
Abstract
The U.S. health care system continues to struggle to meet the needs of all members of society. Health disparities are a major concern of the health care system. There are differences in health outcomes related to gender, race, ethnicity, age, and other social indicators. Previous research has focused on differences in access to health care and differences in the delivery of specific medical services. More recently, researchers have examined the way doctors and patients interact to understand health disparities. The current study examines differences in the way doctors and patients interact in terms of information gathering, communicating information, and relationship building, as well as general conduct of the interaction and patient’s satisfaction with the encounter. The study uses data coded from audiotapes of 221 doctor–patient encounters. The results suggest medical encounters differ in important ways depending on patient and physician characteristics. These differences can create and contribute to health disparities.
Introduction
A large body of evidence suggests that health disparities continue to plague the U.S. health care system. Differences in health outcomes based on gender, race, ethnicity, age, and other social indicators are well documented (Smedley, Stith, & Nelson, 2002). To understand these disparities, previous research has focused on differences in access to health care (Agency for Healthcare Research and Quality, 2004) and, to a lesser extent, differences in the technical aspects of health care delivery, such as the receipt of specific medical services (Peck et al., 2004). More recently, researchers have examined the way doctors and patients interact to understand health disparities (Perloff, Bonder, Ray, Ray, & Siminoff, 2006). In the current study, we focus on the latter: How doctor–patient interactions differ in ways that likely contribute to health disparities. We aim to advance our understanding of disparities in health and health care by examining particular processes in the doctor–patient encounter. More specifically, we examine differences in the way doctors and patients interact in terms of the primary functions of the medical encounter—information gathering, communicating information, and relationship building—and doctor and patient characteristics.
Health Disparities
Health disparities are differences in the incidence, prevalence, mortality, and burden of diseases, and other adverse health conditions that exist among specific population groups (Braveman, 2006). Disparities between Whites and racial and ethnic minority groups are one of the most consistent and prevalent findings (Institute of Medicine, 2002). For example, the life expectancy for a White child born today is almost 5 years longer than a Black child (78.5 years vs. 73.6 years; Heron, Hoyert, Xu, Scott, & Tejada-Vera, 2008). There are many examples of disease-specific disparities between Whites and racial and ethnic minorities: diabetes, obesity, heart diseases, cancer, influenza, AIDS, and others (Centers for Disease Control and Prevention, 2008; Heron et al., 2008; Institute of Medicine, 2002; Mead et al., 2008).
Health disparities are not limited to race and ethnicity differences. Differences exist based on gender, education, place of residence, socioeconomic status, and others. For example, women outlive men in the United States by about 5 years (80.2 and 75.1, respectively; National Center for Health Statistics, 2008). Yet, women tend to have poorer health than men in terms of reported symptoms, missed days of work, use of medication, number of chronic conditions, self-reported health status, and use of health care services (MacIntyre, Hunt, & Sweeting, 1996). Those from lower socioeconomic strata have higher incidence and prevalence of disease such as asthma, diabetes, influenza, and pneumonia, and are much less likely to seek care or receive treatment for medical conditions (U.S. Department of Health Human Services, 2000). Likewise, those with less education have higher rates of morbidity and mortality. Recent evidence suggests the gap between the educated and less educated is getting bigger (Meara, Richards, & Cutler, 2008). As a final example, rural Americans have higher incidence and prevalence of many diseases and lower life expectancy compared with urban and suburban residents (Institute of Medicine, Committee on the Future of Rural Health Care, 2005).
These disparities in health are the product of many different factors, such as unequal access to health care services, socioeconomic factors, hazardous work and environmental conditions, nutrition, and differences in health behavior (Geiger, 2002; Marmot & Wilkinson, 2006). Initial efforts to understand health disparities focused on access to medical care. Health insurance facilitates access to health care. Previous studies document that uninsured people are less likely to receive medical care (Hadley, 2007), are more likely to die early (Institute of Medicine, 2004), and have poor health status (Centers for Disease Control and Prevention, 2004). The uninsured report more problems getting care, are diagnosed at later disease stages, and get less therapeutic care. They are sicker when hospitalized and more likely to die during their stay (Hadley, 2002). Like health disparities, racial and ethnic minorities are disproportionately represented among those without insurance. In 2008, more than 46 million Americans did not have health insurance (DeNavas-Walt, Proctor, Smith, & U.S. Census Bureau, 2009). About 10% of the White population do not have health insurance; for Blacks, Hispanics, and American Indians/Alaska Natives, the rates are 2 to 3 times higher (19.1, 30.7, 31.7, respectively; DeNavas-Walt et al., 2009).
Although access to medical care explains much of the differences in health outcomes, it does not explain all the differences. Blacks with access to health care, for example, still fare worse than Whites on many health indicators (Horner et al., 2002). Consequently, the focus of health disparities research broadened to include analyses of the delivery of health care and the doctor–patient encounter. Many of the early analyses of doctor–patient interaction focused on technical aspects of health care. Specifically, these studies focused on the receipt of specific medical services, such as medications, tests, and procedures (Peck et al., 2004). These studies highlighted differences in treatment (Maynard, Fisher, Passamani, & Pullum, 1986) and specific medical outcomes (Horner et al., 2002; Maynard et al., 1986).
Over the last decade or so, researchers again have broadened the focus of inquiry to include the conduct of the medical encounter, that is, the style and nature of interaction and communication between doctors and patients (Roter & Hall, 1992). Studies suggest an association between the nature of interaction and patient satisfaction (Fiscella et al., 2004; S. Williams, Weinman, & Dale, 1998), better adherence to therapeutic recommendations (Safran et al., 1998), and various physical and mental health outcomes (Hall, Roter, & Katz, 1988; Rao, Weinberger, & Kroenke, 2000; Safran et al., 1998). In general, studies focusing on the nature of doctor–patient communication and patient outcomes suggest that visits that are more patient-centered have better outcomes (Epstein et al., 2005). Patient-centered encounters are those characterized by shared decision making so that physicians and patients contribute to the decision-making process, and patients’ desires and expectations are incorporated into the medical decision-making process (Gerteis, Edgman-Levitan, Daley, & Delbanco, 2002; Platt et al., 2001).
Not surprisingly, previous research suggests that patient and physician characteristics, such as gender and race, are associated with the nature of doctor–patient interaction. The gender of physicians and patients, for example, are related to differences in communication patterns. Male physicians are less empathetic in their communication style and generally ask fewer questions of and provide less information to their patients (Roter, Hall, & Aoki, 2002). Female patients prefer a more active role in the medical encounter (Arora & McHorney, 2000) and ask more questions (Roter et al., 2002). Racial and ethnic minority patients (especially, Blacks and Hispanics) tend to receive lower quality care (Hooper, Comstock, Goodwin, & Goodwin, 1982) and are typically less satisfied with their medical care (Barr, 2004). Patients in race- and gender-concordant relationships tend to be more satisfied (Cooper-Patrick et al., 1999).
The Doctor–Patient Encounter
We aim to advance our understanding of disparities in health and health care by examining the specific processes in the doctor–patient encounter. Doctors and patients typically create and develop their relationship in the doctor’s office, more specifically in the examination room. The substance of the interaction between patients and doctors in the exam room is the medical interview. The medical interview is the primary medium of health care; the encounter primarily entails doctors talking with patients and patients talking with doctors (Roter & Hall, 1992). Moreover, the medical encounter generally is not arbitrary dialogue between patient and doctor. Rather, there is a typical structure, format, and content of the medical interview (Clark, Lipkin, Graman, & Shorey, 1999). An often-used framework to describe the medical interview focuses on the primary functions of the medical interview. Functions refer to the general goals of the medical encounter. The three primary functions are gathering information, communicating information, and developing and maintaining a therapeutic relationship (Cohen-Cole & Bird, 1991; Lazare, Putnam, & Lipkin, 1995).
Information or data gathering refers to gathering data from the patient to understand the patient’s chief complaint or concern. Information gathering is widely recognized as the primary purpose of the medical interview. Communicating information refers to informing and educating patients about their condition or illness and providing them with the tools and motivation to adhere to the treatment plan. Finally, developing a therapeutic relationship refers to developing rapport with the patient, responding appropriately to patient emotions, and facilitating patient participation in the decision making (Cohen-Cole & Bird, 1991). These three functions—although separate in purpose—are related to one another. For example, a patient who does not trust or like his or her physician (poor relationship) will not disclose complete information (poor information gathering).
Medical interviews may be highly structured and may be conducted in similar ways from one physician to the next. The way physicians carry out these functional components of the medical interview, however, varies from physician to physician. Some physicians conduct the medical interview in ways that include patient input (more symmetry in control and influence); other physicians include patient input and preferences to a lesser degree (asymmetry in control and influence). The extent to which patient input and influence are part of the segments and functions of the medical encounter determines the nature or model of interaction between doctors and patients.
Research Questions
Our central focus is how doctor–patient interactions differ in ways that likely contribute to health disparities. Previous research suggests that doctors and patients interact differently along a number of dimensions, such as race and gender (Smedley et al., 2002). Few studies, however, have examined differences in interaction as they relate to specific elements—the functions—of the medical interview. We examine whether medical encounters differ by patient and physician characteristics in terms of the primary functions of the encounter (data gathering, communicating information, and building relationships) as well as patient satisfaction with those functions. In addition, we assess these differences from multiple perspectives. Much of the previous research uses assessments from patients’ self-reports or from third-party coders’ ratings (Zolnierek & DiMatteo, 2009). We use patient and coder assessments as well as objective data from the actual conduct of the encounter (i.e., measures independent of patient or coder perceptions). We examine differences by patient characteristics (race, gender, education) and physician characteristics (race, gender, clinical experience).
Method
Sample
To address these questions, we use data collected from study participants (patients and doctors) in a large family medicine practice over an 11-month period in 2007 and 2008. In all, 17 physicians and 221 of their patients participated in the study. Patients were selected from the patient pool of participating physicians. Patients were identified from daily appointment schedules and approached while waiting to see their providers. To be eligible for the study, patients had to be 18-years-old or older, speak and understand English, and had to have a scheduled appointment with the physician who provided their usual source of primary care.
Data Collection
We obtained consent from physicians prior to recruiting patient participants. We obtained consent from patients on the day of their visit. After obtaining consent, trained interviewers administered a previsit questionnaire to assess patients’ general demographic characteristics and information about the purpose for that day’s visit. Immediately after the doctor’s visit while at the clinic, patients completed a postvisit questionnaire to assess what occurred during the visit (tests, procedures, medications, etc.), their satisfaction with the visit and physician, and how they would characterize the interaction with their physician.
The clinic visits were audiotaped and coded by trained coders. The tapes were coded using a coding scheme similar to the Roter Interaction Analysis System (RIAS). The RIAS is a method of coding doctor–patient interaction during the medical visit (Roter & Larson, 2002). It is the most often used method for coding doctor and patient encounters (Thompson, 2001). The RIAS method was influenced largely by Robert Bales, whose work focused on small group interaction during the problem-solving and decision-making process (Bales, 1950) as well as social exchange theories that focus on interpersonal influence, problem solving, and reciprocity (Molm, 2006). Like the RIAS system, we identified every statement or complete thought expressed during the visit (by patients and providers) into mutually exclusive and exhaustive categories. The categories correspond to the general functions of the medical interview described above. The RIAS differs from other methods designed to assess the doctor–patient relationship, including Bales’ Interaction Process Analysis (Bales, 1950) in several significant ways. The coding approach is tailored to exchanges specific to the medical encounter in that coding categories reflect the content and context of typical dialogue between patients and doctors during medical exchanges. In addition, identification and classification of verbal events are coded directly from audiotapes, rather than transcripts, which provide the ability to assess tonal qualities of interaction.
To code the audiotaped medical encounters, we created a coding sheet with operational definitions for the interactional variables. The coders trained by coding practice encounters not used in the analyses. The research staff monitored the training sheets and provided additional training as necessary. Once the trainers were assured the coders understood the coding categories and operational definitions, the audiotapes were coded.
Despite rigorous training and strict coding guidelines, subjective interpretation and coding variability is a possibility. We used several methods to minimize and assess coder variability. First, we used multiple coders who coded the encounters independently. Second, during the coding process, we performed periodic checks to ensure the coders stayed with training guidelines. Finally, after coding was complete, we performed analyses to determine the consistency between the coders. We evaluated interrater agreement by randomly selecting 10% of the audiotapes for double coding. We computed kappa (κ) statistics for a random selection of categorical variables. The κ statistic evaluates the extent of agreement between two or more independent evaluations and takes into account the extent of agreement that could be expected beyond chance alone (Gwet, 2010). We computed intraclass correlation coefficients (ICC) for numeric variables. The ICC is a measure of agreement between coders or raters used when observations are scaled on an interval or ratio scale of measurement (Gwet, 2010). We examined four variables for agreement between the coders. We examined the extent to which the coders agreed (κ statistic) on the overall assessment of how dominant the physician was compared with the patient (on a 1-5 scale) and how warm and friendly the physician was toward the patient (1-5 scale). We also examined the extent to which the coders agreed (ICC) on the amount of biomedical discussion between the doctor and patient and the amount of closed-ended questions asked by the physician. Agreement between the coders was very good. The κ coefficients ranged from 0.92 to 0.98; the ICC scores ranged from 0.88 to 0.97.
Dependent Variables
As noted above, we examine various aspects of the medical encounter. We group the different facets of the doctor–patient encounter into three categories of outcomes: those that assess the actual conduct of the encounter, the three functions of the medical interview (data gathering, communicating information, relationship building) assessed by patient and independent coders, and patient assessment of and satisfaction with the encounter. The appendix summarizes the measures. Each is discussed in turn below.
Conduct of the encounter
These variables measure objective elements of the encounter that are independent of participant or coder perceptions. Length of the visit measures the time from when the doctor entered the room and began the medical interview to the time the encounter concluded and the doctor and/or patient exited the exam room. The variable was measured in seconds and converted to minutes. Amount of physician talk measures the number of statements the physician makes relative to the total number of statements. Doctor communication control measures the extent to which the physician controls or directs the communication. The variable was calculated as a ratio of controlling questions and statements by the physician to controlling statements and questions by the patient. Controlling statements (and questions) are those statements that dictate action or response from the other participant in the encounter (Greenfield, Kaplan, & Ware, 1985; Stewart et al., 1995). Thus, physician communication control relates physician verbal control (physicians’ questions and orientations and patients’ giving information) to patient verbal control (patients’ questions and physicians’ information giving). A value greater than 1.0 indicates that physicians used more controlling language than patients. A value less than 1.0 indicates that patients used more controlling statements and questions than physicians. A value of 1.0 indicates equal usage of controlling language by both.
The variable physician-centered encounter is a cumulative measure of communication and interaction between the doctor and patient. The variable is intended to capture the distinction between a physician- and patient-centered encounter (Stewart et al., 1995). To create the variable, we clustered cases (encounters) that were similar along the dimensions of influence and control in the encounter. We clustered the encounters on six variables, three of which measured patient communication patterns and three that measured physician communication patterns. The variables are biomedical information giving, psychosocial exchanges, and questions (closed and open ended). Each variable is a ratio of all talk to control for length of the encounter. These three categories of variables describing interaction in the medical encounter, questions, biomedical information giving, and psychosocial talk (for patients and physicians) are the most often used to measure the dimensions of the encounter that reflect the patient-centered versus physician-centered continuum of interaction styles (Stewart et al., 1995). The cluster analysis produced observations with two categories: physician-dominated and patient-dominated encounters. The variable is binary, with 1 indicating a physician-dominated encounter.
Functions of the medical interview
The three basic functions of the medical interview are information gathering, communicating information, and relationship building. The functions were measured by coders and patients. The variables represent subjective assessments of the medical encounter by trained coders and the patient participants. The use of trained coders to assess qualities of the medical encounter has a long history in the study of doctor–patient interaction (Adler & Enelow, 1966; Kaplan, Greenfield, & Ware, 1989; Peck, 2011; Roter, 2000).
The coders did not link the ratings directly to specific events but assigned ratings based on their overall impression of the encounter on the different dimensions. The variables represent the coders’ assessment of physicians’ thoroughness and performance in terms of the medical interview and interpersonal style or manner in which the physician gathered data, communicated information, and developed a relationship with the patient.
Coders rated physicians on several items related to each function. Informing patients, for example, was measured by averaging ratings to the items: the doctor offers solutions to the patient, the doctor explains technical language, the doctor checks patient’s understanding, and the doctor provides direct answers to patient’s questions. Coders ranked the items from 1 to 5 (low to high). We calculated an average ranking across the number of items used to assess the dimension. In addition to the coder assessment of physicians’ skills related to technical aspects of the medical interview, coders rated physicians’ interpersonal skills and style (i.e., maintaining a therapeutic relationship). Physicians were rated along the dimensions of friendliness (e.g., the doctor is friendly, jokes, or makes personal remarks), respectfulness (e.g., the doctor shows respect for the patient), and attentiveness (e.g., the doctor is visually attentive to the patient). Like the other items, coders ranked a series of questions from 1 to 5 (low to high). We calculated an average ranking across the number of items used to assess the dimension of doctor–patient interaction. We calculated Cronbach’s alpha for all measures with more than one indicator. The alpha scores were all acceptable in magnitude and ranged from .69 (data gathering) to .92 (friendliness).
Patients assessed their satisfaction with the functions of the medical interview using a 5-point scale (1-5, low to high). Patients ranked their satisfaction with the dimensions of the encounter using a single question to assess the physician’s data gathering and communicating information skills. Patients ranked their satisfaction with the relationship building function by answering the same three questions that coders rated (physician’s level of friendliness, respectfulness, and attentiveness).
Patient satisfaction and assessment
These variables measure patient satisfaction, patient trust, and patient perception of the degree of participatory decision making. We measured overall patient satisfaction using a modified version of the Patient Satisfaction Questionnaire (PSQ Project Co-Investigators, 1989). The 10-item instrument focuses on humanistic attributes and the interpersonal skills of the physician. Respondents provided responses to questions such as, “How would you rate your physician’s performance in terms of using words you can understand when explaining your problems and treatment” and “letting you tell your story and listening carefully.” Responses to each item were recorded using a 1 to 5 scale, with 5 indicating higher satisfaction. The scores were standardized to a 0 to 100 scale, with a higher score indicating higher satisfaction.
We measured patient trust in physician using a modified version of the Trust in Physician Scale (Anderson & Dedrick, 1990; Thom, Ribisl, Stewart, Luke, & The Stanford Trust Study Physicians, 1999). The 11-item instrument evaluates an individual’s trust in his or her primary care physician in the domains of dependability, confidence, and confidentiality of information. All items are scored using a 5-point Likert-type format, with a combination of negatively and positively worded questions (e.g., “I trust my doctor to put my medical needs above all other considerations when treating my medical problems”). The scores were standardized to a 0 to 100 scale, with a higher score indicating higher trust.
Patient’s assessment of the nature of the encounter was measured using an instrument developed to assess level of participatory decision making in the medical encounter (Kaplan, Greenfield, Gandek, Rogers, & Ware, 1996). Patients rated their physician on questions such as, “If there were a choice between treatments, would this doctor ask you to help make the decision?” The scores were standardized to a 0 to 100 scale, with a higher score indicating higher participatory decision making. A higher score is indicative of a patient-centered encounter; a lower score is indicative of a physician-centered encounter.
Independent Variables
The primary independent variables are patient and physician demographic, and status characteristic variables.
Patient characteristics
We measured the patient characteristics race, gender, and education. All are self-reported by the patients. Race was measured using several categories (e.g., White, Black, Native American, Asian). For the current analyses, we use a binary measure of race: White and non-White. Patients who self-identified any race category other than White were classified as non-White. Gender is a binary variable indicating whether the respondent is male or female. Education is a measure of patient’s highest level of school completed. The categories are less than high school, high school graduate (or general educational development), some college (but no degree), college graduate, and graduate degree.
Physician characteristics
We measured the physician characteristics race, gender, and years of medical practice. Like the patient race variable, physician’s race was originally measured using multiple categories. For the current analyses, we use a binary measure that indicates whether the physician is White or non-White. Gender is a binary measure indicating whether the physician is male or female. Years of medical practice was self-reported by physicians and indicates how long the physician has been out of residency and practicing medicine. We transformed the measure into a binary variable indicating whether the physician had 8 or more years of practice versus less than 8 years of medical practice. A total of 8 years represents the median number of years of practice in the sample of physicians. The median cut point is somewhat arbitrary. There is little theoretical or empirical rationale in the literature to suggest another cut point. We analyzed the data using other definitional categories for physician experience. The results were not altered.
Physician–patient race and gender
In addition to the individual patient and physician characteristics, we created variables that represent combined physician and patient demographics. We created binary variables to indicate the race of doctor and patient (e.g., White physician–White patient, White physician–non-White patient). Likewise, we created binary variables to indicate the gender of doctor and patient (e.g., female physician–male patient, female physician–female patient).
Analysis
Our focus is not on predicting a specific patient outcome; rather, the focus is on describing whether differences in how doctors and patients interact are based on patient and physician characteristics. The analyses are largely descriptive and intended to generate hypotheses. We present analyses showing differences in various outcomes by patient and physician characteristics. The analyses are adjusted for patient age and length of the doctor–patient relationship (measured by the number of visits between doctor and patient in the previous 12 months). The specific statistical test used is determined by the variable under examination. For continuous, normal variables, we report findings from ordinary least squares regression. For categorical variables, we report findings from binomial and multinomial logistic regression. All significance tests are corrected to account for nonindependent data (R. L. Williams, 2000). The correction is necessary because the data consist of patients clustered by physicians. As such, the observations are not independent.
Results
Characteristics of the Sample
Basic characteristics of the study participants (patients and physicians) are presented in Table 1. The patient sample has slightly more females than males (52.5% and 47.5%, respectively). A little more than half (56.1%) of patient respondents are White. The non-White respondents are primarily African American (26.2%), Asian (4.1%), and those who identified as another race or a combination of races (12.7%). The patient participants are mostly high school educated or higher. The median education level is more than a high school education but less than a college degree. About a quarter of the patients (24.4%) have a college education. The income for patients in the study is relatively low. The largest income category is less than US$30,000 per year. The relatively low income level is likely related to the average age of the study population. The patients are older than the general population; the median age is 60 years. More than half of the patients are between 56 and 75 years old. The slightly older age profile of the patients is likely due to the makeup of the study clinicians. Although all the physicians in the study are associated with the family practice clinic, at least two of the physicians list geriatrics as their board-certified subspecialty.
Characteristics of the Study Sample

Physician characteristics are also presented in Table 1. A total of 10 of the 17 physicians are male (58.8%). Most physicians (82.4%) are White. The sample includes three non-White physicians. Those non-White physicians account for about one fifth (19.5%) of the medical encounters. The majority (52.9%) of physicians have practiced medicine 8 years or more. The physicians’ ages range from 33 to 54, with slightly more than half (52.9%) 40 years old or younger.
The Medical Encounter and Patient Characteristics
Differences in several facets of the doctor–patient encounter by patient characteristics (race, gender, education) are presented in Table 2. The results show that there are differences in the medical visit based on race, gender, and patient education. In terms of the objective measures of the conduct of the medical visit, there are significant differences based on patient race and education. White patients have significantly longer medical visits than non-White patients (28.5 vs. 23.9 min). The 4.5-min difference represents a 20% longer visit for White patients. Physicians talk significantly more in encounters with non-White patients (55.7%). The verbal control measure is also different for White and non-White patients (2.9 vs. 2.0, respectively). The numbers are ratios of the number of controlling statements and questions by doctors to the number of controlling statements and questions by patients. Physicians had almost 3 times more controlling statements than White patients. Physicians had 2 times more controlling statements than non-White patients. There were no differences based on patient gender in terms of length of visit, amount of physician talk, physician verbal control, or level of patient-centered interaction.
Differences in the Medical Encounter by Patient Characteristics
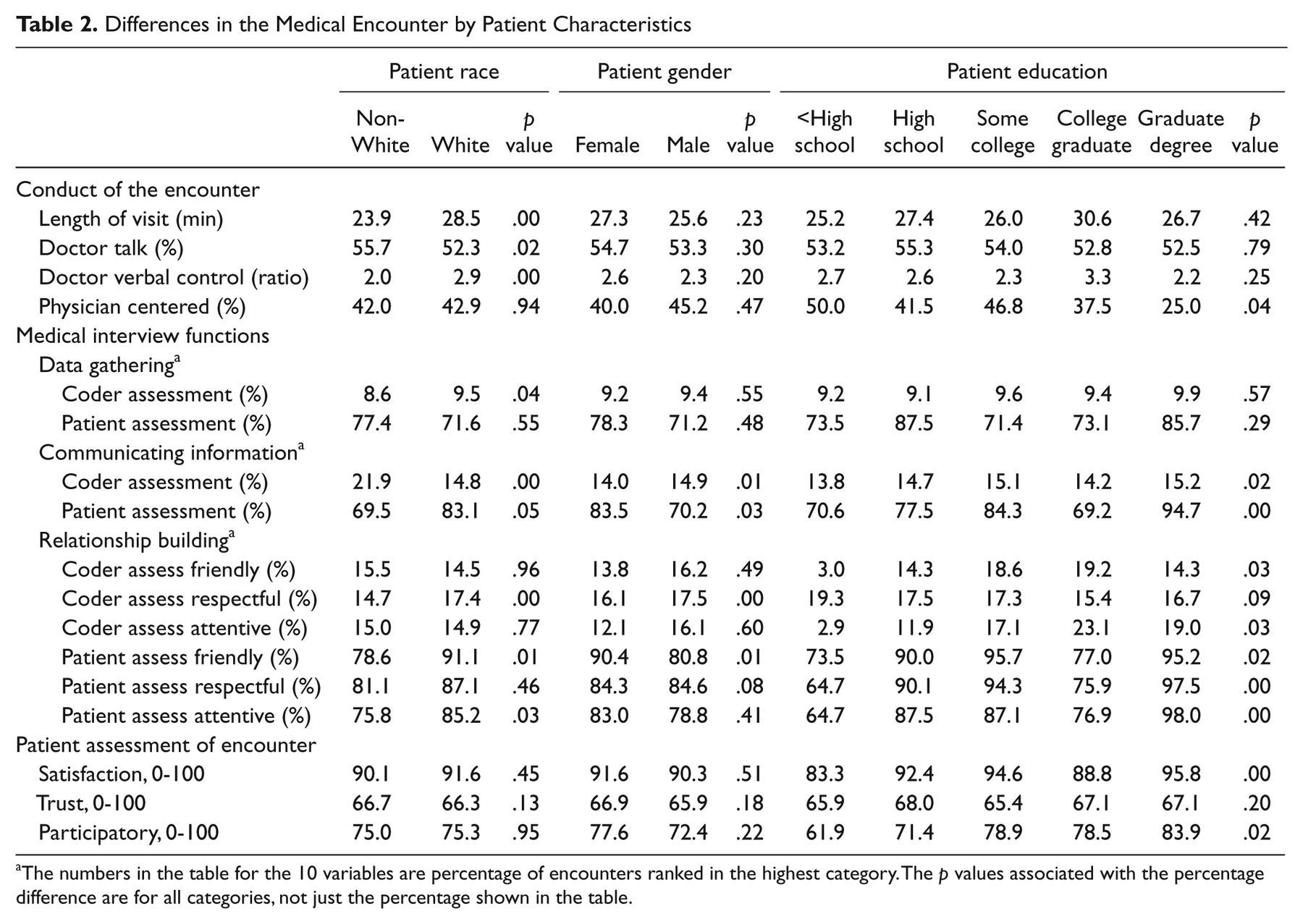
The numbers in the table for the 10 variables are percentage of encounters ranked in the highest category. The p values associated with the percentage difference are for all categories, not just the percentage shown in the table.
There are significant differences in the conduct of the encounter for patients with different education levels. Patients with lower levels of education are more likely to have a physician-centered encounter. A total of 50% of the respondents with less than a high school education had an encounter in which the physician dominated the dialogue and excluded the patient from decision making. Patients with a college or graduate degree were much less likely to have a doctor-centered encounter (37.5% and 25.0%, respectively).
Differences in data gathering, information giving, and relationship building as rated by coders and patients are also evident in Table 2. All but 1 of the 10 variables shows significant differences on at least one patient characteristic. The numbers in the table for the 10 variables are percentage of encounters ranked in the highest category. The p values associated with the percentage difference are for all categories, not just the percentage shown in the table.
Coders rated physician data gathering differently for Whites and non-Whites. There were not significant coder ratings based on patient gender or education. Coders rated the function of communicating information to patients differently for each patient characteristic. Coders rated physicians communicating information better for non-Whites, males, and those with more education. In terms of relationship building, there were significant differences based on coder ratings. Coders rated the interpersonal style and relationship building efforts of physicians higher in terms of friendliness toward those with higher levels of education. Coders rated physicians as more respectful with White and male patients. Coders rated physicians as more attentive with patients who had higher levels of education.
Ratings based on patient ratings also showed significant differences. In terms of communicating information, White patients, female patients, and those with more education rated their physician highly. Similarly, White, female, and more highly educated patients rated physician friendliness higher. The only patient characteristic related to physician respectfulness was education level; higher educated patients rated physicians higher. White and educated patients reported higher rates of satisfaction with physician attentiveness. There were no differences in ratings of data gathering based on patient race, gender, or education.
The final set of variables is patient assessment of the encounter and overall satisfaction. Patient assessment and satisfaction with the medical encounter differs only by education level. More highly educated patients report higher levels of participatory decision making and overall satisfaction. There are differences in medical encounters based on patient race, gender, and education. Only informing the patient was significant for all three patient characteristics. Only trust in physician was not significant for any of the three patient characteristics. The differences in encounters generally favored White and educated patients.
The Medical Encounter and Physician Characteristics
Table 3 shows the differences in the same facets of the doctor–patient encounter discussed above by physician characteristics (race, gender, years of practice). The results suggest that physician characteristics, especially race and gender, influence the conduct of the medical encounter. Non-White physicians talk more (56.6%) in the medical encounter than do White physicians (53.4%). White physicians are more than 2 times more likely to have a physician-centered encounter. Almost half (47.6%) the encounters with White physicians are physician centered. By contrast, about one fifth (20.6%) of encounters in which the physician is non-White are physician centered. Physician gender is also associated with several important differences in the conduct of the medical encounter. Female doctors talk more in the encounter than do male physicians. Female physicians, however, tend to use less controlling statements and questions than male physicians. The ratio of controlling statements by physicians and controlling language by patients is 2.1 for females; female physicians use controlling language at slightly more than double the rate of patients. Male physicians, by contrast, average almost 3 times (2.7) the number of controlling statements compared with their patients. Male doctors are more than twice as likely to have a physician-centered encounter as female physicians (53.8% and 26.0%, respectively). Physician experience—years of service—is associated with only one difference in the conduct of the medical encounter: percentage of encounter that the physician spoke. Doctors with fewer than 8 years of medical practice talk on average more (56.5%) than doctors with more than 8 years of experience (51.1%).
Differences in the Medical Encounter by Physician Characteristics

The numbers in the table for the 10 variables are percentage of encounters ranked in the highest category. The p values associated with the percentage difference are for all categories, not just the percentage shown in the table.
There are several significant differences in the functions of the medical interview by physician characteristics, although there are fewer differences than those by patient characteristics. In fact, none of the patient ratings of data gathering, communicating information, and building relationships differed by physician characteristics. Coder ratings differed by physician gender for data gathering, with males ranked slightly higher than females. There were also significant differences for White and non-White physicians on communicating information, friendliness, and respectfulness. The differences were not uniformly in the same direction. Neither White nor non-White physicians were consistently rated higher or lower. Non-White physicians were rated lower than White physicians on information giving (12.9% and 14.9%, respectively) and respectfulness (15.6% and 17.3%, respectively). White physicians were rated lower than non-White physicians on friendliness (10.7% and 32.6%, respectively).
Interestingly, there are no differences in patient assessment and satisfaction by physician characteristics. Patients reported no differences in trust or satisfaction with physicians based on physician race, gender, or experience. Not only were none of the differences statistically significant, there were no differences marginally significant or near significant. Also of interest is the lack of differences based on physician experience. Years of medical practice have virtually no impact on the doctor–patient relationship. More accurately, years of medical service measured as 8 or more years and less than 8 years have virtually no impact on the doctor–patient relationship. Recall that the categories were created using the median as a cut point, a somewhat arbitrary cut point. We did, however, alter the cut points. We made the cut points as low as 2 years or less (the minimum years of service in the sample of physicians) versus more than 2 years. We also ran the analyses using categories of more than 18 years of service versus 18 or fewer years of service. The results were not altered. Patient and coder ratings of the encounters did not differ by physician’s years of service.
The Medical Encounter and Patient–Physician Characteristics
Differences in the medical encounter by combined (physician and patient) characteristics for race and gender are presented in Table 4. Physicians (White and non-White) spend the most time with White patients. The longest average encounters are between non-White physicians and White patients (30.4 min). Encounters between non-White doctors and non-White patients are on average the shortest encounters in duration (22.9 min). The amount of physician talk is highest in encounters between non-White doctors and non-White patients (56.8%). Encounters between White doctors and White patients have the lowest level of physician talk (52.1%). The content of the language, however, shows a different pattern. Physicians (White and non-White) show higher levels of doctor verbal control with White patients (2.9 for White and non-White doctors). Encounters between non-White doctors and patients have the lowest levels of doctor verbal control (1.8). Similarly, non-White physicians and patients have the lowest percentage of physician-centered encounters (6.7%). White physicians are more likely to have physician-centered encounters, especially with non-White patients (54.8%).
Differences in the Medical Encounter by Patient and Physician Characteristics
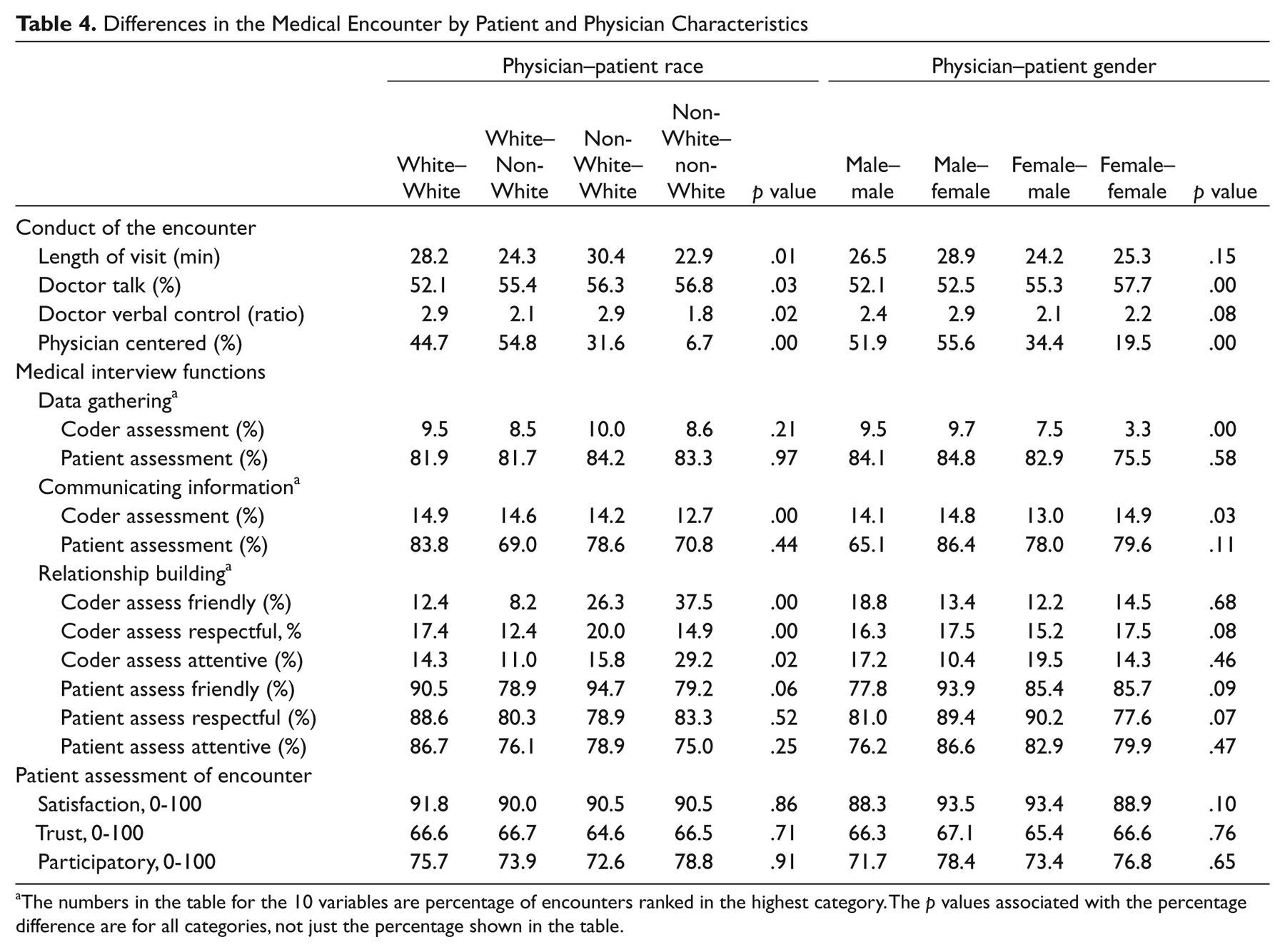
The numbers in the table for the 10 variables are percentage of encounters ranked in the highest category. The p values associated with the percentage difference are for all categories, not just the percentage shown in the table.
Patient and physician gender categories show several differences as well. The amount of physician talk as a percentage of the total talk differs significantly by gender categories. Gender-concordant encounters with males have the lowest percentage of doctor talk (52.1%). By contrast, encounters with both female participants have the highest percentage of doctor talk (57.7%). Medical encounters with female physicians are less likely to be physician centered, especially when the patient is female (19.5%). Male physicians are more likely to have physician-centered encounters, particularly with female patients (55.6%).
There are several significant differences in the execution of the functions of the medical interview as rated by coders. Data gathering differed by gender categories. Female-concordant encounters had the lowest ratings of data gathering, whereas encounters between male physicians and female patients had the highest ratings. There were differences in communicating information for the race and gender categories, with race-concordant encounters with non-White participants having the lowest average rating and White-concordant encounters having the highest rating.
For relationship building, coders rated differences between race categories for all three partnering variables. The results show that, in general, White physicians were rated lower than non-White physicians. Encounters with White physicians and non-White patients had the lowest ratings for physician friendliness, respectfulness, and attentiveness.
There were no statistically significant differences in the medical interview functions by patient and physician gender and race categories as rated by patients. Likewise, there were no statistically significant differences in patient satisfaction, trust, or assessment of participatory decision making in the encounter by the combined race and gender categories.
Conclusion and Discussion
In this study, we sought to determine how and where in the medical encounter differences or disparities occur. The results suggest medical encounters differ in important ways depending on patient and physician characteristics. These differences can create and contribute to health disparities. Patients who are more active participants in the medical decision-making process and more satisfied with the medical encounter, for example, have higher rates of adherence to treatment recommendations, which in turn leads to favorable physical and mental health outcomes (Safran et al., 1998).
We examined 17 components of the medical encounter (4 objective measures coded directly from the audiotapes, 5 subjective measures from trained coders, and 8 subjective measures from patients). We found the most differences in medical encounters examining patient characteristics. We found 9 differences based on patient race, 4 gender differences, and 11 differences based on patient education. The medical encounters also differed by physician characteristics. We found 5 significant differences based on race, 5 based on gender, and 1 based on physician experience. In addition to examining physician and patient characteristics separately, we examined similar and dissimilar doctor–patient dyads based on race and gender. Again, we found significant differences: 8 significant differences by race and 4 by gender. Overall, we found almost twice as many significant differences based on race (22) compared with gender (13). This finding is consistent with previous research that suggests patients have only a weak preference for same-gender physicians, especially when the visit does not focus on gender-specific issues (Roter & Hall, 2001).
Several specific findings are particularly noteworthy in the context of doctor–patient interaction and health disparities. First, the differences in encounters generally followed patterns that might be expected given the patterns of health disparities. It is well documented that racial and ethnic minorities (non-Whites), the less educated, and the poor have a higher burden of disease and adverse health conditions compared with Whites (Institute of Medicine, 2002). If doctor–patient interaction is related to health outcomes, we might expect to find these same groups disadvantaged in terms of the quality of interaction with their physicians. Indeed, we found non-Whites, and the less educated generally had encounters characterized by shorter visits, more physician centered, and lower satisfaction. That finding, however, was not universal. Non-White patients, for example, had higher levels of verbal control and were given more information by their physicians. This “advantage” remained after controlling for physician characteristics.
Second, our results indicate that non-White, male, and less educated patients are consistently less satisfied with their physician and interaction compared with White, female, and educated patients. These differences, however, were largely attenuated after controlling for physician characteristics.
Third, we found interesting differences between coder assessment of elements of the encounters and patient satisfaction with those same elements. For example, coders rated encounters with non-White patients as having higher levels of information giving by the physician. Yet, non-White patients reported lower levels of satisfaction with information giving by the physician. Similarly, coder assessments of information giving in encounters with male patients were significantly higher than encounters with female patients. Male patients, though, rated their satisfaction with physician information giving lower.
Last, we found that physician characteristics have little impact on patient assessment and satisfaction with the medical encounter. Patients reported no differences in trust or satisfaction with the physician or encounter based on physician race, gender, or experience. This suggests patients may be evaluating the medical encounter itself, or their own sociodemographic characteristics are influencing their evaluations. This is somewhat counter to research that suggests patients prefer concordant medical encounters (Cooper-Patrick et al., 1999).
As usual, the findings must be interpreted with some caution given the limitations of our study. The most notable limitation is the sample. Although we randomly selected physicians and patients for inclusion in the study, they did not necessarily participate or refuse randomly. As such, it is difficult to know whether the sample is representative of all medical encounters or even representative of encounters at the study site. The sample of patients is slightly older than national figures. It could be that older patients are different in ways related to doctor–patient interaction. Older patients may be more likely to concede some control and influence to physicians because they have experienced more traditional interaction patterns in the past. Preliminary analyses of the data (not shown), however, do not suggest older patients and doctors interact differently.
Another potential limitation related to the sample is the relatively small number of minority physicians. A larger study that oversamples racial and ethnic minority physicians would provide more evidence and assurance regarding the ways in which White and non-White physicians interact with patients. A larger study with more minority physicians would also allow for a finer distinction along racial and ethnic lines, rather than the simple race categories of White and non-White. Most of the limitations of the sample diminish statistical power to detect differences, meaning the differences we found are likely a conservative estimate of how social characteristics affect doctor–patient interaction.
Our results suggest that medical encounters differ by physician and patient characteristics, and point to several potential avenues of inquiry of the encounter between doctors and patients. One important issue revolves around the impact of the different elements of the medical interview on patient outcomes. That is, which functions of the medical interview—data gathering, communicating information, or building relationships—matter most for different patient outcomes, such as satisfaction or adherence and compliance? The current study documents differences in the way physicians carry out the functions of the medical interview. Future research should parse out the effects of these differences.
As noted above, an important finding from the current study shows third-party coders and participants (patients) differ in their assessment of elements of the doctor–patient encounter. We did not attempt to answer questions or hypothesize about these differences. Our purpose of using coder and patient ratings was simply to have multiple perspectives to better understand the process of the medical interview. The differences between coders and patients, however, beg the question of which assessment matters most. That is, what matters more—what happened in the interaction or what patients (or other participants) perceive happened. In addition, the answer to the question may depend on the outcome in question.
Finally, future studies could focus on the mechanisms through which the differential treatment takes place to help develop theoretical explanations. Two frameworks appear promising: status characteristics theory and cultural health capital. Status characteristics theory focuses on how status characteristics (e.g., race and gender) of members of a small, task-oriented group determine the power and influence in that group (Berger, Cohen, & Zelditch, 1972). Limited empirical research suggests status characteristics theory as a useful framework for understanding the mechanisms and processes of differential interaction in medical encounters (Gallagher, Gregory, Bianchi, Hartung, & Harkness, 2005). The idea of cultural health capital also shows promise as a framework for understanding this phenomenon (Shim, 2010). The framework posits that physicians interact more positively with patients who have cultural health capital. Cultural health capital refers to a set of skills that allow patients to communicate health-related information to providers in a medically understandable and efficient manner (Shim, 2010). Cultural health capital has yet to be tested empirically. Both frameworks provide innovative ways of conceptualizing the doctor–patient interaction and insight into the process through which inequalities occur in the medical encounter.
Footnotes
Appendix
List of Dependent and Independent Variables
| Dependent variable | |
|---|---|
| General conduct of the encounter | Data source: directly from audiotaped medical encounters |
| Length of visit | Length of visit in minutes |
| Doctor talk | Ratio of physician to patient statements |
| Doctor verbal control | Ratio of physician to patient controlling statements/questions |
| Physician-centered encounter | Composite measure from coded categories |
| Functions of the medical interview | Data source: patient questionnaire and coder assessment |
| Data gathering | |
| Physician data gathering | Coder assessment of physician gathering data/information |
| Physician data gathering | Patient rating of physician data/information gathering (4-item) |
| Communicating information | |
| Physician informing patient | Coder assessment of physician communicating information |
| Physician informing patient | Patient satisfaction with physician communicating information |
| Relationship building | |
| Physician friendly | Coder assessment of physician interpersonal style: friendly |
| Physician respectful | Coder assessment of physician interpersonal style: respectful |
| Physician attentive | Coder assessment of physician interpersonal style: attentive/engaged |
| Physician friendly | Patient satisfaction with physician friendliness |
| Physician respectful | Patient satisfaction with physician respect |
| Physician attentive | Patient satisfaction with physician attentiveness |
| Patient assessment of interaction | Data source: patient postvisit interview/questionnaire |
| Patient satisfaction | Overall patient satisfaction scale (10 items), 0-100 |
| Trust in physician | Patient Trust in Physician Scale (11 items), 0-100 |
| Participatory decision making | Patient rating of participatory decision making (3 items), 0-100 |
| Independent variables | |
| Patient characteristics | Data source: patient previsit interview/questionnaire |
| Race | Self-report race, White or non-White |
| Gender | Self-reported gender, male or female |
| Education | Self-reported education categories |
| Physician characteristics | Data source: physician previsit interview/questionnaire |
| Race | Self-reported race, White or non-White |
| Gender | Self-reported gender, male or female |
| Years of medical practice | Self-reported years of medical practice |
| Physician–patient characteristics | Data source: patient and physician interview/questionnaire |
| Physician–patient race | White–White, White–non-White, non-White–White, non-White–non-White |
| Physician–patient gender | Male–male, male–female, female–male, female–female |

Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.