Education, Office of Special Education Programs, 2007). Approximately 61% of students labeled EBD drop out of school and only 32% graduate compared to 75% of students graduating nationally in the United States (U.S. Department of Education, 2004, 2008; U.S. Public Health Service, 2001). Furthermore, high-stakes testing mandated by the No Child Left Behind Act of 2002 was predicted to continue to increase the overall drop-out rate (Schargel, 2003, 2011) and that has indeed been borne out by other researchers (McNeil, Coppola, Radigan, & Vasquez Heilig, 2008). In 2001, nearly 45% of the one million individuals taking the General Educational Development (GED) high school equivalency test self-reported mental health concerns as contributing to their school failure and dropping out (Koller & Bertel, 2006). Historically, relatively few students with EBD have gone on to postsecondary education (Rogers & Rogers, 2001) and this trend appears to be continuing, with approximately one third of students with mental health problems pursuing any postsecondary educational program, 20% enrolling in 2-year community colleges and fewer than 6% entering 4-year colleges according to the National Longitudinal Transition Study–2 (Government Accountability Office [GAO], 2008; Wagner et al., 2005).
Other postschool outcomes are also poor for students with EBD. There are high rates of unstable employment, unemployment, poverty, restricted social networks in the community, and criminal behavior in students with EBD who do not continue to postsecondary education (Bradley, Doolittle, & Bartolotta, 2008; Janz & Banbury, 2009; Substance Abuse and Mental Health Services Administration, 2008). When students with EBD reach the age at which transition to adulthood begins, their rates of substance abuse and criminal activity rise to well above the norm as has been shown for over a decade (Greenbaum et al., 1996; Janz & Banbury, 2009; Wald & Losen, 2003).
As two decades of research indicate, children and adolescents with EBD have both negative school experiences and poor young adult outcomes despite normal or near-normal cognitive functioning. To improve outcomes for students who have experienced severe problems in school, home–school–community collaboration is even more important than it is for typical students according to the National Association of School Psychologists (NASP; Quinn & Lee, 2007). In addition, major U.S. initiatives have long recognized the crucial role parental involvement plays in improving schools in both general and special education settings (No Child Left Behind Act, 2002; Sailor, 2002) and this continues to be true (K. J. Anderson & Minke, 2007; Mandell & Murray, 2009). However, in order for effective parent–school partnerships and collaboration to develop, trust and nurturance are essential. Trust is necessary for the home–school relationship to flourish; while nurturance involves treating all team members with warmth and recognizing the unique expertise that each brings to the table. A nurturing communication style is devoid of judgment and negative stereotyping between school and community partners (Eagle, Dowd-Eagle, & Sheridan, 2008). For parents to trust school professionals they must feel that school professionals understand their unique perspectives and experiences with their children.
Unfortunately, parents of students with EBD may be avoidant of contact with the school because past interactions may have been contentious and challenging (Wang, Dishion, Stormshak, & Willett, 2011). Although accusations are counterproductive and raise tension, professionals tend to blame parents for children’s behavior problems (Hinshaw, 2005) to such a degree that as a group, parents of children with EBD are viewed unidimensionally as either inadequate caregivers or directly contributory to their children’s problems (Home, 2008; Northey, Wells, Silverman, & Bailey, 2003). However, little research has examined the ecological impact a child with EBD has on the family and the family’s functioning (Wang et al., 2011). Children and adolescents who fit either the IDEIA or DSM definitions of emotional and behavioral problems present challenging behavior problems for their parents (M. I. Armstrong, Birnie-Lefcovitch, & Ungar, 2005; Olive & Liu, 2005). Parents of a child with EBD experience extra strain (Scharlach et al., 2006; Taylor-Richardson, Heflinger, & Brown, 2006), more challenges in meeting both family and work demands (Rosenzweig, Brennan, & Ogilvie, 2002), and more parenting stress than parents of normally developing children (M. I. Armstrong et al., 2005; Williford, Calkins, & Keane, 2007).
Furthermore, studies have shown that children with emotional and behavioral problems are costly to raise and educate, for society in general, and presumably, for parents as well (Cohen, Miller, & Rossman, 1994; Loeber, Burke, Lahey, Winters, & Zera, 2000). For example, more than 12 years ago Cohen (1998) found that the cost to society of a single high-risk youth dropping out of school and engaging in criminal behavior ranged between US$1.7 and US$2.3 million dollars; this figure would be approximately US$2.4 to US$3.3 million in 2012. In comparison with other disabilities, emotional and behavioral problems are the most expensive concerns to treat in North America (J. A. Anderson, McIntyre, Rotto, & Robertson, 2002; Bradley et al., 2008); and use of public services throughout youth and adulthood by children with behavior problems is 10 times higher than for children with no conduct problems (Foster & Jones, 2005). Studies show that in addition to relational and overall stress, having a child with an emotional disability includes significant economic burden (M. I. Armstrong et al., 2005). Low-income families are particularly vulnerable to out of pocket expenses for their child with emotional disabilities (Newacheck, Inkelas, & Kim, 2004). In addition to creating an economic burden on the family, perceived financial strain also has a negative impact on children across many domains, including use of positive parenting practices, a child’s self-esteem (Reichman, Corman, & Noonan, 2008), use of mental health services (Brannan, Heflinger, & Foster, 2003; Costello, Compton, Keeler, & Angold, 2003), and increased behavioral problems including impulsivity, antisocial behavior, and depression (Ryan, Boxmeyer, & Lochman, 2009; Wadsworth, Raviv, Compas, & Connor-Smith, 2005). These relationships between perceived financial strain and negative outcomes apply to families across all-income levels.
Parents are charged with the primary responsibility of caring for their children. Federal law as delineated by the Supreme Court of the United States regards parents as the first and best advocates for their children (Winkelman v. Parma City School District, 2007), but many school personnel view parents of students with EBD as difficult to work with and often blame them for their children’s problems (Hinshaw, 2005; Home, 2008). Children spend most of their time in school with teachers or at home with parents and parents have valuable information that is necessary to gain a broader understanding of the child. According to both IDEIA (2004) and independent research on home–school collaboration, parents should have an equal role in decision-making processes for effective home–school collaboration to achieve positive outcomes for children (Christenson & Thurlow, 2004). If children are having problems in school, home–school collaboration is even more important than for typically developing children (Quinn & Lee, 2007). Therefore, gaining the parents’ perspective is invaluable to education professionals serving children with EBD.
Research has not examined parent perspectives on outcomes for adult children with EBD in regard to achieving IDEIA transition goals. The IDEIA goals of postsecondary education, independent living, and financial independence are realistically attainable for this population, more so than for children with severe cognitive and physical disabilities. Little attention has been given to whether or not children with EBD do achieve these goals as young adults, the degree of caregiving strain experienced by parents while raising children with EBD, the relationship between parental financial strain and young adult outcome, and parent attributions relating to their children’s success or lack of success as adults. In addition, as much of the literature on children with EBD explicitly addresses low–socioeconomic status (SES) families, it is important to consider the experiences of parents who had adequate access to financial resources for child rearing to filter out the direct effects of poverty on attainment of IDEIA goals. This study examines the relationship between adult outcomes for children with EBD and IDEIA transition goals, as well as parental strain, financial impact, and parental attributions of their child’s adult outcome for families who are not beset by a large number of social and economic problems
Research Questions
Research Questions 1: How do adult children’s outcomes compare with IDEIA goals of post–high school education, employment, and independent living from the parents’ perspective?
Research Questions 2: How stressful do parents find caring for a child/adolescent with emotional and behavioral problems at differing ages?
Research Questions 3: Does perceived parental financial strain affect the child’s adult outcome?
Research Questions 4: To what do parents attribute their adult child’s success or lack of success?
Method
Participant Characteristics
Participants included 34 parents of children 18 or older who experienced moderate to severe emotional or behavioral problems in childhood or adolescence. The respondents were overwhelmingly female, with 31 females and 3 males, 85% Caucasian, and had a median age range of 50 to 55 years. The parents’ median educational level fell within the “college graduate” range and 7 of the respondents received graduate or professional degrees. During their children’s school years, the SES of the respondents was more normally distributed than education, with 28% of respondents describing themselves as working class or below, 36% as middle class, and 28% as upper-middle class, with 8% as “very poor/unemployed.” By the time the child graduated from high school, 28% described themselves as working class or below, 30% as middle class, and 42% as upper-middle class with no respondent endorsing “very poor/unemployed.”
Sampling Procedures
Recruitment of parents of children with EBD for research is particularly challenging due to the stigma associated with this disability. It can be difficult for researchers to locate adequate samples of adults who experienced EBD as children/adolescents or their parents. Having an “invisible disability,” the stigma of mental illness, and negative stereotyping of parents of children with EBD (Marsh, 2004) contribute to the difficulty in finding participants for follow-up studies. The development of online support forums for parents of children with EBD created a space where family members could communicate with others with similar child-rearing experiences away from the judgment of the public eye. The existence of these forums also gave researchers access to a national pool of participants that heretofore would have been very difficult to contact. There are advantages to studying parents who are online support group members including wide geographic sampling frame, anonymity, and ease of data collection through online survey techniques.
Because the numbers of parents of adults who experienced emotional and behavioral problems as children is a small part of the population of parents of all children with disabilities, invitations were posted on three online parent forums frequented by parents of children, adolescents, and young adults with emotional and behavioral problems to recruit participants. The anonymity of both the participants and the names of the websites was guaranteed to obtain the approval of both the website owners and the institutional review board (IRB) at the sponsoring university. Participants volunteered by clicking on an active link on an invitation that took them to the consent form approved by the IRB. Upon accepting the terms of the consent, the participants were directed to the anonymous survey. As parent participants volunteered for inclusion in the study by completing a survey, and because the number of parents with qualifying children who visited the support group sites during the 30 days the survey was available is unknown, there is no way to calculate the response rate for the survey. Furthermore, as with all anonymous surveys, there is no way to verify that nonresponders are comparable with responders.
Parents rated their adult children on many dimensions, including their perception of whether the child’s transition to adulthood was successful or unsuccessful (description below). To be included in this study, an adult child must have been rated in the highest two categories (successful/extremely successful) or in the lowest two categories (unsuccessful/extremely unsuccessful) on the 7-point index and have congruent parental verbal descriptions of the adult child’s current status. As there were 17 parents who rated their adult child in the successful groups and 43 who rated their child in the unsuccessful groups, 17 were randomly drawn by computer from the 43 in the unsuccessful groups to provide a total sample size of 34 parents.
Measures and Constructs
Survey Instrument
The measures below were operationalized in a survey particularly designed to address the research questions in this study. In addition to the indices described below, parents also provided information regarding their adult child’s type of education—general or special; presence of a behavior intervention plan; highest educational level completed; parent rating of child behavior; presence of DSM diagnoses; and mental health services obtained by parents outside of school settings. In addition, parents supplied demographic information about themselves. Parents rated their child’s behavior at three separate stages, including preschool, elementary/middle school, and high school, to detect differences throughout the child’s development. The Caregiver Strain Questionnaire (CGSQ) was included in its entirety, although in the survey document, it was presented to respondents as a matrix that was not designated by specific name to avoid bias.
Definition of “Successful” and “Unsuccessful”
The revision of IDEIA in 2004 highlights the importance of students in special education pursuing the same goals of postsecondary education, employment, and independent living as typical young adults. Not only are these goals applicable to students in general and special education, but they also largely transcend racial, cultural, and language differences in that changing one’s status from that of a dependent child to an independent adult is not only present in groups within the United States but also internationally (Arnett, 2001). Although the exact formulation of “success” might vary across groups, in the United States, most parents hope their children will complete their education, obtain employment, and assume adult functions commensurate with their abilities. Therefore, achieving the goals of postsecondary education, employment, and independent living in some form may be assumed to be part of a parental definition of “successful” transition to adulthood; however, for young adults with childhood EBD, it was unknown what definitions of being “successful” adults their parents would hold. Experienced parents should be able to determine their child’s attainment of various developmental milestones that mark adulthood and are encompassed by IDEIA goals within the context of the severity of the adult’s child/adolescent problems and their own cultural expectations. Given the belief that parents are valuable sources of information about their child’s overall functioning, their subjective ratings and open-ended descriptions of their child’s success or lack of success were obtained. We wanted parents to evaluate their adult child’s adjustment to adulthood with “all things considered” because no a priori list of criteria or examples of success or lack of success would be universally applicable to this very diverse sample of adults who experienced EBD as children. An implicit purpose of this study was to determine how a “successful” adult or an “unsuccessful” adult with childhood EBD is described from the perspective of the child’s parent. To address this aim in a comprehensive manner, three types of parent measures of successful and unsuccessful adjustment to adulthood were used: a 7-point index that ranged from “extremely successful” to “extremely unsuccessful,” a dichotomous forced choice (successful–unsuccessful), and a qualitative narrative question that was used to verify what parents meant by “success” or “lack of success” and to what they attributed their child’s successful or unsuccessful adult outcome.
The CGSQ
The CGSQ (Brannan, Heflinger, & Bickman, 1997) contains 21 items. The responses range from 1 (not at all a problem) to 5 (very much a problem). To account for possible differences in the strain at various times in the child’s development, parents were asked to rate their child at three ages: preschool, elementary/middle school, and high school. An aggregated mean score was obtained for each parent based on their recollection of stress throughout the child’s development. The CGSQ has been factor analyzed, and the resulting indices were evaluated for internal consistency in this sample using Cronbach’s alpha. Consistent with the literature, high Cronbach’s alpha measures were obtained. The alphas, means, and standard deviations for the factors are as follows: Objective Caregiver Strain, α = .94, x = 3.26, SD = .928; Internalized Subjective Strain, α = .88, x = 3.15, SD = .946; and Externalized Subjective Strain, α = .80, x = 2.04, SD = 1.017. In addition to the three factors identified by Brannan et al. (1997), a fourth index was constructed to measure financial stain using two items from the CGSQ related to financial consequences of caring for a child with behavior problems (4. Family member having to do without things; and 7. Financial strain). This index, which yielded an α = .89, x = 2.26, SD = 1.085, was constructed in response to the unanticipated very high level of parent purchased mental health services and was analyzed separately from the original indices.
Educational Attainment
Parents were asked to report their child’s highest grade completed; whether the child completed high school, and if so, whether a diploma or GED was obtained; and whether their child had pursued any postsecondary education. The responses were coded into three categories: dropping out of school before graduation, completing high school, and attaining postsecondary education.
Employment Status
Employment was coded as “full-time,” “part-time,” or “unemployed.” In the qualitative data, there were apparent differences in the meaning of “unemployed” with some parents characterizing their adult child as currently (but temporarily) unemployed while others indicated that unemployment was a chronic state in which the adult child was “unemployable.” However, for quantitative analyses, these were combined into one category.
Index of Positive Activity
To capture the wide range of experiences described by parents for quantitative data analyses, an index was created to include both postsecondary education and employment in a single measure of the degree to which these adults were “positively occupying” their time. Those who were working full-time, attending school full-time, or attending school at least part-time while working at least part-time were considered to be fully positively occupied. Those adult children who were only working part-time, only attending school part-time, or were stay-at-home parents without part-time employment were considered to be partially positively occupied. Finally, those who were unemployed, not attending school, incarcerated, or whose whereabouts were unknown were considered to be not positively occupied.
Residential Status
Responses detailing an adult child’s living situation were coded as being independent, dependent on the parent, dependent on others, or a negative residential outcome. Parents who described their child as paying his or her own rent were coded as independent; those who stated that their child lived with them and did not contribute to costs of living were coded as dependent on their parent; those who stated that their child lived with a spouse, significant other, or roommate and did not contribute to costs of living were coded as dependent on others; while those who specified that their adult child was homeless, incarcerated, transient living with peers and abusing substances, or whose location was unknown were coded as a negative residential outcome.
Financial Independence
Parents indicated whether their child was totally financially independent; partially independent and receiving minor assistance (from them, a spouse, or from another individual), partially independent and receiving major assistance (from them, a spouse, another individual, or from Social Security Supplementary Income [SSI]); or whether the child was totally dependent on the parent or the state.
Index of Independent Living
This index combined residential living situation and financial independence to create a single measure of attainment of two important IDEIA goals for adult independence. All degrees of residential status and financial independence were assigned weights which were combined to yield a 7-point scale ranging from totally dependent to totally independent. Each adult child was assigned a score on the resulting 7-point scale to represent his or her overall adult independence.
Study Design
Various methodologies have been used to attempt to ass- ess outcomes, including prospective longitudinal, cross- sectional, and retrospective methods. Prospective designs are superior but generally, they are not feasible due to high attrition rates, residential mobility of the sample, cost, and time; therefore, retrospective studies have been utilized despite methodological limitations (Brewin, Andrews, & Gotlib, 1993). For the present study, a retrospective approach was selected.
The design technique of using online surveys is advantageous for accessing individuals who may otherwise not volunteer to participate in a study dealing with sensitive information (McCabe, 2004; Pealer, Weiler, Pigg, Miller, & Dorman, 2001; Tourangeau, Couper, & Steiger, 2001). A further advantage of online surveys is that they often produce more candid answers than intrusive methods such as face-to-face interviewing (Kiernan, Kiernan, Oyler, & Gilles, 2005; Olsen, Wygant, & Brown, 2004). In this study, parents were able to participate anonymously, which may have allowed them to feel more comfortable discussing their children’s difficult problems than otherwise would have been the case (Colvin, Chenoweth, Bold, & Harding, 2004).
Results
Adult Children
Preliminary Analyses
To clarify parent perceptions of the behavior of their developing child, they were asked preliminary questions about their child’s behavior at ages 3 to 5. Despite clear differences in parental ratings of adult adjustment, as young children, these adults were equally problematic in many areas of functioning, and no statistically significant differences were found. The successful and unsuccessful groups were equivalent on the following early childhood measures of severity indicating that both groups had significant emotional or behavioral problems by school entry: presence of DSM diagnosis, age at which problematic behaviors were first noticed by the respondent, attendance in general prekindergarten programs, and their need for or use of early intervention services. The common behavior problems in both samples included opposition and defiance at home, mood swings, “meltdowns,” anxiety, specific fears and phobias, overdependence for age, and language delays. Therefore, these groups appear to be appropriately matched to make comparisons in their outcomes as adults.
Demographic Analyses
Demographic information for the adult children is depicted in Table 1. The majority of the sample of adult children is below age 25 and ranges from 18 to above 35, with a mean of 23 years, and a median of 21 years. When compared with the male–female distribution in the general population, the sample contains an excess of females (61.8%) which was found to be statistically significantly different from the general population. However, as the number of boys with emotional and behavioral problems exceeds the number of girls (Baillargeon et al., 2007; Lahey et al., 1999; Wagner et al., 2005; Zoccolillo, 1993) the excess of girls in the sample does not reflect the underlying population. This may be due to the fact that, in this sample, females were more likely than males to be rated as successful and all individuals rated as either “successful” or “very successful” were included in analyses. The adult children are slightly more diverse than their parents but the children also are predominantly Caucasian. Despite majority racial status of both parents and adult children and most parents reporting at least adequate financial resources by their child’s high school graduation, there is a wide variance in educational outcomes, ranging from an adult child who was expelled from the fifth grade to an adult child with a graduate degree. As reported in Table 1, two adults completed eighth grade or below, 9 completed some high school, 13 completed the 12th grade, and10 adults completed some postsecondary education, with 3 graduating from 4-year colleges and 1 adult obtaining a graduate degree.
Adult Child Demographic Information.

Note: IEP = Individualized Educational Plan; DSM = Diagnostic and Statistical Manual of Mental Disorders.
Research Question 1: How do Adult Children’s Outcomes Compare With IDEIA Goals of Post–High School Education, Employment, and Independent Living?
Several survey items that were used to measure adult child participants’ progress on the IDEIA goals of post–high school education, employment, and independent living are displayed in Table 2. Responses to the education items were analyzed in a number of ways to yield a better picture of the adult children’s education, both past and present. When compared with dropping out, high school graduation alone did not yield a significant relationship with adjustment to adulthood, either successful or unsuccessful, χ2(1) = 3.11, p = .08. However, there was a statistically significant relationship between three levels of education attainment, (dropping out, high school completion, and postsecondary education) and successful outcome, χ2(2) = 5.84 p = .05. Students with higher levels of education were more likely to be rated as successful by their parents, F(2, 31) = 3.22, p = .05. In post hoc analyses using Bonferroni, only the paired differences between dropping out and postsecondary education were significant, p = .016.
Adult Child Progress on IDEIA Goals.

Note: IDEIA = Individuals With Disabilities Education Improvement Act.
Neither having an IEP nor a Behavioral Intervention Plan (BIP) was significantly associated with success. However, students who were expelled from high school were significantly more likely to be unsuccessful as adults, χ2(1) = 3.74, p = .05. It should be noted that no student who was rated as successful was expelled from high school and the overall expulsion rate for this sample was 16% in comparison with a general education high school expulsion rate of approximately 3% (Stillwell et al., 2011).
As with educational achievement, adult children’s attainment of IDEIA goals related to employment yielded a positive relationship between employment status and parent rating of adjustment to adulthood. Higher levels of employment were significantly associated with a more successful adjustment to adulthood, χ2(3) = 17.65, p = .001. To account for adult children who were completing postsecondary education, those parents who reported that their child was a full-time student were differentiated from those who specified that their child was unemployed. At the time of the study, only three adult children were both unemployed and full-time college students; all three were characterized by their parents as achieving a successful adjustment to adulthood.
The means and standard deviations for the combined Indices of Positive Activity and Independent Living are shown in Table 3. An analysis of the Index of Positive Activity was used to examine the adult child’s current combined education and employment status. A significant relationship was found between positively occupying time and successful adjustment to adulthood, χ2(2) = 20.57, p = .001. Thirteen of the 14 adult children who were fully positively occupied were rated as successful, while 13 out of 14 adult children not positively occupied were rated as unsuccessful.
Combined Indices of Progress.

Adult children’s current residential situation was analyzed in a number of ways to capture parents’ descriptions of their child’s independent living status. A significant relationship was found between independent living status and successful adjustment to adulthood, χ2(3) = 13.91, p < .01. Of the 20 adult children who lived in an independent residential setting, 19 were characterized as making a successful adjustment to adulthood. None of the 6 adult children who were in a negative residential setting were described by their parent as successful.
Greater financial independence was significantly related to successful adjustment to adulthood, χ2(3) = 17.14, p < .001. Of the 17 adult children who were totally dependent, 15 were described as unsuccessful. In contrast, however, of the 6 adult children who were totally independent, 5 were characterized as being successful while 1 was characterized by the parent as being unsuccessful apparently due to continuing alcohol abuse, unemployment, and arrest record. In addition, her financial independence was attributed to spousal support.
Financial independence was taken into account as well as residential status when determining an adult child’s status on the Independent Living Index. A univariate analysis of variance of this index indicated that, taken together, residential and financial independence were significantly associated with more successful outcomes as adults, F(1, 34) = 23.51, p < .001.
Research Question 2: How Stressful Do Parents Find Caring for a Child/Adolescent With Emotional and Behavioral Problems?
The original caregiver strain indices, Objective Caregiver Strain, Internalized Subjective Strain, and Externalized Subjective Strain are displayed in Table 4. These results were evaluated together using MANOVA. The assumption of homogeneity of variance was met (Box’s M = 21.236, p = .068). Parents of children described as unsuccessful reported more strain on each subscale than those whose children were described as successful. The overall F(4, 21) = 5.95, p = .002, was significant and two of three univariate Fs were significant and the third approached significance: Objective, F(1, 25) = 6.21, p =.02; Internalized, F(1, 25) = 13.28, p = .001; and Externalized, F(1, 25) = 2.82, p = .10.
Results for Parent Stress Indices.
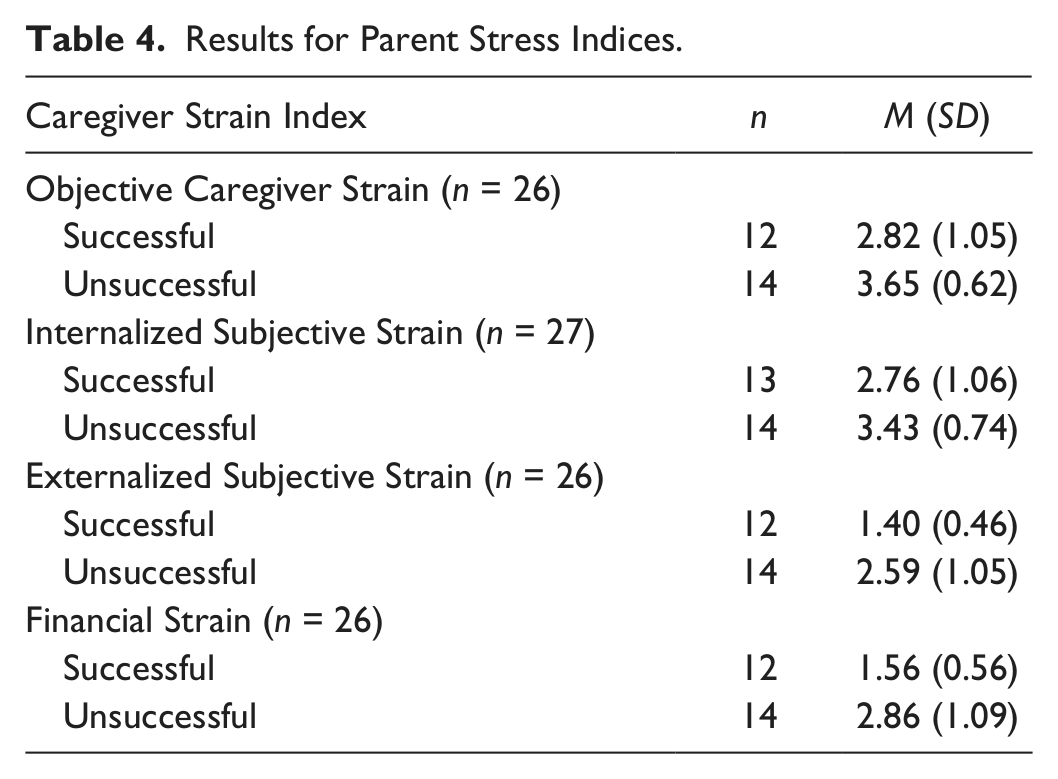
In addition to the CGSQ, stress levels that were experienced by parents include reported impact on the parents’ physical and mental health due to raising a child with EBD. Results of a univariate ANOVA indicated that parents of unsuccessful adult children reported a more negative impact on their own mental health as the child was growing up, F(1, 26) = 11.00, p = .003. Although reported impact on physical health was also rated more negatively by parents of unsuccessful adult children, it was not statistically significant.
Research Question 3: Does Parental Financial Strain Impact the Child’s Adult Outcome?
As shown in Table 4, two items of the CGSQ asked parents about the degree to which they experienced financial “strain” as a parent of a child with EBD. There were significant differences between the groups, which were evaluated using MANOVA. The assumption of homogeneity of variances was not met (Box’s M = 13.723, p = .006). Parents of children described as unsuccessful reported more financial distress on each item than those whose children were successful. The overall F(2, 23) = 6.73, p = .005, was significant and both of the univariate Fs were significant: Strain, F(1, 25) = 10.39, p = .004; and Deprivation, F(1, 25) = 11.66, p = .002.
Results from other survey items suggest that both groups of parents tried to purchase as many services outside the school as possible because private service utilization was high in both groups but not significantly different. Both groups frequently obtained mental health assessments (86% unsuccessful and 77% successful, respectively). Both groups utilized residential treatment via parental placement at a high rate (47% unsuccessful and 53% successful) indicating many parents purchased services that would cause strain in most family financial situations. Twenty-six of 34 (76.5%) adults were treated in a Residential Treatment Center (RTC) at some point during their school years. However, those who had been treated in an RTC were no more or less likely to be successful as adults.
While the long-term adult outcomes of treatment in an RTC were inconclusive for this sample, the prevalence of its use as a form of treatment provides an indirect measure of severity of individuals’ problems: 15 of 17 unsuccessful adults and 11 of 17 successful adults received residential treatment. This finding suggests that the level of severity of problems was very high and that parents sought independent interventions frequently.
There was a significant difference in type of placement: When all involuntary placements were compared with voluntary parental placements, the difference was significant, χ2(1) = 4.51, p = .03. Successful adults were only placed outside the home by parents whereas unsuccessful adults were placed outside the home by other agencies, particularly by the courts.
Research Question 4: To What Do Parents Attribute Their Adult Child’s Success or Lack of Success?
Parents were asked, using an open-ended response format, to describe factors to which they attributed their child’s successful or unsuccessful adjustment to adulthood. Tables 5 and 6 depict their responses.
Parent Attributions of Child’s Successful Adjustment to Adulthood (n = 31).

Parent Attributions of Child’s Unsuccessful Adjustment to Adulthood (n = 31).

Note: DSM = Diagnostic and Statistical Manual of Mental Disorders.
As can be seen in Table 5, parents most often attribute their child’s successful adjustment to adulthood to factors within the child such as intelligence, talent, positive attitude, maturity, motivation, or work ethic, and factors within the parent or family environment such as family support, financial assistance, and forced independence or tough love. In addition, mental health services were mentioned by parents as aiding in their child’s positive adjustment. Few parents (6.4%) cited education or school-based services as helping their child achieve a positive adult outcome.
The data in Table 6 show that parents most often attribute their child’s unsuccessful adjustment to adulthood to factors within the child such as emotional problems, stubbornness, impulsivity, opposition, defiance, poor coping skills, an inability to hold a job, lack of respect for authority figures, negative life choices, risky sexual behaviors, poor judgment, ignorance of stated rules, noncompliance with medication or treatment, substance abuse, or other symptoms of a mental illness or specific conditions included in their DSM diagnoses. Nearly 10% of parents cited poor school supports, a lack of education, or negative school environment as contributing to their child’s unsuccessful adult outcome.
Discussion
In an era when the graduation rate for students with EBD is less than 50% (GAO, 2008), the most important finding of this study is staying in school through postsecondary education contributes to adult success of those who were identified as children/adolescents with EBD. The IDEIA goal of postsecondary education was associated with parent perception of success, and to some, this might seem to be an obvious relationship. While graduating from high school alone was not associated with success in this study, perhaps because the majority of these students completed 12th grade thus restricting the variance, dropping out of high school and pursuing postsecondary education were clearly important predictors of unsuccessful and successful adult outcomes, respectively. In this sample, there was a 68% high school completion rate and a 29% participation in postsecondary education suggesting that these parents went to great lengths to keep their children engaged in education. Thus, even in a small sample, the results are congruent with IDEIA’s emphasis on postsecondary education apparently because those engaged in postsecondary education were more likely to be rated as successful by their parents. However, as students with behavioral problems in general are much more likely to drop out or be expelled from high school, achieving the IDEIA goal of postsecondary education (that should be attainable for this group of students based on cognitive ability) deserves more attention than current educational policies support. IEP transition plans for high school students with EBD should be tied to postsecondary educational goals stressing specific skills that will lead to improved employment opportunities.
In contrast, another important finding was the relationship of expulsion and unsuccessful outcomes. Expulsion is an extremely negative predictor of success of students with EBD. No student in this study who was expelled was rated as successful in adulthood despite majority status and adequate social capital of his or her family. It is generally known that students with EBD are more likely to violate school rules, be suspended, and eventually expelled from school. In this study, use of punitive discipline was not associated with positive outcomes.
Adult Adjustment and IDEIA Goals
Successful adjustment to adulthood was significantly related to employment status as well as independent living and financial independence. Considering all of the parent ratings, 10 of 31 (32%) adult children were employed full-time and an additional 5 (16%) were employed part-time. Furthermore, only 14 adults (41%) were considered to be “fully positively occupied,” suggesting that many students with EBD leave high school unprepared for either employment or postsecondary education. Although 20 adults (59%) were living independently, only 6 (18%) adult children were described as being fully financially independent. This suggests that while there is clearly a positive benefit to achieving the IDEIA goal of postsecondary employment and independent living, a large majority of adult children in this sample have not achieved financial independence. Given that the adult children were all reported to be of normal or high-average cognitive functioning, it is not surprising that the majority attained independent living status, meaning they can successfully manage and care for themselves. However, the contrast between percentage that attained independent living and the percentage that attained financial independence indicates that they may not be achieving their full potential.
These findings are even more troubling when one considers that these adults have parents with at least average educational and SES levels and the sample includes more individuals with majority status than those generally depicted in the literature or than would be expected in a random sample of parents of all students with EBD. If the young adult children of parents with this level of social capital experience problems fully occupying themselves either with full-time work or postsecondary education, it is difficult to imagine that young adults with EBD in childhood who have less well-educated and resourced parents would fare better or even as well. Thus, the somewhat positive skew of the current sample probably depicts a picture that is optimistic compared with the underlying group of adults who had EBD during childhood/adolescence. This strongly suggests that even higher levels of negative adult outcomes in children with EBD than shown in this study are likely in the population. Furthermore, at the time these data were collected, the economy had begun to deteriorate, which probably would depress outcomes for all young adults, with childhood EBD or not. Future studies could include a more diverse sample in the study to verify these results as well as take changing economic conditions into account.
Parental Strain
Not surprisingly, parents whose adult children were unsuccessful reported higher levels of strain during their child-rearing years in all measured spheres and more negative effects on their mental health. It is easy to understand why having a child with serious emotional and behavioral problems of long duration would be stressful for any parent (Long, Gurka, & Blackman, 2008). Causality cannot be established, but parents of the adult children who did not improve year after year and therefore were still unsuccessful reported significantly more strain than parents of the successful adult children, who experienced equivalent problems as young children. Conversely, seeing a child/adolescent on an improving trajectory leading eventually to a parent rating of successful or highly successful obviously could reduce perceived stress. It is possible that the adults’ current outcome affected parents’ recall of their strain. Attempts were made to guard against this bias, however, by asking parents to reflect on strain at three levels of child development. Nevertheless, as many of the unsuccessful adult children remain under their parents’ care, or at least are financially dependent, parents may have reported current as well as historic strain.
Financial Strain
In a similar pattern to parental strain, parents of unsuccessful adult children reported significantly more perceived financial strain during their child’s youth than parents of successful adult children. This relationship existed despite the parents reporting equivalent incomes and parental purchase of costly mental health services and residential treatment was high in both groups. However, “financial strain” is subjective and it is possible that parents whose intervention attempts were not succeeding stretched their family budgets further than parents of successful adults by trying to provide all possible interventions. In addition, while there was no significant difference in the rate of residential placement among the adult children, it is possible when residential placements failed to produce improvement, the parents perceived more financial strain due to anticipating the need to purchase additional services.
Parent Attributions of Success or Lack of Success
Parents commonly attributed both successful and unsuccessful adjustment in adulthood to factors internal to the child. Even though one third of the adult children had IEPs as youth, less than 10% of the parents mentioned school services as affecting outcomes. This result may be somewhat discouraging to professionals who are working with this population of students and are attempting to provide interventions that will foster positive growth and development within the child’s home or school environment. However, knowing that parents feel that internal characteristics are very important to determining adult outcomes for this group of children, professionals can try to adapt and design interventions that capitalize on positive individual traits and alleviate the effects of negative personal characteristics.
Implications and Future Research
Despite the stigma associated with being identified as a student with EBD under IDEIA, qualifying for special education may serve as a protective function for students who are more likely than average to violate school rules. Increasing school identification of students with DSM diagnoses under IDEIA criteria may be beneficial because an IEP provides legal protection against arbitrary disciplinary actions as well as access to transition planning. Consequently, it is possible that the presence of an IEP alone would have protected the unsuccessful students from expulsion and thereby increased their chances for success. In this study, however, the presence of an IEP was not directly related to successful or unsuccessful adult outcomes perhaps due to the time period in which these adult children were in school.
In this study, no successful student was expelled, making it clear that expulsion is connected to negative outcomes for this sample. School staff should work to develop preventive strategies such as positive behavioral interventions and supports that would bring student behavior to acceptable levels and obviate the need to use highly punitive measures such as expulsion.
Online parent samples can be problematic as parent participants may be better educated and more affluent than the population of parents of children with EBD in general; furthermore, participating parents must be computer literate and have access to a computer. While it is true that the sample in this study is positively skewed in terms of educational and SES level, we wanted to investigate the achievement of IDEIA 2004 goals in a sample of parents of adult children who experienced EBD as children/adolescents under the condition of having family resources and a level of parent education that are higher than other samples of parents of students with EBD. The rationale was that if the children of parents who were financially stable and reasonably well-educated did not fare well, it is unlikely that outcomes would be better if the parents had lacked access to education, were poor, and were undergoing many stresses in addition to parenting a child with EBD. If the adult children had done exceptionally well, then there would be a confound with their parents’ resources. As only 17% of the adult children rated by the entire sample were considered “successful” or “very successful,” the design is not confounded. Based on the findings from this study, it would be beneficial for additional research to examine the adult outcomes for a larger sample of children that is more racially and socioeconomically diverse for purposes of comparison. Additional focus should be given to school-based services and whether or not preventive measures or appropriate special education services would produce positive outcomes for this population. Finally, as shown by the current study, the percentage of students with EBD who actually receive specialized services in school is small compared with the numbers of children and adolescents who experience significant emotional and behavioral problems. Therefore, it would be important for future studies of children with emotional and behavioral problems to include children with DSM diagnoses in addition to students found eligible for special education services under IDEIA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) received no financial support for the research and/or authorship of this article.