
Abstract
Objective:
This study evaluated whether harp therapy reduces levels of stress and improves clinical outcomes in patients undergoing embryo transfer.
Design:
This prospective randomized trial enrolled 181 women undergoing embryo transfer, who were randomized to harp therapy during embryo transfer or standard treatment. Patients underwent standardized psychological testing and physiologic assessment of stress.
Setting:
The study was conducted in a reproductive medicine practice.
Results:
No statistically significant differences were found in the heart and respiratory rates, nor was there a significant difference in event-based anxiety at baseline. Harp therapy had a significantly larger decrease in state anxiety from pre– to post–embryo transfer. Clinical pregnancy was 53% versus 48% for the harp therapy and standard treatment groups, respectively.
Conclusion:
Harp therapy decreases state, or event-based, anxiety, significantly lowering state scores posttransfer and having a positive effect on acute levels of stress. There was an increased pregnancy rate, but larger sample sizes are needed to evaluate whether harp therapy has an effect on clinical outcomes.
Since the first successful birth resulting from in vitro fertilization–embryo transfer in 1978, there have been numerous advances with in vitro fertilization–embryo transfer. 1 These advances have occurred in almost every aspect of the in vitro fertilization process. Current ovarian stimulation regimens now include the use of gonadotropin-releasing hormone agonist as well as antagonists that prevent premature luteinizing hormone surges and ovulation. 2 There have also been changes in the medications used to stimulate multifollicular oocyte development from urinary-derived gonadotropins to now highly purified recombinant derived products. 2 The in vitro culture environment has been modified from media originally borrowed from the growth of somatic cells to the current media that contains nutritional requirements specific for the growing human embryo. 3 In 1991, the introduction of microsurgical fertilization (intracytoplasmic sperm injection) revolutionized the treatment of male factor infertility. 4 These important changes have been critical to the steady increase in “take home babies” from in vitro fertilization–embryo transfer. Despite these advances, the overall success rate for in vitro fertilization–embryo transfer still remains less than 50%. One important aspect that has been neglected is the utilization of complementary alternative medical therapies to enhance in vitro fertilization–embryo transfer success. This is what led to the exploration of music therapy, specifically harp therapy, as an adjunctive therapy in the in vitro fertilization process in an attempt to reduce patient anxiety and improve in vitro fertilization success.
For over a decade, music therapy has been shown to reduce patient anxiety, alleviate pain, and modify a number of physiologic parameters. A recent meta-analysis evaluated the efficacy of music therapy for premature infants and found an overall positive effect on observed infant behaviors, reduction in heart rate and respiratory rate, improved oxygen saturation, improved weight gain, reduced hospital stay, improved feeding rate, and nonnutritive sucking rate. 5 Music therapy provides other benefits in the care of premature infants, including promoting bonding with family members, pacification and developmental stimulation, and assisting with the infant’s transition to the home environment. 5 A 2006 study objectively assessed the physiologic alterations caused by music therapy were. The authors noted that heart rate, blood pressure, minute ventilation, and middle cerebral artery flow velocity were all altered by different tempo and rhythmic structures of musical compositions. The authors suggested that the appropriate selection of music, by altering fast and slower rhythms and pauses, can induce relaxation and reduce sympathetic activity and thus be potentially useful in the management of cardiovascular disease. 6 The Cochrane Database of Systematic Reviews in April 2006 published findings on music for pain relief. This meta-analysis included only randomized clinical trials and noted that listening to music reduced pain intensity and opioid requirements, but the magnitude of these benefits is small and, therefore, the clinical importance unclear. 7 Currently, there are no published reports of music therapy in the assisted reproductive medicine literature.
It has become increasingly clear that nontraditional alternative therapies have some profound psychological as well as physiologic effects in clinical medicine. In the past, these therapies have not gained respect due to the lack of well-designed clinical trials supporting the touted benefits. Now that improved scientific studies have begun to show statistical benefits in a number of psychological and physiologic parameters, many academic institutions are beginning to integrate complementary and alternative medicine into their clinical armamentarium. This study is an innovative prospective randomized trial evaluating harp music therapy in assisted reproductive medicine.
Materials and Methods
This was a prospective randomized trial conducted at a community hospital–based reproductive medicine practice. The patients were subfertile women aged 21 to 44, all under the care of Abington Reproductive Medicine and Genetics and requiring in vitro fertilization–embryo transfer. Patients were excluded if they were already enrolled in other in vitro fertilization–embryo transfer clinical trials or undergoing preimplantation genetic diagnosis. Controlled ovarian stimulation protocols based on patient’s previous response to ovarian stimulation, age, and day 3 follicle-stimulating hormone and estradiol hormonal status were implemented. Follicular maturation was monitored by daily estradiol levels and transvaginal ultrasounds. Human chorionic gonadotropin (5000–10 000 IU) was administered when at least 2 follicles reached a mean diameter of greater than or equal to 17 mm. Transvaginal oocyte retrieval was performed 35 hours later. Conventional in vitro insemination or intracytoplasmic sperm injection was performed on the basis of appropriate indications. 8 Preimplantation embryo growth was then monitored on a daily basis, as routinely done by the embryologists. The appropriate numbers of embryos were then transferred to the patients per the American Society of Reproductive Medicine guidelines on number of embryos to transfer, based on the patient’s age and associated fertility history. 9 Before embryo transfer, the patients were randomized per a random-numbers table to the harp therapy group or the standard treatment group. Specifically, women were randomized to receive either harp therapy for 20 minutes with embryo transfer or standard treatment. A certified music practitioner performed harp therapy. All patients had their blood pressure, heart rate, and respiratory rate assessed pre–embryo transfer, during embryo transfer, and post–embryo transfer. In addition, all patients answered the State-Trait Anxiety Inventory questionnaire before and after embryo transfer. The patient’s clinical outcome was assessed according to implantation rate and clinical pregnancy rate.
The primary hypothesis was that harp therapy improved anxiety-related clinical outcomes. Based on clinical experience with similar patient populations, an estimated one-third (33%) of the patients would experience elevated blood pressure and/or heart rate readings in the moderate-to-severe range during the course of the standard procedure. However, harp therapy was expected to reduce the proportion of moderately to severely stressed women to 20% or less. According to these estimates, 180 women per group (total 360) would be needed to achieve statistical significance at the alpha level of 0.05 with 80% power (Table 1).
Sample Size Required to Achieve Statistical Significance, Assuming Various Reduced Stress Rates as a Consequence of Using Harp Therapya.

aAlpha = 0.05, power = 80%.
The secondary hypothesis was that harp therapy would result in a statistically significant increase in the pregnancy rate compared to standard treatment. Based on a mean pregnancy rate of 40% per the standard treatment, harp therapy was expected to increase the pregnancy rate above 50%. According to these estimates, 388 subjects per group (total 776) would be needed to achieve statistical significance at the alpha level of 0.05 with 80% power (Table 2).
Sample Size Necessary to Achieve Statistical Significance, Assuming Various Pregnancy Rates as a Consequence of Using Harp Therapya.

aAlpha = 0.05, power = 80%.
All patients filled out a State-Trait Anxiety Inventory questionnaire pre– and post–embryo transfer. This questionnaire differentiates between temporary or event-based (“state”) anxiety and long-standing (“trait”) anxiety. Higher scores indicate greater levels of anxiety.
The 2 groups were compared on demographic and clinical factors to examine for balance by randomization. A 2-sample t test was compared age, and Wilcoxon rank-sum tests compared variables, such as follicle-stimulating hormone levels, estradiol levels, and number of transferred embryos. Results are presented as odds ratios with 95% confidence intervals.
Poisson regression was used to test for differences in the implantation rate (number of fetal sacs per number of transferred embryos), again both unadjusted and after adjusting for age, follicle-stimulating hormone, and estradiol. Results are presented as rate ratios with 95% confidence intervals. All analyses were performed with SAS 9.2 (SAS Institute, Cary, NC).
Results
There were 101 treated and 101 nontreated women enrolled in the study. Three in the harp therapy group and 1 in the standard treatment group were excluded for canceled cycles. Additionally, another 3 in the harp therapy group and 7 in the standard treatment group had zero embryos transferred and were excluded from final analysis. Finally, 5 in the harp therapy group withdrew or did not receive harp therapy during in vitro fertilization–embryo transfer and were therefore excluded, as well as 2 in the standard treatment group who were found to be ineligible or not included. This left a final sample size of 90 women who received harp therapy and 91 women who did not. Table 3 shows the demographic and clinical characteristics stratified by treatment group. There were no statistically significant differences between the groups.
Demographic and Clinical Characteristics of Treatment Groups.

aMean ± standard deviation, 2-sample t test.
bMedian (Q1-Q3), Wilcoxon rank-sum test.
cNo. (%), χ2 test.
Table 4 shows the means and standard deviations for the vital measurements at 3 time points (pre–, during, and post–embryo transfer). Table 5 shows the means and standard deviations for the changes in these measurements from baseline (pre–embryo transfer). Women in the control group had statistically significant higher systolic (124.9 ± 13.0 vs 131.2 ± 16.1, P = .0046) and diastolic (79.0 ± 11.7 vs 84.2 ± 11.0, P = .0026) blood pressure measurements pre–embryo transfer as well as systolic blood pressure (118.8 ± 12.3 vs 124.1 ± 13.5, P = .0075) post–embryo transfer. However, there was no difference found during embryo transfer. Regarding changes over time, women in the standard treatment group had a larger decrease in systolic and diastolic blood pressure from pre–embryo transfer to during embryo transfer (unadjusted P = .0409 and .0067, respectively), but this difference was not significant when adjusted for baseline measures (adjusted P = .3309 and .2877, respectively). No statistically significant differences were found in the heart rate or respiratory rate at any of the 3 time points or in changes from baseline with either group.
Vitals by Treatment Group.

aMean ± standard deviation.
bTwo-sample t test.
cAdjusted for age, gravity, parity.
Change in Vitals by Treatment Group.

aMean ± standard deviation.
bTwo-sample t test.
cAdjusted for age, gravity, parity, vital measurements at time 1.
Table 6 presents the means and standard deviations for the pre- and posttransfer State-Trait Anxiety Inventory scores, where higher scores indicate greater levels of anxiety. For the state score, no significant difference was found between groups at baseline, but women in the standard treatment group had statistically significantly higher state scores posttransfer (adjusted P = .0018). Women receiving harp therapy had a significantly larger decrease in state score from pre– to post–embryo transfer compared to women receiving standard treatment (adjusted P < .0001, Table 7). For trait scores, women in the harp therapy group had statistically significantly higher scores pre–embryo transfer (adjusted P = .0322) but not post–embryo transfer (adjusted P = .3779). The difference from pre– to post–embryo transfer was significant in the unadjusted model (P = .0355) but not after adjusting for pre–embryo transfer trait scores (P = .1400; Table 7).
State-Trait Anxiety Inventory Scores by Treatment Group.

aMean ± standard deviation.
bTwo-sample t test.
cAdjusted for age, gravity, parity, and prescore.
Changes in State-Trait Anxiety Inventory Score by Treatment Group.

aMean ± standard deviation.
bTwo-sample t test.
cAdjusted for age, gravity, parity, and prescore.
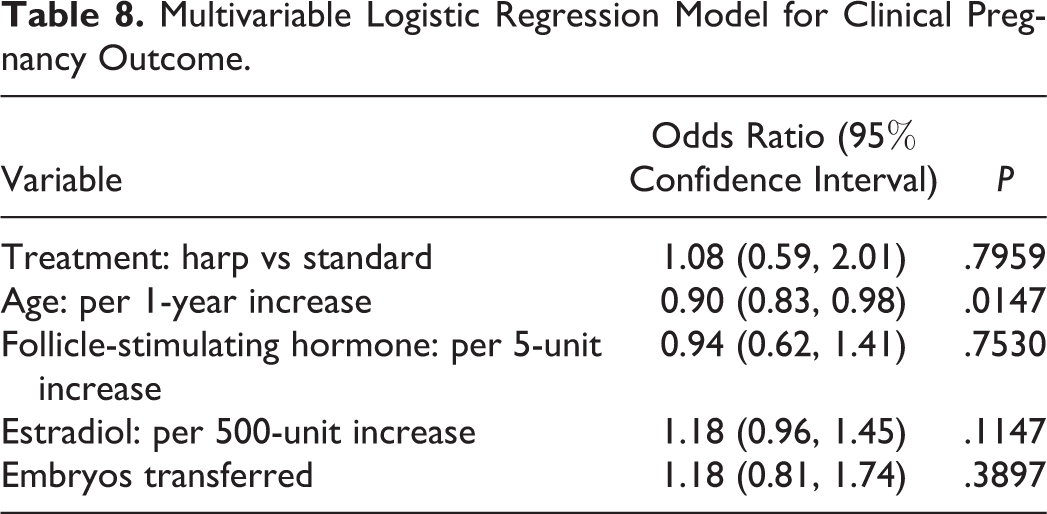
Fifty-three percent of the women receiving harp therapy had a successful clinical pregnancy versus 48% in the standard treatment group. The odds of clinical pregnancy were not statistically significant between the 2 groups (odds ratios, 1.22; 95% confidence intervals: 0.68, 2.19; P = .50). Table 8 shows the results from a multivariable logistic regression model for the clinical pregnancy rate. After adjustment for age, follicle-stimulating hormone, estradiol, and the number of embryos transferred, harp therapy still had no effect on the clinical pregnancy rate (odds ratios =1.08; 95% confidence intervals: 0.59, 2.01; P = .80). Age was associated with a decrease in the pregnancy rate (odds ratios = 0.90 per 1-year increase in age; 95% confidence intervals: 0.83, 0.98; P = .01). Hormone levels (estradiol and follicle-stimulating hormone) and the number of transferred embryos were not associated with the clinical pregnancy rate.
Multivariable Logistic Regression Model for Clinical Pregnancy Outcome.
The median implantation rate in women receiving harp therapy was 0.3 versus 0 in the standard treatment group. The implantation rate in the harp therapy group was 1.17 times greater than those in the standard treatment group, but this was not statistically significant (rate ratio = 1.17; 95% confidence intervals: 0.84, 1.64; P = .35). Table 9 shows the results of a multivariable Poisson regression model for the implantation rate. Harp therapy was not significantly associated with implantation rate after adjustment for age and hormone levels (rate ratio = 1.14; 95% confidence intervals: 0.81, 1.60; P = 0.45). Age was associated with a decrease in the implantation rate (rate ratio = 0.94; 95% confidence intervals: 0.90, 0.98; P = .002). Hormone levels were not associated with implantation rate.
Multivariable Poisson Regression Model for Implantation Rate Outcome.

Discussion
This is the first clinical trial evaluating an innovative complementary therapy (harp therapy) and its effect on in vitro fertilization–embryo transfer. The goal was to reduce the anxiety associated with the in vitro fertilization–embryo transfer process and improve clinical outcomes. Prior studies on the psychological effects of the in vitro fertilization–embryo transfer process on pregnancy outcomes have been varied. Inconsistencies may be found in the unstandardized measurement of these psychological variables. It is highly dependent on subjective patient derived data. Also, there has been a lack of data looking at possible underlying psychological diagnosis that may be affecting the variables. Lee et al found that women that are about to undergo in vitro fertilization–embryo transfer report higher levels of depressive symptoms as well as more intense feelings of emotions, positive and negative, as compared to women of a similar age. 10 Another study by the same group found a strong relationship between negative emotions and embryo quality in patients with a prior poor prognosis (age > 40 years, high follicle-stimulating hormone > 14). 11 However a recent meta-analysis by Boivin et al looked at 14 studies with 3583 women undergoing a cycle of assisted reproductive technology. The conclusion of this analysis was that emotional distress before treatment did not affect the pregnancy rate after 1 cycle of treatment with assisted reproductive technology. 12 Although stress may not decrease pregnancy outcomes, there is evidence that that psychological or complementary treatments targeted at anxiety and depression may help improve quality of life during this process. 10
An integral part of the in vitro fertilization process is the patient’s mental well-being and ability to remain in treatment. A Swedish study published in 2002 found that approximately 60% of patients with paid cycles dropped out of their in vitro fertilization treatment. Of these patients, greater than 25% stated psychological burden as their reason. 13 Another similar study performed a psychiatric assessment on 112 women before starting a new in vitro fertilization cycle and found that 40.2% had some anxiety or depression disorder and that only 6.7% had ever sought prior psychiatric treatment. 14
Our current study demonstrated that harp therapy decreases patients “state,” or event-based, anxiety. Women in the standard treatment group had significantly higher state scores posttransfer, thus demonstrating that harp therapy has a positive effect on acute levels of stress as assessed by psychological measures. Physiologic markers of stress, such as blood pressure, heart rate, and respiratory rate, did not have a statistically significant change over the course of treatment in either group. It was shown that the standard treatment group did have pre–embryo transfer blood pressures that were significantly higher than the harp therapy group, as well as higher systolic blood pressure post–embryo transfer. This indicates that harp therapy creates a more relaxing environment that may reduce physiologic levels of stress. With a larger sample size, changes in physiologic measures may become significant. Also, it appears that patients in the standard treatment group may have had baseline elevation in their blood pressure and some of these patients may have been predisposed to high blood pressure. Overall, there was a downward trend in all physiologic markers of stress in both groups throughout the procedure. These markers are very dynamic, and it may be beneficial to have more recordings during in vitro fertilization–embryo transfer to determine if there are any significant changes in these markers and if harp therapy has any effect.
Although not statistically significant, there was a small trend of increased implantation rate and clinical pregnancy rate in the harp therapy group. As demonstrated by the power analysis, a much larger sample size would be needed to detect statistically significant differences. Ideally, larger multicenter studies will be designed to answer the clinical outcome questions.
Limitations of the study include the lack of data on prior psychiatric diagnosis or treatment that may have an effect on the State-Trait Anxiety Inventory trait score. This information may help to assess which patients are more at risk for having issues with anxiety during the in vitro fertilization–embryo transfer process. A larger sample size would be ideal to better assess whether harp therapy truly has a significant effect on pregnancy outcomes. Strengths of this study include its design (ie, a prospective randomized trial) and ease of reproducibility in other clinical settings. Also, standardized psychological testing was used to more accurately evaluate the patients’ anxiety status.
In conclusion, the present study demonstrated that advanced medical therapies can easily be integrated with complementary and alternative treatments, such as music therapy. If music therapy can reduce patients’ stress levels and if patients perceive the process of in vitro fertilization to be better as a result, then this may reduce the dropout rates and ultimately lead to better clinical outcomes. The current study should be used as a building block for future studies to continue to find the link between mind and body and to promote optimal health and treat infertility by addressing contributing factors, such as stress and anxiety.
Footnotes
Acknowledgements
Study was performed at Abington Memorial Hospital, Abington, PA.
Author Contributions
Manuscript preparation, data analysis: EMM. Recruitment of patients, direct patient care: JN, SGS, MS, LIB. Provided psychological consultation and the State-Trait Anxiety Inventory questionnaire: AB. Mentor who contributed equally to this work: LIB.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Project funded by Innovators’ Circle program grant at Abington Memorial Hospital.
Ethical Approval
This study was reviewed and approved by the Abington Memorial Hospital Institutional Review Board.