
Abstract
Refugees and migrants in need of protection (MNP) experience high levels of psychological distress and somatic symptoms—physical symptoms linked to stress. While a large body of literature explores the relationship between pre-migration trauma and health, less is known about the role of post-migration stressors. Drawing on a novel 13-week intensive panel survey (N=247 individuals; 3,093 observations) and in-depth interviews (N=65) with MNP in Costa Rica, I examine the relationship among stressors, psychological distress, and physical symptoms in the receiving context. Quantitative analysis highlights that post-migration stressors, including economic precarity and discrimination, are strongly associated with heightened psychological distress, which in turn increases the likelihood of somatic symptoms. Interview data corroborate these results and further uncover how MNP perceive and articulate the process of somatization. This study advances understanding of the dynamic pathways linking stressors, psychological distress, and physical health, offering both theoretical insights and practical recommendations for service providers and policymakers.
Amid the backdrop of intensifying global threats such as armed conflict and political persecution, an unprecedented wave of people is fleeing across international borders. An estimated 52 million people are currently considered “migrants in need of international protection” (MNP), a designation used by the United National High Commissioner for Refugees (UNHCR 2025b) to encompass recognized refugees, asylum-seekers, individuals with temporary forms of protection, and those who have been “forcibly displaced across international borders.” This broader category is significant because it includes migrants who face serious threats but fall outside narrow legal definitions of refugeehood (UNHCR 2025b).
MNP face compounded vulnerabilities stemming from pre-migration trauma, displacement, and the challenges of adjusting to new environments (Benabdeljlil 2022; Rohlof, Knipscheer, and Kleber 2014). After migration, they encounter significant structural challenges, including economic hardship, housing instability, discrimination, family separation, and legal precarity (Goodkind et al. 2021; Schweitzer et al. 2011; Weitzman, Blanton, and Brenes Camacho, 2025). These stressors exacerbate a range of mental and physical health issues and have been collectively described as the “social determinants of health in the post-migration context” (Hynie 2018:297).
There is an increasing cross-disciplinary consensus—long anticipated by the Stress Process Model (Pearlin et al. 1981)—that stressful experiences affect psychological states, which in turn undermine physical health (Cohen, Gianaros, and Manuck 2016; Goldring and Bolger 2021). Stress from difficult experiences leads to negative emotional responses or “psychological distress,” which triggers multisystem physiological responses, including immune system activation, inflammatory responses, and neuroendocrine fluctuations (Almeida 2005; Epel et al. 2018; Pearlin et al. 1981). These changes can produce physical symptoms such as pain, sleep disturbances, or gastrointestinal issues (Epel et al. 2018; Goldring and Bolger 2021)— tangible manifestations of stress “getting under the skin” (McEwen 2012).
Although often referred to as “somatization,” this concept remains complex and contested (De Gucht and Fischler 2002). Traditional definitions of somatization emphasize “medically unexplained” symptoms or somatoform disorders, but this framing can obscure the broader physiological mechanisms linking stress to physical symptoms (Goldberg et al. 2016; Löwe et al. 2022). In this study, I adopt a broader framework of somatic processes, emphasizing the interconnected pathways through which stressors, psychological distress, and physical symptoms interact (Goldring and Bolger 2021). This perspective situates somatic symptoms as measurable outcomes of stress-induced physiological changes rather than as unexplained phenomena, aligning with contemporary understandings of stress and health (Epel et al. 2018; McEwen 2012).
These stress-induced symptoms represent a significant public health challenge with widespread implications for healthcare systems and patient wellbeing (Vigo, Thornicroft, and Atun 2016). Individuals with somatic symptoms utilize medical care at higher rates, incur greater healthcare costs, and report poorer quality of life (Barsky, Orav, and Bates 2005). Among migrants, somatic complaints are often the most common reasons for seeking primary care in new destinations (Aragona et al. 2010; Lin, Carter, and Kleinman 1985), placing additional strain on already overburdened healthcare systems and potentially hindering successful resettlement (Tonui 2022). In Costa Rica, asylum seekers and refugees can access public healthcare through various programs, including a UNHCR supported agreement with the national health system (UNHCR 2025a). 1
MNP experience higher rates of somatic symptoms, partly due to their high prevalence of pre-migration trauma (Gupta 2013). While extensive research has explored the relationship between trauma and physical symptoms (Aragona et al. 2010; Benabdeljlil 2022; Hondius et al. 2000), most of this work relies on cross-sectional data, which cannot capture how somatic symptoms evolve over time in the post-migration context (Rohlof et al. 2014).
A central question thus remains: what triggers somatic symptoms in the receiving context? A key challenge in understanding post-migration somatic symptoms lies in disentangling the effects of new stressors from pre-migration conditions. Stressors such as economic precarity and legal insecurity are shaped by prior experiences, making it difficult to isolate their unique contributions to psychological distress and somatic symptoms. Addressing this requires panel data capable of controlling for both observed and unobserved confounders, such as pre-migration trauma and fixed demographic characteristics.
However, due to data collection challenges among this hidden and highly mobile population, who may be suspicious of researchers, panel data is scarce. To address this gap, I leverage data from one of the first intensive panel studies of MNP worldwide (Weitzman et al. 2024). These data allow me to use person fixed effects models, controlling for stable characteristics and isolating the role of post-migration stressors, thus providing a clearer understanding of what impacts mental and physical health in the receiving context.
While panel data provide a robust quantitative foundation, integrating qualitative data enhances this study by offering insights into how MNP perceive and articulate their experiences of somatic symptoms. For a population facing significant barriers to healthcare access, qualitative narratives provide critical depth and context, illuminating the social forces that shape both mental and physical health outcomes in ways that quantitative data alone cannot capture.
This paper presents a mixed-methods study on the interplay between stressors, psychological distress, and somatic symptoms among MNP in Costa Rica, a key destination in the Americas that is experiencing a surge in migrant arrivals (UNHCR 2023). Drawing on a 13-week survey panel and 65 in-depth interviews with adult MNP living in Costa Rica, I aim to address the following research questions: What stressors trigger psychological distress and physical symptoms among MNP in the post-migration context? How long do physical symptoms persist after fluctuations in stressors and psychological distress? How do MNP perceive and articulate the pathways through which stressors and psychological distress impact their physical health?
Through these comprehensive analyses, I make three key contributions. First, I illuminate the pathways through which post-migration stressors impact physical health, both directly and indirectly through psychological distress, with factors such as economic precarity and housing insecurity playing a central role. My fixed effects approach underscores the sensitivity of mental and physical distress to the structural stressors that MNP routinely face, net of fixed pre-migration factors that are associated with these stressors. Next, I reveal how MNP not only experience but also recognize and articulate these interconnected somatic processes. Lastly, I establish the predominantly immediate nature of the relationship between physical symptoms and stressors and psychological distress, which can resolve quickly after situational changes or external supports. Together, these contributions significantly enhance our understanding of how stress manifests in vulnerable populations, providing both theoretical insights and practical implications.
Background
Pathways Linking Stressors to Mental and Physical Health
While epidemiologists, psychologists, and biologists have traditionally approached stress using different methods and definitions, the past few decades have seen increasing integration across these disciplines. Cohen and colleagues (2016) synthesized these perspectives into the “Stage Model of Disease,” which conceptualizes stress as a broad set of constructs capable of triggering psychological, behavioral, and biological responses that elevate the risk for disease. This model posits a straightforward pathway from stressful life events to negative emotional responses, which activate regulatory and neuroendocrine systems with “downstream implications for disease onset and severity” (Cohen et al. 2016:459). While the model is deliberately simple, it has provided a foundation for understanding how stress impacts health outcomes across multiple systems.
Goldring and Bolger’s (2021)“Mediational Daily Stress Framework” expands upon the Stage Model by emphasizing the dynamic, short-term pathways through which daily stressors influence physical symptoms both directly and through psychological distress. This focus is particularly relevant for understanding the lived experiences of MNP, who face dynamic, significant stressors that shape their mental and physical health. Figure 1 adapts their framework, highlighting the specific pathways most pertinent to this study: (a) stressor-induced psychological distress (psychological reactivity), (b) the influence of psychological distress on physical symptoms (distress somatization), and (c) the direct impact of stressors on physical symptoms (stressor somatization). 2
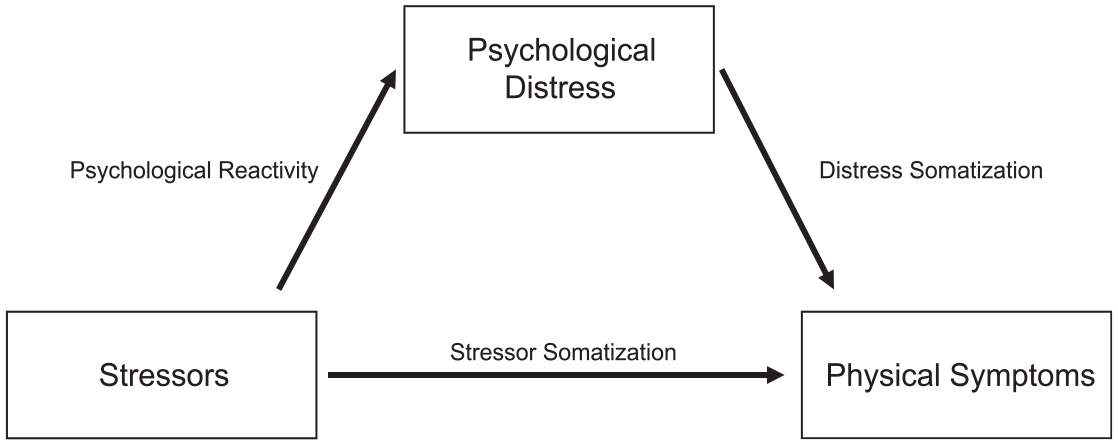
Conceptual framework: Stressors, psychological distress, and somatic pathways.
For instance, psychological reactivity might occur when experiences like job loss or discrimination trigger intense feelings of anxiety or sadness. Distress somatization can follow, as sustained emotional strain manifests physically through symptoms like headaches or digestive issues. In some cases, stressor somatization may arise more directly—such as when hunger or housing instability produces fatigue or sleep difficulties independent of conscious psychological distress.
These pathways are central to examining how post-migration stressors manifest in the mental and physical health of MNP. While Goldring and Bolger’s (2021) original framework acknowledges reciprocal effects, such as physical symptoms exacerbating psychological distress or creating additional stressors, this study focuses solely on the primary pathways due to its scope and methodological design.
Post-Migration Stressors and Health among MNP
Somatic symptoms are especially prevalent among MNP and have been observed across various settings and populations (Benabdeljlil 2022). Given that MNP are ten times more likely to have PTSD than their age-matched counterparts (Blackmore et al. 2020), research on somatization in this population has overwhelmingly centered on trauma and its somatic implications (Rohlof et al. 2014). However, emerging evidence suggests that the range of experiences influencing somatic symptoms extends beyond initial trauma, encompassing a broader set of stressors encountered in the post-migration context (Hynie 2018).
A follow-up survey of settled refugees in Norway revealed increases in post-traumatic stress indicators (PTSS-16), psychological distress, and physical health outcomes three years after resettlement (Lie 2002). Researchers found that post-flight stressful events explained some of the variance in the increase in post-traumatic indicators, leading to the hypothesis that challenges in the receiving context “may reduce the ability to cope” with previous trauma, exacerbating psychological distress and its physical manifestations (Lie 2002:423). Similarly, a mixed-methods study on MNP in the Netherlands identified housing problems and negative developments in the origin context as the most commonly cited post-migration stressors (Hondius et al. 2000). While these stressors were less strongly linked to physical symptoms than traumatic events, they showed significant associations with psychological complaints. The authors concluded that future research should broaden its focus to include a “rather broad spectrum of stressful experiences as variables” (Hondius et al. 2000:632).
Post-migration stressors are increasingly prioritized in broader research on MNP mental health (Li, Liddell, and Nickerson 2016; Weitzman, Blanton, and Camacho 2023). Structural factors include economic precarity, employment, housing stability, discrimination, family separation, or distressing developments in origin countries (Carter and Osborne 2009; Schweitzer et al. 2011). For MNP, economic precarity is a major source of distress that can compound and cascade into further stressors. For instance, without sufficient income, MNP can be forced to delay necessary health care, language learning, and family reunification (Goodkind et al. 2021). In a study of recently resettled refugees in the United States, economic difficulties, including insufficient income and housing issues, were found to mediate the effects of pre-migration trauma exposure on emotional distress and PTSD (Goodkind et al. 2021).
Despite growing recognition of post-migration stressors, comprehensive analyses that explore their dynamic relationships with mental and physical health outcomes remain sparse. Existing scholarship largely examines the cross-sectional association between stressors and psychological outcomes, such as anxiety and depression, as well as somatic symptoms, including headache, fatigue, gastrointestinal complaints, trouble sleeping, and chest pain (Chaturvedi and Desai 2013). For instance, studies of Ethiopian migrants in Toronto (Fenta et al. 2010) and refugees in Australia (Schweitzer et al. 2011) have linked post-migration difficulties to increased anxiety, depression, and somatic symptoms, yet these studies fail to capture how these relationships evolve over time. Questions thus remain: Are these associations static or do they change over time? What is missed in cross-sectional snapshots? Under what circumstances is recovery and improvement possible? While researchers are increasingly using diary methods to explore the contemporaneous associations among stressors, psychological distress, and physical symptoms in broader populations (Xie et al. 2024), related research on MNP is scarce.
In this study, I address the existing gaps in our understanding of post-migration stressors and their impact on mental and physical outcomes among MNP with weekly panel data and in-depth interviews. These data allow me to disentangle the relationship among stressors, psychological distress, and physical symptoms while inherently controlling for all time-invariant personal characteristics and pre-migration experiences. Qualitative insights complement the analysis, providing a deeper understanding of how the lived experiences of poverty, discrimination, family separation, and other structural stressors shape mental and physical health outcomes among MNP. In the discussion, I examine how these findings inform the social determinants of health among MNP, including legal violence, and their implications for service providers, policymakers, and sociological research on MNP wellbeing in the post-migration context.
Data and Methods
Study Design
This study employed an interactive convergent mixed-methods design, in which qualitative and quantitative data were collected in multiple phases and used to iteratively inform each stage of research (Fetters, Curry, and Creswell 2013). Initial interviews with MNP informed the construction of a 13-week longitudinal survey, including the inclusion of mental health and stressor measures. Following the survey, a second wave of interviews with survey participants was conducted. 3 This study draws upon 65 in-depth interviews and a longitudinal survey with 247 MNP participants. 4 For all data collection, we collaborated with and recruited through Fundación Mujer, a prominent NGO in Costa Rica with over 25 years of experience serving MNP.
Study Context
Costa Rica is a small Central American nation with approximately 5 million residents. Its central location between violent areas of northern Central America and politically turbulent areas of South America has made it a traditional nexus for those seeking refuge (Organisation for Economic Co-operation and Development and Fundación de la Universidad de Costa Rica para la Investigación 2017). However, the explosive growth of MNP worldwide accelerated this trend. Over the past eight years, Costa Rica’s MNP population has grown more than twenty-three-fold (UNHCR 2025b). In 2022, Costa Rica was the 3rd largest recipient of new asylum cases worldwide (UNHCR 2022), and MNP now comprise approximately 5% of the nation’s population (UNHCR 2023).
Historically, Costa Rica’s hospitable immigration policies have been a significant draw (Weitzman et al. 2022). The country boasts generous rights for asylum seekers and provisions for migrant children to receive free medical care and education (UNHCR 2025a). However, the recent surge in MNP arrivals has strained the country’s refugee infrastructure, contributing to processing delays and growing public resentment (Basok and Candiz 2025). Between 2018 and 2021, more than 100,000 people applied for refugee status, yet only a small fraction of claims were approved, leaving a massive backlog (UNHCR 2023). In response, recent policy changes have introduced stricter administrative procedures that further restrict long-term settlement. Amid these gaps, nonprofit organizations such as Fundación Mujer have played a vital role in supporting MNP, offering services like job training, language classes, and educational opportunities to facilitate resettlement and socioeconomic integration.
Qualitative Sampling and Data Collection
Between January and March 2020, the study’s principal investigator (PI) and a research assistant conducted semi-structured, in-depth interviews with 34 MNP women from Nicaragua, Venezuela, Cuba, and El Salvador. Between August and December 2022, the PI and three research assistants interviewed an additional 31 MNP women and men from the same nations. Most interviews were conducted in person, but four were conducted using WhatsApp video calls. All interviews were conducted in Spanish and lasted from 1.5 to 2.5 hours. The interviews were audio-recorded with consent and transcribed, with identifying details removed. To maintain confidentiality, all interviewees were assigned pseudonyms for record-keeping and analysis. Using a life history approach, we concentrated on the evolution of family relationships and wellbeing from early life through international displacement.
Quantitative Sampling and Data Collection
ERESS, or the Encuesta de Refugiados: Experiencias Sociales y Salud (ERESS) (Survey of Refugees: Social Experiences and Health) is a 13-week longitudinal survey of adult MNP in Costa Rica. The survey produced 3,126 observations collected from 260 participants. However, given this study’s emphasis on changes over time, I focus on participants who completed at least one follow-up (N = 3,093 observations; 247 participants). Among this group, retention was high: 88% completed the final week of the study (Week 13) and 70% completed all 12 follow-up surveys (see Supplemental Table 1 for weekly sample sizes). 5 Attrition was not systematically associated with demographic characteristics or any of the predictor variables used in the analysis.
We defined MNP based on any of the following criteria: having applied for asylum; citing danger, insecurity, or political turmoil in their country as a key motivation for migration; or having migrated from a country undergoing a significant humanitarian crisis in the year they migrated. At least one of these criteria was met by 97% of participants. We recruited participants from October 2021 to April 2022 on a rolling basis by sharing information about the study in online Fundación Mujer workshops and subsequent snowballing. Eligible participants were adult (≥ 18 years old) migrants who had lived in Costa Rica for at least six months. This criterion was used to help distinguish migrants who were more likely to settle in Costa Rica from those in short-term transit (Selee et al. 2021), a distinction important for the study’s broader focus on post-migration incorporation.
ERESS included a baseline survey and a series of weekly follow-ups. Lasting an average of 35 minutes, baseline surveys were administered by phone by members of the research team. After completion, participants received a $5 phone credit. In the survey, we collected information on demographics, household structure, adverse childhood events, pre-migration violence exposure, migration history and status; socioeconomic incorporation, mental and physical health; and local and transnational family dynamics. After the baseline survey, participants were invited to complete a series of 12 weekly follow-up surveys. We chose an intensive, weekly design to capture short-term fluctuations in experiences and wellbeing during the incorporation process in Costa Rica, rather than focusing on long-term change over multiple years.
Every Friday, we provided enrolled participants with a four-digit pin to access the online follow-up surveys via a Qualtrics link distributed through WhatsApp. The follow-up surveys repeated the main measures of the baseline. The online surveys took approximately 10 minutes to complete, and participants were sent a $5 phone credit after every completed survey. See Table 1 for descriptive statistics of both the interview sample and ERESS participants. The two samples are similar, though the interview sample includes a higher proportion of women, fewer Venezuelans (and more Salvadorans), and participants with lower education levels compared to the ERESS sample. To provide additional context, Supplemental Table 2 compares the ERESS sample to UNHCR surveys and an RDS survey conducted in 2022. These comparisons suggest that, while there is no reliable sampling frame to ensure representativeness, the ERESS sample aligns with other MNP samples in Costa Rica in terms of demographic and migration characteristics.
Baseline Descriptive Statistics of ERESS and Interview Samples.
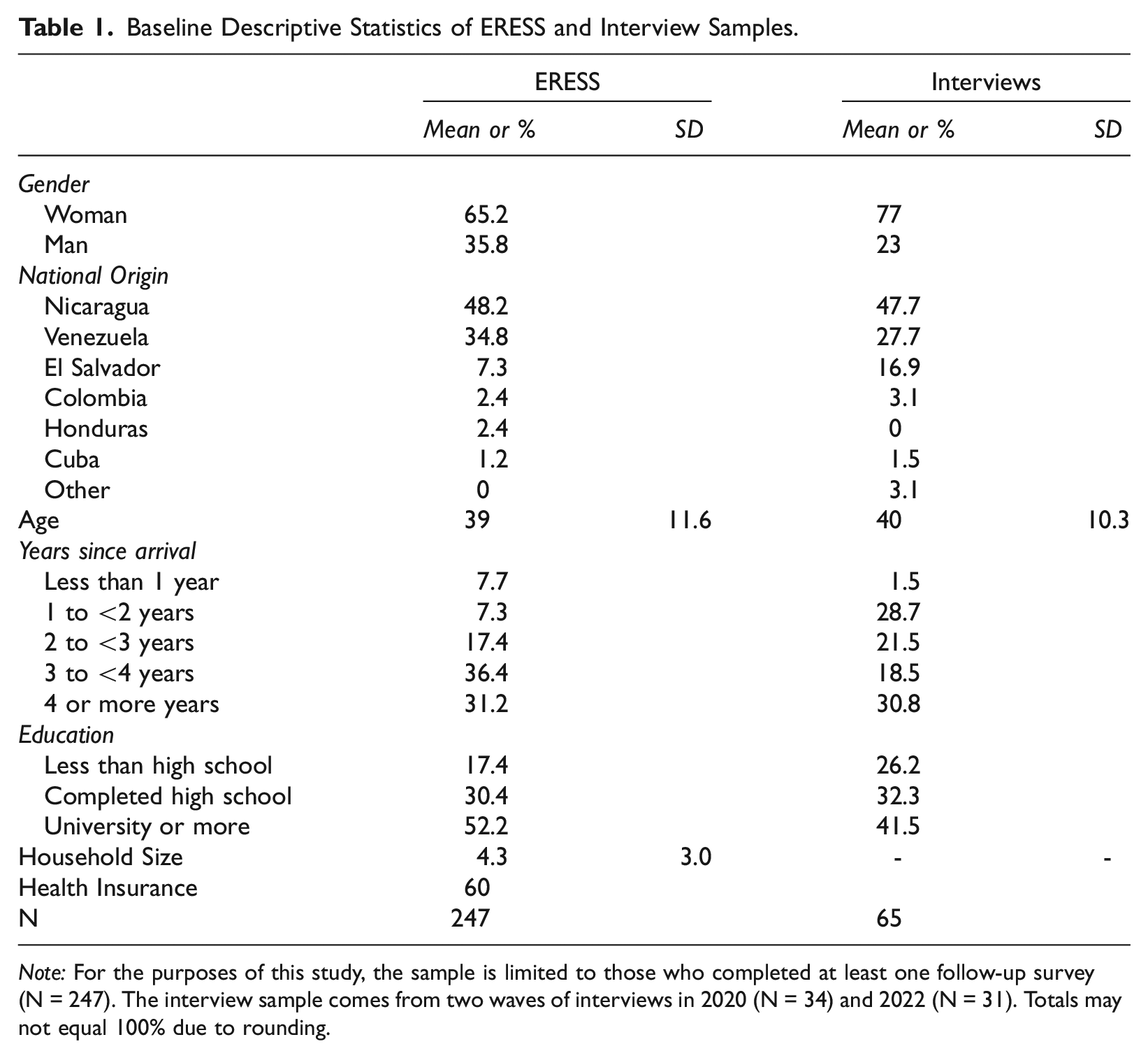
Note: For the purposes of this study, the sample is limited to those who completed at least one follow-up survey (N = 247). The interview sample comes from two waves of interviews in 2020 (N = 34) and 2022 (N = 31). Totals may not equal 100% due to rounding.
Measures
Supplemental Table 3 details the specific question wording and response options for all survey measures analyzed in this study.
Mental health
In ERESS, mental health was assessed using six questions from previously validated scales. 6 These questions were administered at baseline and during each follow-up survey and asked participants to reflect on their experiences over the past week. All six items are ordinal and share the same response scale, ranging from 0 to 4. Life satisfaction was rated from “Very unsatisfied” (0) to “Very satisfied” (4), and levels of nervousness from “Never” (0) to “Always” (4). The other four measures—stress, sadness, difficulty concentrating, and loneliness—used a Likert scale from “Totally disagree” (0) to “Totally agree” (4). To ensure consistency across all items, life satisfaction scores were reversed so that higher scores indicated greater distress (life dissatisfaction), and all six items were standardized before being averaged to create a composite psychological distress scale (Cronbach’s alpha = .84). 7 While descriptive statistics reflect the raw 0–4 scale, the standardized version of the scale is used in all regression analyses.
Physical symptoms
At baseline and in each follow-up survey, participants were asked about their recent physical health symptoms (“Which of the following symptoms have you experienced in the last week? Mark all that apply”). This list included common somatic symptoms: digestive problems, lack of appetite, sleep disturbances, and headaches. From this list, a collection of dichotomous variables was created, each corresponding to a specific symptom during each participant week. A value of 1 denotes the presence of this symptom, whereas 0 signifies its absence during each week in which the participant completed the survey. I also generated a weekly symptom count, which represents the total number of symptoms (0–4) experienced by a participant in a given week, including at baseline.
Stressors
ERESS participants were asked about post-migration stressors at baseline and in follow-up surveys. Given variations in how certain questions were posed between the baseline and follow-up phases, as well as the introduction of new questions post-baseline, all stressor variables are derived exclusively from follow-up responses. In each follow-up survey, participants were asked about perceived discrimination and survival actions (“Had to do something you were not proud of to survive or earn money”).
They were then asked, “Did anything else happen this week that caused you stress?,” with a list of possible answers that included homelessness, hunger, and the loss of a job. This list was populated with options derived from our previous interviews. Notably, the answer used for the homelessness measure was falta de vivienda (literally “lack of housing”), which in this context likely captures a broader range of instability, including overcrowding, evictions, and informal or precarious living arrangements (Spicker 2009). I also aggregated one category from individual responses that encompassed stresses originating from their countries of origin (e.g., bad news about a loved one, situation worsened). Dichotomous variables for each of these were created, where a value of 1 denotes the presence of the stressor, whereas 0 signifies its absence during each participant week after baseline. I then generated an additive “stressors scale,” which summed the total number of stressors experienced that week (0–6). Again, a standardized version of this scale is used in all regression models.
Controls
All models account for time-varying factors that could influence mental and physical health, with all variables standardized for comparability. These include whether participants believed they had COVID-19 during a given week, health insurance status for the week in question, and household size.
Analytical Approach
In this study, I adopt a mixed-methods analytical approach. For each thematic focus, I present quantitative data followed by a qualitative analysis. First, I present the descriptive statistics of the sample, highlighting prevalence and variability in stressor exposure, and mental and physical health throughout the study. Given the panel nature of the data, I use fixed effects models to examine within-individual variations over time.
I then examine the relationships among stressors, psychological distress, and physical symptoms, organizing the analysis into three key pathways: psychological reactivity, distress somatization, and stressor somatization. First, I assess psychological reactivity using fixed effects OLS models to predict psychological distress with the stressors scale and each individual stressor. Since stressors were first measured in the initial follow-up survey, baseline psychological distress was excluded from these models to minimize concerns about reverse causality. Next, I analyze distress somatization, estimating fixed effects Poisson models to predict weekly symptom count with psychological distress, and fixed effects linear probability models to predict each symptom individually. 8 To explore stressor somatization, I extend the Poisson models to include both psychological distress and stressors as predictors, allowing for an examination of the direct relationship between stressors and physical symptoms, net of psychological distress. Finally, I investigate the temporal dynamics of these pathways by estimating lagged models, predicting physical symptoms with both psychological distress and stressors from one and two weeks prior.
To deepen and contextualize the statistical findings, I analyze in-depth interviews with 65 MNP. The research team, including the study PI and two research assistants, iteratively coded and analyzed the transcripts in Spanish. Using a method inspired by Charmaz (2006), we developed thematic codes to extract analytical and theoretical insights from the data. We coded the transcripts based on the primary themes we identified, holding regular meetings to ensure consistency and accuracy. While the initial analysis drew from a constructivist grounded theory approach, it also incorporated abductive reasoning (Tavory and Timmermans 2014), as emergent themes were interpreted in conversation with the quantitative findings and relevant theories. Although all analysis was conducted in Spanish, selected illustrative quotes have been translated into English for this article.
Results
Quantitative Sample Description and Variability
Respondents consistently reported stressors, psychological distress, and somatic symptoms throughout the study (Table 2). On average, they experienced stressors in 90% of observation weeks, with a mean of 1 stressor per week. Discrimination and stress from origin country were the most prevalent, reported in 41 and 21% of weeks, respectively. Homelessness was the least common, reported in only 6% of weeks.
Mean and Variation of Reported Stressors, and Physical and Mental Health Indicators.
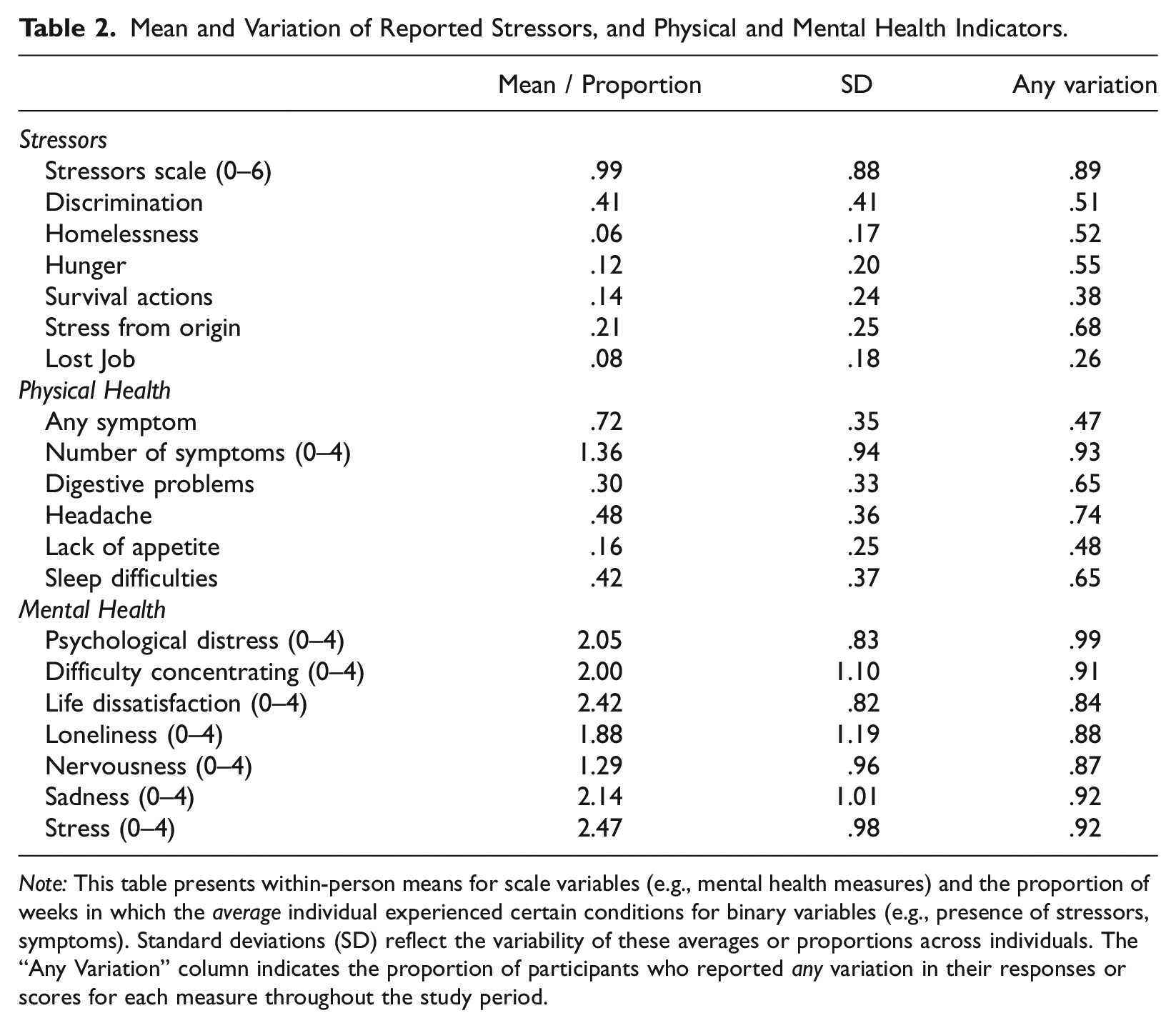
Note: This table presents within-person means for scale variables (e.g., mental health measures) and the proportion of weeks in which the average individual experienced certain conditions for binary variables (e.g., presence of stressors, symptoms). Standard deviations (SD) reflect the variability of these averages or proportions across individuals. The “Any Variation” column indicates the proportion of participants who reported any variation in their responses or scores for each measure throughout the study period.
The respondents generally indicated moderate levels of mental health. While the mean score for the composite variable of psychological distress was 2.1, individual measures varied considerably. On average, participants reported physical symptoms in 72% of observation weeks, with a mean of 1.4 symptoms per week. Headaches and sleep difficulties were the most common, reported in 48 and 42% of weeks, respectively. Lack of appetite was the least common, noted in only 16% of weeks.
Participants demonstrated considerable variation in stressor exposure and in mental and physical health throughout the study period. While not central to the main research questions, these patterns of variation are essential for the modeling approach, enabling the analysis of short-term associations between changes in stressors, psychological distress, and physical symptoms. Over 90% of participants reported variations in feelings of sadness, stress, and difficulty concentrating. Over 80% of participants reported variations in all other mental health indicators. Most participants varied in their reported headaches (74%), sleep difficulties (65%), and digestive problems (65%).
Supplemental Figure 1 details the frequency of these fluctuations, showing the mean percentage of weeks in which respondents reported changes from their prior observation for all stressors, mental health measures, and physical symptoms. Reported variation was common across all domains, though it differed by measure. Mental health indicators showed the greatest variability, with the average participant varying in 40% of the follow-ups for sadness, stress, nervousness, and difficulty concentrating.
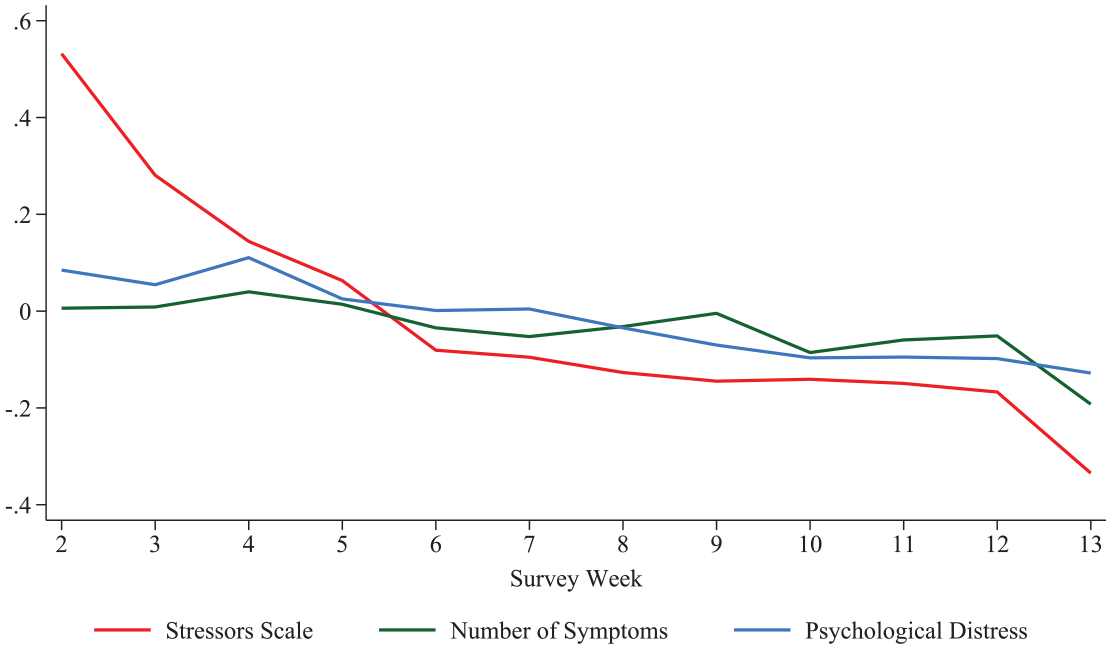
To complement this, Figure 2 presents a time-series plot that illustrates changes in the standardized means of stressors, symptoms, and psychological distress across survey weeks, where values reflect deviations from each respondent’s own average level. All three indicators decline over the study period, though psychological distress and symptoms remain relatively stable after the midpoint. Stressors decrease steadily from about 0.5 standard deviations above participants’ average to 0.3 below, indicating a notable reduction in reported stress exposure over the study period.
Standardized trends in stressors, psychological distress, and physical symptoms by survey week.
Psychological Reactivity: Stressors and Psychological Distress
Both quantitative and qualitative data illustrate the phenomenon of psychological reactivity, where post-migration stressors are closely associated with heightened psychological distress among MNP. In the panel data, a statistically significant weekly-level association exists between stressors and psychological distress. Model 1 (Table 3) is a fixed effects OLS model predicting psychological distress using the standardized stressors scale. For the average participant, a one-standard-deviation increase in stressors relative to their typical level throughout the study period is associated with a .15 standard deviation increase in psychological distress (p < 0.001).
Fixed-Effects Regression Models Exploring the Relationships among Stressors, Psychological Distress, and Physical Symptoms.
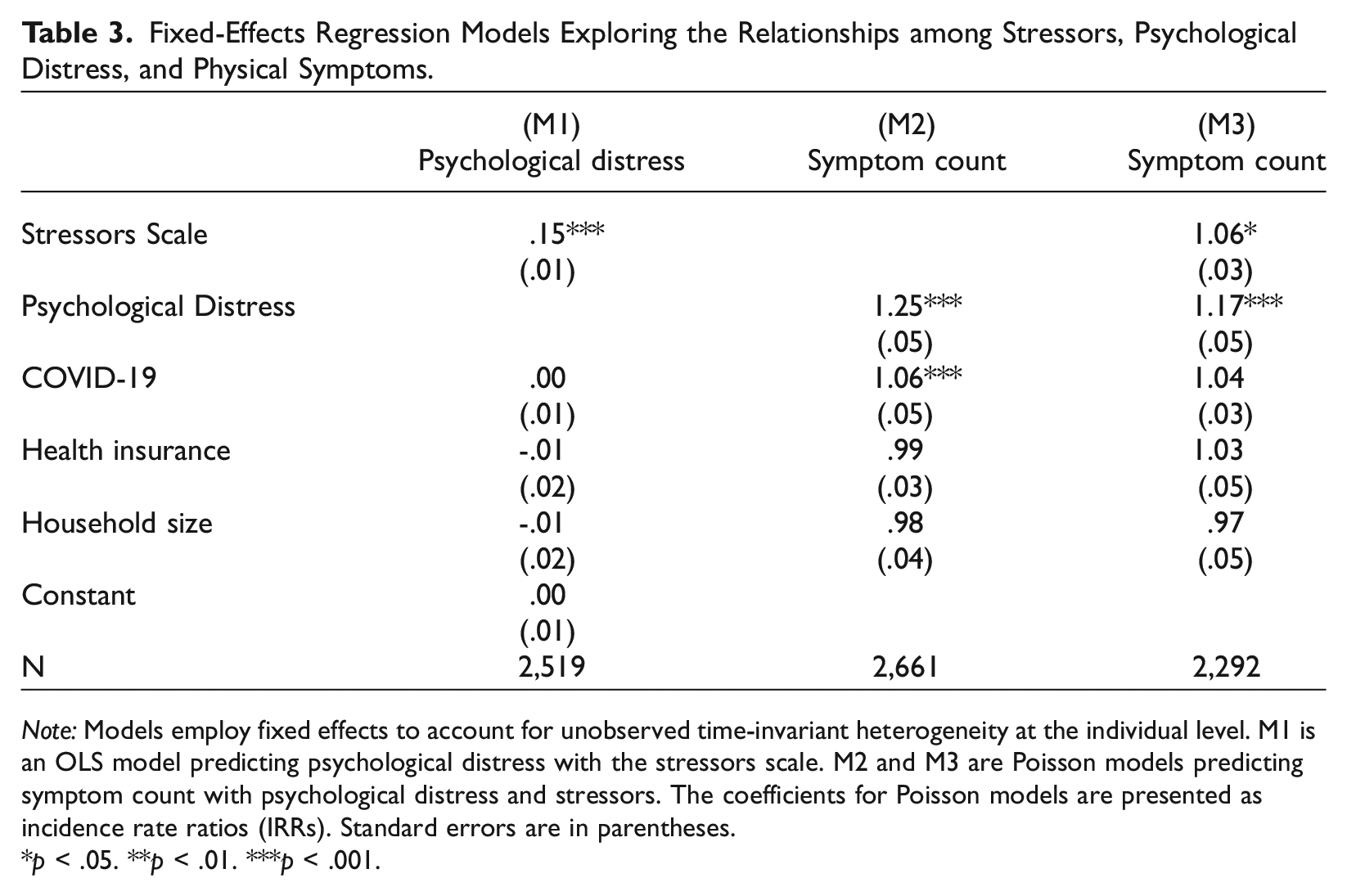
Note: Models employ fixed effects to account for unobserved time-invariant heterogeneity at the individual level. M1 is an OLS model predicting psychological distress with the stressors scale. M2 and M3 are Poisson models predicting symptom count with psychological distress and stressors. The coefficients for Poisson models are presented as incidence rate ratios (IRRs). Standard errors are in parentheses.
p < .05. **p < .01. ***p < .001.
To further understand the relationships between individual stressors and psychological distress, I disaggregated the general stressor scale into its individual components. Figure 3 displays a coefficient plot from fixed-effects OLS regression models that separately examine the relationship between each specific stressor and the standardized psychological distress scale. The coefficients reflect the expected change in psychological distress (measured in standard deviations) for the average individual when each stressor is present compared to when it is not, all else being constant. Each stressor demonstrates a statistically significant positive association with psychological distress, with hunger, loss of a job, discrimination, and homelessness showing the largest effect sizes. While referred to as homelessness in the models, this measure captures falta de vivienda—a broader construct reflecting housing instability, which aligns with the challenges participants described in the interviews.
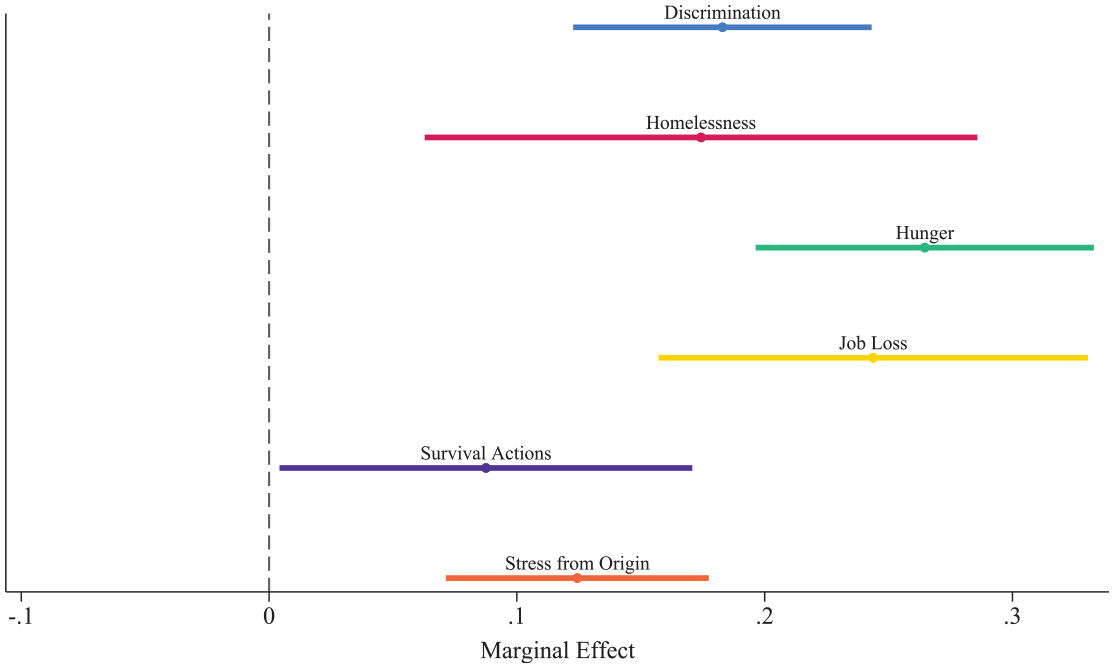
Coefficient plot from fixed effects OLS models: Association of individual stressors with psychological distress.
Quantitative findings are echoed in the interviews, where individuals vividly outlined how stressors exacerbated psychological distress, revealing an interconnected relationship between the challenges they faced and their mental wellbeing week to week. Interviewees described a range of structural stressors affecting their lives in Costa Rica, including unemployment, economic hardship, difficulty finding housing, discrimination, family separation, and distressing developments in their countries of origin. These experiences were not isolated; rather, they interwove in complex ways, compounding their impacts. For instance, unemployment heightened economic precarity and exacerbated housing insecurities. Similarly, these problems were often due to underlying discrimination in the workplace or by landlords. The interviews thus extend the statistical models by revealing how multiple stressors are experienced simultaneously and in mutually reinforcing ways.
Toward the end of each interview, participants were prompted: “Since you arrived in Costa Rica, what has been the most difficult or stressful moment?” Consistent with the statistical models, the frequency of responses, summarized in Table 4, underscores the prevalence of unemployment, economic hardship, and housing as the foremost stressors. These were also the most common stressors mentioned throughout the interviews and implicated in accounts of stress-induced physical symptoms.
Frequency of Stressors Identified as Most Difficult in Qualitative Interviews.
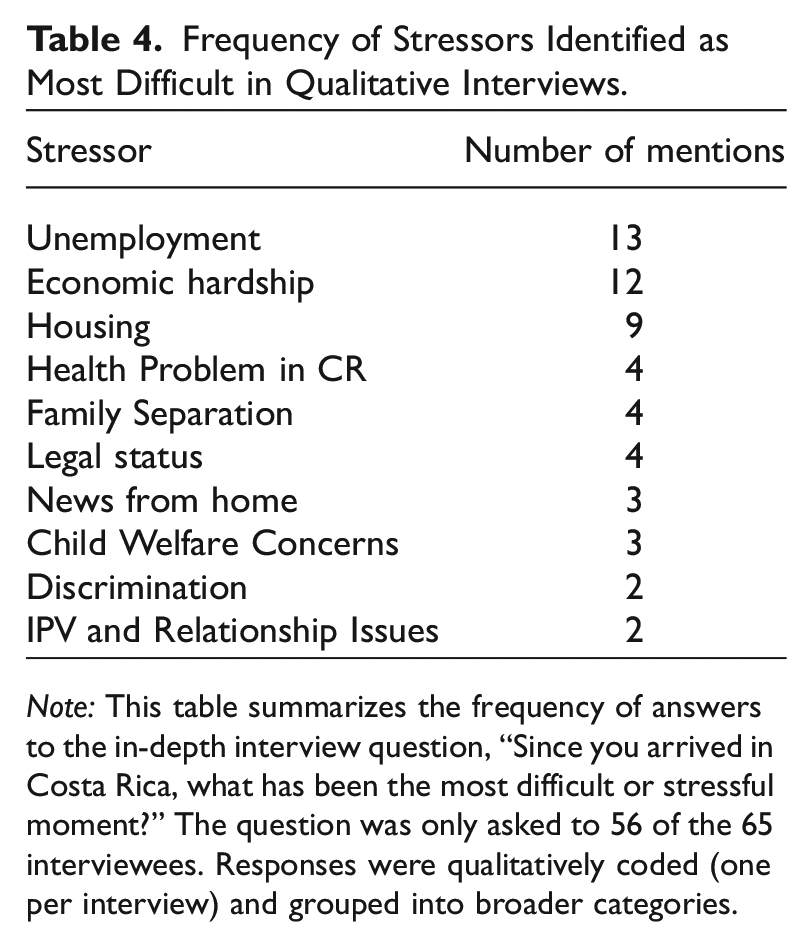
Note: This table summarizes the frequency of answers to the in-depth interview question, “Since you arrived in Costa Rica, what has been the most difficult or stressful moment?” The question was only asked to 56 of the 65 interviewees. Responses were qualitatively coded (one per interview) and grouped into broader categories.
In addition to a general shortage of formal jobs in Costa Rica, interviewees described the unique challenges they faced as migrants and “solicitantes,” a formal legal category for those who have applied for asylum and are awaiting an interview. For one, foreigners are often turned away from potential employers and maligned for trying to take the jobs of native Costa Ricans. Some described how even with legal work permits, they were rejected and accused of falsifying documents. Facing expensive and complicated bureaucratic hurdles to legalizing their university transcripts and licenses, lawyers and engineers sought employment in corner stores and auto shops, only to be told they were overqualified. As such, many interviewees resorted to unscrupulous informal jobs in which they were regularly overworked, underpaid, and exploited. These experiences help contextualize why discrimination emerged as one of the strongest predictors of psychological distress in the statistical models.
The widespread lack of employment and livable wages among interviewees led to chronic stress about meeting basic needs. Dalia’s summary of her biggest sources of stress in Costa Rica was true for most: “It’s two things. Food and a room.” Housing instability was widespread in this group, with interviewees sharing stories of sleeping in parks or shelters, squatting, overstaying their welcome with distant family or friends, or overcrowding in small apartments. Housing costs were the main barrier to entry, but as vulnerable migrants, they also faced discriminatory practices like refusal to return deposits, being turned away from applying, and overcharging for rent. Interviewees also regularly described hunger and the inability to afford three meals a day for their families. Jimena shared: The most stressful moments are when my daughters are crying and asking for milk, they wanted milk, and I couldn’t give them milk because I didn’t have the money to buy it for them. And I cried hard, and I prayed, “but God, why?”
Similarly, Ingrid confided that “what depresses me the most is the times I don’t have food to give my kids…it is my biggest anguish.” Maria, a political asylee from Nicaragua, eloquently summarized the Maslowian association articulated by so many interviewees: “Really the economic part helps to stabilize you emotionally because when you, for instance, don’t have a job to provide basic needs you get very unstable, anxious, and everything.”
Somatic Pathways: Distress and Stressor Somatization
Emotional turbulence, deeply rooted in economic and social stressors, often leads to distress somatization, where psychological stress manifests into physical symptoms. In weeks where participants experienced increases in psychological distress, there was a corresponding increase in the likelihood of worsened physical health. Model 2 (Table 3) is a fixed effects Poisson model predicting weekly symptom count with psychological distress. The coefficient for psychological distress is an incidence rate ratio (IRR) of 1.25 (p < 0.001), indicating that for the average participant, experiencing a standard deviation increase in psychological distress above their own average level of distress across the study period is associated with a 25% increase in the expected count of symptoms in a week. This magnitude is larger even than the effect of experiencing COVID-19 (IRR = 1.06, p < 0.001), compared to weeks when COVID-19 is not experienced.
Figure 4 further explores the relationship between psychological distress and physical symptoms, illustrating how specific physical symptoms correspond with changes in mental health. This figure plots the coefficients from a series of fixed effects linear probability models predicting each symptom with psychological distress. A significant association exists between psychological distress and all reported symptoms. Sleep difficulties and lack of appetite exhibit the strongest associations with psychological distress, with sleep difficulties showing a coefficient twice as large as any other measure. The personal experiences of MNP provide essential context for these statistical models, demonstrating how emotional distress frequently translates into a range of physical symptoms.
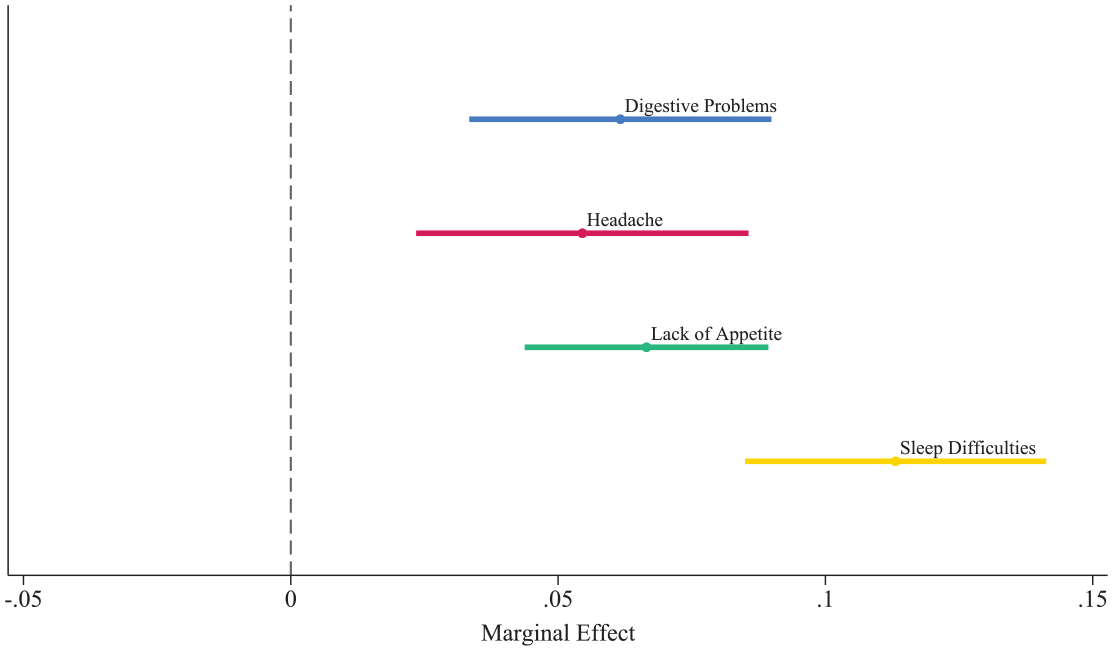
Coefficient plot from fixed effects linear probability models: Association of psychological distress with individual symptoms.
Although not directly prompted, interviewees regularly discussed their physical health. While some recounted ailments unrelated to psychological factors, the most common narrative thread explicitly highlighted how psychological distress precipitated physical symptoms. A majority (36 individuals or 55%) of interviewees described experiencing somatic symptoms, or physical symptoms brought on by stressors or mental states (Table 5). Sleep disturbances and lack of appetite topped the list, with 13 and 12 mentions, respectively. These particular symptoms corroborate the dominant pattern observed in the quantitative analysis.
Frequency of Reported Somatic Symptoms in Qualitative Interviews.
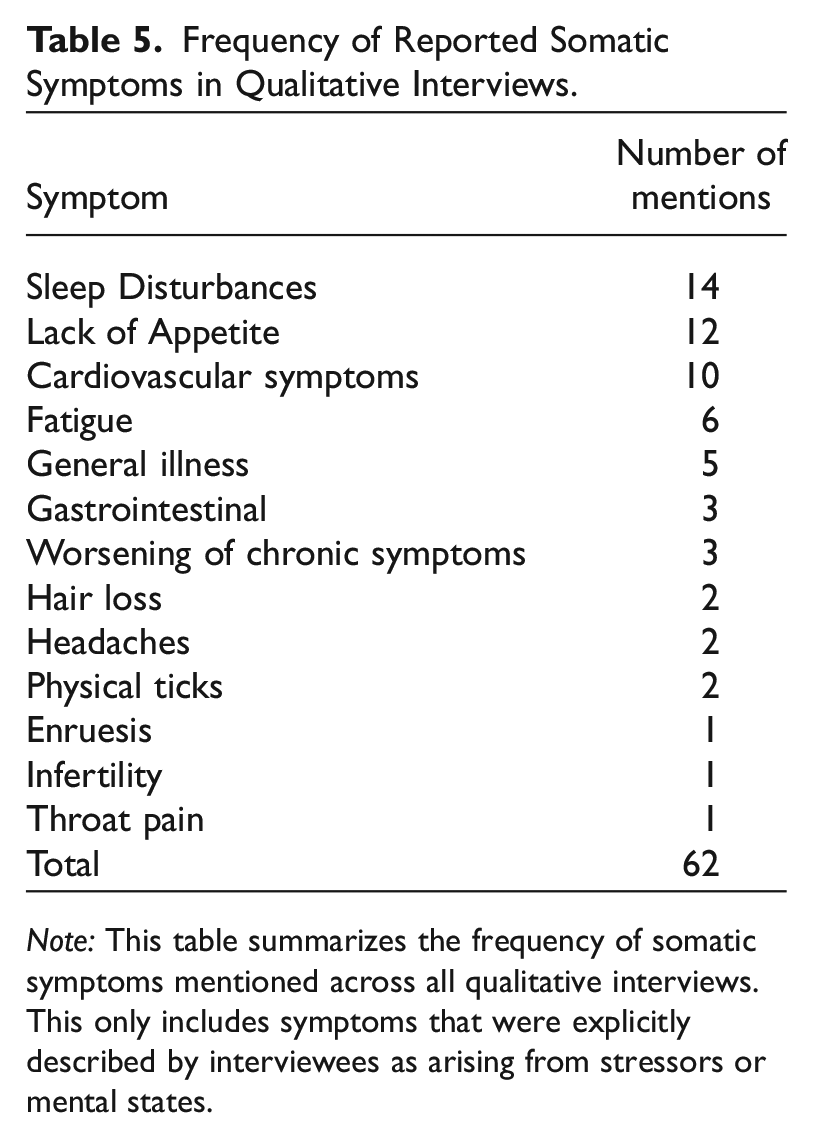
Note: This table summarizes the frequency of somatic symptoms mentioned across all qualitative interviews. This only includes symptoms that were explicitly described by interviewees as arising from stressors or mental states.
Housing challenges, economic hardship, and unemployment were repeatedly implicated in narratives of somatic symptoms. Jaime’s situation demonstrates how these stressors interact, along with other factors like discrimination and institutional obstacles, to produce especially challenging situations. After an attempt on his and his son’s life by pro-regime agitators in Nicaragua, Jaime and his family fled across the border to Costa Rica. His wife was a professional with a master’s degree but, unable to afford to legalize her paperwork, she took a job in a restaurant kitchen. She was treated poorly and often made to work 14-hour shifts with no overtime pay. Their first apartment was in a commercial district where the utilities were unusually high. After a few months, and without Jaime being able to find work, they fell behind in payments. When they found another apartment that was surprisingly affordable, Jaime’s son borrowed against his future wages at his job for the deposit. Days later, the landlord rejected their application and refused to return the deposit. After spending several desperate days awaiting homelessness, Jaime’s 18-year-old son had a hypertensive emergency, with his systolic blood pressure spiking suddenly to 200. While the doctors were unsure about the diagnosis, Jaime was confident that he knew the reason: “I know it was all the tears upon tears. Every night wondering what we would do, we didn’t know anything.”
Even when individuals have housing and employment, Costa Rica’s high cost of living exacerbates daily stress about meeting even the most basic of needs. Lucas, who escaped gang violence from El Salvador with his family of four, explained the psychological and physical impact of this deficit: Imagine you are paying $320
9
for an apartment, and you are together making $450 a month. With $130 you can’t get through the month, because my kids were studying, I had to pay for their transport, their food, there had to be food in the house, we had to pay for electricity and water. So, we saw that and thought, ‘we will never get out of this’… so I fell into a depression, I didn’t want to leave, didn’t want to eat, didn’t want to do anything… the headaches were a kind of desperation, a tachycardia would come on occasionally. But I said to myself, “No, I have to keep going. I have to keep going.”
Another major source of daily distress for MNP in Costa Rica is ongoing anxiety about situations in their home countries and grief about family separation, both of which featured prominently in accounts of the physical manifestations of stressors. One poignant example is Vanessa, who fled to Costa Rica to escape gang violence and extortion in El Salvador. She experienced frequent death threats from gang members and endured the sudden death of her partner in a related incident. When asked if she stays in touch with anyone from her former neighborhood, Vanessa explained that she avoids contact, sharing: Six months ago, I spoke with my best friend there and she only told me sad things, it made me depressed. So, I would rather not know things because if it gets into that, I get sick. I start to remember his death, how everything happened, how my arrival was, and that makes me sick.
In her life in Costa Rica, this “sickness” manifested in various ways, such as fatigue, lack of appetite, weight loss, and general malaise.
Eva confidently articulated the physical effects of mental anguish surrounding family separation. She was forced to flee political tension in Venezuela, leaving behind a prosperous cosmetic business and a comfortable upper-class life. Due to complications with her family’s passports, she had to unexpectedly travel to Costa Rica first. The trauma of family separation was exacerbated by regular sexual harassment in her new job. Eva’s distress manifested physically as she lost her appetite, quickly shedding 15 pounds and battling physical weakness. This challenging phase profoundly altered her understanding of healthcare, leading to a paradigm shift in the business she had restarted in Costa Rica: The venture involves the formulation, production, and marketing of cosmetic products and spa techniques. But really, it is something else. I mean, it was something that I had to learn here in Costa Rica because I used to do one thing and another thing separately. But here, I have been integrating them. So now, I address all skin problems through emotional aspects. If there is a collagen degeneration issue, I physiologically understand what is happening. But, what is attacking you emotionally? What in that area is affecting this?
Although family separation was not measured in the survey, the qualitative data confirm its centrality as a post-migration stressor—extending the analysis beyond what was examined in the quantitative models.
While distress somatization was the dominant pathway reflected in both the quantitative and qualitative data, the findings also demonstrate the significance of stressor somatization. This process, where stressors exert a direct influence on physical symptoms beyond their effects through psychological distress, was evident in both statistical models and a subset of participant narratives. M3 (Table 3) is a fixed-effects Poisson model that includes both psychological distress and stressors as predictors of weekly symptom count. In this model, stressors maintain a statistically significant association with physical symptoms, with an IRR of 1.06 (p < 0.05), indicating that stressors have a direct influence on physical symptoms that is independent of their relationship with psychological distress. The coefficient for psychological distress remains significant but decreases to an IRR of 1.17 (p < 0.001).
Stressor somatization is also reflected in interviewees, where some individuals directly attributed physical symptoms to acute stressors, without explicitly linking them to an emotional or mental state. For instance, Evelyn recounted how the day before, she had gone shopping and saw a young boy who looked just like her son left behind in Nicaragua: “When I saw him, I suddenly, quickly got a headache.” Similarly, Nayeli shared that when she hears loud noises, like a car backfiring, she remembers gunshots during a violent period in Nicaragua and immediately experiences stomach pain. 10
Temporal Dynamics and Alleviation of Somatic Symptoms
Somatic symptoms generally subside swiftly once stressors and psychological distress are alleviated. To examine the temporal dynamics of these associations, I conducted an analysis incorporating lagged effects. I estimated fixed effects Poisson models predicting weekly symptom count with stressors and psychological distress from one and two weeks prior. There was no significant relationship with psychological distress in prior weeks. However, stressors from the preceding week had a significant association with physical symptoms, with an incidence rate ratio (IRR) of 1.05 (p < 0.05). This association was no longer significant by the second week.
To further explore these temporal patterns, I estimated linear probability fixed-effects models for each individual symptom using the lagged predictors. Among the eight psychological distress models, the only statistically significant relationship was between sleep difficulties and psychological distress from the previous week (Supplemental Figure 2). In contrast, among the eight stressors models, there were significant associations for lack of appetite and stressors from the prior week, as well as for sleep difficulties and stressors from each of the past two weeks. The relationship with sleep difficulties and stressors diminished over time and was not statistically significant by the third week.
These findings confirm a generally immediate association among stressors, psychological distress, and physical health. However, the stressors scale demonstrated a more enduring association compared to psychological distress, particularly in the case of sleep difficulties. This persistence provides further evidence for stressor somatization, where stressors maintain a direct and distinct association with physical symptoms beyond their influence through psychological distress.
Interviewees corroborated these findings, describing a dynamic process where physical symptoms closely followed the presence of stressors and psychological distress. This relationship was short-term and reversible; improvements in their situation or mental state often led to a reduction or complete resolution of somatic complaints. At the time of the interviews, many individuals had not yet experienced this recovery. Those that had, however, highlighted stabilization in housing and economic conditions, alongside family reunification, as the situational changes that most improved their well-being. Additionally, nonprofit counseling services, religious faith and communities, and the perceived peace and safety in Costa Rica played crucial roles in mitigating somatic symptoms.
Among the individuals mentioned here, several had seen resolution of somatic symptoms. Ingrid, who mentioned the “anguish” of being unable to buy food for her children, confided that she had been suffering for two days from chest pain because of stress and anxiety. However, by the end of the interview, after having ample time to share and “desahogarse,” (relieve herself) the pain had dissipated. Jaime’s son, who had a hypertensive emergency, stabilized and is in good health after a friend in the United States sent emergency funds for them to move to a new apartment, and their religious congregation provided them with food assistance. Lucas, who struggled with depression, headaches, and tachycardia, happily shared that compared to where he was, they are now “in paradise,” because of economic stabilization and improvement in housing. Lastly, Eva returned to health when she was reunited with her family in Costa Rica.
Discussion and Conclusion
The health impacts of post-migration stressors are profound, yet they are often overshadowed by a focus on pre-migration trauma. This study provides new insights into how stressors in the receiving context shape the mental and physical health of MNP. Using a conceptual framework grounded in somatic processes and drawing on an intensive panel survey and in-depth interviews with MNP in Costa Rica, this study unearths new insights into the complex health challenges faced by vulnerable populations. These findings reveal three major takeaways.
First, post-migration stressors provoke physical symptoms among MNP, both directly and through psychological distress. Economic stress, discrimination, and ongoing family separation had a particularly acute impact on mental and physical health. These findings move beyond static cross-sectional associations to reveal that somatic symptoms respond sensitively to fluctuating stressor exposure, manifesting within a tight temporal framework.
Second, the relationships between stressors, psychological distress, and physical symptoms are largely immediate, with no significant persistence in physical symptoms in the weeks following changes in mental health. For MNP, who endure considerable trauma and stress, this suggests frequent ebbs and flows in physical health that are intricately tied to their life stressors and psychological state. However, this also implies that interventions may rapidly alleviate somatic symptoms, highlighting the potential for targeted support strategies.
Third, interviewees perceived and explicitly described the somatic process from stressors to psychological distress to physical symptoms. This challenges the practices and assumptions in healthcare settings that marginalized groups lack literacy or awareness concerning their own health (Hamed et al. 2022). As in the case of Eva, interviewee’s narratives suggest that the actual experience of compounded hardship plays a role in heightening their ability to recognize the dynamic connections between external stressors and mental and physical health. This awareness must be considered within the broader sociopolitical structures that exacerbate their marginalization. Limited access to resources, systemic discrimination, and inadequate services force MNP to internalize stress and independently manage their well-being.
The escalating number of MNP worldwide presents host governments with significant challenges. Post-migration stressors such as employment precarity, housing instability, and family separation—often driven by restrictive policies and bureaucratic obstacles—significantly contribute to psychological distress and physical health problems among MNP. These stress-induced health issues, including somatic symptoms, often lead individuals to seek care in primary healthcare settings, straining already limited resources in low- and middle-income countries like Costa Rica. Current policies frequently perpetuate structural stressors, embodying a form of legal violence that further harms MNP. In contexts where governments are indifferent to—or actively exacerbate—these harms, nongovernmental and humanitarian organizations often play a critical role in mitigating damage and advocating for MNP’s health and rights.
Developed through an analysis of Central American immigrants in the United States, the concept of “legal violence” refers to the “harmful effects of the law that can potentially obstruct and derail immigrants’ paths of incorporation” (Menjívar and Abrego 2012:1383). Legal violence is usually experienced in the spheres of family, work, and school and often includes negative effects on migrants’ livelihood. In Costa Rica, legal violence affecting employment and family separation—areas essential to overall wellbeing—will likely exacerbate psychological distress and somatic symptoms among the MNP population.
The most notable protective factor against somatic consequences, reflected in both the quantitative and qualitative data, was the ability of MNP to financially support their families. Interviewees emphasized that securing employment with livable wages was difficult for migrants for three reasons: active discrimination and ignorance of the law, expensive and complicated procedures for legalizing foreign academic and professional documentation, and workplace exploitation. In Costa Rica, lawmakers should prioritize the enforcement of existing workplace protection legislation and streamline the apostille process to reduce costs and facilitate the recognition of foreign qualifications. However, recent policy reforms to refugee law have moved in the opposite direction, restricting work permit eligibility and increasing wait times for those who qualify (Téllez 2023). These policies exemplify legal violence by increasing economic insecurity and stress among MNP, leading to worsening mental and physical health outcomes.
Interviewees also highlighted the crucial role of family reunification in alleviating stress and improving physical health outcomes. Facilitating reunification can offer substantial relief and support to MNP, contributing to their stabilization and integration within host societies. Until recently, Venezuelans could arrive legally in Costa Rica without a pre-arranged visa. However, in a sudden policy shift in February 2022, the Costa Rican government mandated that Venezuelans must apply for a visa before their arrival (Murillo 2022). Announced merely four days before its enactment, this change undoubtedly disrupted the plans of countless Venezuelan families aiming for reunification. Such abrupt obstacles to reunification certainly exacerbate the stressors and challenges faced by MNP, which can, in turn, lead to mental and physical health consequences.
Menjívar and Abrego note that legal violence produces immediate “social suffering” and long-term harm with repercussion for incorporation (2012: 1384). This study extends this concept by demonstrating how legal violence not only leads to social suffering but also can precipitate mental and physical suffering in the short term. While the policy examples presented here focus on Costa Rica, similar dynamics are present in other contexts, including the United States, where recent policy shifts have reduced protections for MNP. In such settings, even when governments retreat from protective policies, these findings offer important guidance for humanitarian organizations, health providers, and advocates. Addressing structural and legal violence remains essential for improving the holistic well-being of MNP and for informing more humane and health-conscious responses—whether led by governments or civil society.
Although this study offers valuable insights, it is not without limitations. Both the survey and interviews relied on self-reporting, which can inherently introduce biases due to factors like recall inaccuracies or the desire to present oneself in a certain way. Moreover, both datasets were non-representative samples and thus may lack external validity. That said, the study team purposively sampled MNP from a variety of countries to capture a wide spectrum of experiences.
Additionally, while the composite psychological distress scale used in this study was validated through factor analysis, it is based on six mental health items rather than full scales. This approach may underestimate the complexity of mental distress, representing a potential limitation in fully capturing participants’ experiences. Relatedly, while many interviewees described experiences consistent with trauma and post-traumatic stress, the study did not include a validated measure of PTSD. Future research could benefit from employing more comprehensive mental health instruments, including full diagnostic scales.
The broader study also excluded key subpopulations. Newly arrived migrants (within six months of arrival) were not included in the survey, limiting our ability to understand the immediate health effects of resettlement. We also did not include youth, and their mental and physical health trajectories may differ from those of adults.
Finally, the study’s design does not account for potential feedback loops or reciprocal causality between stressors, psychological distress, and physical symptoms. For example, somatic symptoms themselves may exacerbate psychological distress or create additional stressors, such as job loss due to poor health. While these feedback mechanisms were recognized in the conceptual framework, they were not directly tested in the models, representing a limitation of this analysis. Future research could address these complexities by employing methodologies such as structural equation modeling or cross-lagged panel designs to better capture these dynamic processes.
In conclusion, this study advances understanding of the health consequences of post-migration stressors among MNP by highlighting the dynamic connection between stressors, psychological distress, and physical symptoms. By advancing beyond a focus on pre-migration trauma, this research provides new insights into the immediate health impacts of post-migration challenges. These findings emphasize the importance of developing interventions that address the mental and physical health needs of MNP while advocating for broader policies that target root causes like secure employment, stable housing, and family reunification. Despite the study’s limitations, the results offer a compelling foundation for future research, urging further exploration of how post-migration social contexts impact health outcomes among MNP over time.
Supplemental Material
sj-docx-1-smh-10.1177_21568693251345117 – Supplemental material for Post-Migration Stressors and Mental and Physical Health among Refugees and Migrants in Need of Protection: A Mixed-Methods Analysis with Weekly Panel Data
Supplemental material, sj-docx-1-smh-10.1177_21568693251345117 for Post-Migration Stressors and Mental and Physical Health among Refugees and Migrants in Need of Protection: A Mixed-Methods Analysis with Weekly Panel Data by Matthew Blanton in Society and Mental Health
Footnotes
Acknowledgements
I am grateful to the study’s participants for generously sharing their experiences and to Fundación Mujer for their instrumental role in the recruitment process. I also thank Abigail Weitzman, Néstor Rodríguez, Diane Coffey, Amy Johnson, Jared Thorpe, and KJ Davidson-Turner for their instructive feedback on this study’s development and design.
Funding
The author(s) disclosed receipt of the following financial support for research, authorship, and/or publication of this article: This research was made possible with funding from grants from the National Institute for Child Health and Human Development (K01HD099313, PI Weitzman; T32HD007081, Blanton) and with population center grants from the National Institute for Child Health and Human Development to the Population Research Center at the University of Texas at Austin (P2CHD042849). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.