
Abstract
Aim
This retrospective study aimed to evaluate the predictive value of serum cancer antigen 125 (CA125) levels before hormone replacement therapy on pregnancy outcomes in women with adenomyosis undergoing frozen embryo transfer.
Methods
A total of 509 women with adenomyosis were screened and 84 patients receiving a total of 114 cycles of frozen embryo transfer were included, based on the inclusion and exclusion criteria. Patients were divided into two groups based on their CA125 levels (≤ or >35 IU/mL) before hormone replacement therapy. The basic characteristics and main outcomes of the two groups were compared. Receiver operating characteristic curve and subgroup analyses were also conducted.
Results
There were no significant differences in clinical outcomes of frozen embryo transfer cycles in patients with different serum CA125 levels before hormone replacement therapy. Receiver operating characteristic curve analysis demonstrated that CA125 levels before hormone replacement therapy were not predictive of clinical pregnancy outcomes.
Conclusions
Serum CA125 levels before hormone replacement therapy are not associated with the clinical outcomes of frozen embryo transfer among women with adenomyosis.
Keywords
Introduction
Adenomyosis is a benign disease of the uterus characterized by the presence of endometrial glands and stroma within the myometrium. 1 Although the results of studies evaluating the effects of adenomyosis on the outcome of in vitro fertilization–embryo transplantation (IVF-ET) have been controversial, 2 most have reported a negative impact.3–5 Some women with adenomyosis thus receive pretreatment with a gonadotropin-releasing hormone (GnRH) agonist before frozen embryo transfer (FET). 6 However, the effect and duration of pretreatment with a GnRH agonist before FET remain controversial.7,8 Moreover, long-term pretreatment with a GnRH agonist before FET increases the duration and costs of therapy. There is thus a need to identify a noninvasive biological marker to predict the clinical outcome of FET in women with adenomyosis, to assess the necessity of pretreatment and predict the optimal timing of hormone replacement therapy (HRT).
Cancer antigen 125 (CA125) is the most common serum marker used in screening for the presence and extent of adenomyosis. 9 Sheth and Ray reported that greater enlargement of the uterus due to severe adenomyosis was associated with a greater increase in CA125 levels, 10 and Kil et al. 9 reported that the mean serum CA125 level was significantly higher in women with adenomyosis than in patients with myoma. However, the association between serum CA125 levels before HRT and the clinical outcome of FET in patients with adenomyosis has not been reported.
This retrospective study thus aimed to evaluate the predictive value of serum CA125 levels before HRT on the pregnancy outcomes of women with adenomyosis during FET cycles.
Methods
Patient population
This retrospective study included 509 women with adenomyosis undergoing IVF/intracytoplasmic sperm injection (ICSI) at the Institute of Reproductive Medicine, The First Affiliated Hospital of Sun Yat-Sen University (Guangzhou, Guangdong, China), between January 2013 and April 2019. The inclusion criteria for the study were: (i) diagnosis of adenomyosis by transvaginal color Doppler ultrasonography or magnetic resonance imaging before FET and (ii) age ≤39 years at the time of commencement of IVF/ICSI. The exclusion criteria were: (i) the presence of hydrosalpinges, intrauterine adhesion, tumor-related disease, pelvic inflammatory diseases, or endometriosis, (ii) endometrial thickness <7 mm on the day of transformation before FET, (iii) prior preimplantation genetic testing, and (iv) patient’s partner underwent testicular sperm extraction because of non-obstructive azoospermia.
Eighty-four patients who underwent a total of 114 cycles of FET were included in the final analysis. Given that serum CA125 levels <35 U/mL were previously reported 11 in more than 95% of healthy women, we divided the included FET cycles into two groups based on a serum CA125 cut-off value of 35 U/L before endometrial preparation using HRT: group A had normal CA125 levels (≤35 U/mL, n = 70 cycles) and group B had abnormal CA125 levels (>35 U/mL, n = 44 cycles).
This study was approved by the Institutional Review Board of the First Affiliated Hospital of Sun Yat-Sen University on 11 January 2020 (reference number: 2020080). The participants were de-identified and the Institutional Review Board therefore waived the need for informed consent.
Cryopreservation and thawing
After ovarian stimulation and oocyte retrieval, embryos were obtained by IVF or ICSI. The embryos were graded on day 3 or 5 after oocyte retrieval using a standardized scoring system. Embryos that met the eligibility criteria were regarded as viable and were subsequently cryopreserved using the vitrification freezing method. The vitrification and thawing procedures were carried out as described by Kuwayama et al. 12 Briefly, embryo vitrification was performed using a Cryotop® Vitrification system (Kitazato Corporation, Tokyo, Japan) with dimethyl sulfoxide, ethylene glycol, and sucrose as cryoprotectants. The embryos were thawed in decreasing levels of sucrose solution (1, 0.5, and 0 M).
FET procedure
Over 80% of the included patients received depot GnRH agonist pretreatment before HRT for 1 to 4 months, with 3.75 or 1.875 mg triptorelin (Decapeptyl®; Ferring Pharmaceuticals, Kiel, Germany) per month. The first injection was administered during the early follicular phase of the menstrual cycle. Serum CA125 levels were measured the day before starting the HRT protocol. Oral estradiol valerate was administered at 4 mg/day for 14 days. Patients were monitored by transvaginal ultrasound and blood hormone levels. Endometrial thickness, uterus volume, and type of adenomyosis were recorded during ultrasound monitoring. Uterine volume (V) was calculated by assuming that it was an ellipsoid, using the formula V = D1×D2×D3 × 0.52, where D1 = transverse diameter, D2 = anteroposterior diameter, and D3 = longitudinal diameter. Progesterone was administered if the thickness of the endometrium was ≥7 mm. Day 3 (D3) embryos were transferred on D4 of progesterone administration, and D5 or D6 blastocysts were transferred on D6 of progesterone administration. If the endometrium had not reached a thickness of 7 mm by D15, the dose of estradiol valerate was increased and continued for an additional 3 to 5 days. If the endometrial thickness had not reached 7 mm by D20, the cycle was usually cancelled.
The same doses of estrogen and progesterone were administered until a serum beta human chorionic gonadotropin assay was conducted at D14 after FET. If the assay result was positive, HRT was continued until week 10 of the pregnancy.
Outcome measures
Implantation rate was defined as the number of gestational sacs observed on ultrasonography divided by the number of transferred embryos. Clinical pregnancy was defined as the presence of an active fetal heart detected by ultrasonography at 5 to 6 weeks after FET. The miscarriage rate was defined as the number of clinical pregnancies lost before 28 weeks of pregnancy divided by the total number of clinical pregnancies. Ongoing pregnancy was defined as a viable intrauterine pregnancy of at least 12 weeks, confirmed by ultrasonography.
Statistical analysis
The Kolmogorov–Smirnov test was used to determine if the continuous variables were normally distributed. Normally distributed data were compared using unpaired Student’s t-tests, and skewed data using the Mann–Whitney U test. Categorical variables were analyzed using χ2 or Fisher’s exact test, where appropriate. Binary logistic regression analysis was performed to detect the association between serum CA125 levels before HRT and the clinical outcomes of FET, while controlling for important confounders. Receiver operating characteristic (ROC) curve analysis was used to evaluate the ability of serum CA125 levels before HRT to predict the clinical outcomes of FET. Statistical analysis was performed using IBM SPSS Statistics for Windows Version 23.0 (IBM Corporation, Armonk, NY, USA). A P value ≤0.05 was considered statistically significant.
Results
The patient selection process is shown in Figure 1. Eighty-four patients who underwent 114 FET cycles were included in the analysis. Adenomyosis was diagnosed by transvaginal color Doppler ultrasonography or magnetic resonance imaging. Serum CA125 levels >35 U/mL occurred before 44 cycles of HRT and levels ≤35 U/mL before 70 cycles.

Flowchart of patient selection procedures.
The baseline demographic and clinical variables of the two groups of patients are presented in Table 1. There was no significant difference in age at freezing, age at thawing, body mass index, duration of infertility, cause of infertility, fertilization method, previous number of thawing cycles, developmental stage of the transferred embryos, number of transferred embryos, distribution of GnRH agonist pretreatment, distribution of coexisting endometriosis, type of adenomyosis, or baseline uterine volume between the groups. There was also no significant difference in endometrium thickness, estradiol (E2) levels, or progesterone levels between the two groups on the day of progesterone administration. However, the mean serum CA125 level before GnRH agonist administration was significantly higher in the CA125 >35 U/mL group compared with the CA125 ≤35 U/mL group.
Baseline demographic and clinical variables of patients in relation to cancer antigen 125 levels.

Values given as mean ± standard deviation or n(%).
CA125, cancer antigen 125; FET, frozen embryo transfer; BMI, body mass index; IVF, in vitro fertilization; ICSI, intracytoplasmic sperm injection; GnRHa, gonadotropin-releasing hormone agonist; E2, estradiol; P, progesterone.
The clinical outcomes of the two groups are shown in Table 2. There were no significant differences in implantation rates between the CA125 ≤35 U/mL and CA125 >35 U/mL groups (28.45% vs. 22.89%, respectively). The clinical pregnancy rate was slightly higher in the CA125 ≤35 U/mL group before HRT, but the difference was not significant (35.71% vs. 31.82%, respectively). Moreover, the ongoing pregnancy rate was also slightly higher in the CA125 ≤35 U/mL group (31.43% vs. 27.27%, respectively) and the miscarriage rate was slightly lower (20.00% vs. 35.71%, respectively), but neither of these results was significant.
Clinical outcome of patients in relation to cancer antigen 125 levels.

CA125, cancer antigen 125; FET, frozen embryo transfer.
Given that pretreatment with a GnRH agonist is an important factor affecting the pregnancy outcomes of FET, we analyzed the data separately for patients pretreated with a GnRH agonist (Table 3). Notably, there were no significant differences in the clinical outcomes of patients pretreated with a GnRH in relation to CA125 level.
Subgroup analysis of patients with gonadotropin-releasing hormone agonist pretreatment before hormone replacement therapy.

GnRHa, gonadotropin-releasing hormone agonist; CA125, cancer antigen 125; HRT, hormone replacement therapy.
The two groups still had similar chances of clinical pregnancy after adjusting for age, baseline serum CA125 levels, and serum CA125 before FET (adjusted odds ratio [OR] = 1.31; 95% confidence interval [CI] = 0.56–3.06), ongoing pregnancy (adjusted OR = 1.36; 95% CI = 0.57–3.27), and miscarriage (adjusted OR = 0.48; 95% CI = 0.08–2.76). Patients pretreated with GnRH agonist also had similar chances of clinical pregnancy (adjusted OR = 1.16; 95% CI = 0.45–2.95), ongoing pregnancy (adjusted OR = 1.20; 95% CI = 0.45–3.22), and miscarriage (adjusted OR = 0.92; 95% CI = 0.12–7.35), irrespective of CA125 level. The results of the binary logistic regression analyses are shown in Tables 4 and 5.
Logistic regression analysis of pregnancy outcomes in relation to cancer antigen 125 levels.
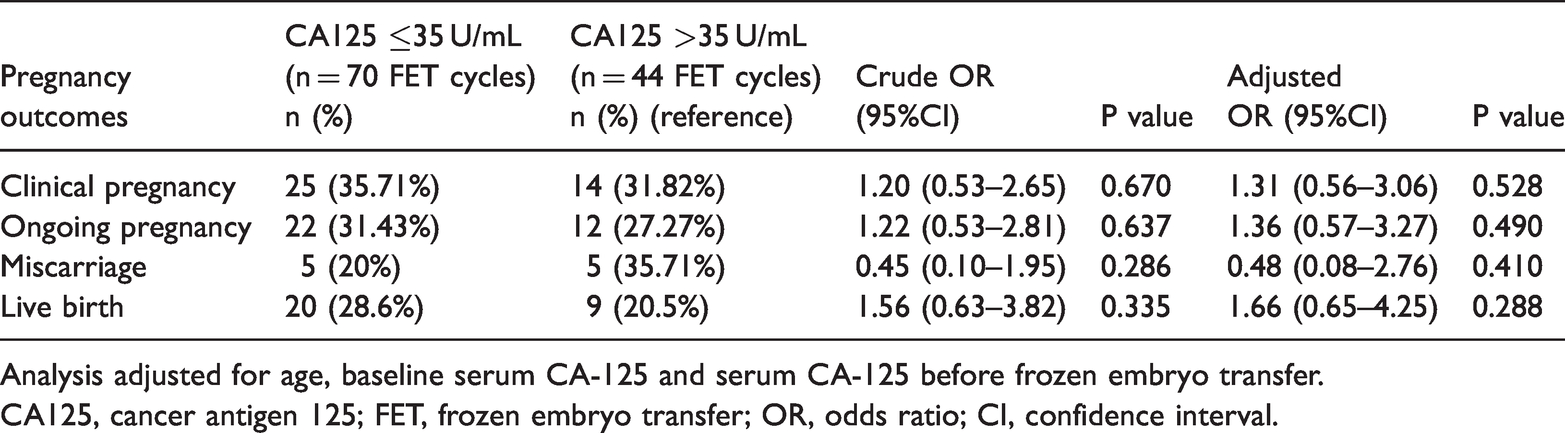
Analysis adjusted for age, baseline serum CA-125 and serum CA-125 before frozen embryo transfer.
CA125, cancer antigen 125; FET, frozen embryo transfer; OR, odds ratio; CI, confidence interval.
Logistic regression analysis of pregnancy outcomes in patients with gonadotropin-releasing hormone agonist pretreatment in relation to cancer antigen 125 levels.

Analysis adjusted for age, baseline serum CA-125 and serum CA125 before frozen embryo transfer.
GnRHa, gonadotropin-releasing hormone agonist; CA125, cancer antigen 125; FET, frozen embryo transfer.
The area under the ROC curve (0.474) indicated that CA125 levels had no predictive value for the outcome of clinical pregnancy (Figure 2).

Receiver operating characteristic (ROC) curve for serum levels of cancer antigen 125 before hormone replacement therapy as predictor of clinical pregnancy among patients with adenomyosis undergoing frozen embryo transfer cycles.
Discussion
To the best of our knowledge, this study provides the first evidence qualifying the impact of adenomyosis on pregnancy outcomes of FET, based on serum CA125 as a biological marker. The results demonstrated that CA125 levels before HRT had no prognostic significance on the outcome of FET.
The extent of adenomyosis has previously been associated with reproductive outcomes, 13 and more severe adenomyosis was associated with a greater increase in serum CA125 levels. 10 However, adenomyosis may be associated with numerous conditions that could impair embryo implantation. The junctional zone of myometrial activity was reported to be affected by adenomyosis 14 , and research also revealed that abnormal contractile activity of the junctional zone in patients with adenomyosis was associated with lower implantation and pregnancy rates following IVF-ET. 15 Moreover, vascularization of the endometrial stroma was unexpectedly increased in patients with adenomyosis, with negative effects on embryo implantation. 16 Furthermore, changes in expression profiles of cytokines and growth factors in the endometrium have been related to adenomyosis-associated infertility. 17 These studies suggest that a mere increase in serum CA125 levels is not an appropriate measure reflecting the complex influence of adenomyosis on the clinical outcome of FET. Furthermore, serum CA125 is a less reliable marker in premenopausal women because of increases in response to various conditions, such as endometriosis, adenomyosis, tumor formation, and even menstruation, 18 and an irrelevant increase in serum CA125 levels could result in misdiagnosis.
The results of subgroup analysis showed that serum CA125 levels before HRT were not associated with the clinical outcome of FET in patients pretreated with a GnRH agonist. Xie et al. 19 reported that serum CA125 levels were significantly reduced after long-term treatment with a GnRH agonist in patients with adenomyosis, and Niu et al. 20 found that long-term pituitary downregulation before FET improved pregnancy outcomes in these women. Lower serum CA125 levels could be associated with shrinking of the uterus and milder pelvic adhesions. 10 , 21 However, the reasons for the improved pregnancy outcomes in these patients are complicated and not well understood. 22 , 23 Thus, a decrease in serum CA125 levels before HRT is not predictive of the clinical outcome of FET in patients with adenomyosis.
There were some limitations to this study, including the retrospective nature of the study and the relatively small sample size, which could cause bias. Further prospective studies with larger cohorts are therefore required to verify the results of this study.
In conclusion, the results of our study suggest that serum CA125 levels before HRT are not related to the rates of implantation, clinical pregnancy, ongoing pregnancy, or miscarriage following FET in women with adenomyosis. Sole detection of serum CA125 levels before HRT is thus not a valid measure, resulting in unnecessary cost and increased anxiety for the patient. The combined detection of other biological markers and/or the identification of novel markers is required to increase the predictive accuracy in the future.
Footnotes
Availability of data and materials
The data sets used and/or analyzed during the current study are available from the database of Center for Reproductive Medicine in the First Affiliated Hospital of Sun Yat-Sen University on reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Guangdong Provincial Key Laboratory of Reproductive Medicine [grant number 2012A061400003] and National Key Research and Development Program [grant number 2016YFC1000205].