
Abstract
Lesbian, gay, bisexual, transgender, and queer (LGBTQ) people disproportionately report high exposure to adverse childhood experiences (ACEs). In this study, we examine the ways that LGBTQ people with high ACEs also describe experiencing adverse communication with family systems about mental health, childhood sexual abuse (CSA), and their gender identity. From interviews with a racially diverse sample of 82 LGBTQ people in South Texas, we analyze how this adverse communication—including gaslighting, silence, denial and ignoring—is attentive to courtesy stigma dynamics. This adverse communication impacts transgender people, cisgender LGBTQ people, and Black or Latinx LGBTQ people differently; for example, Black and Latinx LGBTQ people discussed adverse communication about mental health and therapy within their families that prioritized the respectability of the family. These findings provide insight into family dynamics and communication practices in the lives of LGBTQ people, particularly at the intersections of multiple marginalized identities.
Adult children often communicate with their family about important but challenging topics: their own mental health, their childhood experiences, and their gender or sexual identity. Lesbian, gay, bisexual, transgender, and queer (LGBTQ) people consistently report challenging communications with their families about gender and sexual identity, which may involve denial and even violence (Reczek and Bosley-Smith 2021; Rogers 2017; Schmitz, Robinson, and Sanchez 2020). Some families have stronger reactions than others. In this study, we questioned whether individuals with many adverse childhood experiences (ACEs) also have family systems that produce negative communication about these challenging topics. ACEs are stressful or traumatic events prior to adulthood, including abuse, neglect, and household challenges such as family members being incarcerated (Felitti et al. 1998, 2019) An extensive body of research has demonstrated an association between higher exposure to ACEs and adverse mental and physical health in adulthood (Blosnich and Andersen 2015; Felitti 2009; Hughes et al. 2017; Kalmakis and Chandler 2015; Schilling, Aseltine, and Gore 2007). Scholars also have identified family behaviors that mitigate the relationship between ACEs and mental health issues. Positive family communication soften the impact of ACEs on adolescent and adult mental health (Lackova Rebicova et al. 2020; Lensch et al. 2021). However, to date there is little research on the specific dynamics of family communication involving LGBTQ people and discussions around mental health, ACEs, and gender or sexual identity.
In this study, we examined the narratives of family communication about mental health, childhood sexual abuse (CSA), and LGBTQ identity in a racially diverse sample of 82 LGBTQ people in South Texas, half of whom reported a high number of ACEs. We argued that for interviewees with high ACEs, they perceived adverse communication from family members in reaction to discussions of ACEs or LGBTQ identity. Adverse communication includes gaslighting, silence, denial, and ignoring. Interviewees specifically observed this adverse communication around discussions of mental health for Black and Latinx family members, transgender or non-binary identities, and CSA for women within the family. Black and Latinx LGBTQ people reported more gaslighting and denial around discussions of mental health issues, possibly due to the perceived pressure on these family’s courtesy stigma dynamics. Courtesy stigma refers to prejudice and discrimination due to one’s association with a person with the stigmatized identity (Corrigan, Watson, and Miller 2006).
This work is an important contribution to understanding the relationship between family communication and ACEs. Rather than understanding aversion about mental health services within the family as related entirely to mental health stigma, there is value in examining the commonalities with other forms of communication about family troubles. Misogyny, transphobia, and mental health stigma all play a role in adverse communications within the family context. As such, we argue that scholars need to take an intersectional approach to understanding the pressures on families to control the reputation of the family, to have respectability regarding gender, sexuality, and mental health within the family. Adverse communication may be related to family courtesy stigma dynamics.
Furthermore, this work has implications for both future research and clinical practice. Mental health providers can use this research to develop interventions that address adverse communication in the family system and provide those who have experienced ACEs the tools to navigate their families’ fears of courtesy stigma. The diversity of this research sample allows for theorizing that does not depend on predominately White, cisgender, heterosexual samples; instead, we highlighted the experiences of Latinx, Black, transgender, and non-binary people.
Background
LGBTQ people have some of the highest ACEs scores among adults in the United States (Andersen and Blosnich 2013; Andre van Mol 2021; Austin, Herrick, and Proescholdbell 2016; McCabe et al. 2020). One recent study found that over three-quarters (86 percent) of LGBTQ youth (ages 14–18) reported having experienced at least one ACE, and over a third (40 percent) reported high ACEs exposure (four or more ACEs; Craig et al. 2020). Among the LGBTQ population, transgender and non-binary people report disproportionately higher ACEs exposure compared with cisgender people (Schnarrs et al. 2019).
Furthermore, LGBTQ people experience ACEs in the context of heterosexism: a societal level preference for heterosexuality and the devaluation of other sexual and gender identities (Jun 2018). Stigma and discrimination related to heterosexism due to sexual or gender minority identity is referred to as minority stress (Brooks 1981; Meyer 2003). Minority stress is a well-documented determinant of adverse mental health and well-being in LGBTQ populations (Mongelli et al. 2019; Vargas, Huey, and Miranda 2020). Higher rates of ACEs exposure (Friedman et al. 2011; Xu and Zheng 2015), may in part account for the higher rates of mental health issues among LGBTQ adults when compared with their heterosexual counterparts (Blosnich and Andersen 2015).
Protection from the Impact of ACEs
Existing research emphasizes the importance of resiliency strategies and coping mechanisms to help mitigate the effects of exposure to multiple ACEs on mental health and wellbeing (Poole, Dobson, and Pusch 2017). Racial differences in the effects of ACEs among White, Black, and Hispanic people indicate that the mental health effects of multiple ACEs are consistently stronger among White people than Black or Hispanic people (Schilling et al. 2007). An explanation for this could be seen in the coping mechanisms developed by racial minority individuals, especially those who are also LGBTQ, as a result of their disproportionate experiences with racism, homophobia, and other forms of discrimination (Brown et al. 2018). The social environment of an individual, particularly their social support from others, may be important for these coping mechanisms.
Social support has been identified as an important factor in mitigating the adverse effects of discrimination (e.g., racial, homophobic, & transphobic) and ACEs (Prelow, Mosher, and Bowman 2006; Trujillo et al. 2017). Researcher Peggy Thoits (1982, 1986) conceptualized social support as assistance provided for individuals to cope with stressful life events. For negative stressful events in particular, social support can buffer against the adverse effects of negative stress Thoits (1982, 1986) Support can be provided by anyone in the individuals’ social network, but is typically provided by family members, friends, and romantic partners (Thoits 1986).
Regarding coping, social support can be problem-focused or emotion-focused. Problem-focused support assists in managing the stressful event itself. Perceived emotion-focused support may mitigate against psychological distress associated with negative stressful events and chronic strains (Thoits 1986). For example, social support in the form of positive family communication has been found to mitigate the impact of ACEs on adolescent mental health (Lackova Rebicova et al. 2020; Lensch et al. 2021). However, a family’s ability to provide this social support can be compromised as ACEs can dramatically impact family communication; ACEs scores of parents have been linked repeatedly to dysfunctional parent–child relationships and reduced communication between the familial unit (Lê-Scherban et al. 2018). This may be explained by a link between ACEs and parenting stress, which increases the likelihood of childhood trauma and household dysfunction (Lange, Callinan, and Smith 2019). This study analyzed the role of family communication in the lives of LGBTQ people with high exposure to ACEs.
Adverse Communication and ACEs
We argued that for LGBTQ people, perceptions of adverse communication practices from family members (i.e., gaslighting, denial, silencing, and ignoring) around ACEs extend into adulthood as identity-related abuse. Identity-related abuse refers to range of actions a perpetrator may take to target a sexual or gender minority individual’s identity, controlling or demeaning them (Riggs et al. 2016). Identity-related abuse can encompass physical, emotional, and financial abuse. Parents may deny their children’s identities, comment negatively on their children’s gender expression, misgender their children, “deadname” their children (i.e., referring to a transgender individual by the name they were assigned in infancy; Turton 2021), withhold gender-affirming healthcare from their children, and prevent their children from disclosing their identities to others (Riggs and Bartholomaeus 2018; Rogers 2017). LGBTQ people experience high levels of victimization specific to their identities. One national survey of over 27,000 transgender adults in the United States, found that half of interviewees reported familial rejection, including identity-related abuse (James et al. 2016). This identity-related abuse directed at adults may be an extension of abusive dynamics from their childhood (Authors forthcoming). In this study, adverse communication practices refer to behaviors of gaslighting, denial, silencing, and ignoring. Gaslighting can be defined as a set of attempts to create a “surreal” (Ferraro 2006) social environment by making the other in an intimate relationship seem or feel “crazy” (Sweet 2019). Gaslighting is a form of identity-related abuse such that the perpetrator aims to persuade an individual that their thoughts and perceptions are false (Riggs and Bartholomaeus 2018). Gaslighting is effective when it is rooted in social inequalities, especially gender and sexual identity, and executed in power-laden intimate relationships (Sweet 2019). Sweet argues that gaslighting tactics become consequential when abusers mobilize macro-level inequalities related to gender, sexual identity, race, nationality, and class against an intimate other. Gaslighting uses these macro-level inequalities and turns them into micro-level strategies of abuse (Sweet 2019). Denial is often a component of gaslighting and another form of identity-related abuse. It is often difficult to disentangle the two. For example, common forms of both denial and gaslighting may be misgendering and deadnaming. Parents of gender diverse children may employ these tactics to the detriment of their children (Olson et al. 2016; Simons et al. 2013). Silencing and ignoring refers to quieting, being non-responsive, or avoiding communication with family members. silence is often understood as a lack of communication, but also can communicate resistance (Khan and Masud 2017; MacLure et al. 2010; Zhang and Siminoff 2003).
Why adverse communications? An intersectional approach to courtesy stigma
These perceived adverse communications can be a form of identity-related abuse that fit within the broader context of family conflict between LGBTQ adult children and their families of origin (Reczek and Bosley-Smith 2021). Many scholars have examined conflictual and estranged relationships between LGBTQ adults and their families of origin (McConnell, Birkett, and Mustanski 2016; Oswald 2008; Robinson 2018; Roe 2017). In their study of LGBTQ young adults who experienced family rejection and homelessness, Brandon Andrew Robinson (2018) argued that this rejection fits into a history of family instability, which can include “economic hardship, parental, marital, and romantic transitions, residential movement, familial conflict and abuse, family alcohol and drug use in the home, and parent’s mental health challenges” (Robinson 2018:385). Poverty and existing family instability further strained ties between parents and their LGBTQ children. In these “conditional families” that were already strained due to ongoing family instability, youth must meet certain conditions related to gender and sexuality (i.e., abide by heteronormative standards) to be part of the family (Robinson 2018:387).
For LGBTQ people, family relations constantly operate within systems of intersecting oppressive social structures and marginalized identities (Schmitz, Robinson, and Sanchez 2020; Schmitz, Robinson, Tabler, et al. 2020). We take an intersectional family systems approach to examine the multiple sources of oppression within family systems that interact to influence these adverse communication practices (Schmitz, Robinson, and Sanchez 2020; Schmitz, Robinson, Tabler, et al. 2020). Intersectionality as an approach clarifies ways that racism, classism, sexism, and heterosexism intersect in the lives of individuals and families (Cho, Crenshaw, and McCall 2013; Collins 2004; Crenshaw 1990). Families in this study are at the center of intersecting discrimination based on race, class, and gender. For example, Black and Latinx family members may experience more social pressure to police the gender and sexuality of transgender and non-binary family members (Acosta 2010; Higginbotham 1994; Moore 2011; White 2010; Wolcott 2013). Research on familial experiences of Latinx transgender and other gender diverse individuals is limited. In this study, many LGBTQ interviewees identified as Latino, Latina, or Hispanic, and their families may include practices such as promoting machismo or other family strategies to prevent divergent gender identity or behavior (Ocampo 2012; Schmitz, Robinson, and Sanchez 2020). Latin-origin families may place more importance on the needs and values of the family rather than individual family members, an allocentric phenomenon referred to as familism or familismo (i.e., Acosta 2010; Muñoz-Laboy et al. 2009). Latina family members who are sexual minorities may avoid interpersonal conflict in an effort to maintain familial stability (Acosta 2010). This familism orientation may magnify perceptions of adverse communication.
An intersectional family systems approach seriously considers the motivations for families engaging in adverse communication. Underlying the adverse communication may be a resistance to deepening the already existing instabilities within the family. This resistance to increased instability may be related to the possibility of courtesy stigma. Goffman, and others, have documented the “social risks” of associating with stigmatized individuals (Goffman 1963; Östman and Kjellin 2002; Pryor, Reeder, and Monroe 2012), including the spread of stigma to those who are connected to the stigmatized person (Francis 2012). Courtesy stigma is defined as the prejudice and discrimination that is extended to people not because of some mark (e.g., mental illness or disorder) that they manifest, but rather because they are somehow linked to a person with the stigmatized mark (Corrigan et al. 2006). Family stigma is one type of courtesy stigma. There are three common attributes that define family stigma: avoidance and negative attitudes toward a family by others, the belief by others that association with the family could taint or harm them, and the belief that the entire family is contaminated by association with the stigmatized family member (O’Shay-Wallace 2020). For example, family relationships to those with mental illness have been found to be perceived as shameful or to be kept hidden entirely (Angermeyer, Schulze, and Dietrich 2003; Phelan, Bromet, and Link 1998). Stigma within the family also varies within familial roles. Spouses and parents are more likely to be blamed for a person’s mental illness than any other family member (Corrigan et al. 2006). Parents of children with psychological and behavioral disorders experience both courtesy stigma and stigma related to being perceived as bad parents (Corrigan et al. 2006; Francis 2012; Goffman 1963).
Conceptualizing adverse communication as part of courtesy stigma dynamics addresses the different ways family members respond to courtesy stigma (Meisenbach 2010). Both familial and community perceptions on the stigmatized subject define how the family manages the stigma. Black and Hispanic families report experiencing greater stigma associated with mental illness and may experience greater pressure to maintain their family reputation (Corrigan 2005; Wong 2019), including avoiding therapy when they experience traumatic events (Harris 2020). How parents deal with courtesy stigma is often a reaction to external expectations from their community, but they respond to an internalized sense of responsibility in the context of immediate family (Angermeyer et al. 2003). Felt stigma pushes relatives of stigmatized individuals to react to courtesy stigma. To counter the stigmatizing marks, parents, especially mothers, work hard to develop parenting strategies that will place themselves and their child within the realm of normalcy (O’Shay-Wallace 2020). Michaela Rogers (2017) argued that transgender people experience abuse as a result of family members’ perceptions of courtesy stigma, such that “often the gender normative status of families was frequently privileged over and above the well-being of the trans[gender] family member” (p. 237).
Many forms of adverse communications are also courtesy stigma management practices. Sometimes parents’ stigma management attempts result in negative responses and further alienating actions, such as denying the existence of their child’s stigmatized identity (Angermeyer et al. 2003; O’Shay-Wallace 2020). Denial and social distancing from other family members were common courtesy stigma management practices used by parents to try and regain a sense of normalcy in their child. For example, Candy J. Noltensmeyer and Rebecca J. Meisenbach (2016) found that relational partners of burn survivors managed stigma by engaging in denial and ignoring or displaying: challenging others’ perceptions of the stigma (O’Shay-Wallace 2020). Some studies have found that relatives will defend their family against stigma through logical denial by describing how the relative’s substance abuse was inconsistent with the family’s values (O’Shay-Wallace 2020). Families may pressure silence because disclosure threatens their privacy, which is a form of courtesy stigma management (Brule and Eckstein 2016). The culture of silence around family violence further strengthens the impact of courtesy stigma.
Intersectional discrimination based on racism, classism, and homophobia may magnify the pressure to engage in courtesy stigmas. For example, CSA is not acknowledged in some families despite child disclosure or parental discovery, regardless of the sexual or gender identity of the child (Fontes and Plummer 2010). However, LGBTQ adults report greater exposure to CSA than their cisgender and heterosexual peers and may experience more pressure to not speak about this trauma (Blosnich and Andersen 2015). Mignon Moore (2011) analyzed how Black families adjust to the visibility of their adult lesbian children at public and family events; open lesbianism challenges discourses of sexual respectability, expectations of sexual conformity and the conflation of this conformity with respectability. Sometimes Black lesbians engage in “covering” (Goffman 1963; Yoshino 2007) among their family members by minimizing public expression of their lesbianism to reduce stigma associated with their sexual minority identity (Moore 2011). This project took an intersectional family systems approach to understanding how perceived adverse communication practices from family members impact LGBTQ people.
Methods
This study analyzed 82 semi-structured interviews with LGBTQ adults that were part of the 2018 Strengthening Colors of Pride (SCoP) Interview Study. SCoP is a community-based participatory research (CBPR) project aimed at better understanding the development and activation of resilience among LGBTQ individuals living in South Texas, the area that spans from San Antonio down to the border of Mexico. All research for the project was approved by the IRB of [blinded] and funded by the Robert Wood Johnson Foundation Interdisciplinary Research Leaders Program. IRB approval include the allowance of 16- and 17-year-old participants in the study. This project began as a three-year study of resilience among LGBTQ individuals in San Antonio, Texas, as a response to an open call for studies on resilience. The project leaders, two faculty members and a community organizer, all LGBTQ-identified, wrote the grant and reworked the project methods in consultation with a community advisory board (CAB) of nonprofit organization leaders, government officials, and community members. The CAB shaped the interview questions, assisted with recruitment, and assisted with disseminating a pre-screener survey to community members.
Recruitment
The SCoP research team conducted interviews with 82 LGBTQ people 16 years and older between the months of May and September 2018 in San Antonio, Texas. San Antonio is a city with a high poverty rate and a thriving LGBTQ community. Based on Census data, 64 of SanAntonio residents identify as Hispanic, 24 percent identify as non-Hispanic White, 7 percent identify as Black or African American, and 0.7 percent identify as American Indian. The poverty rate is 18.6 percent and the median income is US$53,420.
Interviewees were recruited through an online screening survey. We employed a diverse recruitment strategy that included online recruitment through social media sites (Facebook and Instagram), our CAB networks on- and off-line, community outreach events, table tents at local gay-owned businesses, and during the annual LGBTQ PRIDE event in San Antonio. The online screening survey asked basic demographic information, measures of community connectedness, questions about LGBTQ health, the Brief Resilience Scale (BRS), and a measure of ACEs. Respondents received one point for each adverse childhood experience (abuse, neglect, or household dysfunction) with scores ranging from 0 to 10. The BRS features questions like “I have a hard time making it through stressful events” and “I tend to bounce back quickly after hard times” (Smith et al. 2008).
All interviewees who were recruited into the project were LGBTQ people who lived in San Antonio or the surrounding counties, endorsed at least two positive items on the BRS and reported either a personal income of less than US$30,000 a year or a score of four or more on ACEs. An ACEs score of four or greater has been associated with negative health outcomes in adulthood (Dube et al. 2003). Qualifying individuals were contacted via email or phone, and the research team set up a meeting date and time to conduct the interview at either the Pride Center downtown or the nearest public library to the interviewee’s home. The interviews captured a sample of LGBTQ individuals who may have needed to develop coping mechanisms due to childhood trauma or economic disadvantage.
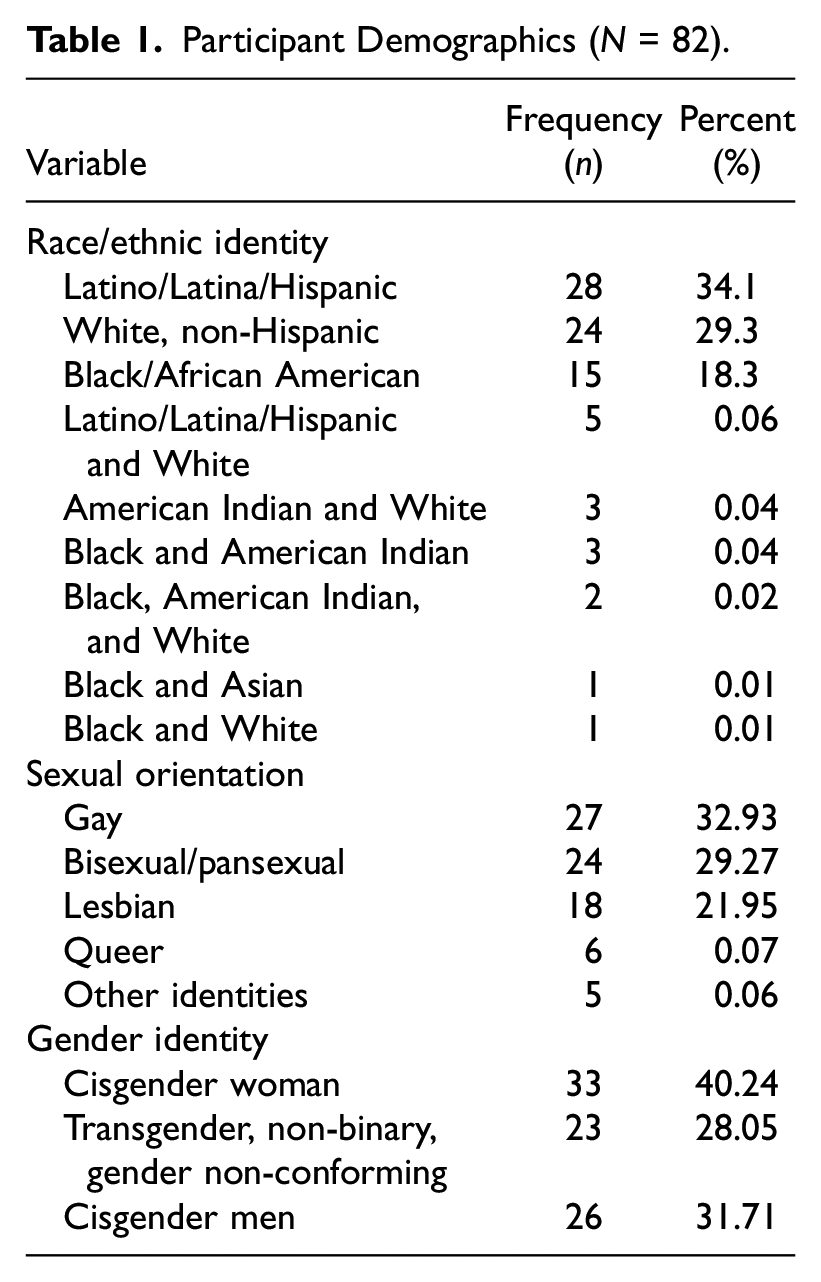
This study focused on an analysis of 82 LGBTQ interviewees, the majority of whom identified as Latinx, White, or Black. Twenty-eight interviewees identified as Latinx or Hispanic, 24 interviewees identified as White and not Hispanic, and 15 interviewees identified as Black or African American. Fifteen interviewees had multiracial identifications that are described in Table 1; the most common multiracial identity was Latinx/Hispanic and White (n = 5). Eight interviewees identified as American Indian or indigenous in combination with other racial or ethnic identities. Interviewees were relatively evenly divided between gay (n = 27), lesbian (n = 18), and bisexual/pansexual (n = 24) adults, except for eleven interviewees who identified as queer or another identity. These interviewees ranged in age from 16 to 71 years old with an average age of 34 years old (SD = 13.4); almost all interviewees were between the ages of 25 and 40 years old. Twenty-three interviewees identified as transgender, non-binary, or gender nonconforming. The most common level of education was some college (n = 28). Most interviewees did not have a college degree and made less than US$40,000 a year. Over half of the interviewees (n = 45) had an ACEs score of 4 or greater.
Participant Demographics (N = 82).
Researchers’ Reflexivity
The research team included nine interviewers: four undergraduate research assistants, two faculty members, one graduate student, and two community members. The team included two Latinx bisexual cisgender women, one Latinx cisgender gay man, one Black cisgender gay man, one Anglo lesbian cisgender woman, one Anglo non-binary queer person, one Anglo cisgender gay man, and an Anglo cisgender bisexual woman. All interviewees were trained in interviewing as a team with a six-hour interview training session, along with two practice interviews, a paired interview with the project PI, and weekly check-ins about the interview process. We were reflective throughout the research process about the racial diversity of our team, our preconceptions about what we would find in our interviews, and the themes about family and mental health throughout the process.
Interview Methods
All interviewees used the same interview protocol to facilitate semi-structured interviews, which included questions about how interviewees navigated challenging experiences, including whether family helped during hard times or made hard times more challenging. All interviews began after covering an extensive consent form. Interviews lasted between 45 and 120 minutes and were conducted in person with one or two research team members. Participants received a US$40 VISA check card to compensate them for their time. All interviews were recorded. All interviews except one were conducted in English. All interviews were transcribed by a professional transcriptionist and entered into NVivo. Interviewers were provided with a handout on mental health resources to provide to interviewees, along with a protocol for reporting mental health crises to the PI.
All participants were given a pseudonym. For cisgender respondents, these pseudonyms were based on the most common baby names for their race and gender. For transgender and non-binary respondents, these names reflect trends in the interviewees’ original names, as they reflect aspects of respondents’ identity they want to emphasize. For example, interviewees with gender-neutral names were given gender-neutral pseudonyms common for their race/ethnicity.
A graduate research assistant coded major themes—mental health, childhood trauma, family, and coming out—using flexible coding techniques common to large-scale interview project data analysis (Deterding and Waters 2021). Sixty-two interviewees mentioned mental health, and among interviewees with ACEs scores of 4 or more, there were 136 references to mental health. The first author analyzed within this theme for family responses to mental health, finding four common themes: “family member has mental health disorders,”“family attitudes toward adults mental health diagnoses,”“family trauma contributing to mental health,” and “childhood mental health issues.” The first author also analyzed the theme “childhood trauma,” which was mentioned by 48 interviewees, and coded any reference to “family not believing or minimizing trauma.” The second author analyzed within this theme for family responses to CSA or disclosure of sexual or gender minority identity, finding four themes: “family member directly/indirectly affirming the participant’s identity,”“family member ignoring or denying the participant’s identity,”“family member estrangement due to identity,” and “family member reacting negatively to participant’s identity.” Using a thematic coding approach, we identified three major domains in the experiences of interviewees: mental health, childhood trauma, sexual and gender identity (Braun and Clarke 2006). Subsequently, using a flexible coding approach, we examined narratives of family communication around the three major domains (Deterding and Waters 2021). We identified four major forms of adverse communication reported by our interviewees: gaslighting, silence, denial, and ignoring.
Findings
Adverse Communication
Interviewees with high ACEs (exposure to four or more ACEs) mentioned many examples of gaslighting, denial, silencing, and ignoring. These types of communication often blurred together or overlapped. Gaslighting was seen primarily in response to sexual or gender nonconformity but also mental health and CSA. Participants who identified as transgender, reported that their parents referred to their transgender identity as a ploy for attention, a mental illness, or an otherwise invalid identity. Furthermore, participants who did not identify with a binary gender (e.g., nonbinary or genderqueer) or who were attracted to individuals of multiple genders (e.g., bisexual), were often told their identities were not “real.” Participants who recalled CSA or mental illness also reported perceived parental gaslighting and denial to disclosure.
Evren, a White bisexual transgender man in his 30s, explained in his interview that “there was a lot of child sexual abuse in my family. It just was not talked about and still isn’t talked about.” He remembered telling his mother about it and getting a response of denial: We’re not gonna talk about this, it didn’t happen. You’re confused.” That was the reaction, which has . . . always been the reaction of my family. It was the same thing I got when I told them that I was gonna date women. It was the same thing I got when I told them that I was gonna transition. It’s kind of always been that reaction. Like “No, you’re just doing this for attention. You’re just making it up. It’s not real.
Evren reported that family members responded to both CSA and his transgender transition saying that the family does not talk about these issues. If he did talk about these issues, his family told him that the phenomenon is not real or did not happen,and communicating about these issues is attention-seeking behavior. Regardless, Evren is the one who speaks of these topics out loud in his family.
Evren talked about the history of sexual abuse in his family, which is not discussed among family members. After opening up about the fact that he was sexually abused, one of Evren’s siblings seemed to understand and believe him. However, his other siblings refused to acknowledge that he had been sexually abused, saying “No. That never happened. I don’t know what you’re talking about.” However, speaking out as an adult was not the first time that Evren had attempted to tell someone about his situation. When he was between the ages of four and six, he attempted to talk to his mother about his sexual abuse. She dismissed it in a similar manner, saying “We’re not going to talk about this. It didn’t happen. You’re confused.” These assertions that the family does not talk about trauma and that the trauma is not being remembered correctly are perceived as forms of gaslighting. Evren compared this with when he told his family that he was going to date women and eventually transition, where he was told that doing it for attention or making it all up. Trauma was at times dismissed because it conflicted with heteronormativity in the family.
Victoria, a White pansexual, cisgender woman in her late twenties, described her mother’s reaction to her rape by her stepfather as “I tell her and she didn’t believe me. She thought I must have had a bad dream and pretended it never happened.” Later, Victoria delayed telling her mother about further sexual harassment, only deciding to tell her in an attempt to protect her siblings, and was met with anger: “she was so mad at me for not telling her. It’s like, how can you be mad at me for not telling you when I told you everything to begin with and you ignored me and you’ve still been with him?” Victoria’s mother consistently gaslit her, claiming that she “must be remembering that wrong” or that events never happened atall.
Other interviewees reported less direct responses from parents and other family members, including silencing and ignoring. For example, Brandi, a White cisgender bisexual woman in her thirties, recalled that if her family was not “comfortable with something, we just avoided talking about it.” One interviewee reported that silencing was used by his parents whenever he brought up accounts of CSA. Bruce, a gay, White cisgender man in his sixties, described his relationship with an abuser as a teenager, noting that his “whole neighborhood had known what was going on.” Yet, his experiences were dismissed consistently. Bruce expressed his immense frustration with these authority figures: “you’re supposed to be my parents, you’re supposed to be the adults. You’re supposed to protect me, and you’re not paying attention. You’re not taking me seriously. What’s wrong with this picture?” In contrast to denial or gaslighting, interviewees reported that their parents ignored expressions of their LGBTQ identities.
Several Black interviewees mentioned that family members ignored their gender expression. Arjana, a Black bisexual transgender woman in her late twenties, sought affirmation from their stepfather on their appearance in association with their gender identity, asking him: “hey, dad, don’t me and mom looked beautiful?.” To which, their stepfather responded “yes, your mom looks beautiful.” In this moment Arjana perceived her father as ignoring their request for affirmation by only addressing the mother’s appearance. Similarly, Kortland, a Black transgender man in their twenties, shared an account of sending their mother a card signed “from your son” to align with their gender identity and reported their mother “didn’t acknowledge it or anything.” Furthermore, Kortland sent photos to their mother (portraying an appearance that matches their gender), and “she just didn’t reply. I knew that was probably going to happen.” Ignoring may be perceived as a relational tactic for parents who are less likely to directly victimize their LGBTQ children (e.g., kicking them out of the house), instead choosing to maintain a stigmatizing, non-affirming environment.
Avoiding Courtesy Stigma, Protecting Family Culture
Most references to parental gaslighting and denial were from Latinx interviewees. Familism and the prioritization of family strength may cultivate gaslighting and denial when individual family members challenge family cohesiveness or values. In one example of both gaslighting and denial, Sebastian, a Latinx bisexual transgender man in his early twenties, disclosed their gender identity to their parents and recalled being told: “no, that’s not who you are,” and “you’re not mentally stable—you need to get help.” Sebastian reported that their parents both denied the existence of their (i.e., Sebastian’s) identity, and felt that they gaslit them by questioning their mental sense, and therefore their view of reality. The perception of their parents’ denial and gaslighting of their identity—as opposed to acknowledging it—may allow for parents to avoid direct confrontation and keep the existing family dynamics intact. Similar to Sebastian’s account, Linda, a Latina transgender woman in their thirties, described their mother’s reaction to their decision to pursue gender-affirming care: “what the hell you mean you’re transitioning? I go I’m becoming a female, I go I’m on hormones. she’s like oh you need to go seek help. I said I already do. He believes me, too, so. She goes you’re both crazy.” Linda reported that their mother gaslit them about their mental state and their gender identity questioning the mental state of Linda’s health professional provider care.
Although transgender and non-binary family were accused of having mental health issues, by contrast other discussions about mental health were off limits in family conversations. Stephanie, a Latinx non-binary person in their twenties, has a White father and Hispanic mother, and described their father’s side of the family as having more people diagnosed with depression and other kinds of mental illness. When Stephanie told their mother about their mental health issues, they reported that their mother responded “that’s some White people bullshit. you need to stop it.” Sebastian as well explained that his father comes from a traditional Hispanic family and “Hispanic families, from my experience, don’t really talk about mental illness.” When Sebastian told them he was struggling with depression and anxiety, he reported that family members responded that they were going to pray for him. Sebastian described that “Hispanic culture over all, as far as mental illness goes, they don’t accept it. You don’t need to go talk to a doctor. You need to ignore it. That’s what everyone else did before you . . . We’re all just going to ignore it and we’re not going to talk about it.”
Silencing included preventing communication or disclosure (i.e., of sexual or gender minority identity) between LGBTQ children and other family members. Sebastian recalled their father preventing them from coming out to their ailing great aunt: My dad was like, “Hey, you can’t—this isn’t your time to come out. You can’t do this, not right now. there’s too much going on and this isn’t about you.” That kind of thing. It really messed me up because . . . this is a person that helped raise me, helped me become the person I am. They don’t get to know who I really am before they pass away.
Familism is central to this interaction, such that Sebastian perceived their father’s response as a prioritization of familial stability over the mental health of his child.
When Marie, a Latinx transgender woman in her mid-twenties, explained to their mother that her boyfriend was touching her inappropriately.
And I would tell her, growing up, little by little, she’d like, “No, that never happened, that never happened. He wasn’t gay, he wasn’t gay. He may have been shooting up heroin, but I know he wouldn’t never do that.” To this day, she still don’t believe me, when I’ve told her several times.”
Marie’s mother’s denial and subsequent gaslighting of the CSA perpetuating by their mother’s boyfriend, was perceived as an attempt to deflect responsibility as a parent for familial instability. Marie’s account fits into a larger theme described by other interviewees of perceived family cultures that supported the denials of sexual violence. When Valeria, a Latina cisgender woman, was molested by a cousin, her grandmother and aunt“said that I basically gave myself to my cousin . . . my dad’s family was Mexican-American and so they had a very different idea of what it was to walk in the world.” But this denial also fit within a family culture of “quietness,” according to Valeria: It wasn’t even just my cousin, it was just, “Oh, here’s another thing that’s breaking my family apart . . . another thing that makes me different.” . . . the queerness, the quietness, this thing with my family. Our family was broken, I didn’t want to make it worse.
Valeria reported that she had internalized an allocentric perspective that places family stability as a priority above her mental health, despite experiencing traumatic CSA. Once again, this perspective may promote gaslighting and denial as mechanisms to promote familial stability.
Furthermore, interviewees reported that primarily their fathers and uncles ignored mental health issues. In one instance, Samantha’s cousin was 13 years old when she had her first manic episode and ran around the house with a knife while at Samantha’s mother’s house. Samantha and her mother took the cousin to the hospital, but her uncle declared that “there’s nothing wrong with her.” Samantha explained that he “had it in his head, how his daughter could not be mentally ill.” Her uncle ended communication with his granddaughter because she is mentally ill. “It’s so strange . . . that whole stereotype of what it is to be macho also won’t allow him to accept any mental illness in the family. Like it’s a blemish. Like it’s seen as a weakness so therefore it doesn’t exist.” Not all interviewees reported this same experience with Latinx men, regarding disclosure of mental illness.
Mateo, a Latinx cisgender gay man in his twenties, reported he had a “macho” uncle who helped him the most. Both times when teenage Mateo tried to commit suicide, he reported that his uncle came to the mental hospital and said “this is not what you are supposed to do. Do you remember that I’m always going to be here for you, that there is no sense in doing this to yourself.” Mateo’s uncle also gave him important advice about interacting with bullies who were beating him up for being gay to “He said, ‘Just tell them this is who you are and that nothing has changed about you’. My uncle he always told me that, ‘Never change who you are . . . keep reminding them.’”
Non-Hispanic interviewees also reported that their family did not believe in mental illness or therapists as part of the family ethos. Eric, a White bisexual non-binary person in their fifties discusses bipolar disorder in their family: My dad first started having real symptoms of this when I was in high school and had to retire early from his job at a lower pension. My mother . . . didn’t believe in psychiatrists and would yell at him, just get your lazy ass out of bed . . . go to work.
Jazmine, a Black bisexual cisgender woman in her thirties, described that both her mother and grandmother had depression but were not diagnosed until later in life, in her 70s for her grandmother, and “they didn’t know how to deal with it.” Jazmine explained that “I don’t know if its a Black thing, I don’t know what it is but my family was like, why do you need to go to a therapist? We don’t deal with our problems, we don’t talk to people about our problems. They say, There’s nothing wrong with you, you want attention. Or you’re being extra or you’re just doing things that just don’t make sense.” For Jazmine, dismissal of mental health issues went together with lack of communication about them, as she reported family members did not like to speak to people outside the family about their problems, and the problems themselves were minimized as attention seeking or “being extra.” Other interviewees, like Mia, a Latina bisexual woman in her late thirties, explained that therapy is taboo in their family.
Multiple individuals reported silencing as a reactionary strategy used by their parents. However, Latinx interviewees were more likely to report that their parents gave an allocentric justification than other interviewees. Shane, a White transgender man in his twenties, was told by their parents they were not allowed to see or share with their grandparents that they were transitioning, and Alex, a White and American Indian transgender man in his twenties, was told by family members, including a brother not to speak to them ever again after coming out. Furthermore, Alex was told not to communicate with their half-sister on social media by their mother. After coming out, Kortland reported that their father did not speak to them for three months. By contrast, these acts were not followed up with an explanation that the family unit was important than the individual.
White interviewees were more likely to report being taken to therapy or a mental hospital as a child, but it often fit into patterns of forced institutionalization. At times, interviewees reported family did acknowledge mental health issues, but only reacted with insufficient treatment, family conflict, and forced institutionalization. Some interviewees experienced treatment of their mental health disorders in childhood, including Jack who reported he was put into a substance abuse facility for children. Devon reported he was hospitalized with anorexia but he remembers that his family viewed his treatment program “as bullshit.” Similarly, Shawn reported he was in and out of mental hospitals throughout his childhood. One Black cisgender woman interviewee, Mistie, reported she was taken to a mental hospital at 16 years old after she called the police and told them “I’m going to kill myself” during a fight with her mother. Mistie stated she the police knew she “was fine” but took her to the mental hospital to “teach her a lesson.” Mistie perceived the attention to her mental health as punitive.
Discussion and Conclusions
In this study, we examined narratives of family communication about mental health, CSA, and sexual or gender minority identity in a diverse sample of 82 LGBTQ people in South Texas. We considered how multiple sources of oppression interact to influence experiences of adverse communication for LGBTQ people within the context of the family system. Furthermore, within this intersectional family systems approach (Schmitz, Robinson, and Sanchez et al. 2020; Schmitz, Robinson, Tabler, et al. 2020), we drew from the theoretical frameworks of minority stress theory and social support. LGBTQ people experience compromised mental health due to stigma and discrimination associated with minority identities (e.g., sexual, gender, or racial/ethnic minority identities; Meyer 2003). In the presence of minority stress, social support may serve as a protective factor (Meyer 2003; Snapp et al. 2015; Thoits 1986). Typically, people receive social support from family members, friends, and romantic partners (Thoits 1986). However, for LGBTQ people, the expectation of social support may be compromised by parental rejection due to their LGBTQ identities (Meyer 2003). Furthermore, occurrence of ACEs within the family system can impact family communication compromising familial social support (Lê-Scherban et al. 2018).
In this sample, we found that interviewees with greater ACEs exposure, perceived greater adverse communication from their families surrounding discussions of ACEs or LGBTQ identity. Participants’ narratives of adverse communication centered on a theme of courtesy stigma, such that participants perceived communication strategies employed by family members as attempts to avoid stigma associated with LGBTQ identities and ACEs (e.g., CSA; Corrigan et al. 2006; Goffman 1963). Avoiding courtesy stigma may be rooted in familism (i.e., allocentrism). Research on Latinx families has found that familismo prioritizes the stability and needs of the family unit over any one individual member (Acosta 2010; Muñozaboy et al. 2009). In our study, interviewees perceivedadverse communication to avoid association with stigma around mental health. Gaslighting and denial—more active forms of adverse communication—were commonly reported in these discussions. By contrast, in discussions around CSA and LGBTQ identity, passive forms of adverse communication: silence and ignoring, were often employed.
Adverse communication in the family context can reinforce self-stigma for people with mental illness or victims of CSA. Self-stigma can undermine a person’s efforts to pursue mental health treatment or even life goals (Corrigan et al. 2006). Similar self-stigma reinforcement (i.e., internalized cis-heterosexism) may occur regarding sexual or gender minority identity. With growing social acceptance of homosexuality, the range of familial responses to disclosure of sexual or gender minority identity, has grown beyond the dichotomy of acceptance/rejection (Seidman 2002). Qualitative research has documented the nuanced ways in which parents of LGBTQ people of color respond to their children’s identities. For example, Latinx parents of sexually nonconforming women may exhibit unspoken tolerance toward their children’s minority identities (Acosta 2010).
Similarly, some research has found parents of Black lesbian women adjust to the visibility of their children in public and expect their adult children to engage in masking behaviors (Moore 2011; Yoshino 2007). Similar to family discussions around mental illness, the many ways parents of LGBTQ adult children negotiate their children’s identities to avoid courtesy stigma are often rooted in familism. Family members of transgender people may withhold gender affirming care or silence them from disclosing their identities, placing perceived needs of the family unit over the well-being of the transgender child. The adverse communication practices we observed in this study: gaslighting, denial, silence, and ignoring, are forms of identity-related abuse. Research has found that sexual or gender identity concealment is associated with poorer psychological well-being (Bockting et al. 2013; Riggle et al. 2017).
The findings of this study have several implications for clinical practice. Understanding family communication dynamics, cultural contexts, and underlying family motivations, will better inform how mental health professionals work with LGBTQ populations. Prior research has found that family-focused interventions are critical in promoting identity affirmation and well-being in LGBTQ people (Lothwell, Libby, and Adelson 2020). A component of family-focused interventions is helping LGBTQ people identify the ways in which they experience discrimination or stigma in the family context. Family members of sexual or gender minority people may not have the tools necessary to engage in positive communication regarding sexual or gender minority identity. Particularly for LGBTQ people exposed to ACEs, resiliency strategies and coping mechanisms are important to mitigating adverse mental health effects and promoting well-being (Poole, Dobson, and Pusch 2017). In the absence of family acceptance toward their children’s sexual or gender minority identity, mental health professionals can further develop interventions that promote coping strategies (Lothwell et al. 2020). For example, promoting community connectedness and positive identity affirmation, and finding alternative sources of social support (e.g., friends, romantic partners) are strategies that LGBTQ people may employ to lessen the impact of adverse experiences (Matsuno and Israel 2018; Meyer 2015).
This study is not without limitations. First, due to the small sample size, our findings may not show the complete picture of the patterns of adverse communication around family discussions of mental health, family violence, and LGBTQ identities for LGBTQ people. There is some degree of self-selection bias that is unavoidable when examining the experiences of LGBTQ people such that those recruited are more open about their minority identities. Therefore, we may be missing the experiences of the those who are most marginalized by their families and who are unable to express their identities as openly. Moreover, our sample is a Texas-based sample of LGBTQ people and may not be as generalizable to other LGBTQ populations. Texas is one of the Bible Belt states (i.e., socially conservative) and its population tends to have less favorable views of non-heteronormative behaviors and identities than other more liberal states. (Barton 2012) While regional influences likely play a role in shaping courtesy stigma, our findings suggest that cultural dynamics related to race/ethnicity and gender (i.e., heteronormative expectations) may play more significant roles in shaping how families experience courtesy stigma.
This study has several strengths as well. Our data were drawn from a qualitative study that used a CBPR approach, ensuring the CAB was consulted at each stage of data collection. The CBPR approach emphasizes power sharing among stakeholders and is particularly useful for reaching marginalized communities (i.e., people of color, lower income households) who may have distrust toward academic researchers for understandable reasons (Israel et al. 2010). As such we were able to recruit a diverse sample with regards to race/ethnicity, sexual identity, and gender identity. To date, research on LGBTQ populations has typically focused on White cisgender gay men. Many scholars have long called for an intersectional approach to studying the experiences of LGBTQ populations, examining experiences at the intersections of gender diverse identity and racial/ethnic minority identity. And finally, our objective was to explore subjective views of adverse communication from concrete experiences of sexual minority people who experienced trauma and mental illness. The qualitative approach afforded us a view of adverse communication (and broader family dynamics) informed by family member interactions described by interviewees. In addition, generating a typology of adverse communication experiences from verbal statements illustrates interviewees’ understanding of their family’s motivation (i.e., avoiding courtesy stigma) for engaging in adverse communication.
Our findings are an important contribution to understanding family dynamics and communication practices in the lives of LGBTQ people, particularly at the intersections of multiple marginalized identities. The findings suggest that for LGBTQ people—who are disproportionately more likely to report experiences ACEs—perceived adverse communication in response to discussions of mental health, family violence, and LGBTQ identities may contribute to the enduring psychosocial effects of trauma for this population. However, despite the adverse experiences reported in this sample, most of our interviewees demonstrated the development of coping strategies. Therefore, mental health professionals may interpret our findingsas a call to focus on promoting adaptive coping mechanisms in the absence of healthy family relationships.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was completed with research support from Rosie Davis, Monty McKeon, Katie Sibley, Charlotte Georgiou, and Samsara Davalos-Reyes and funding from the Robert Wood Johnson Foundation Interdisciplinary Research Leaders program.