
Abstract
Financial hardship was pervasive during the COVID-19 pandemic, with adverse consequences for mental health. However, access to state-level paid sick leave during the pandemic had the potential to reduce the mental health burden of financial hardship—a possibility that has not been tested in prior research. Using nationally representative survey data on more than 1.7 million individuals from the Household Pulse Survey (August 2020 to November 2022) merged with state-level data on paid sick leave policies, we estimated a battery of two-way fixed-effects linear probability models to examine whether paid leave policies buffered the association between financial hardship and depression and anxiety risks. Results show that experiencing financial hardship increased depression and anxiety risks but that the mental health consequences of financial hardship were dampened for respondents living in a state with an active paid sick leave policy. Moreover, because racially minoritized adults, women, transgender adults, and less-educated adults were more likely to experience financial hardship over the period, our study highlights the potential for paid leave policies to reduce population inequities in mental health. We point to paid sick leave policies as an important macro-level determinant of mental health with especially salient mental health consequences for marginalized groups.
Few households in the United States were spared from the economic consequences of the COVID-19 pandemic. In the early months of 2020, massive unemployment and wage losses created an initial economic shock (Bureau of Labor Statistics 2020). In the ensuing months and years, millions of U.S. households experienced financial hardship stemming from continued unemployment or underemployment, periods of lost work due to illness and caregiving demands, and soaring inflation that limited purchasing power. Indeed, throughout the pandemic, approximately one-third of adults reported difficulty paying for household expenses (U.S. Census Bureau Household Pulse Survey N.d.). Although pandemic policies such as stimulus payments, expanded unemployment insurance benefits, and child tax credits provided much-needed financial assistance to millions of families in 2021 (Fulford 2023; Parolin 2023), these policies were short-lived and poverty rates soared again by 2022 (U.S. Census Bureau 2023). The high prevalence of financial hardship is particularly concerning in light of robust linkages between financial hardship and mental health during the pandemic (Boen et al. 2023; Kim 2021; Zheng et al. 2021).
However, it is possible that state policies enacted during this period buffered some of the adverse mental health consequences of financial hardship. In the first 2 years of the COVID-19 pandemic, states passed and implemented massive suites of policies (e.g., eviction moratoria, freezes on utility shutoffs), and a growing body of research highlights that these state-level policies had indirect effects on population-level mental health, especially among financially vulnerable adults (Boen et al. 2023; Donnelly and Farina 2021; Donnelly and Schoenbachler 2024). While some states established paid sick leave in the years prior to the pandemic, several others implemented paid sick leave policies during the pandemic. Increased access to sick leave during the pandemic may have helped to reduce the mental health burden of financial hardship for financially vulnerable households. For instance, paid sick leave policies can protect individuals and households from experiencing lost wages and/or the threat of job loss due to illness or caregiving demands. In this sense, paid sick leave policies may have minimized income loss and reduced stress in ways that protected mental health, especially for financially vulnerable households. Despite this possibility, we lack understanding of the role of state-level-level paid sick leave policies for the mental health of adults in the United States.
This study, then, examines whether state paid sick leave policies during the COVID-19 pandemic moderated the association between financial hardship and depression and anxiety risks. To do so, we use nationally representative survey data from the Household Pulse Survey (HPS; August 2020 and November 2022) merged with time-varying, state-level data on paid sick leave policies. In the absence of a national paid leave policy, state-specific policies emerged as a patchwork social safety net prior to and during the pandemic. We harness variability in whether states implemented paid sick leave policies and the timing of such policies to understand the role of state paid leave policies for the mental health of adults experiencing financial hardship. Moreover, we consider these findings in the context of stark inequities in exposure to financial hardship by race/ethnicity, educational attainment, and gender. By examining two different mental health outcomes (i.e., depression and anxiety risks), our study demonstrates the robust impacts of financial hardship and paid sick leave for mental health broadly.
This study makes three main contributions. First, prior research on state paid sick leave laws often focuses on changes in health outcomes in single states following the enactment of such laws (e.g., Jeung, Lee, and Gimm 2021; Ko and Glied 2021; Schneider 2020). We build on this research by harnessing data from all 50 states, providing a more comprehensive view of the impacts of these state-level policies. Second, the few studies that examine paid leave policies across multiple states prior to and during the COVID-19 pandemic tend to focus on markers of viral transmission, including influenza and COVID-19 (Pichler, Wen, and Ziebarth 2020; Pichler, Wen, and Ziebarth 2021). We extend this line of inquiry to consider the indirect impacts of these policies on mental health outcomes. Paid sick leave policies may not be implemented for the purpose of improving mental health, but our study documents the unintended and indirect benefits of these policies for mental health, especially for individuals experiencing financial hardship. Finally, our estimation strategy includes a battery of linear probability models with state and week fixed effects and controls for other state-level pandemic-related policies implemented during this time, which together helps to account for observed and unobserved sources of potential confounding. Altogether, our study sheds light on the promise of state-level paid sick leave policies to reduce mental health consequences of financial hardship—a critical endeavor in light of the mental health crisis occurring during the COVID-19 pandemic (Coley et al. 2022; Czeisler, Howard, and Rajaratnam 2021; Ettman et al. 2020; Twenge and Joiner 2020) and rising levels of inequality in the United States more broadly (Qureshi 2023; Semega and Kollar 2022).
Background
Financial Hardship and Mental Health during the COVID-19 Pandemic
The economic downturn of the COVID-19 pandemic sent financial shockwaves through U.S. households. Historic levels of unemployment in the first months of the pandemic (Bureau of Labor Statistics 2020) were accompanied by wage freezes and wage cuts (Cajner et al. 2020), resulting in income losses for almost half of American households (Donnelly and Farina 2021). Moreover, inflation soared in 2021 and 2022 (Bureau of Labor Statistics 2023), reducing the purchasing power of most households. Consequently, approximately one in three households reported difficulty paying for expenses throughout the first two years of the pandemic (U.S. Census Bureau Household Pulse Survey N.d.). Although not a direct comparison, only 6 percent of adults reported that they found it difficult to get by in 2019 (Board of Governors of the Federal Reserve System 2020), suggesting a substantial increase in financial hardship during the COVID-19 pandemic.
High levels of financial hardship during the pandemic likely had adverse consequences for mental health. Indeed, linkages between financial hardship and mental health are well documented (for a review, see Frankham, Richardson, and Maguire 2020). Research further confirms the salience of this association during the pandemic. For instance, recent studies document robust associations between financial hardship and mental health outcomes such as depression and anxiety throughout the first years of the pandemic (e.g., Boen et al. 2023; Cozen et al. 2024; Kim 2021; Zheng et al. 2021), even after accounting for pre-pandemic economic hardship and baseline mental health (Bierman et al. 2021). Financial hardship can undermine mental health through a number of channels, including by increasing psychological distress (Alhomsi et al. 2023b), decreasing mastery and self-esteem (Koltai, Bierman, and Schieman 2018), disrupting sleep (Kalousová, Xiao, and Burgard 2019), and contributing to food and housing insecurity (Kim 2021).
Importantly, we emphasize that inequities in exposure to financial hardship during the pandemic may have had devastating consequences for population-level inequities in mental health. Prior to the pandemic, there were striking inequities in financial well-being. Less-educated adults and racially minoritized groups, in particular, experienced greater risks of involuntary job loss (e.g., Brand 2006; Farber 2010; Moore 2010) and financial hardship (Barker et al. 2022; Iceland and Sakamoto 2022) compared to more advantaged groups. During the pandemic, the burden of financial hardship fell disproportionately on lower socioeconomic status individuals, racially minoritized adults, and women (e.g., Alhomsi et al. 2023a; Boen et al. 2023; Garcia, Thierry, and Pendergrast 2022; Kim 2021; Zheng et al. 2021) in part because these groups experienced disproportionate job and income losses (e.g., Acs and Karpman 2020; Cajner et al. 2020; Kochar 2020; Landivar and DeWolf 2022; Moen, Pedtke, and Flood 2020). These inequities align with employment patterns during previous recessions, wherein women and Black Americans were more likely to experience unstable employment trajectories during the Great Recession and subsequent recovery (Kalousová and Burgard 2022). In this sense, given documented linkages between financial hardship and mental health, differential exposure to financial hardship during the COVID-19 pandemic likely amplified existing inequalities in mental health.
The Role of State-level Paid Sick Leave Policies
In response to the unprecedented and acute economic challenges brought on by the pandemic, federal and state governments introduced legislation to curb some of the most severe economic effects. Federal efforts largely aimed to provide economic assistance to individuals and families through measures such as expanded unemployment insurance benefits and the provision of stimulus payments. However, the United States did not guarantee access to paid sick leave prior to the pandemic, and there was a lack of comprehensive federal legislation that provided extensive paid sick leave to workers during the pandemic, even as COVID-19 case rates soared. The Families First Coronavirus Response Act (enacted in March 2020) mandated national-level paid sick leave but excluded workers at companies with more than 500 employees (U.S. Department of Labor N.d.). Furthermore, the policy was only in place for a short period and expired at the end of 2020, despite the ongoing public health threat posed by the pandemic. As a result, access to paid sick leave remained elusive to most workers throughout the pandemic—a problematic shortcoming given the severity of viral transmission and COVID-19-related mortality in the United States.
In the absence of a national policy, some states implemented paid sick leave policies prior to the pandemic. The onset of the pandemic spurred additional states to implement their own paid sick leave policies to provide workers with paid time off, especially in the event of COVID-19-related illness or quarantine. Still, only 12 states had paid sick leave policies prior to 2020, and four states plus Washington, D.C. implemented a paid sick leave policy during the pandemic, leaving millions of Americans without access to paid sick leave. Moreover, the patchwork of policies at the state level created inequities in access to paid leave. For example, low-income workers, women, and people of color were less likely to report access to paid leave than their higher-income, male, and White counterparts (Harknett and Schneider 2022; Raifman et al. 2021; Schneider and Harknett 2022), even though historically marginalized and vulnerable adults were more likely to experience financial hardship during the pandemic (e.g., Alhomsi et al. 2023a; Boen et al. 2023; Garcia et al. 2022; Kim 2021; Zheng et al. 2021).
Prior research on the effects of state-level paid leave policies has focused largely on health behaviors and physical health outcomes. For instance, evidence suggests that states that provided access to paid sick leave during the pandemic saw decreases in COVID-19 cases (Pichler et al. 2020). This finding aligns with prior research suggesting that state paid leave laws can have physical health-related benefits, such as reducing the share of workers who work while sick (Schneider 2020) and lowering influenza transmission rates (Pichler et al. 2021). However, there is a dearth of research prior to or during the pandemic examining the consequences of state-level paid leave policies for mental health outcomes, perhaps because of the lack of paid leave policies in the United States.
We speculate that state-level paid sick leave policies might have reduced mental health risks during the pandemic, especially among adults who reported experiencing financial hardship. State-level paid sick leave policies have the potential to reduce adverse mental health consequences of financial hardship by directly minimizing income loss and by indirectly reducing stress that may arise when adults are faced with illness or quarantine in their household. Indeed, evidence suggests that the adoption of state-level paid sick leave increases income (Slopen 2024) in ways that likely positively affect mental health. Paid sick leave may also reduce stress by providing a sense of job security when workers must miss work due to illness or quarantine. That is, when they have access to paid sick leave, workers may not experience the threat of job loss if they need to miss work for sickness or caregiving. Moreover, access to paid sick leave may allow workers to balance work and caregiving demands in a way that reduces stress and improves mental health. Taken together, paid leave policies likely reduce stress stemming from actual or anticipated income loss and related financial difficulties, which may be especially consequential for households experiencing financial hardship. As such, we anticipate any mental health impacts of paid sick leave policies will be especially salient for economically vulnerable households. Here, we build on studies of the impacts of individual-level access to paid sick leave (e.g., through an employer) that find reductions in finance-related worries and improvements in mental health when workers take paid leave (Alang, Harris, and Carter 2023; DeRigne et al. 2019; Goodman and Schneider 2021; Kirwin and Ettinger 2022; Stoddard-Dare et al. 2017). We further draw on prior research suggesting that state-level policies have the strongest associations with the mental health of socioeconomically vulnerable populations, in particular (e.g., Boen et al. 2023; Donnelly and Farina 2021; Sances and Campbell 2021).
In considering linkages between financial hardship, paid sick leave, and mental health, we further consider differences in associations across race/ethnicity, gender, and educational attainment. Although previous findings in this area are mixed, there is some evidence of differential vulnerability to stress-related exposures across subgroups, including by race (Brown et al. 2023) and gender (Read and Gorman 2010). Moreover, some evidence suggests that state policies and contexts are especially salient predictors of health among less-educated adults (Donnelly and Schoenbachler 2024; Montez et al. 2019; Slopen 2024), women (Montez, Zajacova, and Hayward 2016), and racially minoritized adults (Homan, Brown, and King 2021). For example, the state policy environment is more likely to affect the choices and constraints of adults with lower levels of education, whereas adults with higher levels of education can deploy their individual resources to protect their health, regardless of the policy environment. Similarly, women and racially minoritized adults may be more vulnerable to the state policy environment compared to men and White adults given that they are more likely to be socioeconomically disadvantaged, caring for children and aging parents, and/or employed in lower-paying jobs. Applying these prior findings to the context of paid sick leave suggests that sick leave may reduce the mental health consequences of financial hardship for marginalized and minoritized groups more so than their advantaged counterparts.
In this study, we test the following specific hypotheses:
Hypothesis 1. In line with prior research, financial hardship will be associated with higher levels of anxiety and depression during the COVID-19 pandemic (August 2020 to November 2022).
Hypothesis 2. State-level paid sick leave policies will moderate the association between financial hardship and depression and anxiety, such that the associations will be weaker for financially vulnerable households living in states with paid leave policies compared to financially vulnerable households living in states without active paid leave policies.
Hypothesis 3. The moderating role of state paid sick leave in the association between financial hardship and depression and anxiety will be especially pronounced for adults with lower (compared to higher) levels of education (Hypothesis 3a), women and transgender people (compared to men) (Hypothesis 3b), and racially minoritized (compared to White) adults (Hypothesis 3c).
Method
Data and Sample
This study draws on data from two sources: (a) nationally representative survey data from the HPS and (a) a state-level dataset on paid sick leave policies. First, the HPS is a 20-minute online survey designed specifically to assess the social and economic implications of the coronavirus pandemic. Although the HPS has a relatively low response rate (between 5% and 7% in most weeks) compared to other population-based social surveys (Peterson et al. 2021), it is uniquely suited for this study because it includes a large, geographically diverse sample and includes information about respondents’ state of residence and mental health, collects data at regular intervals throughout the pandemic, and quickly makes data available to researchers. Similarly large national surveys (e.g., American Community Survey, Current Population Survey) do not assess mental health, whereas other nationally representative surveys that do include mental health questions (e.g., National Health Interview Survey, Health and Retirement Study) do not survey respondents nearly as frequently as the HPS and have considerably smaller samples, precluding a thorough examination of state-level paid sick leave policies.
The HPS is currently administered by the U.S. Census Bureau with other federal agencies. The HPS uses a probability design, relying on the Census Bureau’s Master Address File (MAF) to select a large sample that can produce estimates at the state level. Sampled households are contacted by email and/or text. Data collection began on April 1, 2020, and is ongoing at the time of writing. Surveys were administered weekly for the first 12 weeks of the study before switching to a biweekly schedule. Analyses included data from 39 different waves, starting in August 2020 (HPS Week 13) and ending in November 2022 (HPS Week 51). We started our analysis in August 2020 because the financial hardship question was not asked until week 13.
Second, we created a state-level dataset on paid sick leave policies that included information on whether and when states had active paid sick leave policies. We identified states that had already implemented paid sick leave policies prior to the pandemic (12 states), as well as states that implemented sick leave policies during the pandemic (four states plus Washington, D.C.). For states that implemented paid sick leave policies during the pandemic, we triangulated information from multiple sources (e.g., Barone 2022; A Better Balance 2023) on the start and end dates of each state’s policy. We merged these time-varying, state-level data with the HPS data based on state and survey week.
We restricted the analytic sample to adults between the ages of 18 and 65, given that paid leave policies are most relevant to working aged adults. As a robustness check, we restricted the sample to adults who worked within the past 7 days, and results were similar (available upon request). We present results from all adults aged 18 to 65 as people may use paid leave to support household members such that the benefits of access to paid sick leave may extend beyond the employed respondent. We excluded respondents with missing data on financial hardship (about 5% of the sample) and any of the covariates included in the models (less than 1% of the sample). The final analytic sample consisted of 1,747,288 respondents for depression and 1,748,667 respondents for anxiety.
Measures
The outcomes of interest were depression and anxiety risks (hereafter, depression and anxiety). Depression was assessed using the two-item patient health questionnaire (PHQ-2; Gilbody et al. 2007). The items covered how often over the past 7 days 1 respondents had been bothered by (a) having little interest or pleasure in doing things and (b) feeling down, depressed, or hopeless. Anxiety was assessed using the two-item Generalized Anxiety Disorder scale (GAD-2; Kroenke et al. 2007). The items covered how often over the past 7 days respondents had been bothered by (a) feeling nervous, anxious, or on edge and (b) not being able to stop or control worrying. For each relevant survey question, response options were the following: not at all (0), several days (1), more than half the days (2), and nearly every day (3). From here, each of the scale’s two items were added together (range 0–6). Consistent with prior studies on mental health (Gilbody et al. 2007; Kroenke et al. 2007; Kroenke, Spitzer, and Williams 2003), we consider scores of three or more on the PHQ-2 or GAD-2 as indicative of probable depression and anxiety, respectively.
Although depression and anxiety can be co-morbid conditions, they are distinct outcomes and represent two different dimensions of mental health (Kessler et al. 2008). As such, examining them as separate outcomes provides more nuanced understanding of the mental health consequences of financial hardship and paid sick leave. The use of validated cut points and the examination of two distinct mental health outcomes (i.e., probable depression and anxiety) aligns with recent research on mental health outcomes during the COVID-19 pandemic using data from the HPS (e.g., Boen et al. 2023; Donnelly and Farina 2021; Donnelly and Schoenbachler 2024; Thomeer 2023; Thomeer, Moody, and Yahirun 2023; Twenge and Joiner 2020).
Our primary independent variable was financial hardship, assessed with the following question about difficulty with expenses: “In the last 7 days, how difficult has it been for your household to pay for usual household expenses, included but not limited to food, rent or mortgage, car payments, medical expenses, student loans, and so on?” Response options included “not at all difficult,” “a little difficult,” “somewhat difficult,” and “very difficult.” We coded households that responded somewhat or very difficult as having difficulty paying expenses (1 = has difficulty).
In addition, we included a measure on whether and when states had implemented a paid sick leave policy. This measure was time-varying; thus, we coded the variable as 1 if the state had an active policy in place at the time of the survey and 0 if it had no active policy in place. Paid sick leave policies were fairly similar in their implementation across states in terms of restrictions and the amount of sick leave that could be earned (A Better Balance 2023). Paid sick leave policies typically applied to all employers in the state, although some states required a minimum of 10 to 15 employees in a company (e.g., Arizona, Maine, Maryland). In addition, covered employees could typically earn up to 40 to 48 hours of paid sick time per year.
We included key sociodemographic covariates that may be associated with financial hardship and mental health. Covariates include age (in years), gender (male [reference], female, transgender/none of these), race/ethnicity (non-Hispanic White [reference], non-Hispanic Black, non-Hispanic Asian, Hispanic, other race/ethnicity), educational attainment (less than high school diploma, high school diploma or GED/some college/associate’s degree [reference], Bachelor’s degree, graduate degree), recent income loss (1 = yes), marital status (currently married [reference], previously married, never married), children in household (1 = yes), and household size (continuous). For gender, the response options “transgender” and “none of these” were added in HPS Week 34; gender was dichotomous (male/female) in survey waves prior to Week 34. We also account for two time-varying, state-level policies enacted during this period that may be associated with financial hardship and mental health: eviction moratoria and freezes on utility shutoffs. We coded these variables as 1 if states had an active policy in place at the time of the survey and 0 otherwise.
Analytic Approach
We first present descriptive statistics for the full analytic sample and stratified by financial hardship and state-level paid sick leave policy. We also present descriptive time trends of the paid sick leave policies across states during the study period, as well as descriptive time trends of financial hardship, depression, and anxiety by race/ethnicity, gender, and educational attainment.
To test associations between financial hardship, paid sick leave policies, and mental health outcomes, we estimate linear probability models with state and week fixed effects. The week fixed effects absorb time trends at the national level (e.g., federal policy change), and state fixed effects absorb time-invariant confounders at the state level (e.g., age, race, or gender composition of the state population). Because of the time frame of the study (August 2020 to November 2022), the state fixed effects also absorb state-level policy confounders that are stable during this time. State and week fixed effects essentially allow us to examine the mental health of individuals living in the same state over time. We rely on linear probability models over other models (e.g., logistic regression models) because linear probability models can produce less-biased estimates when including multiple fixed effects in models with binary outcomes (Gomila 2021). We first regress each outcome (i.e., depression, anxiety) on financial hardship and the state-paid sick leave policy before adding the interaction of financial hardship with paid sick leave in a second model. All models include the sociodemographic and state-level policy covariates.
We applied sampling weights to the descriptive statistics and the linear probability models to account for the survey design. We clustered standard errors by state in regression models.
Results
Descriptive Statistics
Table 1 presents the weighted descriptive statistics for the analytic sample and separately by financial hardship and state paid sick leave. Financial hardship was pervasive during this time period (August 2020 to November 2022): one in three respondents (35%) reported difficulty paying for usual household expenses. Table 1 also shows the high prevalence of depression (27%) and anxiety (34%) in the sample, with stark inequities in mental health by exposure to financial hardship. For instance, the prevalence of depression was almost three times higher for adults experiencing financial hardship compared to adults with little or no financial hardship. The prevalence of anxiety was about 2.5 times higher for adults with financial hardship relative to adults not experiencing financial hardship. Individuals experiencing financial hardship were more likely to be women or transgender adults, non-Hispanic Black or Hispanic adults, have lower levels of educational attainment, unmarried, and have children in the house.
Weighted Descriptive Statistics for Analytic Sample (Household Pulse Survey, n = 1,747,288).
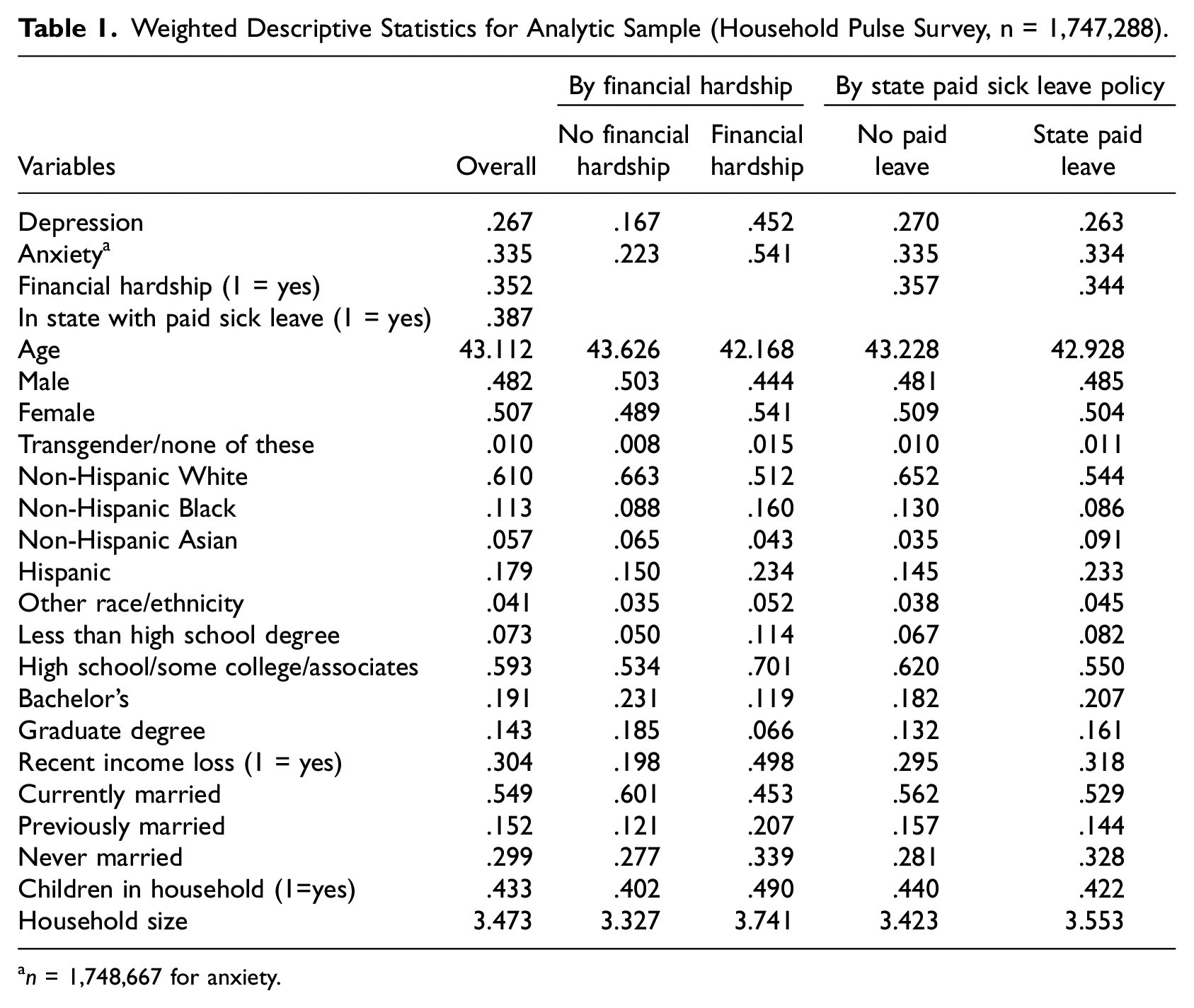
n = 1,748,667 for anxiety.
Table 1 also shows that 38.7% of respondents lived in a state with paid sick leave. Levels of financial hardship were slightly higher in states without paid sick leave compared to states with paid sick leave. Respondents in states without paid sick leave were also more likely to be non-Hispanic White or non-Hispanic Black and to have a high school diploma or some college education.
Figure 1 shows the timing of paid sick leave policies in each state and the District of Columbia from August 2020 to November 2022 (weeks 13–51 of the HPS). The majority of states never had a paid sick leave policy during this time. Among the states that had a paid sick leave policy, 12 had a policy prior to the pandemic, two implemented a policy in the first months of the pandemic (i.e., prior to Week 13 of the HPS), and three implemented a policy after the first months of the pandemic (i.e., after Week 13 of the HPS). Altogether, Figure 1 demonstrates heterogeneity in the presence and timing of paid leave policies across states. In Figure 2, we present the proportion of respondents in the HPS living in a state with an active paid sick leave in each week of the study period. Figure 2 shows some variation over time as states adopted paid sick leave policies and as the composition of the HPS changed slightly over time.
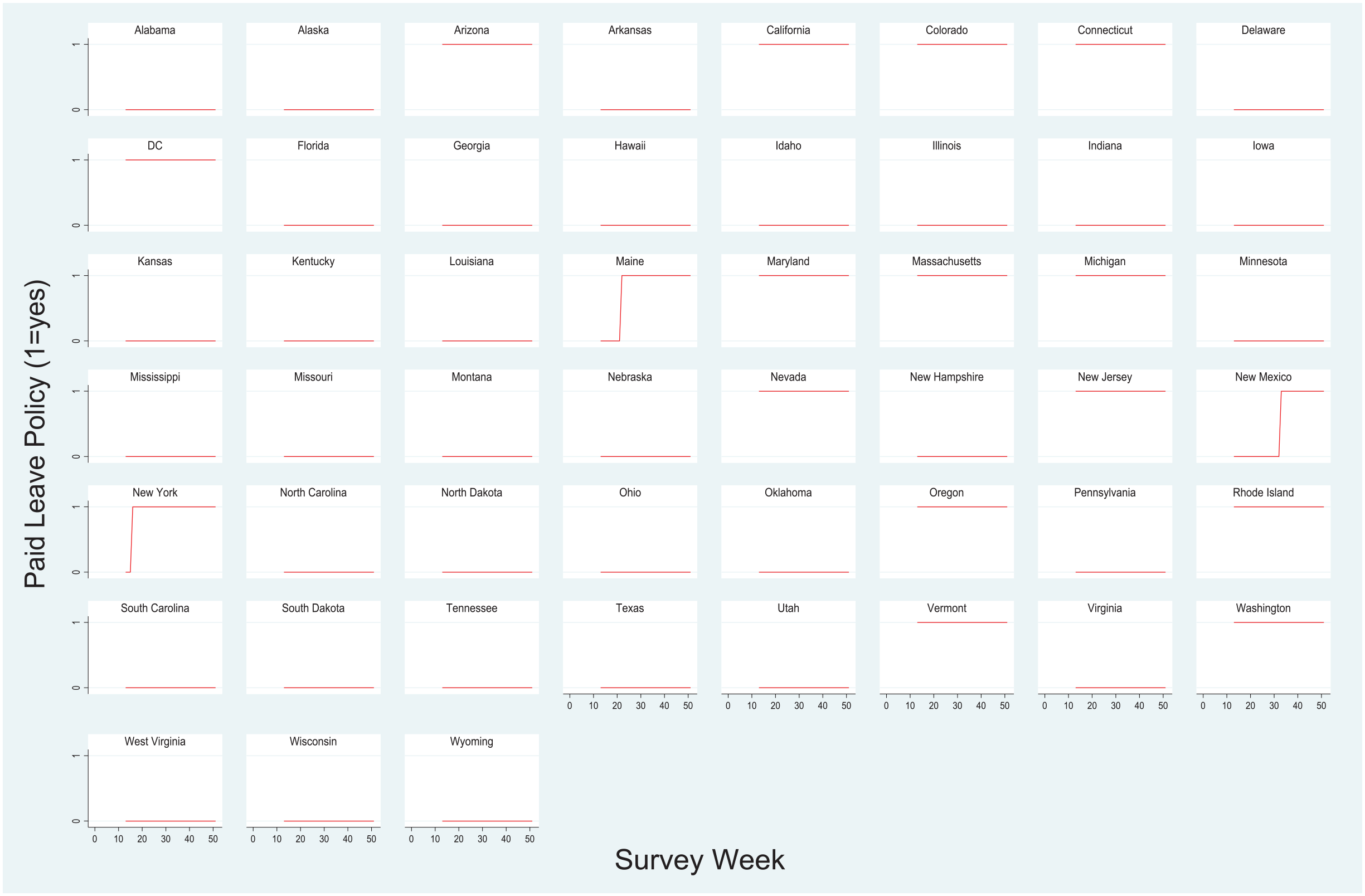
Paid sick leave policy by state and week of Household Pulse Survey.
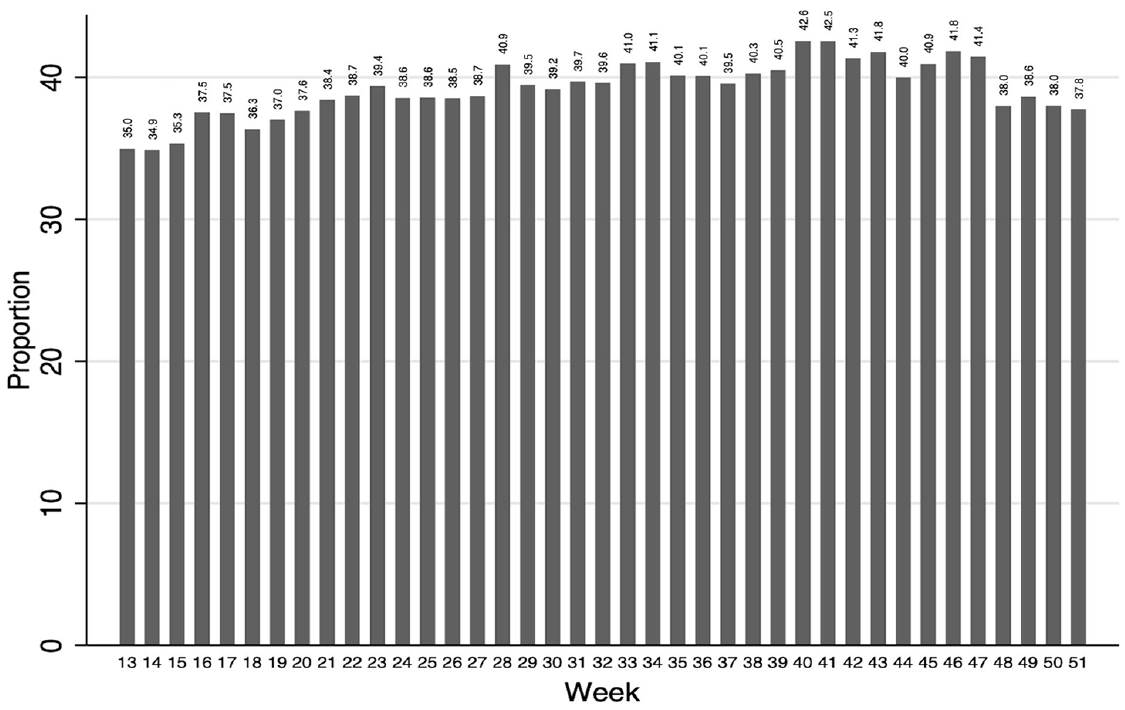
Proportion of respondents living in a state with an active paid sick leave policy by week of the Household Pulse Survey.
Financial Hardship, State-Paid Sick Leave Policies, and Mental Health
Table 2 presents results from linear probability models regressing depression (Panel A) and anxiety (Panel B) on financial hardship. Results in Model 1 of Panels A and B show robust associations between financial hardship and depression and anxiety, respectively. Results show that reporting financial hardship is associated with a 24.2 percentage point increase in the probability of depression (p < .001; Panel A, Model 1) and a 28.4 percentage point increase in the probability of anxiety (p < .001; Panel B, Model 1), net of covariates. Findings provide strong support for Hypothesis 1. Results also shows that living in a state with an active paid sick leave policy is associated with a slight reduction in depression (0.4 percentage point reduction; p < .05; Panel A) and anxiety (0.7 percentage point reduction; p < .05; Panel B).
Weighted Linear Probability Models Regressing Mental Health on Financial Hardship and State-Level Paid Sick Leave Policy (Household Pulse Survey).
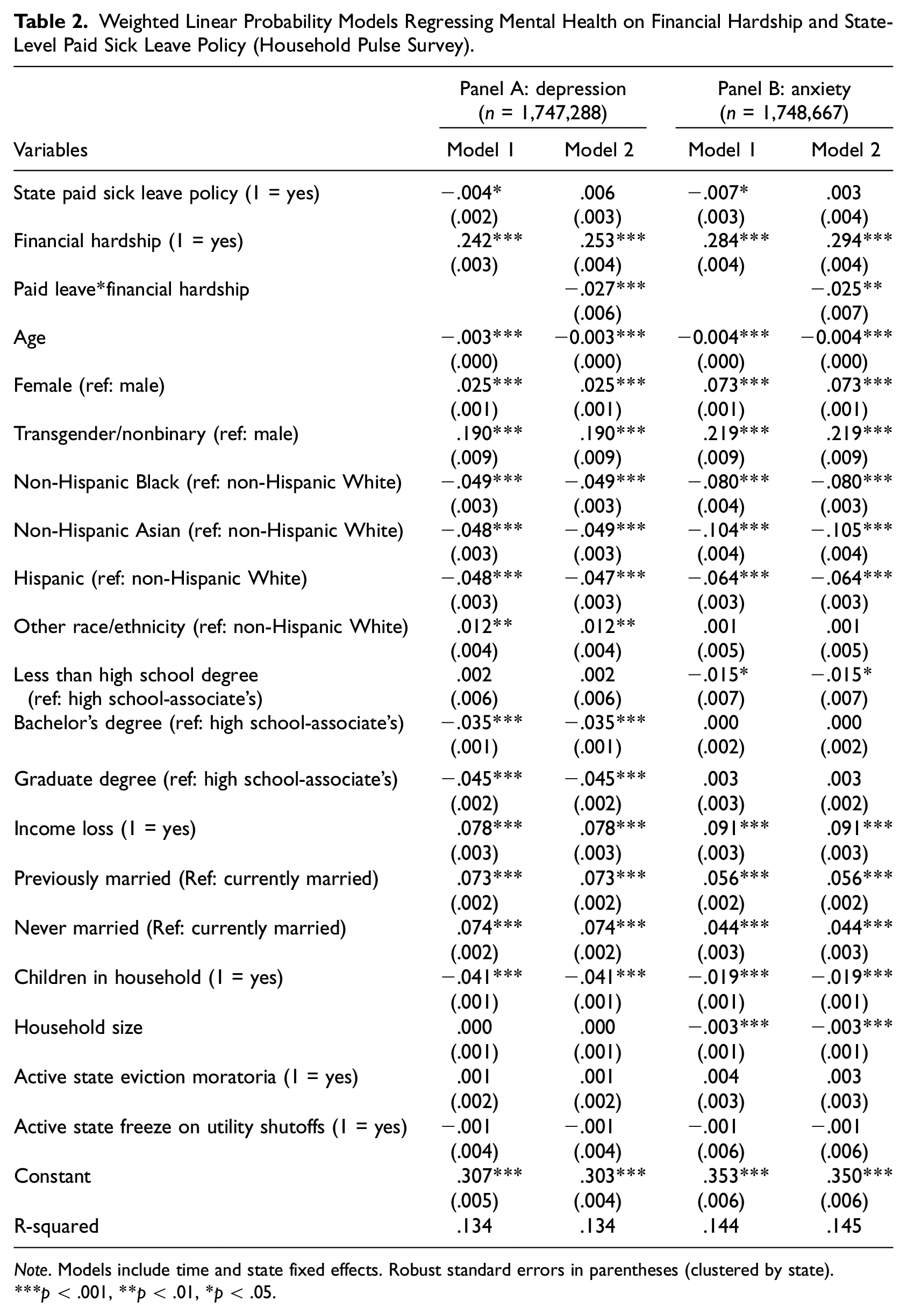
Note. Models include time and state fixed effects. Robust standard errors in parentheses (clustered by state).
p < .001, **p < .01, *p < .05.
Model 2 adds the interaction of financial hardship with state-level paid sick leave policy. The significant and negative interaction term indicates that living in a state with a paid sick leave policy weakens the association between financial hardship and depression (Panel A) and anxiety (Panel B). The main effect for financial hardship in Model 2 shows that difficulty paying for usual household expenses is associated with higher probability of depression (b = 0.253; p < .001) and anxiety (b = 0.294; p < .001) for respondents living in a state without a paid sick leave policy. However, this mental health disparity is slightly smaller in states with active paid sick leave policies. Specifically, living in a state with a paid sick leave policy reduces this disparity by 2.7 percentage points for depression and 2.5 percentage points for anxiety. Findings provide support for Hypothesis 2. Notably, the non-significant main effect of state-paid leave policy in Model 2 suggests that living in a state with a paid sick leave policy is not directly associated with depression or anxiety for adults who are not experiencing financial hardship.
Based on the estimates in Model 2 of Table 2, Figure 3 illustrates the results by showing the average marginal effect of financial hardship by state policy context (i.e., presence of paid sick leave policy). Figure 3 reveals large inequities in the probability of depression and anxiety by financial hardship status in states without a paid leave policy and in states with a paid leave policy as evidence by the large, positive values for each bar in the figure. However, the inequity is about 3 percentage points smaller in states with active paid sick leave policies. Put differently, compared to adults without financial hardship, adults with financial hardship had a 25.3 percentage point increase in the risk of depression in states without a paid sick leave policy; in states with a paid leave policy, adults with financial hardship had a 22.5 percentage point increase in risk of depression relative to adults without financial hardship.
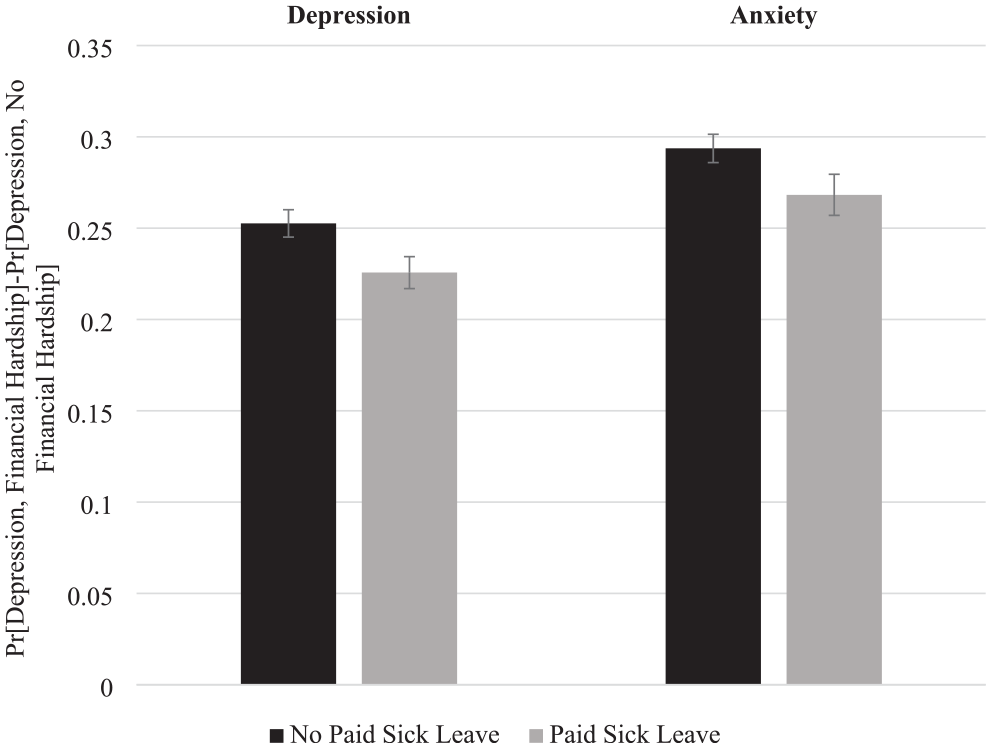
Average marginal effect of financial hardship on depression and anxiety by state paid sick leave policy (Household Pulse Survey).
As a robustness check, we examine whether paid sick leave policies weaken associations between recent income loss—another socioeconomic indicator—and depression and anxiety (Supplement A). The negative and significant interaction term in Panel A indicates that sick leave policies weakened the association between income loss and depression. Specifically, the difference in depression between those experiencing recent income loss and those not experiencing income loss is about 1.7 percentage points smaller in states with an active paid sick leave policy (b = −0.017; p < .01). Although the interaction term is negative in Panel B, it is not statistically significant, suggesting that paid sick leave policies may not weaken the adverse consequences of income loss for anxiety. Overall, these results add support to the hypothesis that paid sick leave policies can help to protect the mental health of financially vulnerable households.
Inequities by Race/ethnicity, Gender, and Educational Attainment
Table 1 shows that women, transgender adults, non-Hispanic Black adults, Hispanic adults, and adults with lower levels of educational attainment were more likely to report difficulty paying for household expenses compared to their male, non-Hispanic White, and higher educated counterparts. To explore these inequities over the study period, we plot descriptive time trends in financial hardship, depression, and anxiety by race/ethnicity, gender, and educational attainment (Figure 4). Figure 4 confirms stark inequities in exposure to financial hardship by race/ethnicity, gender, and educational attainment. Compared to non-Hispanic White and Asian adults, non-Hispanic Black, Hispanic, and other racial/ethnic adults were about twice as likely to report difficulty paying for household expenses in every week (Panel A). Moreover, transgender adults and women were more likely to experience financial hardship compared to men (Panel B). Panel C reveals a stark gradient in financial hardship by educational attainment. For instance, adults without a high school diploma were almost three times as likely to experience financial hardship compared to adults with a Bachelor’s or graduate degree.
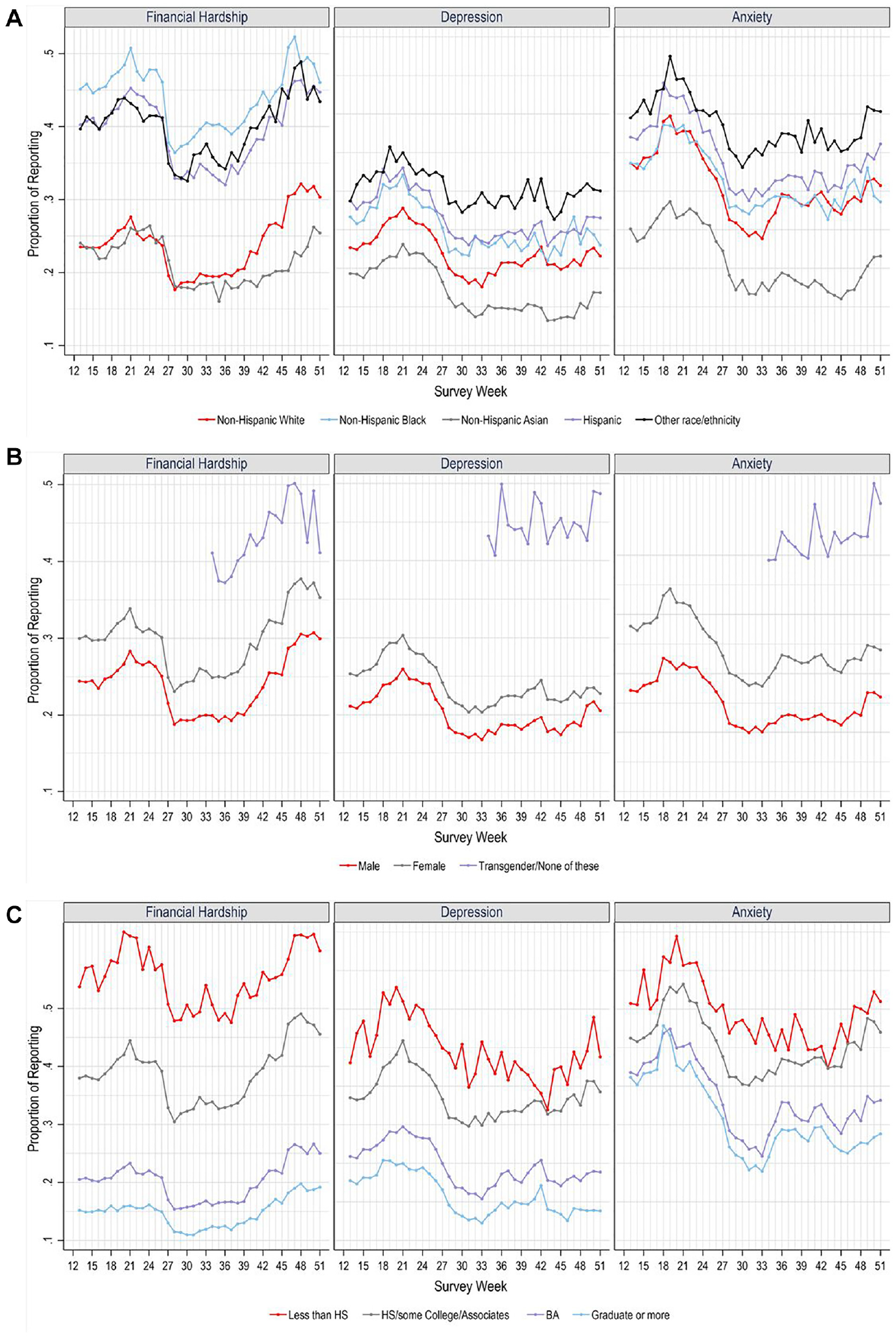
Descriptive time trends in financial hardship and mental health by race/ethnicity, gender, and educational attainment (Household Pulse Survey). Panel A. By Race-Ethnicity. Panel B. By Gender. Panel C. By Educational Attainment.
Across race/ethnicity, gender, and educational attainment, Figure 4 shows that the prevalence of financial hardship was not stable over time. Financial hardship generally decreased around week 26 (March 2021) followed by an increase that began to accelerate around week 40 (December 2021). Notably, some COVID-19-era safety nets began to expire at the end of 2021, such as the expanded child tax credit, and inflation continued to soar.
Figure 4 also shows inequities in the prevalence of depression and anxiety by race/ethnicity, gender, and educational attainment. For instance, non-Hispanic Asian adults reported the lowest rates of depression and anxiety, whereas other racial/ethnic minoritized adults had the highest risk (Panel A). Moreover, the prevalence of depression and anxiety was significantly heightened among transgender adults followed by women, with the lowest prevalence of depression and anxiety among men (Panel B). When considering educational attainment, adults with lower levels of educational attainment (i.e., less than a Bachelor’s degree) had higher rates of depression and anxiety compared to higher educated adults (i.e., adults with a Bachelor’s or graduate degree) (Panel C). Overall, Figure 4 shows stark inequities in financial hardship, depression, and anxiety by race/ethnicity, gender, and educational attainment across the study period (August 2020 to November 2022).
We also examined the possibility of differential vulnerability in the associations between financial hardship and mental health, including the moderating role of state-paid leave policies, by examining models stratified by race/ethnicity, gender, and educational attainment. Results (Supplement B) indicate robust, positive associations between financial hardship and mental health outcomes across gender, race/ethnicity, and educational attainment. Moreover, when examining the moderating role of state paid sick leave, results were generally similar across gender and most racial/ethnic groups: living in a state with a paid sick leave policy weakened the association between financial hardship and mental health. We note that the interaction term was not statistically significant for transgender adults and for some racial/ethnic groups (i.e., non-Hispanic Black, Hispanic) despite coefficients of similar magnitude; we speculate that some stratified models may be lacking statistical power. However, the interaction term was near zero for non-Hispanic Asian adults, providing initial evidence of a weaker impact of paid sick leave for these adults. When examining educational attainment, state paid sick leave policies generally moderated the association between financial hardship and mental health across all levels of educational attainment except for adults with a graduate degree. Altogether, findings from these stratified models generally provide support for Hypothesis 3a (education) but limited support for Hypothesis 3b (gender) and Hypothesis 3c (race/ethnicity).
Discussion
In addition to its devastating impacts on population mortality, the COVID-19 pandemic fueled high rates of financial hardship in the United States—a significant concern for population health and well-being. While prior research documents adverse mental health outcomes stemming from financial hardship during the pandemic (Boen et al. 2023; Kim 2021; Zheng et al. 2021), questions remained as to whether state paid sick leave policies buffered the adverse consequences of financial hardship during the pandemic. To address this gap, we examined whether state-level -paid sick leave policies moderated the association between financial hardship and depression and anxiety risks during the pandemic. Broadly, findings from this study point to the importance of state policies as a macro-level determinant of mental health; more specifically, this study highlights the utility of paid sick leave policies as an intervention for protecting the mental health of financially vulnerable adults. Our study supports three broad conclusions.
First, in line with prior research on the mental health challenges during the COVID-19 pandemic (e.g., Boen et al. 2023; Kim 2021; Zheng et al. 2021), we found that experiencing financial hardship was associated with increased risk of depression and anxiety during this time (August 2020 to November 2022). This study covered a longer period than prior research, confirming the continued toll of financial hardship throughout the course of the pandemic. In addition to the direct public health threat of COVID-19, our study adds to the growing body of research showing that the widespread economic consequences of the pandemic spurred a concurrent mental health crisis. Many mechanisms likely linked financial hardship to adverse mental health outcomes, including increases in distress (Alhomsi et al. 2023b), reduced self-esteem and sense of control (Koltai et al. 2018), sleep disruptions (Kalousová et al. 2019), and heightened food and housing insecurity (Kim 2021). Overall, financial hardship affected one in three households during this time and represented a significant concern for population mental health.
Second, our study underscores the importance of state-level paid sick leave policies for the mental health of vulnerable adults, in particular—a link that has not received much scholarly attention. Our findings indicated that the mental health consequences of financial hardship were weaker for respondents living in a state with an active paid sick leave policy. This finding aligns with prior evidence that state policies such as eviction moratoria and unemployment insurance weakened the adverse mental health consequences of financial hardship (Boen et al. 2023) and household income loss (Donnelly and Farina 2021). While a previous study found that state paid sick leave policies weakened associations between household income loss and mental health during the first 3 months of the pandemic (Sances and Campbell 2021), we extended this research by taking a rigorous analytic approach that used time and state fixed effects to examine how state paid sick leave policies buffered individuals from the mental health consequences of financial hardship over a 2-year period (August 2020-November 2022). Although previous research showed that paid sick leave policies reduce illness transmission (Pichler et al. 2020, 2021) primarily by reducing the share of workers who worked while they were ill (Schneider 2020), our findings suggest that paid sick leave policies also have indirect and unintended benefits for population-level mental health, particularly among financially vulnerable individuals. By limiting the loss of income and/or reducing stress from the threat of job loss when workers had to miss work due to illness or caregiving needs, paid sick leave policies likely prevented the loss of needed resources among households experiencing financial hardship, while also reducing stress.
Taken together, paid sick leave policies helped to reduce mental health consequences stemming from financial hardship. Although the effect size was modest, the reduction in the risks of anxiety or depression associated with these policies may be quite meaningful on a population level. Specifically, these reductions represent a decrease in levels of depression and anxiety among millions of Americans. Therefore, the reduction in the number of people with probable depression and anxiety resulting from these policies is an important step forward toward the goal of improving population mental health. Furthermore, the paid sick leave policy was just one policy that likely operated in tandem with other policies (e.g., eviction moratoria, protections against food insecurity, access to affordable childcare) to create a meaningful social security net for vulnerable Americans. Indeed, a recent study found that living in a state with an active eviction moratorium reduced anxiety and depression among individuals experiencing financial hardship between 2.3 percent and 5.0 percent (Boen et al. 2023)—effect sizes similar to the ones in this study (i.e., 2.5% and 2.7%). Together, these pandemic-related safety net policies may have meaningfully protected population mental health during an extremely stressful and tumultuous period.
Finally, findings point to the potential of paid sick leave policies for ameliorating inequities in mental health. We found that paid sick leave policies reduced the risk of depression and anxiety among financially vulnerable adults in similar ways across race/ethnicity, gender, and educational attainment (with the exception of the highest educated, who received fewer mental health benefits from these policies). The limited buffering role of state paid sick leave among the highest educated respondents aligns with prior research suggesting that individuals with less education are more vulnerable than higher-educated adults to state-level policies (Montez et al. 2019). Adults with higher levels of education can harness their resources to promote health and well-being regardless of the policy environment. Results from the stratified analyses generally supported the conclusion that the impacts of paid sick leave policies were similar across subgroups. Despite the general lack of support for differential vulnerability to financial hardship or paid sick leave policies, our results suggest that differential exposure to financial hardship likely played an important role in mental health inequities during the pandemic. Indeed, differential exposure to social exposures like financial hardship is a central pathway underlying the production of inequities in health and well-being (Ward et al. 2019). Moreover, because racially minoritized adults, women, transgender adults, and less-educated adults were more likely to be exposed to financial hardship, paid leave policies would be especially beneficial for mental health in these populations. Thus, unequal exposure to financial hardship is a pressing issue for population health, especially in times of crisis. In light of unequal exposure to financial hardship, our results point to the potential of paid sick leave policies for promoting health equity, as these policies may reduce the mental health burden among financially vulnerable adults who are disproportionately racially minoritized, women, transgender, and less-educated adults.
Although we found that state paid sick leave policies were important in the context of a public health crisis, the mental health benefits of state paid leave policies likely extend beyond the height of the pandemic, as people continue to face illness and caregiving demands in everyday life. Indeed, prior research showed that individual access to paid leave is associated with less psychological distress (Alang, Harris, and Carter 2023; Stoddard-Dare et al. 2017). However, much remains to be known about how state paid sick leave policies impact the mental health of citizens beyond the pandemic—an important avenue for future research. This study offers a useful framework for understanding how individual experiences and state policy environments intersect to shape mental health. However, we emphasize that the haphazard adoption of paid leave policies by states creates vastly unequal living conditions for residents depending on their state of residence, fueling geographic inequities in mental health. A national paid leave policy that uniformly affects all households would be an equitable approach to improving mental health in the population, especially among financially vulnerable households. Indeed, the United States remains the only high-income country without access to paid sick leave (Rho, Fremstad, and Gaby-Biegel 2020)—a significant concern for population health and well-being.
This study provides new and important insights into the population health benefits of state-level paid sick leave policies. However, limitations should be noted. First, we rely on cross-sectional data from the HPS, so we are unable to look at within person changes in mental health as policies are implemented and allowed to expire, for example. We also cannot account for baseline mental health, which might raise concerns about reverse causality in the associations between financial hardship and mental health. We note, however, that prior research finds support for a causal linkage between financial hardship and mental health beyond selection effects (Bierman et al. 2021).
Second, we are unable to assess the chronicity of hardship in this study. Compared to short-term, episodic exposure, longer durations of financial hardship have an especially pernicious effect on health and well-being (e.g., Bierman et al. 2021; Kahn and Pearlin 2006; Shippee, Wilkinson, and Ferraro 2012), but we are unable to capture heterogeneity in exposure to hardship in this study. Still, it is possible that the benefits of paid leave policies may differ depending on the duration or extent of financial hardship.
Third, although we assess the availability of state-level paid sick leave, we do not know whether respondents were aware of their eligibility for these policies. Indeed, more than half of employees were unaware of the paid sick leave options provided under the Families First Coronavirus Response Act in 2020 (Jelliffe et al. 2021). It is possible that if employees were unaware of their ability to access paid sick leave, they would not reap the mental health benefits from the policy. This scenario is separate from the possibility that employees knew about their ability to access paid sick leave, but it did not affect their mental health, in which case raising awareness of the policy would not improve population mental health. Understanding the role of differential awareness to state policies is an important endeavor for future research in this area.
Fourth, if paid sick leave policies reduce financial hardship in the population, then the composition of the financially vulnerable population could change over time after policy implementation. The possible effect on results in this study is unclear (i.e., whether differences in mental health by financial hardship would widen, narrow, or stay the same), and this issue warrants consideration in future research.
Finally, the HPS is an internet-based study with a relatively low response rate, and the most financially vulnerable adults (who may benefit the most from paid sick leave policies) may be less likely to participate in the study than more financially secure adults. This selection bias would likely lead to conservative estimates in this study.
This study contributes to a growing research area on the importance of state policies for the health (Montez, Hayward, and Zajacova 2021), including mental health (Boen et al. 2023; Donnelly and Farina 2021), of adults in the United States. The increasingly polarized state policy environment in the United States (Montez 2020) suggests that Americans will have vastly different experiences of health and well-being depending on where they live. This possibility is especially true for structurally marginalized and/or vulnerable adults who tend to feel the effects of state policies more acutely (Montez et al. 2019), including households that experience financial hardship. Although this study considered the benefits of paid sick leave—one policy embedded in the broader sociopolitical landscape—we document a notable decrease in depression and anxiety among financially vulnerable adults. One in three households experienced financial hardship during this time period (U.S. Census Bureau Household Pulse Survey N.d.), making these paid leave policies a valuable resource to millions of Americans. As more states continue to adopt paid leave policies beyond the pandemic, future research should document the range of benefits for population health. We point to paid sick leave policies as an important avenue for promoting mental health in the population and for reducing inequities in mental health.
Supplemental Material
sj-docx-1-smh-10.1177_21568693241300133 – Supplemental material for State-Level Paid Sick Leave Policies and Population Mental Health during the COVID-19 Pandemic in the United States
Supplemental material, sj-docx-1-smh-10.1177_21568693241300133 for State-Level Paid Sick Leave Policies and Population Mental Health during the COVID-19 Pandemic in the United States by Rachel Donnelly, Whitney Frierson, Zhe Zhang and Courtney E. Boen in Society and Mental Health
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: R.D. is grateful to the National Institute of Mental Health (grant no. R03 MH128649) and the Dean’s Faculty Fellowship program at Vanderbilt University for support. C.E.B. is grateful to the the Population Studies and Training Center at Brown University, which receives funding from the NIH (P2C HD041020), for general support.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.