
Abstract
The purpose of the study was to assess the health-related quality of life and treatment satisfaction of diabetes patients (n = 36) with foot ulcers undergoing insulin and ayurvedic adjunct therapy. Retrospective hospital based cross-sectional design considered patients with diabetes foot ulcers undergoing 4-week treatment with insulin and ayurvedic combinatorial therapy. The Audit of Diabetes Dependent Quality of Life Questionnaire and Diabetes Treatment Satisfaction Questionnaire were completed for the assessment. The mean duration of diabetes among participants was 9.32 ± 5.3 years. Assessment of Diabetes Treatment Satisfaction Questionnaire (total treatment satisfaction) score was found to be 26.0139 ± 5.20369, and Audit of Diabetes Dependent Quality of Life Questionnaire (average weighted impact) score was −3.0819 ± 1.83003. Relationship with diabetes complications showed that Audit of Diabetes Dependent Quality of Life Questionnaire score (P = .383) had no relationship, but Diabetes Treatment Satisfaction Questionnaire score (P = .039) showed significance. Integrated approaches for diabetes foot ulcer management with insulin and ayurvedic management have a favorable impact on patient-perceived quality of life.
Introduction
Diabetes epidemic is the major cause of morbidity and mortality globally, which is burdened with an increased risk of complications. 1 It also affects patients’ quality of life and has socioeconomic implications. 2,3 People with diabetes usually report poorer health status compared to those not affected. 4,5 The International Diabetes Federation estimated that 366 million people were living with diabetes in the year 2011. 6 Diabetic foot ulcer is one of the most serious and most important complication, having a major impact on patient health-related quality of life. 7,8 Studies advocated that 15% diabetes patients develop foot ulcers throughout their life span, and troubles continue for longer periods due to development of serious complications. 9,10 Moreover, 4% to 6% of the patients are subjected to lower limb amputations. 11,12 Since India has the highest number of patients with diabetes worldwide and is also the highest regional contributor in terms of diabetes mortality, 13 about 40 000 lower limb amputations are performed each year in India due to diabetic complications as per the World Diabetes Foundation. 14 Epidemiological data show that approximately 90% of the Indians with diabetes had diabetic foot infections, of which 30% underwent a major amputation and 70% a minor amputation. 15,16 Reports also state sociocultural acts are the main source of diabetic foot infection among Indians. 17
Ayurveda describes ulcer (Vrana) as a discontinuity or break in the continuity of the body or bodily tissues, creating permanent changes in the body in the form of scar even after healing. 18 To promote the process of wound healing, which is termed as Ropana in ayurveda, drugs that facilitate the growth of the normal tissue for wound healing are prescribed. Ghrita (clarified butter), Tila Taila (sesame oil), and Siktaka (wax) are used as base for the preparation of the topical dosage forms useful for the Shodhana (detoxification) and Ropana (wound healing) of the Vrana. 19,20 These lipid-based preparations have slower and prolonged absorption through the skin and can be conveniently applied to the local area of damage. 21 This study can provide the evidences for the use of combinatorial herbal with insulin and herbomineral therapy in the view of “polypharmacology.” 22 This integrative approach is based on a combination of a conventional drug regimen with ayurvedic intervention and is termed as ayurvedic adjunct therapy. This treatment strategy is quite viable in integrative medicine point of view. It seems to be a novel option in treatment of complex metabolic disorders like diabetes with dire consequences such as foot ulcers in improving patient quality of life and treatment satisfaction. 23,24
Material and Methods
Hospital-based cross-sectional study for assessing quality of life and treatment satisfaction (Diabetes Treatment Satisfaction Questionnaire) among patients with diabetes was conducted. Thirty-six patients with diabetes foot ulcers as complications, from the surgery outpatient clinic at SDM College of Ayurveda and Hospital, Hassan, Karnataka, India, over a 3-month period between June and August 2013, were considered for this observational study. Patients with diagnosed type 2 diabetes complying with the World Health Organization criteria were considered eligible for the study. 13 All patients had been managed in a joint diabetes clinic and had received dietary advice from a specialist dietitian. Patients were on insulin therapy before regular meals with dose calculated according to glucose levels and tolerance. Patients were also administered ayurvedic poly-herbomineral formulations (see section on Drug Regimen) externally and orally. This is the normal Ayurvedic adjunct treatment regimen followed for patients with diabetes foot ulcers in the hospital. Patients receiving a minimum of 4 weeks of ayurvedic adjunct therapy (insulin + ayurvedic intervention) were considered for the study. Patients who had undergone treatment for at least 4 weeks were invited to complete the Audit of Diabetes Dependent Quality of Life Questionnaire and the Diabetes Treatment Satisfaction Questionnaire. 25 –29 The work was considered a retrospective audit and was approved by the institutional ethics committee.
Patient-Reported Outcome Measures
Diabetes Treatment Satisfaction Questionnaire
The Diabetes Treatment Satisfaction Questionnaire is used to assess a patient’s satisfaction with specific areas of their treatment and perceived frequencies of hyperglycemia and hypoglycemia. The Diabetes Treatment Satisfaction Questionnaire is designed as a supervised self-reported questionnaire. That is, the patients should complete the questionnaire themselves, with someone available to provide assistance if required. In the case of this study, however, patients were offered the option of having the questions read to them. It was felt that this would avoid any difficulties regarding literacy problems, and indeed relieve the patient of any undue pressure they may experience in completing such a questionnaire. The Diabetes Treatment Satisfaction Questionnaire is a validated self-administered questionnaire consisting of 6 items (current treatment, convenience, flexibility, understanding, recommend, continue). Each item is scored from 0 to 6 on a 7-point Likert-type scale. The total treatment satisfaction score can therefore range from 0 (very dissatisfied) to 36 (very satisfied). The Diabetes Treatment Satisfaction Questionnaire also includes 2 additional items, which measure perceived perception of hyper- or hypoglycemia. These are also scored from 0 (none of the time) to 6 (most of the time). 25,26,29
Audit of Diabetes Dependent Quality of Life Questionnaire
The Audit of Diabetes Dependent Quality of Life Questionnaire is designed to measure individuals’ perceptions of the impact of diabetes on their quality of life. As in the case of the Diabetes Treatment Satisfaction Questionnaire, patients were offered the option of having the questions read to them. Diabetes-specific quality of life was assessed using the Audit of Diabetes Dependent Quality of Life Questionnaire–19 questionnaire consisting of 2 overview items: one measures generic overall quality of life (−3 to +3) and the second measures the specific impact of diabetes on quality of life (−3 to +1). A further 19 domains concerned with the impact of diabetes on specific aspects of life are also measured. Participants are asked to rate the impact of diabetes on each domain and the importance of the domain for their quality of life. These 2 scores are then multiplied to yield a weighted impact score for each domain (range = −9 [maximum negative impact of diabetes] to +3 [maximum positive impact of diabetes]). Finally, an average weighted impact (average weighted impact) score is calculated for the entire scale. 27 –29
Drugs Regimen
Insulin Actrapid was administered daily before meals, and the administered dose was according to the patients’ medical condition and physicians’ discretion, depending on glucose levels and tolerance. Triphala Guggulu is a poly-herbal compound having Guggulu (Commiphora mukul) as its base. The administered dose was 500 mg to 1000 mg, 2 to 3 times a day before food. 30 –32 Gandhaka Rasayana is a poly-herbomineral compound having purified Gandhaka (sulfur) as its main ingredient. The administered dose was 1 to 3 g, once or twice a day before or after food. 33 –35 Asanadi Kashayam is a poly-herbal combinatorial in water decoction form. The administered dose was 5 to 10 mL of Kashaya (decoction) once or twice a day. 36,37 Jatyadi Taila (oil) was used for external application. 38 –40
Data Analysis
The data were managed, entered, and analyzed using Statistical Package for Social Sciences (SPSS) version 15. Fisher exact tests (analysis of variance) and Pearson correlation were used to find the association between quality of life, treatment satisfaction scores, and sociodemographic variables. Statistical significance was considered at P < .05.
Results
The demographic distribution of the study population shows highest prevalence of diabetes foot ulcers among males aged 55 to 64 and females aged 45 to 64. The age distribution of the study population is shown in Figure 1. The mean age (in years) of the study population was 58.31 ± 12.601. The demographic data of the study subjects are shown in Table 1. Most of patients (38.9%) completed college/university education, while the lowest was found to be primary level of school education. Most patients (88.9%) were married and only one (2.8%) was unmarried. The occupation of the study subjects represented mostly retired personnel (30.6%), followed by self-employed (27.8%) and homemaker (25.0%). The family history of diabetes among participants shows that more than half of the patients (55.8%) had no family history of diabetes. It was recorded that 14% of them have a history of diabetes among their siblings with 5.6% having both parents. The mean duration of diabetes among the participants were found to be 9.32 ± 5.3 years. This indicates that patients with diabetes of at least 4 years developed diabetes foot ulcer. The diabetes complications and their frequencies are summarized in Table 2. It was found that 19.5% of the patients had foot ulcer and skin infections. Five of the patients had at least 4 related complications with foot ulcer. Four patients had hypertension together with the foot ulcer.
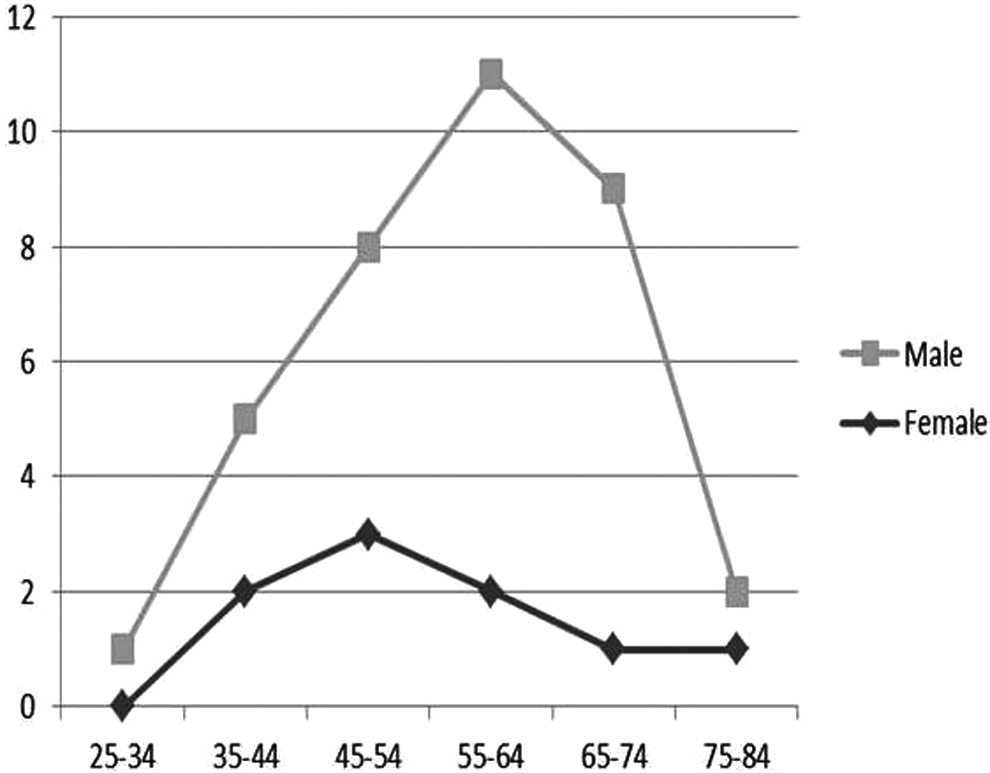
Age distribution of the participants.
Distribution of Demographic Characteristics of the Participants.

Distribution of Diabetes Complications Associated With Foot Ulcers.
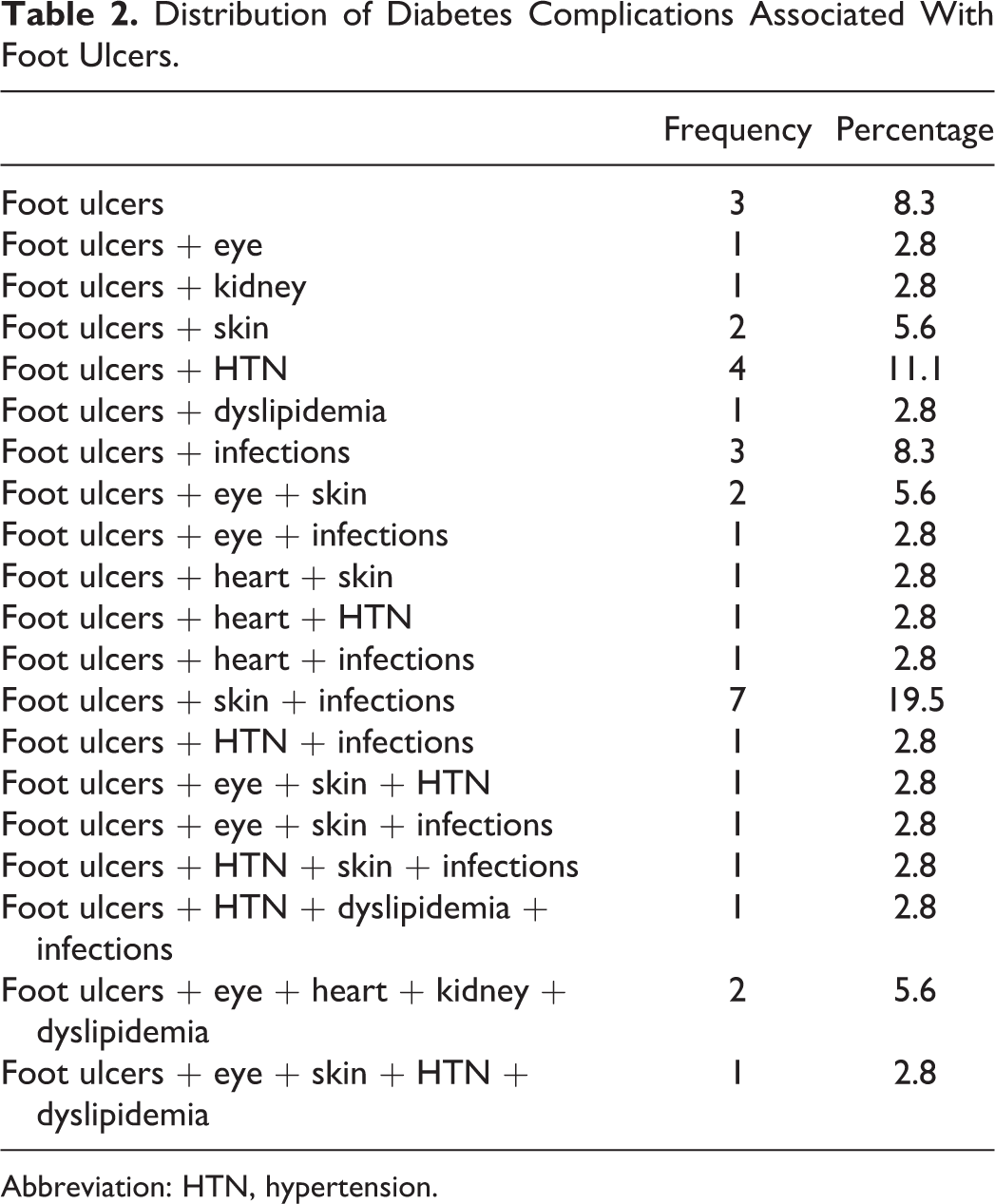
Abbreviation: HTN, hypertension.
Diabetes Treatment Satisfaction Questionnaire
Analysis of results indicated that participants had a mean (SD) Diabetes Treatment Satisfaction Questionnaire score of 26.0139 ± 5.20369. Scores ranged from a high of 36 to a low of 13. The average score for perceived frequency of hyperglycemia was 3.3333 ± 1.92725 while that for perceived frequency of hypoglycemia was 0.8889 ± 1.30445. The recommendation of this kind of treatment to other patients had the highest positive score of 5.0278 ± 1.13354 (Figure 2).

Distribution of Diabetes Treatment Satisfaction Questionnaire (total treatment satisfaction) score of the 8 domains.
Audit of Diabetes Dependent Quality of Life Questionnaire
Diabetes was found to have on average a negative impact on all the 19 items. The item “living conditions” had the greatest negative impact in all participants (−4.5278). This was followed by “freedom to eat” (−4.0556). The way in which patients perceive society’s reaction to them had the least negative impact, with a score of −1.9167. When average scores for each item were summed and divided by the number of domains, the average weighted impact score for the 36 participants in the study was found to be −3.0819 ± 1.83003, which ranged from a minimum of −7.50 to a maximum of −0.60. Of the 2 overview items, the first, measuring the present quality of life showed a mean (SD) sore of −0.1667 ± 0.91026. For the second overview item, measuring the impact of diabetes on the quality of life, the mean (SD) score was −1.9722 ± 0.84468.
Pearson’s correlation analysis between Diabetes Treatment Satisfaction Questionnaire (total treatment satisfaction) score and Audit of Diabetes Dependent Quality of Life Questionnaire (average weighted impact) score revealed a nonsignificant (P = .283) relationship of the calculated parameters. Relationship between diabetes-associated markers showed that duration of diabetes was not significant with Diabetes Treatment Satisfaction Questionnaire (total treatment satisfaction) score (P = .184) and Audit of Diabetes Dependent Quality of Life Questionnaire (average weighted impact) score (P = .518). When relationship with diabetes complications were assessed using analysis of variance it was found that Audit of Diabetes Dependent Quality of Life Questionnaire (average weighted impact) score (F = 1.171; P = .383) had no relationship, but Diabetes Treatment Satisfaction Questionnaire (total treatment satisfaction) score (F = 2.475; P = .039) showed significance. Association with sociodemographic variables were also observed, which showed that age (Pearson correlation) was not a factor to influence Diabetes Treatment Satisfaction Questionnaire (total treatment satisfaction) score (P = .769) and Audit of Diabetes Dependent Quality of Life Questionnaire (average weighted impact) score (P = .426). Mann–Whitney analysis proved that Audit of Diabetes Dependent Quality of Life Questionnaire (average weighted impact) score (P = .039) was significantly related to gender of patients, while Diabetes Treatment Satisfaction Questionnaire (total treatment satisfaction) score (P = .634) showed insignificant association. Analysis of variance for assessing relationship between education level and Audit of Diabetes Dependent Quality of Life Questionnaire (average weighted impact) score (F = 3.427; P = .020) showed significant association. On the contrary, Diabetes Treatment Satisfaction Questionnaire (total treatment satisfaction) score (F = 1.209; P = .327) showed no relationship with education. Also no significant association was seen between Audit of Diabetes Dependent Quality of Life Questionnaire (average weighted impact) score, marital status (F = 1.628; P = .183) and work status (F = 0.103; P = .902) of the participants.

Distribution of Audit of Diabetes Dependent Quality of Life Questionnaire (average weighted impact) score according to individual 19 domains.
Discussion
The impediment of diabetes foot ulceration is quite severe, preceding 84% of lower extremity amputations in the resource-scarce parts of the world where diabetes prevalence is higher but efficient diagnostic, therapeutic, and rehabilitative facilities are inadequate. 41,42 The dispute of management challenge of diabetes foot ulcer in developing countries is that most patients with diabetes foot ulcer present to health care facilities late with advanced foot ulcers. The grounds for late perceptive include poor economic competencies in cost-shared health care systems, inadequate knowledge of self-care, sociocultural reasons, and poor and/or inadequate diabetes health care. 43 The foot ulcer has relentless consequences for patients, family, health care system, and society. Mortality in this patient group is soaring, 2- to 4-fold compared with diabetes patients without ulcers, 42 especially for patients with critical ischemia. 44 Furthermore, it has been highlighted that good diabetes care can only be ensured if the health care professionals share patients’ personal perception of living with diabetes, apart from professional understanding of the illness. 45 Qualitative researches over the years have established the clinical opinion that diabetic foot ulcers have enormous physical, psychological, and social effect. 42,46 Patients’ viewpoint about health, illness, control, and cure are predictive of the product of lifestyle changes and pharmacological treatment.
In this study, the diabetes foot ulcer patients under insulin and ayurveda intervention reported quality of life, either assessed as a global score or as specific items across important life domains. Patients treated with this combination therapy reported that foot ulcer had the ameliorative impact on their quality of life. Similar findings have been conveyed by several other studies, which found that health-related quality of life scores were significantly poorer for patients with diabetes foot ulcers. 47 –51 In this study, male patients represented more than female patients, which may provide insight that foot ulcers are more common in males. 3 Studying the relationship between quality of life and the study variables, a nonsignificant relationship was observed between diabetes duration, complications, and quality of life for all domains. As patients were having multiple complications with increased diabetes duration, they already affected the quality of life with recorded negative Audit of Diabetes Dependent Quality of Life Questionnaire (average weighted impact) score. So which particular associated complication affected the quality of life did not matter, since it is a known fact that lower quality of life is associated with comorbidities and diabetic complications. 52 –54 There was a significant relationship between gender and quality of life, which affects the domains of daily activities, friendship, family relationships and positive attitude, pleasure of life, physical health and emotions in women; this may reflect the deep impact of this variable on the quality of life of women than men; also supported by other studies stating that women reported poorer physical and psychological well-being than men. 8,55 No significant relationship was observed in quality of life and employment status. Interestingly, association was found between education and quality of life. This trend shows that perception about quality of life seems to be different with changing educational level. 8
Drugs like Gandhaka Rasayana and Triphala Guggulu have anti-inflammatory effects. Jatyadi Taila is known for its wound healing property. Our study recognized that ayurvedic adjunct therapy together with insulin can show efficient wound healing and foot ulcer management. Gandhaka Rasayana is sulfur-based herbomineral immunomodulator, which can efficiently enhance the immune status of the diabetic patients, helping the wound healing internally. Triphala Guggulu and Jatyadi Taila have anti-inflammatory and wound healing property, which on topical application has very good wound healing property due to the bioactive phytomolecules present, known for their antimicrobial, immunomodulator, anti-inflammatory, and detoxifying property. 30,32,35 –37,39,40
Diabetes Treatment Satisfaction Questionnaire is a measure of treatment satisfaction that was designed explicitly to measure issues of importance to patients and therefore it was significant to assess this ayurveda combination therapy. 25 The Diabetes Treatment Satisfaction Questionnaire is highly sensitive to major changes in treatment, for example, from tablets to injections or from conventional (more rigid insulin regimen with fixed meal times) to a more flexible insulin dosing (allowing for dietary freedom). 56,57 It is seen that treatment satisfaction score correlates with the duration of diabetes and perceived blood glucose control. 58 Nevertheless, we found that ayurvedic drugs significantly increased treatment satisfaction among patients. The satisfaction may due to positive pharmacological action and no adverse effects sometimes found in standard treatment regime.
Diabetes poses special problems in the later years of life, which call for different therapeutic goals and a “package of care” orientated more toward secondary prevention and maintaining psychosocial well-being than strictly metabolic goals. Health education plays a very crucial role in prevention and control of diabetes and its complications. Importantly, repeated health education/reinforcement and motivation are bound to bring about a positive change in self-care practices with regard to diabetes control. The study was not multicentric (and hence results are not generalizable), blinding was not done, and treatment was not randomized; these were some of the limitations or lacunae in the present study. Furthermore, we did not have the opportunity to assess quality of life or diabetes treatment satisfaction before commencing treatment, which might have been useful to record the change in quality of life associated with treatment. The study findings have implications for clinical and policy decisions, as well as for the foundation and design for future studies with larger sample sizes. In particular, our findings underscore the importance of health-related quality of life, treatment satisfaction, and an integrated therapeutic approach in the management of patients with diabetes foot ulcers.
In summary, this study is evidence of the fact that ayurvedic intervention is associated with improved treatment satisfaction and a favorable impact on quality of life together with insulin in combination. However, further studies are needed to confirm this finding using a randomized controlled trial design.
Footnotes
Acknowledgements
The authors would like to acknowledge Professor Clare Bradley, Health Psychology Research, Royal Holloway University of London, Surrey, UK, for giving permission to use the Audit of Diabetes Dependent Quality of Life Questionnaire and Diabetes Treatment Satisfaction Questionnaire. The authors would also like to thank the patients, the nurses, and the hospital that made this study possible.
Author Contributions
PD and AP: Clinical research, data collection, analysis, manuscript preparation. SB: pharmacological or pharmaceutical aspect of clinical research, reviews of literature, manuscript preparation. PNR, TBT, AA, and SK: Overall monitoring, study design, and concept.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from Institutional Ethics Committee of SDM College of Ayurveda and Hospital, Hassan, India.