
Abstract
Young adults in the United States have the highest prevalence of suicidal thoughts of any adult age group. While limited, research indicates food insecurity heightens the risk of suicide ideation among young adults. However, research has not explored the pathways underlying the food insecurity—suicide ideation association among this population. Using 2008 data from Wave IV of the National Longitudinal Study of Adolescent to Adult Health (Add Health), we fill this gap by testing for the mediating roles of perceived stress and social isolation in the association between the risk for food insecurity and suicide ideation among young adults ages 24–32 (N = 14,897). Our findings reveal that perceived stress and social isolation account for almost half of this association. Given the eradication of food insecurity in the United States is unlikely imminent, our results indicate an exigent need for interventions and programs to address psychosocial risk factors associated with food insecurity.
Introduction
Suicide is currently the third leading cause of death among adults between the ages of 25 and 44 in the United States (Heron 2021). In the past two decades, suicide rates have risen by 44 percent among this age group (Centers for Disease Control and Prevention, National Center for Health Statistics 2022). As of 2015–2019, young adults between the ages of 18 and 39 have the highest prevalence of suicidal thoughts, plans, and attempts out of any adult age group (Ivey-Stephenson et al. 2022). Given that suicide is a leading preventable cause of premature mortality among young people, identification of factors that contribute to suicidal thoughts and behaviors is imperative for suicide prevention and intervention efforts among this population.
Food insecurity, defined as limited access to adequate food for active and healthy living due to insufficient material resources, is a critical component of economic hardship linked with important psychological and behavioral outcomes (Gunderson and Ziliak 2015; Myers 2020). Food insecurity is broader than the physical sensation of hunger and encompasses issues associated with accessing food in socially acceptable ways, limited variety of dietary choices, and anxiety about food resources potentially running out. Food insecurity is also related to but empirically and conceptually distinct from other indicators of economic hardship as evidenced by research findings indicating that not all households with incomes below the poverty line experience food insecurity (Chang, Chatterjee, and Kim 2014).
Recently, food insecurity has been increasingly recognized as an overlooked risk factor for suicidal thoughts and behaviors among adolescents (Alaimo, Olson, and Frongillo 2002; Brinkman et al. 2021; Koyanagi et al. 2019) and adults (Davison, Marshall-Fabien, and Tecson 2015; Kamdar et al. 2021; Men, Elgar, and Tarasuk 2021; Nagata et al. 2019b; Pryor et al. 2016). However, there is a paucity of scholarship on food insecurity and suicide ideation among young adults, and the research that does exist has been largely limited to nonrepresentative samples (Men, Elgar, and Tarasuk 2021; Pryor et al. 2016). To our knowledge, only one study to date has considered the association between food insecurity and suicide ideation among a nationally representative sample of young adults in the United States (Nagata et al. 2019b). Specifically, using data from Wave IV of the National Longitudinal Study of Adolescent to Adult Health (Add Health), Nagata and colleagues (2019b) found that food-insecure individuals had significantly higher odds of suicide ideation relative to their food-secure counterparts (adjusted odds ratio [AOR] 3.34 vs. 2.76, p < .001). Furthermore, despite the proposed pathways of poorer nutritional intake (Davison, Gondara, and Kaplan 2017; Leung et al. 2014), stress exposure (Ciciurkaite and Brown 2022; Koyanagi et al. 2019; Nagata et al. 2019b; Pryor et al. 2016), social isolation (Nagata et al. 2019b), and stigmatization (Palar et al. 2018) linking food insecurity with adverse physical and mental health outcomes in adult populations, little is known about the mechanisms linking food insecurity and suicide ideation among young adults.
To address this gap, our study builds on and extends extant scholarship by assessing the contribution of two potential pathways—perceived stress and social isolation—underlying this association. Both factors have been established as correlates of food insecurity (Bruening, Dinour, and Chavez 2017; Bruening et al. 2018; Diamond, Stebleton, and delMas 2020; Whittle et al. 2019; Wolfson, Garcia, and Leung 2021) and predictors of suicide ideation (Calati et al. 2019; Chen and Kuo 2020; Cole et al. 2015; King and Merchant 2008; Trout 1980; Wilcox et al. 2010; Xu et al. 2022) in cross-sectional and longitudinal analyses, alike. To test these considerations, we build directly upon Nagata et al.’s (2019b) study by using 2008 Wave IV data from the National Longitudinal Study of Adolescent to Adult Health (Add Health) to examine the extent to which the risk for food insecurity is associated with an increase in perceived stress and social isolation, thereby increasing the likelihood of suicidal ideation among a nationally representative sample of young adults between the ages of 24 and 32.
Background
Young Adulthood and the Risk for Food Insecurity
Young adulthood is a unique phase during the life course typified by significant life transitions such as leaving the family home, entering into tertiary education, entering into employment, and forming unions and households through cohabitation, marriage, and/or parenthood (Arnett 2019; Wood et al. 2018). During this phase of the life course, most young adults are shifting into a state of self-sufficiency (Gooding, Walls, and Richmond 2012) and are no longer bound to their parents (Arnett 2019), including their protective resources such as economic security, which subsequently can have implications for increased risk for food insecurity. Furthermore, young adults may be particularly vulnerable to experiencing food insecurity due to their educational transitions, employment uncertainty, and economic instability (Maia et al. 2019; Nagata et al. 2021).
The Great Recession had especially pernicious economic consequences for young adults in the United States (Manning 2020). For example, in 2009, a greater portion of young adults between the ages of 18 and 34 were living in poverty than the national average (Settersten 2012). Unsurprisingly, 2007–2014 data from the National Health and Nutrition Examination Survey (NHANES) indicated that among adults aged 20 and older with an income-to-poverty ratio of less than 3, those with marginal, low, and very low food security were significantly more likely to be between the ages of 20 and 39 than 40 or older (Bergmans et al. 2018). Furthermore, more recent estimates from a population-based sample suggest that because of educational and economic transitions, close to a quarter of young adults experience food insecurity, higher than the national average (Larson, Laska, and Neumark-Sztainer 2020). Given the well-established association between food insecurity and poor health, we can appreciate that young adulthood may be a particularly challenging life course phase when it comes to consistent and socially acceptable ways to accessing a well-balanced diet and its associated health outcomes. In the following sections, we propose and outline the theoretical underpinnings linking food insecurity to suicide ideation among young adults with the focus on the pathways of perceived stress and social isolation.
The Mediating Role of Social Stress
Stressful life experiences can be traced back to an individual’s place within social systems of stratification that cut across social and economic class, race and ethnicity, age, and gender lines (Pearlin 1989). Positionality within these systems of stratification predicts how much stressful stimuli individuals experience, which subsequently affects health outcomes (Pearlin 1989). For example, economic hardship, including the limited ability to acquire basic levels of goods and services, such as food, housing, and health care, is a consequence of the unequally distributed resources and opportunities across social statuses and one of the most critical sources of chronic stress that has been linked with depressive symptomology, anxiety, and other mood disorders (Chai, Schieman, and Bierman 2021; Kahn and Pearlin 2006; Mirowsky and Ross 2001; Ross and Hill 2013; Williams and Cheadle 2016). Unsurprisingly, unequal exposure to chronic stressors such as economic hardship is a significant source of mental and physical health disparities (Turner 2013).
Food insecurity, as previously noted, is one of the key dimensions of economic hardship and a chronic stressor (Laraia, Vinikoor-Imler, and Siega-Riz 2015; López-Cepero et al. 2020; Nagata et al. 2019b; Ross and Hill 2013). Different dimensions of hardship may vary in their prevalence and severity, however, the persistence of one form of chronic life strain may lead to the co-occurrence of a different form of chronic strain, a phenomenon known as stress proliferation (Pearlin 1989). Further, prior or concurrent stressful life experiences might also make the resolution of chronic life strains more difficult (Brown, Richman, and Rospenda 2017). As an illustration, more economically disadvantaged groups experienced greater financial shock relative to their more economically advantaged counterparts during the Great Recession, and also faced greater recovery difficulties due to institutional constraints imposed on those with fewer financial assets (Brown et al. 2019; Burgard and Kalousova 2015). Thus, there are grounds to anticipate that individuals who struggle with meeting their nutritional needs may also report greater perception of stress in other domains of daily life.
Unsurprisingly, a large body of quantitative research has documented a robust association between food insecurity and increased perceived stress (Bruening et al. 2017, 2018; Coffino et al. 2021; Laraia et al. 2015; López-Cepero et al. 2020; Martin et al. 2016; Whittle et al. 2019; Wolfson et al. 2021), as well as uncertainty, worry, and anxiety, which can stimulate stress responses (Maynard et al. 2018; Pourmotabbed et al. 2020; Wolfson et al. 2021). Worry about having enough food to eat in the future may be an especially salient contributor to stress as it is largely a preoccupation with survival (Hamelin, Beaudry, and Habicht 2002). Indeed, prolonged struggles with accessing food have been described by informants in qualitative research as “depressing” and “frustrating” at once, and worry, fear, and anxiety were listed as some of the most common psychological states (Knowles et al. 2016).
Suicide is considered a stress-induced pathology in which the precursor to suicide is often profoundly stressful life experiences (Rubinstein 1986). Indeed, life stress is a predominant component of major etiological theories of suicide (Liu and Miller 2014; Stewart et al. 2019). Considering that life stressors serve as a function for the development of suicidality, a positive association between various life stressors and suicide ideation (Cole et al. 2015; Dixon, Heppner, and Anderson 1991; Lin et al. 2020; Liu and Miller 2014; Vilhjalmsson, Kristjansdottir, and Sveinbjarnardottir 1998), suicide attempts (Liu and Miller 2014), and suicide mortality (Feskanich et al. 2002) has been observed by a number of scholars. Furthermore, stressful experiences, such as worry about access to adequate food, can augment perception of stress which subsequently may increase the vulnerability to experiencing poorer mental health outcomes, such as suicide ideation (Martin et al. 2016).
Stress mechanisms have been proposed to account for the observed food insecurity—poor mental health association in adult samples, including suicide ideation (Ciciurkaite and Brown 2022; Davison et al. 2015). For instance, Davison et al. (2015) note that stress from worry about not having enough money for food may contribute to maladaptive psychological responses, such as impaired concentration and decision-making, which may in turn lead to suicidal ideation. There is also support for considering ongoing difficulties, such as persistent food insecurity, as pernicious risk factors for suicidal ideation due to the concomitant chronic stress. As chronic stress can be overtaxing, people experiencing chronic strains may become overwhelmed, despondent, lose hope, and feel nothing is worthwhile anymore—antecedents to suicidal thoughts (Bryan et al. 2015; Vilhjalmsson, Kristjansdottir, and Sveinbjarnardottir 1998). Given these considerations, we anticipate that being at risk for food insecurity will lead to increased perception of stress, which in turn will augment the risk of experiencing suicide ideation.
The Mediating Role of Social Isolation
In addition, extant evidence indicates that food insecurity may contribute to social alienation, lack of social acceptance, and social withdrawal (Hamelin, Beaudry, and Habicht 2002; Pineau et al. 2021; Pryor et al. 2016), and a number of studies have considered the factors that may either unilaterally increase the sense of social isolation or compound to produce feelings of social isolation. First, food-insecure individuals may feel forced to forgo participating in social activities that entail financial costs associated with food, such as celebrations in which individuals are expected to bring or provide food (Meijs et al. 2020; Purdam, Garratt, and Esmail 2016; Stewart et al. 2009). Thus, food-insecure individuals may be limited in their ability to visit with friends and family, attend social events, have guests over, and celebrate special occasions which contributes to feelings of social exclusion, isolation, and lack of meaningful social relationships (Meijs et al. 2020; Meza et al. 2019; Purdam et al. 2016; Runnels, Kristjansson, and Calhoun 2011). Second, food-insecure individuals may experience guilt and worry about having to rely on others for access to food through avenues such as community food programs, which may contribute to feelings of social difference and isolation (Martin et al. 2016). Third, food-insecure individuals may be subjected to shame from others due to the inability to provide for themselves and/or their families (Gucciardi et al. 2014), leading to social withdrawal and its concomitant feelings of alienation and/or social isolation (Pineau et al. 2021; Purdam et al. 2016).
Finally, food-insecure individuals may experience feelings of social isolation because of their stigmatized status (Pineau et al. 2021; Swales et al. 2020; Wu and Schimmele 2006). As an example, food-insecure individuals are often portrayed as lazy, uneducated, or uncaring of their health (Pineau et al. 2021; Swales et al. 2020). Stigmatized individuals may be devalued, rejected, and excluded based on characteristics deemed as undesirable (Link and Phelan 2001) and, consequently, stigma can constrain social interactions (Power, Little, and Collins 2015). More explicitly, stigma can lead to feelings of social isolation as individuals with concealable stigmas (i.e., food-insecure individuals) may avoid social interactions and close social relationships out of fear that others will uncover their stigmatized attributes and reject or exclude them (Hatzenbuehler, Phelan, and Link 2013). For example, research suggests that food-insecure individuals often hide their food situations from family, friends, and neighbors to avoid experiencing food insecurity–related stigma (Wu and Schimmele 2006) which may subsequently contribute to feelings of social isolation.
Social isolation is arguably the most well-documented social contributor to suicidality dating back to the origins of the sociology of suicide. In his seminal work on suicide, Durkheim ([1897] 1951) ascertained a connection between social isolation and “egoistic” suicide, and his theory still serves as the foundation for research on social disconnectedness and suicide. A robust body of literature indicates that facets of social isolation such as dissonant social relationships (Bearman and Moody 2004), limited social interactions (Beautrais 2002; Calati et al. 2019; Trout 1980), lack of social ties (Hall-Lande et al. 2007; Trout 1980), and lack of social support (Endo et al. 2017; Hall-Lande et al. 2007; Hernandez et al. 2021; Heuser and Howe 2019) contribute to suicidality and suicide mortality. Given that food insecurity can lead to feelings of social isolation and the clear indication that social isolation is a risk factor for suicidal thoughts, we anticipate that perceived social isolation will mediate the association between the risk for food insecurity and suicide ideation.
Present Study
In summary, previous research findings provide grounds for anticipating that greater perceived stress and increased perception of social isolation may substantially account for the risk for food insecurity—suicide ideation association. Based upon prior research, the present study tests the following hypotheses among a nationally representative sample of young adults:
Hypothesis 1. The association, between the risk for food insecurity and suicide ideation will be mediated by greater levels of perceived stress.
Hypothesis 2. The association between the risk for food insecurity and suicide ideation will be mediated by increased perceived social isolation.
Methods
Data
Data were drawn from Wave IV of the National Longitudinal Study of Adolescent to Adult Health (Add Health). Add Health is a longitudinal study of adolescents in grades 7th–12th in 1994–1995 with four subsequent waves of data collected through 2016–2018. The first wave of data (Wave I) was collected from an original sample of 90,118 students from 145 middle, junior, and high schools with 20,745 of them selected to participate in the 1994–1995 in-home interview. The second wave of data (Wave II) was collected from 14,738 adolescents from the Wave I cohort in 1996 and excluded respondents who were in 12th grade or in the disabled sample in Wave I. Wave III data were collected in 2001–2002 when the respondents were emerging adults between the ages of 18 and 26 and included 15,197 respondents from the original Wave I cohort. Wave IV data were collected in 2008 when the respondents were young adults between the ages of 24–32 and included 15,701 respondents from the original Wave I cohort. The most recent wave of data (Wave V) was collected between 2016 and 2018 when respondents were between the ages of 33 and 43 and included 12,300 respondents from the original Wave I cohort.
For this study, we use data from Wave IV when respondents were between the ages of 24 and 32 (N = 15,701). We also use Wave I sociodemographic data such as race/ethnicity, sex, and nativity. We use listwise deletion to exclude respondents who were missing information on the dependent variable or any of the independent variables (N = 804). This results in approximately 5 percent of missing cases and our final analytic sample size is 14,897 young adults.
Measures
Summary statistics for study variables are presented in Table 1. The main outcome in this study is suicide ideation.
Descriptive Statistics (n = 14,897).
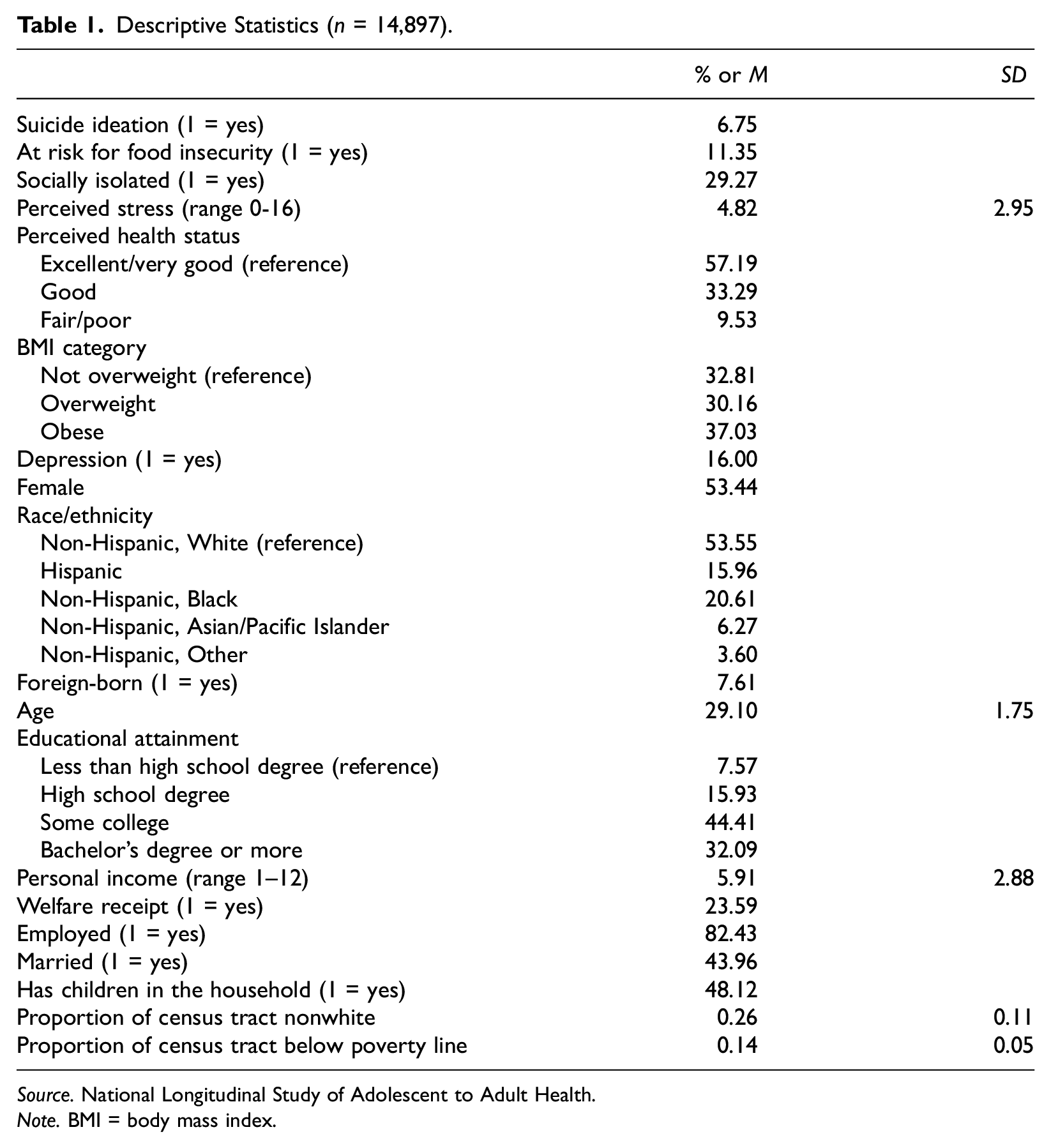
Source. National Longitudinal Study of Adolescent to Adult Health.
Note. BMI = body mass index.
Suicide ideation
Wave IV of Add Health asks the question, “During the past 12 months, did you ever seriously think about committing suicide?” Respondents who responded “no” were coded as 0 and respondents who responded “yes” were coded as 1.
Our focal independent variable is past-year risk for food insecurity, and mediator variables include perceived stress and social isolation.
Risk for food insecurity
Wave IV of Add Health asks, “In the past 12 months, was there a time when {YOU/YOUR HOUSEHOLD WERE/WAS} worried whether food would run out before you would get money to buy more?” Respondents who answered “no” were coded as 0 and respondents who answered “yes” were coded as 1. This dichotomous measure of the risk for food insecurity has an 85–87 percent specificity for determining food insecurity as defined by the 18-item U.S. Household Food Security Scale (Nagata et al. 2019b) and has been used in other studies examining the association between food insecurity and mental and physical health outcomes, as well as substance use (Nagata et al. 2019a, 2019b, 2019c, 2021).
Perceived stress
The perceived stress indicator was created from four items of the Perceived Stress Scale (PSS), a psychological instrument that measures perception of stress (Cohen, Kamarck, and Mermelstein 1983). Questions on the scale included: “In the past 30 days, how often have you felt that you were unable to control the important things in your life?”“In the past 30 days, how often have you felt confident in your ability to handle your personal problems?”“In the past 30 days, how often have you felt that things were going your way?”, and “In the past 30 days, how often have you felt that difficulties were piling up so high that you could not overcome them?” Responses included 0 = “never,” 1 = “almost never,” 2 = “sometimes,” 3 = “fairly often,” and 4 = “very often.” Questions 2 and 3 were reverse coded and responses to the four questions were summed to create a stress scale with a range of 0–16. We computed Cronbach’s alpha score and ran an exploratory factor analysis which indicated that the PSS variable has acceptable internal reliability (Cronbach’s alpha = .73) and validity (no factor loadings < 0.50).
Perceived social isolation
The measure for perceived social isolation is based on the question: “How often do you feel isolated from others?” Responses included “never,”“rarely,”“sometimes,” and “often.” A dichotomous measure was created by combining “never/rarely” and “sometimes/often” (1 = yes). Other studies have used this dichotomous measure of social isolation in Add Health (Carbonaro 2022).
We control for a number of physical and mental health, sociodemographic, and socioeconomic status indicators that could potentially confound the relationship between the risk for food insecurity and suicide ideation. Physical and mental health status indicators include perceived health status—“excellent/very good” (reference), “good,” and “fair/poor,”BMI category (“not overweight” (reference), “overweight,” and “obese”), and depression (1 = yes). We constructed BMI scores using Wave IV interviewer assessments of measured weight and height and created our BMI categories according to the Centers for Disease Control and Prevention (CDC) guidelines—“not overweight” (BMI < 25.0), “overweight” (25.0 ≤ BMI ≤ 29.9), and “obese” (BMI > 30.0). We created the depression variable based on a modified 10-item Center for Epidemiological Studies (CES-D) instrument that asks respondents questions such as “about how often in the past week they could not shake the blues” or “about how often in the past week they felt like they were not as good as others.” When response items were summed (range 0–30), higher scores were indicative of depression. In accordance with previous research, a score of 11 or greater (Frisco, Houle, and Lippert 2013) indicates depression (1 = yes).
Sociodemographic indicators include race/ethnicity as coded according to the Add Health guidelines—“non-Hispanic, White” (reference), “Hispanic,”“non-Hispanic, Black,”“non-Hispanic, Asian/Pacific Islander,” and “non-Hispanic, Other,”nativity (1 = foreign-born), sex (1 = female), and age (continuous, range 24–32). Socioeconomic status indicators include educational attainment (“less than high school degree” (reference), “high school degree,”“some college,” and “bachelor’s degree or more”), personal income, and welfare receipt (1 = yes). We chose to include personal income rather than household income in accordance with Nagata et al. (2019b). We also control for employment status (1 = employed), marital status (1 = married), presence of children in the household (1 = yes) and neighborhood racial and socioeconomic status composition (proportion of census tract nonwhite and proportion of census tract below the poverty line). Neighborhood poverty and racial/ethnic composition have been found to be associated with individual-level food insecurity (Kimbro, Denney, and Panchang 2012; Morrissey et al. 2016).
Analytic Strategy
First, we estimated the descriptive statistics for each of the study variables for the overall sample which help to contextualize our findings. Second, we computed the correlation matrix of our dependent variable, main independent variable, and mediators. Next, we used a generalized structural equation modeling (GSEM) approach to examine the extent to which the odds of suicide ideation were influenced by greater perceived stress and social isolation in the context of the risk for food insecurity. The GSEM approach is flexible in that it allows us to fit a logistic regression model with a binary outcome variable and a binary mediator. A preliminary association was first established between the risk for food insecurity and suicide ideation, adjusting for control variables. Then, the mediating variables of perceived stress and social isolation were added to the model.
To formally test for the significance of indirect effects, we used Stata program binary_mediation. The binary_mediation program allows for multiple mediators, both binary and continuous, in a nonlinear model. Furthermore, this program rescales (or standardizes) coefficients before computing indirect effects to account for the fixed residual variance in logistic regression and the changing residual variance in ordinary least squares (OLS) regression as variables are entered or removed from the regression equation. Coefficients from the OLS models are rescaled using the standard deviations of the observed variables and the coefficients from the logistic regression models are rescaled using the standard deviation of the underlying latent variable for the binary variables. Rescaling (or standardizing) the indirect effects allows us to also compute the total indirect effect using the product of the coefficients. We formally assessed the direct and indirect effects using a bootstrapping approach as outlined by Preacher and Hayes (2008) with 1,000 replications to compute standard errors and 95 percent confidence intervals. Finally, we estimated the proportion of the effect that was mediated (PME) by dividing the total indirect effect by the total effect (PME = a1b1+ a2b2/c) (Figure 1).
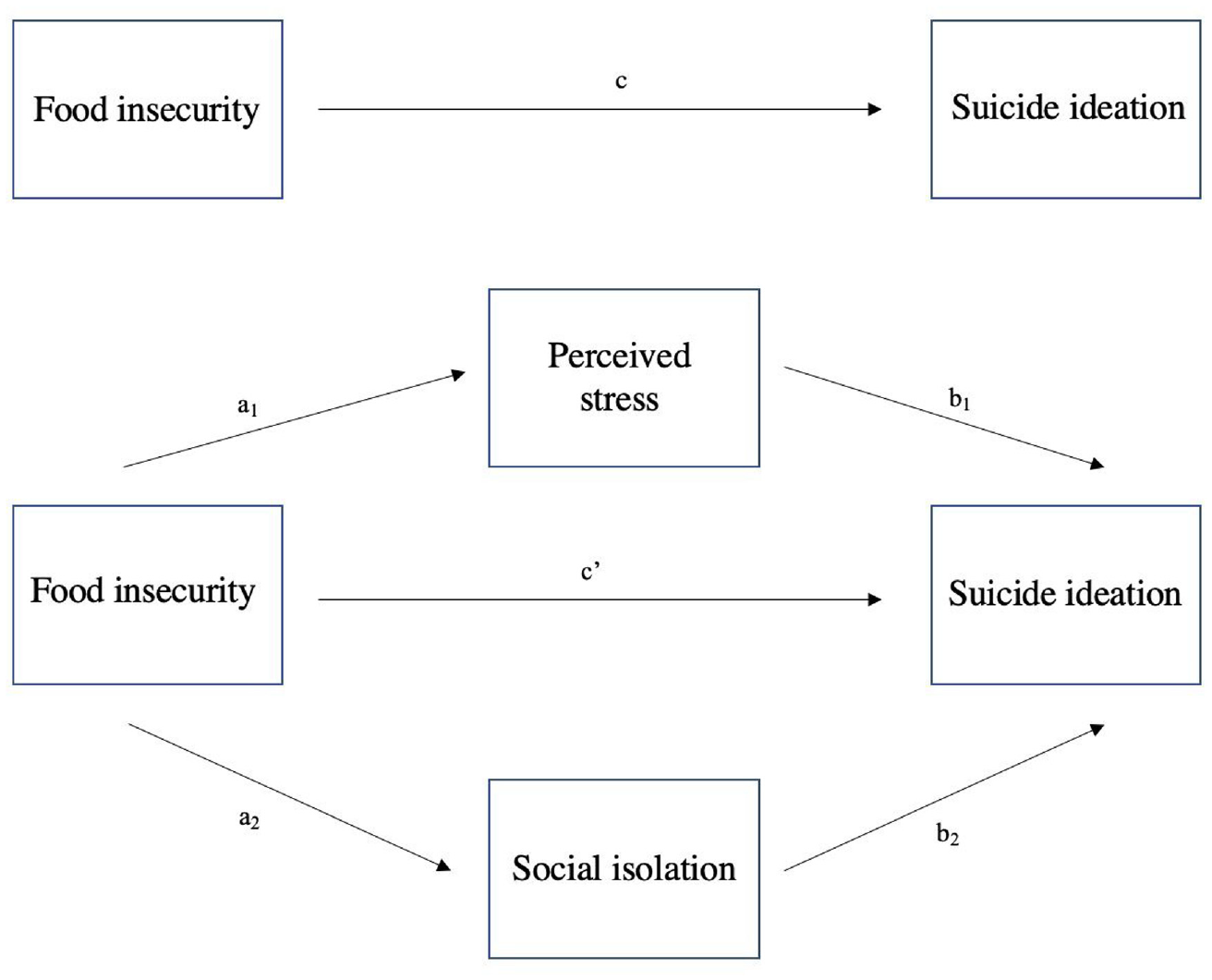
Hypothesized conceptual model of the direct effect (c′) of risk for food insecurity (food insecurity) on suicide ideation, the total indirect effect (a1b1+ a2b2) of risk for food insecurity on suicide ideation through the proposed mediators and total effect (c = c′+ a1b1+ a2b2).
Results
Descriptive statistics of the main study variables are presented in Table 1. Suicide ideation was relatively rare in our sample as less than 7 percent of young adults indicated they had experienced suicide ideation in the past 12 months. Furthermore, about 11 percent of the respondents indicated they were at risk for food insecurity at some point in the past 12 months, and about a third of the sample (29.3 percent) reported feeling socially isolated “sometimes” or “often.” The average perceived stress score was 4.8 with a range of 0–16. Of note, the largest proportion of respondents had a highest educational attainment level of some college, 82.4 percent were employed, and less than half were married and/or had children in the household. Finally, close to a quarter of respondents were welfare recipients.
Table 2 presents the correlations between suicide ideation, the risk for food insecurity, perceived stress, and social isolation, all of which are significant at the p < .001 level. Each of the constructs are weakly and positively correlated.
Correlation Matrix for Dependent, Main Independent, and Mediator Variables.
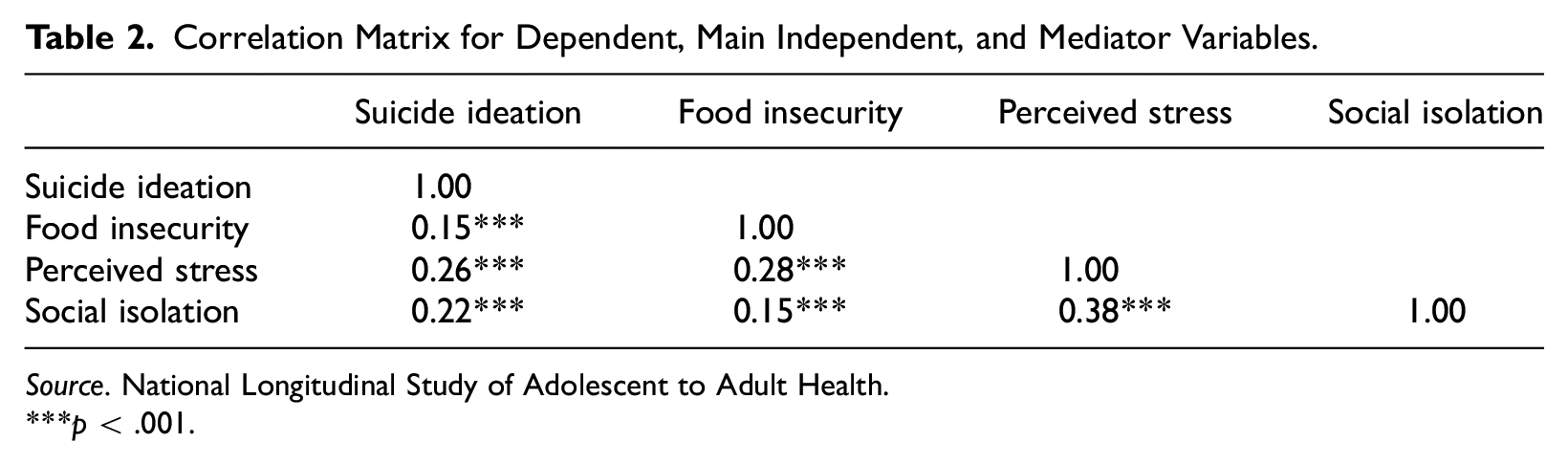
Source. National Longitudinal Study of Adolescent to Adult Health.
p < .001.
Figure 2 displays the results of the preliminary association between the risk for food insecurity and suicide ideation, adjusted for the control variables. The significant path coefficient demonstrates that being at risk for food insecurity is associated with greater log odds of suicide ideation (β = 0.66, SE = 0.09). With the addition of perceived stress and social isolation, the coefficient for the path from the risk for food insecurity to suicide ideation is attenuated in magnitude but remains significant (β = 0.40, SE = 0.09) (Figure 3). As displayed in Figure 3, being at risk for food insecurity is significantly associated with increased levels of perceived stress (β = 1.33, SE = 0.07) and increased log odds of perceived social isolation (β = 0.49, SE = 0.06). Furthermore, greater perceived stress is significantly associated with increased log odds of suicide ideation (β = 0.18, SE = 0.01) and perceived social isolation is significantly associated with increased log odds of suicide ideation (β = 0.88, SE = 0.08). Table 1 in the appendix displays the detailed pathway regression models which include the coefficients from our control variables.

Structural equation model of the preliminary association between risk for food insecurity (food insecurity) and suicide ideation without mediators (unstandardized coefficient) (n = 14,897).
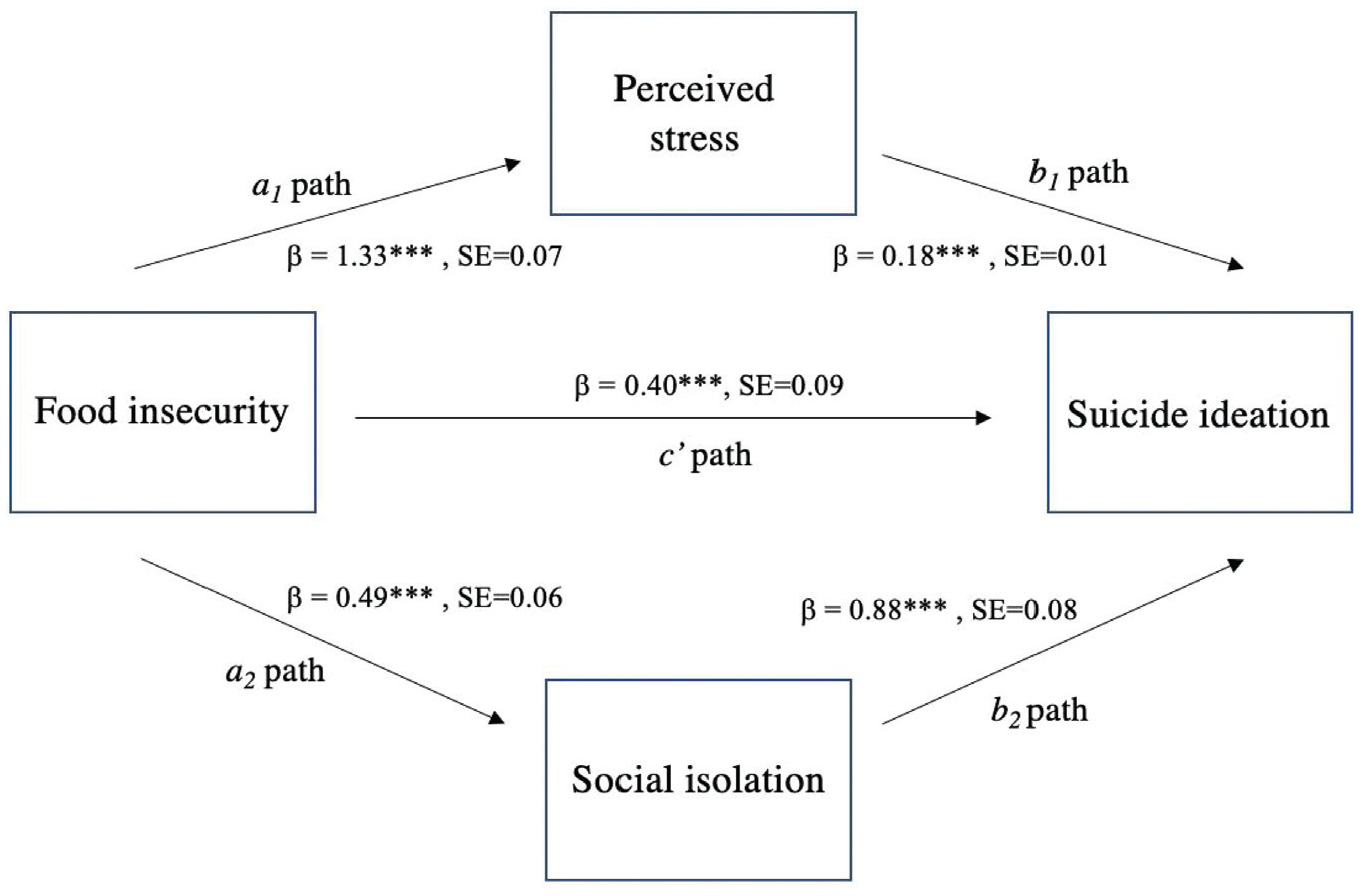
Structural equation model of the association between risk for food insecurity (food insecurity) and suicide ideation through perceived stress and social isolation (unstandardized coefficients) (n = 14,897).
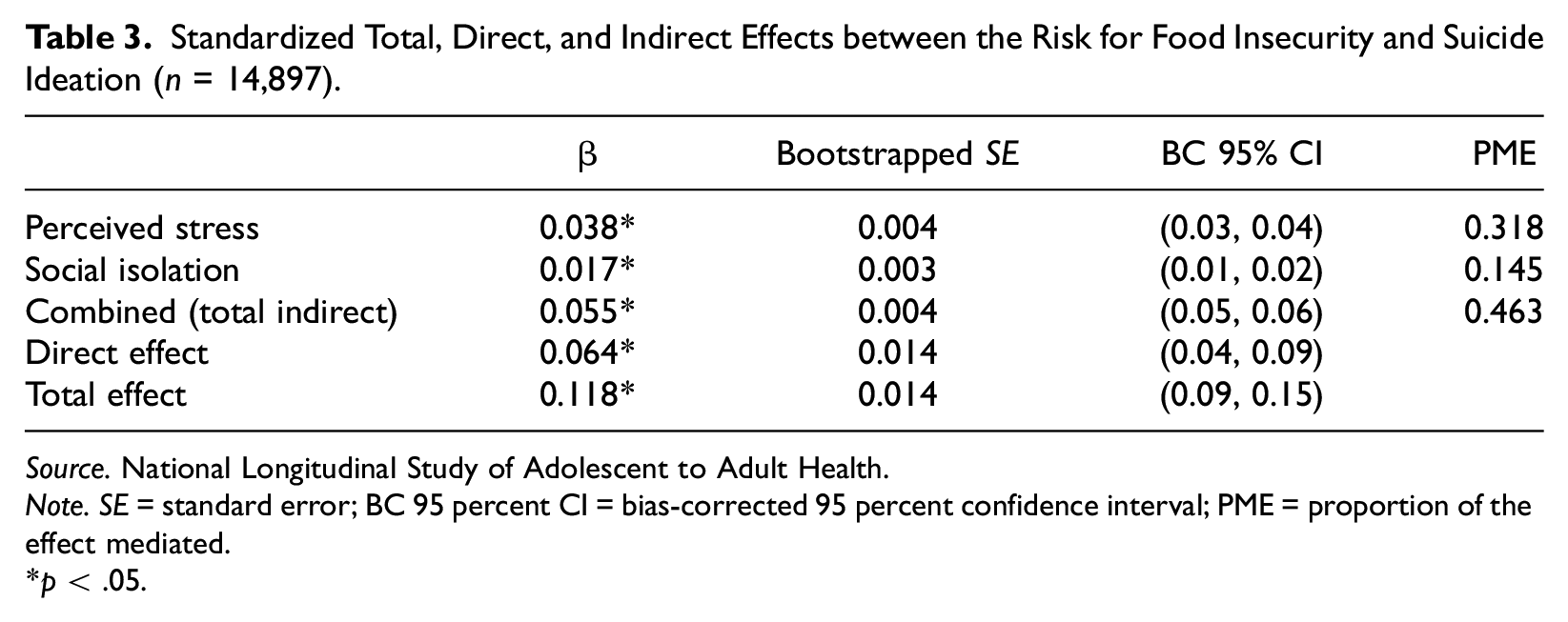
The standardized coefficients of the indirect effect of each mediator and the combined (total) indirect effect along with the bootstrapped standard errors, the bias-corrected 95 percent confidence intervals, and the proportion of the effect mediated (PME) are displayed in Table 3. As shown, both perceived stress and social isolation have significant indirect effects on suicide ideation, although perceived stress has a larger indirect effect (β = 0.038, SE=0.004) than perceived social isolation (β = 0.017, SE = 0.003). The PMEs indicate that 14.5 percent of the total effect is mediated by perceived social isolation and 31.8 percent of the total effect is mediated by perceived stress. Subsequently, the total indirect effect (β = 0.055, SE = 0.004) indicates that 46.3 percent of the total effect is mediated by perceived social isolation and perceived stress.
Standardized Total, Direct, and Indirect Effects between the Risk for Food Insecurity and Suicide Ideation (n = 14,897).
Source. National Longitudinal Study of Adolescent to Adult Health.
Note. SE = standard error; BC 95 percent CI = bias-corrected 95 percent confidence interval; PME = proportion of the effect mediated.
p < .05.
Sensitivity Analyses
We also ran several sensitivity analyses (available upon request). First, because SEM with categorical variables does not accommodate survey weights, we ran a series of ordinary logistic regressions with and without Add Health Wave IV survey weights as a sensitivity analysis. Our results confirmed (1) the association between the risk for food insecurity and suicide ideation persists net of our control variables and (2) there is a significant association between the risk for food insecurity and each of our mediators net of our control variables with and without survey weights in the analyses. Results from regressions with and without survey weights were substantively similar.
Second, we ran our models with the inclusion of household income as a control variable to determine whether household income confounds the relationships between the risk for food insecurity and suicide ideation, perceived stress, and perceived social isolation. Including the household income measure did not affect our results. Finally, we ran our models using the KHB-method (Breen, Karlson, and Holm 2013) which allows for the decomposition of the total effect in logit models into direct and indirect effects. The PME of the indirect effects and ratio of the total effect to direct effect from the KHB method were comparable to our results using binary_mediation (PME difference of 1.5 percent and ratio of the total effect to direct effect difference of 0.05).
Discussion
The main goal of our study was to extend the line of the food insecurity—suicide ideation scholarship by considering the role of two potential pathways underlying this association in a nationally representative sample of young adults. Specifically, using data from Wave IV of the National Longitudinal Study of Adolescent to Adult Health (Add Health), we build directly on Nagata and colleagues’ (2019b) work and consider the possibility that being at risk for food insecurity will lead to greater perceived stress and social isolation, thereby increasing the risk for suicide ideation.
Confirming results from Nagata et al. (2019b), baseline analyses revealed that being at risk for food insecurity was significantly associated with increased odds of experiencing suicide ideation, net of control variables. Furthermore, supporting Hypotheses 1 and 2, we found that being at risk for food insecurity was associated with increases in perceived stress and social isolation which in turn influenced the increase in the odds of suicide ideation. In fact, formal mediation analyses revealed that perceived stress accounted for 31.8 percent and perceived social isolation accounted for 14.5 percent of the indirect effect of suicide ideation. Previous scholars have speculated that stress exposure and social isolation may underlie the association between food insecurity and suicide ideation (Koyanagi et al. 2019; Nagata et al. 2019b; Pryor et al. 2016) and our study is the first, to our knowledge, to explicitly test and confirm this.
Overall, our study adds to the growing scholarship demonstrating the detrimental mental and behavioral health effects associated with food insecurity. While cross-sectional and longitudinal studies have documented that food insecurity is a strong risk factor for depressive symptoms or incidence of a major depressive episode (Heflin, Siefert, and Williams 2005; Siefert et al. 2004; Whitaker, Phillips, and Orzol 2006), anxiety, and sleep disorders (Arenas et al. 2019), as well as increased substance use (Ciciurkaite and Brown 2017; Nagata et al. 2021; Pryor et al. 2016), risk for suicidality has received less scholarly attention (Alaimo et al. 2002; Brinkman et al. 2021; Davison et al. 2015; Kamdar et al. 2021; Koyanagi et al. 2019; Men, Elgar, and Tarasuk 2021; Nagata et al. 2019b; Pryor et al. 2016). Notably, scholarship that has considered suicide ideation or attempts as outcomes has primarily focused on either adult or adolescent samples. Young adulthood is a unique developmental period when individuals are no longer shielded from hardships and stressors by their parents and are transitioning toward economic independence (Gooding, Walls, and Richmond 2012). Data from the U.S. Census Bureau show that 41 percent of those aged 18–34 have student debt and about a third of them live at home (Vespa 2017). Given the socioeconomic vulnerability associated with young adulthood, further consideration of food insecurity as a salient source of stress and poor mental health outcomes for this age group is warranted.
Furthermore, our finding that perceived stress relative to perceived social isolation mediates a larger proportion of the total effect between the risk for food insecurity and suicide ideation is noteworthy, yet unsurprising. Previous research has shown that food insecurity as a chronic strain tends to co-occur with other stressors, a process also known as stress proliferation (Pearlin 1989). As an example, qualitative researchers have shown that the inability to meet food needs often co-occurs with difficulties paying rent and utilities, clothing children, or obtaining necessary medical care (Knowles et al. 2016; Mirowsky and Ross 1992). In addition, food-insecure individuals are more likely to experience loss of a family member or a close friend, serious illness, alcohol or drug-related problems, violence, bullying, harassment, and trouble with the police, relative to their food-secure counterparts (Temple 2018; Tolman and Rosen 2001). Furthermore, findings that suggest food insecurity co-occurs with other chronic strains and stressful life events also emphasize the need to consider psychosocial resources, such as mastery or self-esteem, and their role in helping individuals manage stressful experiences. We are encouraged by Wu and Schimmele’s (2006) work demonstrating that social support serves as a buffer from depressive symptoms among food-insecure individuals, and we recommend that research examine the role of other psychosocial coping mechanisms for the food insecurity—suicide ideation association.
Another extension of our research findings may be the consideration of gender differences in this association. Specifically, previous research has documented a stronger food insecurity—depressive symptomology association among women relative to men (Carter et al. 2011; Ciciurkaite and Brown 2017). Women are more often subjected to “role overload” than men due in large part to gendered expectations of women as the predominant care providers of children, spouses, parents, and other family members, and managers of household duties (Martin and Lippert 2012; Moen and Chermack 2005). As such, “feeding the family” largely falls on women, including tasks such as cooking, shopping, and monitoring food supplies (DeVault 1991; Martin and Lippert 2012), and it is reasonable to anticipate that the stress associated with the inability to adequately feed the family (and worry for their family members’ survival) would be especially pronounced among women (Yan 2022), which could manifest in adverse mental health, such as depression and suicidal thoughts. According to role strain theory, mothers may be particularly vulnerable to stress and the concomitant potential for adverse mental health due to the diminished capacity to fulfill their socially prescribed role demand of sufficiently meeting the needs of their children (Yan 2022). Furthermore, research suggests that the normative expectations among women as the primary family caregivers lead women to prioritize their family members’ nutritional needs over their own by reducing their meal sizes or depriving themselves of food altogether to make sure that their children have enough food (DeVault 1991; Olson 2005). However, it is unclear whether the expectations and challenges associated with the mother and wife roles in food-insecure households are also salient sources of suicidal thoughts in young adulthood specifically, and we recommend a more thorough examination of this possibility in future research.
Our study is not without limitations. First, although Add Health uses a longitudinal data collection design, we were only able to use one wave of data given the availability of the risk for food insecurity measure only in Wave IV. As such, we cannot speak to causality between risk for food insecurity and suicide ideation. We are aware that mental health and behavioral problems may compromise socioeconomic well-being, therefore, there is potential for a bidirectional relationship between the factors considered in our study. Given the availability of data, future research could employ a longitudinal analysis to better understand the causal relationship of the mediating roles of stress and social isolation between food insecurity and suicidality. Second, our risk for food insecurity measure is a simple dichotomous measure and does not capture discrete categories of food insecurity, limiting our conclusions regarding the variation in severity of food insecurity and its effect on suicide ideation. If available, more extensive measures such as the validated U.S. Department of Agriculture’s (USDA) 18-item questionnaire (Jilcott et al. 2011) should be used in future research. Of note, we examined the results from the same single-item indicator using the 2008 Current Population Survey: Food Security Supplement (CPS-FSS) data and found approximately 10 percent of young adults aged 24–32 answered they “often” worried about food running out before they had money to buy more, and 7.5 percent qualified as having “marginal food security.” These national estimates are largely consistent with our finding that about 11 percent of young adults responded positively to the question about worrying that food would run out; however, we would like to encourage future researchers to replicate our study using alternative data and measurement sources. Third, the perceived social isolation and stress measures used in our study are subjective in nature, and the use of more objective measures, such as the Lubben Social Network Scale (Gray et al. 2016) and physiological stress indicators (Sharma and Gedeon 2012), could further elucidate the salience of observed associations and strengthen scholarship in this area. Finally, our data are from 2008. In the past two decades, the prevalence of food insecurity peaked between 2008 and 2011 and has since declined (Economic Research Service, USDA 2021). Rates of food insecurity did increase in the early months of the COVID-19 pandemic (Karpman et al. 2020); however, year-trend data indicate that rates of food insecurity eventually returned to pre-pandemic levels by the end of 2020 (Coleman-Jensen et al. 2021). While this decline is attributed to the government’s emergency response through expansion of nutritional assistance programs, unemployment benefits, and stimulus payments to eligible individuals, it is not clear the extent to which young adults were able to benefit from this reversal, and access to the latest data could address this issue.
Limitations notwithstanding, our study provides a novel contribution to the body of literature on the relationship between food insecurity and suicidal thoughts and behaviors by considering the mediating roles of perceived stress and social isolation. Our findings reveal that being at risk for food insecurity is associated with heightened perceived stress and social isolation, which in turn contribute to the increased likelihood of experiencing suicide ideation. Unequivocally, foremost, our research underscores the exigent need to implement policies and initiatives aiming to reduce food insecurity in the United States and its associated mental health burden in young adulthood. For example, food insecurity decreased among low-income households following the increase in Supplemental Nutrition Assistance Program (SNAP) benefits implemented by the American Recovery and Reinvestment Act (ARRA of 2009; Nord and Prell 2011), which yields promise that federal initiatives can help to reduce food insecurity. However, it would be naïve to assume that the eradication of food insecurity in the United States is imminent. In the meantime, our results further suggest a need to address psychosocial risk factors associated with food insecurity to help alleviate the mental health burden among food-insecure individuals, such as alternative programs and interventions specifically focused on social inclusion and community participation (Martin et al. 2013). Overall, our study marks a step toward a better understanding of the potential mechanisms linking food insecurity with suicidality, and we encourage researchers to continue examining the health and behavioral effects of food insecurity as a unique dimension of adversity for the young adult population in the United States.
Supplemental Material
sj-docx-1-smh-10.1177_21568693221120066 – Supplemental material for The Risk for Food Insecurity and Suicide Ideation among Young Adults in the United States: The Mediating Roles of Perceived Stress and Social Isolation
Supplemental material, sj-docx-1-smh-10.1177_21568693221120066 for The Risk for Food Insecurity and Suicide Ideation among Young Adults in the United States: The Mediating Roles of Perceived Stress and Social Isolation by Carlyn Graham and Gabriele Ciciurkaite in Society and Mental Health
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors of the study acknowledge assistance provided by the Population Research Institute at Penn State University, which is supported by an infrastructure grant by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (P2CHD041025). This study uses data from Add Health, which is directed by Robert A. Hummer and funded by the National Institute on Aging cooperative agreements U01 AG071448 (Hummer) and U01AG071450 (Aiello and Hummer) at the University of North Carolina at Chapel Hill. Waves I-V data are from the Add Health Program Project, grant P01 HD31921 (Harris) from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), with cooperative funding from 23 other federal agencies and foundations. Add Health was designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.