
Abstract
Psychological distress is common in patients with implantable cardioverter defibrillators and has been associated with a worse prognosis. The authors examined whether spiritual well-being is associated with reduced psychological distress in patients with ICDs. The Functional Assessment of Chronic Illness Therapy–Spiritual Wellbeing (FACIT-SWB) questionnare and the Hospital Anxiety and Depression Scale (HADS) were used to measure spiritual well-being and overall psychological distress. Multivariate linear regression was used to explore the relationship between these variables. The study sample included 46 implantable cardioverter defibrillator outpatients (32 males, 14 females; age range = 43-83 years). An inverse association between HADS and FACIT-SWB scores was found, persisting after adjustment for demographics, anxiety/depression, medications, therapist support, and functional status (F = .001; β = −0.31, confidence interval = −0.44, −0.19). In conclusion, spiritual well-being was independently associated with lower psychological distress in ICD outpatients. Spiritual well-being could act as a protective factor against psychological distress in these high-risk patients.
Primary and secondary prevention trials have consistently shown the efficacy of implantable cardioverter defibrillators in preventing sudden cardiac death and life-threatening arrhythmias compared with anti-arrhythmic agents alone. According to guidelines published in 2008, 1 the implantable cardioverter defibrillator is now the treatment of choice not only for patients with documented life-threatening arrhythmias but also for patients with impaired cardiac function (ejection fraction <35%), regardless of previous arrhythmic episodes.
However, as an increasing number of patients have received implantable cardioverter defibrillators, several device-related problems have surfaced. 2 Although most patients adapt fairly well to living with an implantable cardioverter defibrillator over time, a significant proportion will experience psychological problems, with estimates reaching up to 38% for clinically significant anxiety. 3 Young age (<50 years), female gender, poor device understanding, and experiencing multiple implantable cardioverter defibrillator shocks are important risk factors for the development of psychological problems in these patients. 3
Psychological and emotional well-being in implantable cardioverter defibrillator patients are important for several reasons. Anxiety and depression can contribute to cardiovascular mortality and morbidity of patients with coronary heart disease, 4,5 and emotional 6,7 and mental 8 stress can have a detrimental effect on cardiac perfusion and function. Reduced heart rate variability, 9,10 impaired baroreflex control, 11,12 and alterations in the coagulation system 13 have been considered as possible mechanisms for the negative effect of anxiety and depression on cardiac outcomes.
Although it is uncertain whether spirituality can have a positive impact on physical health in patients with cardiovascular disease, 14 current evidence suggests that it can protect these patients from emotional distress and improve their quality of life. Spiritual well-being appears to have a protective effect on depression in patients with heart failure, 15 and faith can play a role in the emotional health of individuals recovering from a stroke 16,17 or those with severe chronic disabilities. 18 In addition, pilot spiritual interventions and holistic rehabilitation programs addressing the spiritual needs of cardiac patients have shown promising results in improving the quality of life and psychological well-being of these patients. 19 –21
However, little is known about the possible role of spiritual well-being in buffering psychological distress in patients with implantable cardioverter defibrillators, despite several indications that the spiritual dimension has often been neglected in these patients. Although implantable cardioverter defibrillator carriers are often survivors of a cardiac arrest, have advanced heart failure, and have to face difficult end-of life decisions, the educational material provided to implantable cardioverter defibrillator patients typically addresses only the technical/educational aspects of the implantable cardioverter defibrillator experience while ignoring its emotional and spiritual dimensions. 22 Clinicians are often pressed for time and they are often not forthcoming in the discussion of end-of-life issues with their patients. 23
The purpose of this study was to evaluate whether better overall spiritual well-being can be associated with lower psychological distress in a group of outpatients who underwent implantable cardioverter defibrillator implantation.
Methods
Design and Population
We conducted a cross-sectional analysis on baseline data collected from 46 patients screened for participation in a pilot study of a mindfulness-based intervention for patients with implantable cardioverter defibrillators. The study was conducted at the university campus of the UMass Memorial Medical Center in Worcester, Massachusetts. All consecutive patients scheduled for an implantable cardioverter defibrillator-related procedure at the catheterization lab were screened for study eligibility within a month of the procedure. Patients were eligible if they were >21 years old, able to understand and speak English, and had access to a telephone; exclusion criteria included inability/unwillingness to give informed consent, signs of cognitive impairment, New York Heart Association functional class >III or otherwise clinically unstable, pending coronary bypass or heart transplantation, comorbid life-threatening conditions, and ongoing severe depression or psychosis. The Blessed Orientation Memory and Concentration test 24 was used to screen patients for cognitive impairment, and subjects with scores ≥10 were excluded. Screening for ongoing depression and psychosis was based on DSM criteria of major depressive disorder or psychosis as documented by the physician in the patient’s chart at the time of the most recent medical evaluation. All eligible patients received a letter inviting them to participate in the study, and once they expressed interest, a screening visit was scheduled. After confirmation of study eligibility and provision of informed consent, patients completed a series of self-administered questionnaires.
Psychological Distress
Psychological distress (outcome variable) was assessed using the Hospital Anxiety and Depression Scale (HADS). 25 This is a 14-item self-administered questionnaire with 2 subscales measuring anxiety and depression, with higher scores indicating greater psychological morbidity. The use of this questionnaire has been validated in cardiac patients 26 and is particularly useful in these patients since it focuses on cognitive symptoms of psychological distress instead of physical symptoms, which can be similar to those resulting from the underlying cardiac disease. A cutoff of 8 is used for the 2 subscales, while a cutoff score of 10 is usually recommended for the total score. Total scores of 10 or higher indicate the presence of psychological distress.
Spiritual Well-Being
The primary predictor variable was overall spiritual well-being, assessed using the Functional Assessment of Chronic Illness Therapy–Spiritual Wellbeing (FACIT-SWB). This is a 12-item self-reported measure of spiritual well-being that has shown high internal consistency, reliability, and convergent validity with other measures of religion/spirituality in individuals with chronic diseases. 27 This instrument includes 2 subscales measuring different domains of spiritual well-being—a meaning/peace subscale assessing to what extent an individual experiences peace, harmony, and a sense of meaning, and a faith subscale evaluating the extent to which a patient finds strength or comfort in his or her religious beliefs. The range for the total score is 0 to 48, with higher scores indicating greater spiritual well-being.
Demographic Characteristics and Other Covariates
Information was collected at baseline on patient demographic characteristics and medical history. Demographic characteristics were collected by means of self-reported questionnaires and included age, gender, income, marital status, education, and racial/ethnic background. Information on cardiac diagnosis; previous diagnosis of anxiety or depression; current use of β-blockers, anti-arrhythmics, anxiolytics, and antidepressants; indication for implantable cardioverter defibrillator implantation (primary vs secondary prevention); type and time since implantable cardioverter defibrillator procedure; prior implantable cardioverter defibrillator shocks; New York Heart Association class; and ejection fraction (End diastolic volume − End systolic volume/End diastolic volume from an echocardiogram or a ventriculogram) was gathered from the Medical Record. Functional status was measured using the physical limitation subscale of the Seattle Angina Questionnaire. 28 Patients were also asked to report the number of times they engaged in physical exercise and whether they met with any therapist or spiritual counselor during the previous 4 weeks.
Statistical Analysis
We conducted a preliminary analysis to evaluate the appropriateness of the model’s assumptions and assess correlations between covariates to avoid collinearity in the multivariate model. The distribution of baseline demographic and clinical characteristics was compared between patients with high (≥50th percentile for this population) and low (≤50th percentile) spiritual well-being using t test (or Wilcoxon) for continuous variables and 2-tailed Fisher exact test to compare proportions.
The association between psychological distress and spiritual well-being was assessed using linear regression models. Variables that can confound the association between spiritual well-being and psychological distress (age, gender, income, education, marital status, prior depression or anxiety, use of antidepressants or anxiolytics, cardiovascular disease severity, and functional status), showing an association with the outcome (P ≤ .10), were included in a multivariate linear regression model. Results are presented as unadjusted and adjusted β coefficients (with confidence intervals), where the null hypothesis was that β1 = 0. P values <.05 were considered to be statistically significant. All analyses were performed using STATA 10 (2007) statistical software (StataCorp, LP; College Station, TX).
Results
Forty-six outpatients (32 males, 14 females) aged 43 to 83 years (mean = 65 years) completed a series of questionnaires at the initial screening visit (Table 1). Eighty-five percent of the study sample was in New York Heart Association class II or higher, and the mean ejection fraction was 0.3 (SD = 0.13). Half of the participants had psychological distress scores higher than 10, the threshold indicating the presence of psychological distress. The mean spiritual well-being score was 35 ± 8 (scale range = 0-48). No patient reported to have met a spiritual counselor during the previous month, and 13% reported meeting with a therapist or social worker.
Baseline Demographic and Clinical Characteristics of the Study Sample a
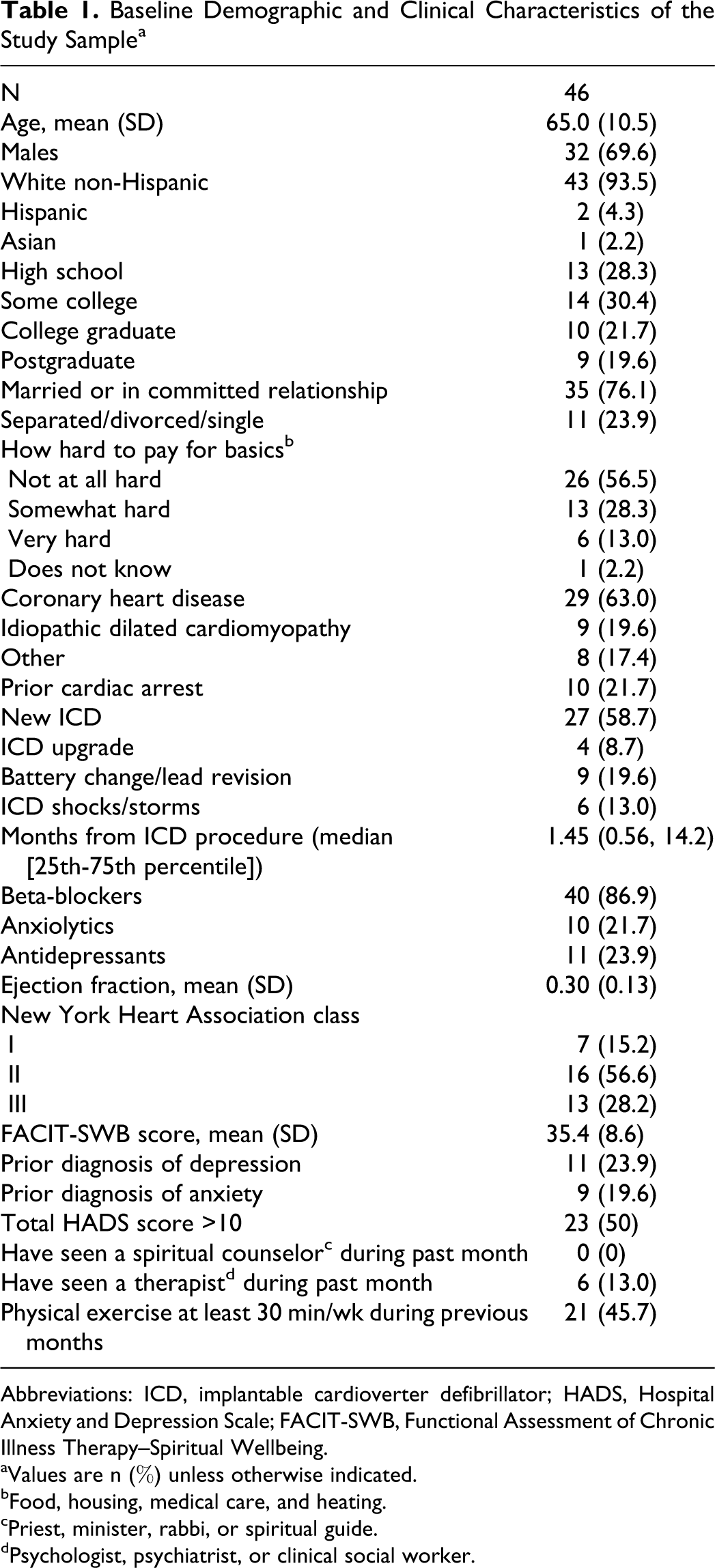
Abbreviations: ICD, implantable cardioverter defibrillator; HADS, Hospital Anxiety and Depression Scale; FACIT-SWB, Functional Assessment of Chronic Illness Therapy–Spiritual Wellbeing.
aValues are n (%) unless otherwise indicated.
bFood, housing, medical care, and heating.
cPriest, minister, rabbi, or spiritual guide.
dPsychologist, psychiatrist, or clinical social worker.
Patients with spiritual well-being scores above the 50th percentile (Table 2) had significantly lower psychological distress scores as well as a lower prevalence of psychological distress compared with patients with spiritual well-being scores below the 50th percentile. Although most differences were not statistically significant due to the relatively small sample size, they were also older, more frequently married, less educated, and had a lower prevalence of a prior diagnosis of anxiety or depression and of use of antidepressants or anxiolytics, while the severity of clinical conditions did not differ between groups as indicated by similar mean ejection fraction values and prevalence of prior cardiac arrest and implantable cardioverter defibrillator shocks.
Baseline Sample Characteristics According to Spiritual Well-Being Status a

Abbreviations: ICD, implantable cardioverter defibrillator; CI, confidence interval; HADS, Hospital Anxiety and Depression Scale; FACIT-SWB, Functional Assessment of Chronic Illness Therapy–Spiritual Wellbeing.
aValues are n (%) unless otherwise indicated.
bWilcoxon or 2-sided Fisher exact test.
cHeating, groceries, and health insurance.
Table 3 shows the results of the unadjusted and adjusted linear regression models. Psychological distress scores were significantly and inversely associated with spiritual well-being scores (Figure 1). In multivariate models, spiritual well-being was significantly associated with lower psychological distress independently of demographics (model 2); of a previous diagnosis of anxiety or depression, use of anxiolytics or antidepressants and counseling (model 3); and of physical exercise or functional status (model 4).

Unadjusted association between overall psychological distress and spiritual well-being
Results of the Unadjusted and Adjusted Linear Regression Models Testing the Association Between Total HADS Scores and FACIT-SWB Scores
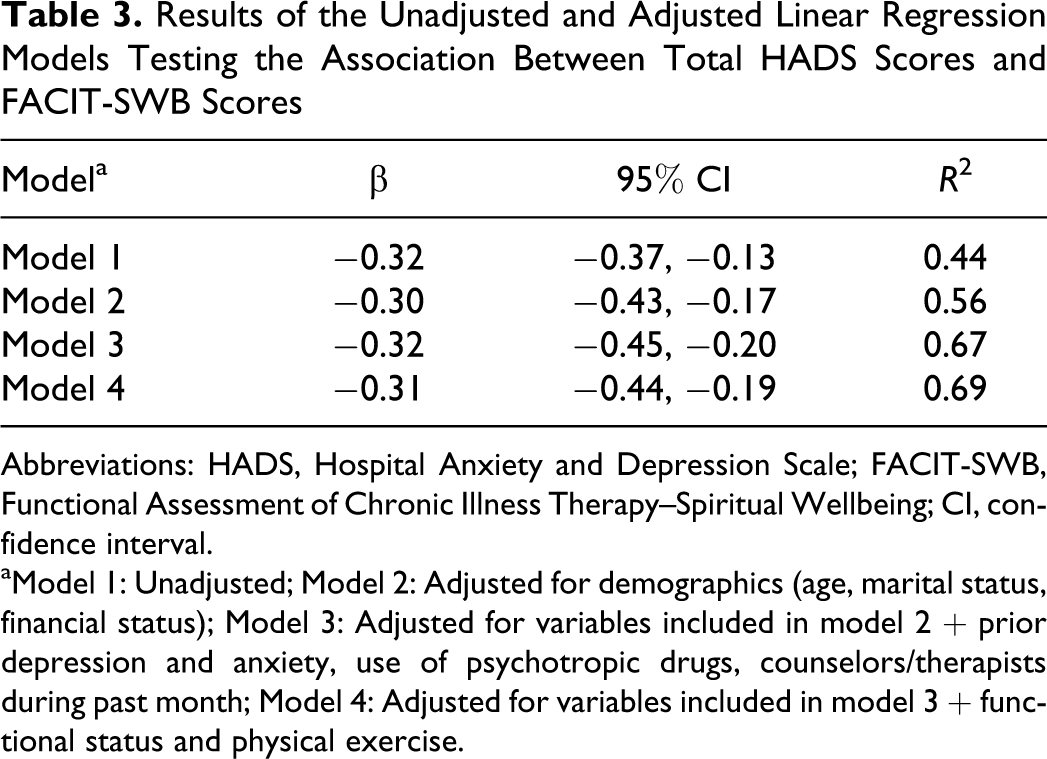
Abbreviations: HADS, Hospital Anxiety and Depression Scale; FACIT-SWB, Functional Assessment of Chronic Illness Therapy–Spiritual Wellbeing; CI, confidence interval.
aModel 1: Unadjusted; Model 2: Adjusted for demographics (age, marital status, financial status); Model 3: Adjusted for variables included in model 2 + prior depression and anxiety, use of psychotropic drugs, counselors/therapists during past month; Model 4: Adjusted for variables included in model 3 + functional status and physical exercise.
Discussion
Despite indications that spirituality is an important component of the psychological well-being of patients with severe chronic diseases, 29 –31 a limited number of studies have examined its characteristics in patients with cardiovascular disease. 15,16,32 A possible explanation for the limited interest in this topic in the cardiology literature is that spirituality is an elusive concept, encompassing both subjective dimensions that are difficult to define and operationalize, and more easily measurable, objective dimensions such as frequency of spiritual activities or spiritual/religious affiliation. 33
This is the first article describing the characteristics associated with spiritual well-being in patients living with an implantable cardioverter defibrillator and investigating the possible impact of spiritual well-being on the self-reported psychological health of these patients. In our study, patients with higher spiritual well-being had significantly less psychological distress and a lower prevalence of concurrent psychiatric morbidity and psychotropic drug use compared with patients with lower spiritual well-being. On the other hand, clinical conditions and functional status were similar between the 2 groups, suggesting that differences in psychological well-being were independent of the severity of the cardiac condition. There was an inverse linear relationship between psychological distress scores and spiritual well-being scores that persisted after taking into account a number of possible confounding variables.
The limited data currently available describing the role of spiritual well-being in patients with chronic cardiovascular disease is typically based on patients with advanced heart failure. These studies, usually qualitative or cross-sectional in nature, have shown the centrality of spirituality in the life of patients and caregivers alike 34,35 and its association with better quality of life 36 and adjustment to advanced heart failure. 37
Our results are consistent with those of a cross-sectional analysis showing a strong inverse association between spiritual well-being and depression in 60 patients with heart failure, independent of gender, income, social support, physical symptoms, and health status. 15 This is not surprising, considering that implantable cardioverter defibrillator patients usually have concomitant heart failure, and in fact, 85% of our patients were in New York Heart Association class II or III. One important addition of our article to the current literature is that we adjusted for other important confounders such as comorbid depression or anxiety, psychotropic medications, and ongoing psychosocial support. Furthermore, patients with implantable cardioverter defibrillators are somewhat unique among patients with heart failure, in that they often have experienced a cardiac arrest (21% of our population) and usually have more severe cardiac conditions.
Several limitations need to be kept in mind in interpreting the results of the present study. The first concerns our choice of the instrument to assess spiritual well-being. The FACIT-SWB is a measure of spiritual well-being, and not of spirituality, and has been criticized because of the overlap with measures of psychological well-being. 30,38 However, the finding of an inverse association between spiritual well-being and psychological distress has been consistently reported in various populations using different measures of spirituality and psychological distress. 30,39 Furthermore, in our analysis the association between spiritual well-being and psychological distress was still evident after we accounted for psychological comorbidity, use of psychotropic medications, and support from therapists, thus suggesting that spiritual well-being can uniquely contribute to reducing overall psychological distress. An additional limitation is that we limited our assessments to one dimension of spirituality, namely its emotional aspects, while we did not address other components such as affiliation or frequency of spiritual practice. Moreover, due to the cross-sectional nature of this study, resulting in the assessment of spiritual well-being and psychological distress at the same point in time, we cannot draw conclusions about the direction of this association. We also cannot exclude the possibility of selection bias, since this analysis was conducted on data collected as part of the baseline assessments of patients screened for participation in a pilot randomized clinical trial. The prevalence of anxiety and depression in our study, however, is consistent with that reported in similar studies of implantable cardioverter defibrillator outpatients. 3,40 The vast majority of our study population was white, and our findings cannot be generalizable to minority populations in which dimensions of spirituality other than spiritual well-being, such as attendance at worship services or spiritual beliefs, could be more relevant.
In conclusion, spiritual well-being was independently associated with lower psychological distress in a group of outpatients with implantable cardioverter defibrillators. These findings need to be confirmed in larger and more diverse populations and using a prospective design to evaluate whether the protective effect of spiritual well-being on psychological distress is maintained over time. In consideration of the possible unique contribution of spiritual well-being to the overall psychological health and quality of life of patients with implantable cardioverter defibrillators, the spiritual/existential dimension of the experience of living with an implantable cardioverter defibrillator should probably receive more attention in the care of these patients.
Footnotes
Acknowledgements
We would like to thank all participants for their contribution to this study; we would also like to thank Mary Stanley, MS, NP, and Karen Rose, MS, NP, for their help with recruitment.
Author Contributions
Elena Salmoirago-Blotcher designed the study, collected the data, conducted the data analysis, and wrote the manuscript draft; Sybil Crawford provided statistical advice and revised the manuscript; Chau Tran contributed to the study design and data collection; Robert Goldberg, Ira Ockene, and Lawrence Rosenthal revised the manuscript. All authors approved the final version of the manuscript for publication.
Authors’ Note
This study has been accepted as a poster presentation at the annual conference of the Society of Behavioral Medicine (New Orleans, April 2012).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by a grant of the National Center of Complementary and Alternative Medicine (F32AT005048). Elena Salmoirago-Blotcher is funded by a grant from the National Center for Complementary and Alternative Medicine (NCCAM F32AT005048).
Ethical Approval
The study protocol and all study materials were approved by the Committee for the Protection of Human Subjects at the University of Massachusetts Medical School (Docket H-13078).