
Abstract
The characteristics of dispositional mindfulness have rarely been explored in unhealthy populations. The authors sought to evaluate its association(s) with psychological morbidity and disease severity in 30 outpatients with implantable cardioverter defibrillators who were naïve to mindfulness training. They used the Five Facets of Mindfulness and the Hospital Anxiety and Depression Scale to measure dispositional mindfulness and anxiety/depression, respectively. Associations were estimated using linear regression models. Higher dispositional mindfulness was observed in patients with lower anxiety scores (β = −1.10, CI = −1.71, −0.49) and no history of depression (β = −7.95; CI = −14.31, −1.6) by univariate analysis. No associations were observed with disease severity or other covariates. In conclusion, psychological well-being and psychological morbidity, and not disease severity, appear to be associated with dispositional mindfulness in patients with implantable cardioverter defibrillators. Further research is needed to confirm these findings.
Accepted for publication March 8, 2011.
Keywords
Introduction
The practice of mindfulness has been central to Eastern philosophies for centuries. In these traditions, the cultivation of mindfulness is an important component of a path leading to a reduction of suffering and an increase in qualities such as compassion, equanimity, and wisdom. In Western medical settings, mindfulness practice has been shown to reduce anxiety, depression, sleep disturbance, and a variety of physical symptoms in different medical conditions, 1 such as cancer,2–5 chronic pain,6,7 anxiety disorders, 8 rheumatoid arthritis, 9 and fibromyalgia, 10 with an estimated effect size of around 0.5.1,11 When associated with cognitive behavioral therapy, mindfulness training reduces the rate of relapse/recurrence in major depression. 12
Although the current evidence for a beneficial role of mindfulness training on physical and psychological health has been fairly well established, very limited work has been done to investigate whether the ability to be mindful in everyday life13,14 (ie, dispositional or trait mindfulness) is associated with better psychological and physical well-being in individuals who were never exposed to formal mindfulness training. In fact, although dispositional mindfulness can be purposely cultivated and enhanced through mindfulness practice, 15 it is not necessarily related to previous training.
Dispositional mindfulness has been linked with several personality and mood characteristics across diverse, generally healthy, populations. Negative correlations have been observed between dispositional mindfulness measured with the Mindful Attention Awareness Scale 13 and personality characteristics such as neuroticism (particularly with the facets of depression, self-consciousness, and angry hostility)13,16,17 and with self-reported aggressiveness and hostile attribution bias. 18 An inverse relationship has been shown with depression and anxiety. 13 Similar associations have been documented by Baer and colleagues19,20 and in a recent cross-sectional, population-based study 21 using the Five Facets of Mindfulness questionnaire. 22
Finally, Shapiro and colleagues 23 have shown that participants in a Mindfulness Based Stress Reduction program with higher levels of pretraining dispositional mindfulness had a better response to mindfulness training, with larger increases in mindfulness, subjective well-being, empathy, and hope and a larger reduction in perceived stress.
The studies of dispositional mindfulness mentioned above, however, have all been conducted in healthy individuals, and the characteristics of dispositional mindfulness have rarely been explored in populations with chronic diseases. In patients with cancer, higher preintervention mindfulness levels were associated with lower mood disturbance and stress. 13 The authors of this study noted that the baseline average mindfulness score in this group was higher than in other populations and hypothesized that the experience of cancer could lead patients to reconsider their view of life and to become more present focused. Patients receiving an implantable cardioverter defibrillator present some characteristics similar to those of cancer patients. Patients with implantable cardioverter defibrillator are facing a severe chronic disease and are, by definition, facing death, either because they are at risk of dying suddenly or because they survived a prior cardiac arrest. Thus, the purpose of this study was to evaluate the characteristics of dispositional mindfulness in a group of patients with severe cardiovascular disease who were naïve to mindfulness practices and specifically to investigate whether mindfulness is associated with indicators of disease severity and with psychological morbidity and well-being.
Methods
This study was a cross-sectional analysis of baseline data collected from 30 patients enrolled in a pilot randomized controlled trial of a mindfulness-based intervention for patients undergoing an implantable cardioverter defibrillator procedure and/or who had implantable cardioverter defibrillator–related events (shocks). The study was conducted at the university campus of the UMass Memorial Medical Center, Worcester, Massachusetts. All consecutive candidates to an implantable cardioverter defibrillator–related procedure were screened for study eligibility within a month of the procedure. Patients were eligible if they were age 21 years or older, able to understand and speak English, and had access to a telephone. Patients were excluded under the following conditions: inability/unwillingness to give informed consent; signs of cognitive impairment; New York Heart Association functional class >III, angina Canadian Cardiovascular Society class III and IV, or otherwise clinically unstable; pending coronary bypass or heart transplantation; comorbid life-threatening conditions; and ongoing severe depression or psychosis. Eligible patients received an interest survey and a letter inviting them to participate in the study. If the patient expressed interest, a screening visit was scheduled. After confirmation of study eligibility and provision of informed consent, patients completed a series of self-administered questionnaires.
Assessments
Mindfulness scores
Baseline and postintervention mindfulness scores were measured using the Five Facets of Mindfulness questionnaire,19,22 a self-report measure of mindfulness derived from a factor analysis of questionnaires measuring mindfulness in daily life. To reduce patient burden, we used a shortened version consisting of 15 items, each rated on a Likert scale ranging from 1 (never or very rarely true) to 5 (very often or always true), with total scores ranging from 0 to 75.
Study covariates
Information was collected on demographic characteristics (age, gender, income, marital status, education, and ethnicity) and on other variables that can affect dispositional mindfulness, such as previous history of anxiety and depression and related prescriptions; baseline anxiety and depression scores; disease-related characteristics such as ejection fraction, New York Heart Association functional class, and history of cardiac arrest; use of other (non-mindfulness-based) alternative therapies during the previous month; and physical activity. Demographic information, functional class, ejection fraction (obtained from the most recent echocardiogram or ventriculogram), and other clinical information were collected from the electronic version of the medical record. Anxiety and depression scores were each measured using the Hospital Anxiety and Depression Scale,24,25 a 14-item self-administered questionnaire with 2 subscales measuring anxiety and depression, with higher scores indicating greater psychological morbidity. Because in cardiac patients symptoms of the underlying cardiac disease can be similar to those resulting from the somatic manifestations of anxiety and depression, we chose the Hospital Anxiety and Depression Scale because it focuses on cognitive symptoms instead of physical symptoms. Its validity has been confirmed in both hospital settings and primary care,26–28 and a correlation between 0.6 and 0.8 has been reported between this scale and the Beck Depression Inventory and the State-Trait Anxiety Inventory. Information about the use of complementary/alternative therapies and physical activity during the previous month was collected through self-administered questionnaires.
Statistical Analysis
A preliminary analysis was conducted to determine the variability and distribution of mindfulness scores, to evaluate the appropriateness of the model’s assumptions, and to assess correlations between covariates to avoid collinearity in the multivariate model. Variables were checked for missing data and distribution, if continuous, and for counts, if categorical. Loess curves were used to examine and test linear versus nonlinear associations. Age, ejection fraction, time from implantable cardioverter defibrillator implantation, anxiety, and mindfulness scores were treated as continuous variables. Sex, race, financial status, marital status, education, use of antidepressants and anxiolytics, previous history of anxiety and depression, psychotropic and antiarrhythmic therapy, type of implantable cardioverter defibrillator implanted (biventricular vs ventricular), prior shocks, history of cardiac arrest or severe cardiac arrhythmia, New York Heart Association class, physical exercise, and use of other complementary therapies in the previous month were treated as categorical variables. Spearman’s ρ was estimated to evaluate correlations between mindfulness scores and continuous variables. Mean baseline mindfulness scores were compared across categories of noncontinuous variables using the t test; the Kruskal-Wallis test was used when the assumption of constant variance was not met. The association between mindfulness scores and the different variables was estimated in univariate linear regression models. Variables associated with the mindfulness scores with P ≤ .10 were then included in a multivariate linear regression model. Results are presented as β coefficients (with confidence intervals). P values <.05 were considered significant. All statistical analyses were performed using STATA 10 (2007) statistical software (StataCorp, LP; College Station, TX).
Results
Baseline data from 30 patients were available for this analysis. The baseline demographic and clinical characteristics of the study sample are presented in Table 1 . The average age at enrollment was 63.1 years (range = 46-78 years). Study participants were mostly men (70%), white, non-Hispanic (90.0%), and married or in a committed relationship (70%); 60% had less than a college degree, and 30% reported that it was somewhat hard to very hard to provide for basics such as heating, food, or health insurance. The most common diagnosis was coronary heart disease; cardiac function was usually compromised, with a mean ejection fraction of 0.31 (normal >0.50); 80% of participants were in functional class II or III. Also, 23% of patients had experienced a previous severe arrhythmia or cardiac arrest, and 20% had experienced a recent implantable cardioverter defibrillator shock; 23% were currently receiving anxiolytics, and 26.7% were on antidepressants, whereas 20% and 26.7% had a prior history of anxiety and depression, respectively. Four patients (13.3%) reported having used other integrative/alternative treatments such as expressive writing (2), reflexology (1), or meditation (1) during the previous month. The mean mindfulness score was 57.3 (standard deviation [SD] = 8.2; range = 38-75).
Baseline Characteristics of the Study Sample

Abbreviations: SD, standard deviation; ICD, implantable cardioverter defibrillator; FFM, Five Facets of Mindfulness.
a Values are n (%) unless otherwise indicated.
b Food, housing, medical care, and heating.
c Expressive writing, reflexology, or meditation (nonmindfulness).
Table 2 shows the mean baseline mindfulness scores by different clinical characteristics. Scores did not differ by demo graphic characteristics, prior shocks, or history of cardiac arrest and cardiac diagnosis. Mindfulness scores were higher in patients with a biventricular implantable cardioverter defibrillator (P = .057). Likewise, mindfulness scores were higher in patients with no history of depression (P = .016) or anxiety as well as in patients not taking antidepressants or anxiolytics. Finally, patients reporting to exercise at least for 30 minutes once a week during the previous month had higher mindfulness scores versus those not exercising (Figure 1). Mindfulness scores were significantly and inversely correlated with baseline anxiety (Spearman ρ = −0.57; P = .0005) and depression scores (Spearman ρ = −0.37; P = .04), whereas there was no association with age (Spearman ρ = 0.09; P = .61), ejection fraction (Spearman ρ = −0.06; P = .73), and time since implantable cardioverter defibrillator procedure (Spearman ρ = 0.13; P = .50).
Mean Values a of FFM Scores by Baseline Characteristic
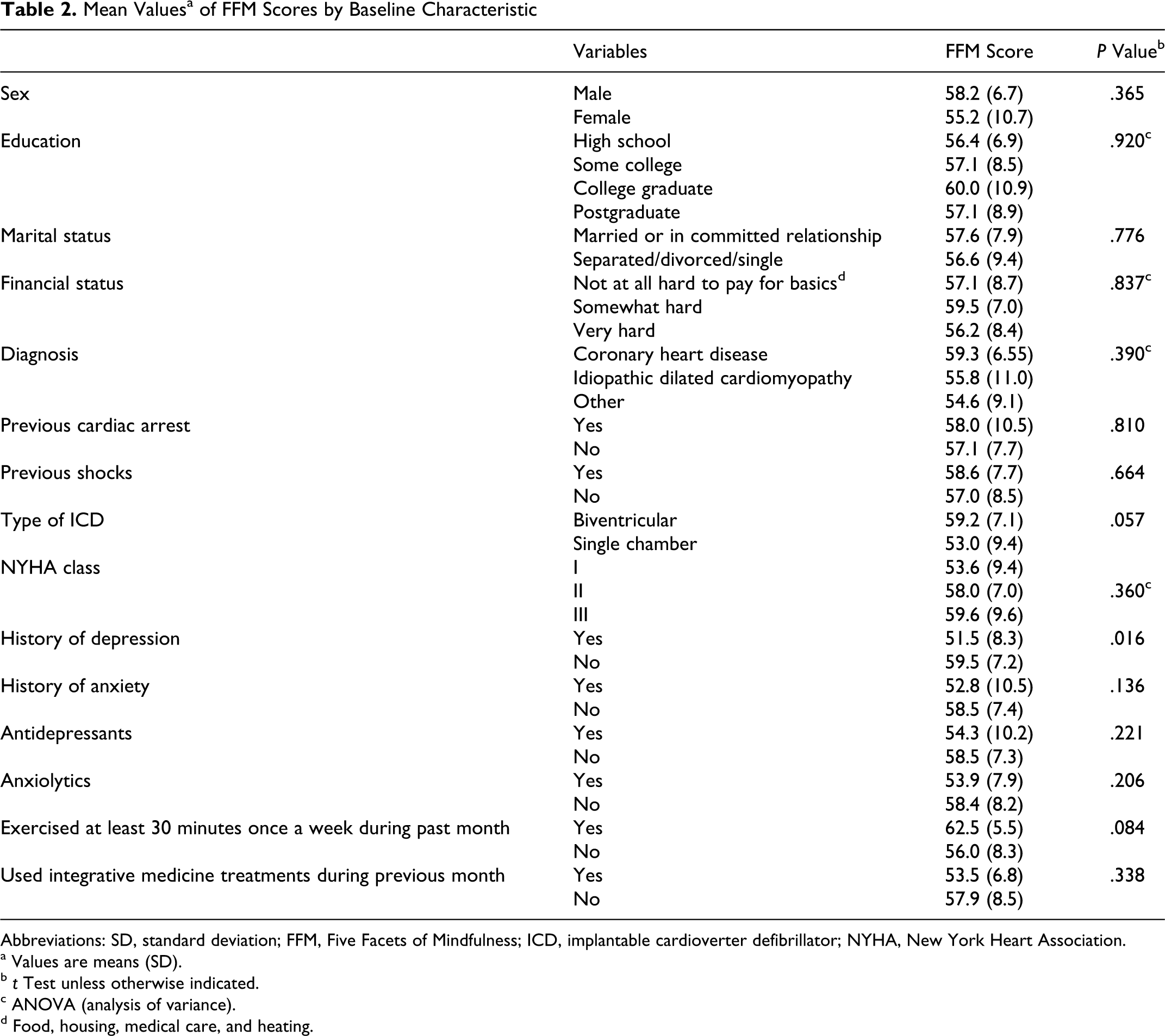
Abbreviations: SD, standard deviation; FFM, Five Facets of Mindfulness; ICD, implantable cardioverter defibrillator; NYHA, New York Heart Association.
a Values are means (SD).
b t Test unless otherwise indicated.
c ANOVA (analysis of variance).
d Food, housing, medical care, and heating.

Mean mindfulness scores by physical activity condition (at least 30 minutes once a week)
Consistent with the above results, in univariate linear regression models (Table 3), baseline mindfulness scores were significantly and inversely associated with baseline anxiety scores (P = .001), with a previous diagnosis of depression (P = .016), and positively associated with type of implantable cardioverter defibrillator implanted (biventricular vs single chamber; P = .057). Baseline mindfulness scores were not associated with age, gender, race/ethnicity, marital status, education, financial status, smoking, ejection fraction, previous cardiovascular procedures, previous cardiac arrest or severe arrhythmia, cardiac diagnosis, time from implantable cardioverter defibrillator procedure, previous implantable cardioverter defibrillator shocks, current use of antiarrhythmics or β-blockers, and use of other complementary/alternative therapies during the past month. There was a positive, nonsignificant association between mindfulness scores and exercise and New York Heart Association class, and an inverse relationship between mindfulness scores and history of anxiety and baseline depression scores.
Univariate and Multivariate Associations With FFM Scores a

Abbreviations: FFM, Five Facets of Mindfulness; CI, confidence interval; HADS, Hospital Anxiety and Depression Scale; ICD, implantable cardioverter defibrillator.
a F(4, 25) = 4.44; probability > F = 0.0076; R2 = 0.4152 (multivariate model).
b Walking or golfing.
Next, a multivariate model was generated that included all the variables that were associated with the outcome with P ≤ .10 in univariate models (Table 3). Psychological variables were highly correlated, and to avoid collinearity, only covariates showing the strongest associations with the outcome in univariate models were included. In the multivariate model, no variable appeared to be independently statistically significantly associated with mindfulness scores (P = .054 for the association between anxiety and mindfulness scores).
Discussion
In this group of patients with severe cardiovascular disease and depressed heart function who underwent implantable cardioverter defibrillator implantation or received recent shocks, dispositional mindfulness was inversely associated with a previous diagnosis of depression and current anxiety symptoms. Associations with other psychological variables (ie, use of antidepressants and anxiolytics, previous anxiety, and current depression scores), although not reaching statistical significance, were in the expected direction—that is, they were inversely associated with dispositional mindfulness—supporting the hypothesis of an inverse association between dispositional mindfulness and negative mind states, in agreement with other studies.13,17,20–22 Dispositional mindfulness was inversely associated with not only self-reported current anxiety and depression scores, which could be dependent on current circumstances such as the implantable cardioverter defibrillator procedure and the recent hospitalization, but also with a prior diagnosis of anxiety and depression.
In univariate models, patients with more severe cardiovascular symptoms tended to show higher dispositional mindfulness, as indicated by the increased mindfulness scores in patients with higher functional class and in those receiving a biventricular implantable cardioverter defibrillator. Biventricular implantable cardioverter defibrillators are usually implanted in patients with more severe heart failure symptoms (ie, patients having an ejection fraction less than or equal to 35%, a QRS duration greater than or equal to 0.12 s, sinus rhythm and New York Heart Association functional class III or IV).29–31 Two hypotheses can be proposed to explain this finding. First, because implantable cardioverter defibrillator patients are usually educated by their providers to pay attention to physical symptoms (such as chest pain, palpitations, or shortness of breath) that could signal a worsening of their conditions, they learn to be more conscious of physical sensations and, in general, to pay more attention to what unfolds in the present. Alternatively, patients could have become more aware of the value of their lives and learned to appreciate the present similarly to what was reported in a study of cancer patients. Higher psychological and interpersonal growth has been reported in survivors of stem cell transplantations compared with healthy volunteers. 32
Dispositional mindfulness was not associated with a history of previous shocks and cardiac arrest—namely, in this group of patients, exposure to conditions close to a near-death experience did not result in an increased attitude to be mindful in everyday life. However, the study was not powered to detect this association, and the number of patients with a history of shocks (6/30) or who received an implantable cardioverter defibrillator following a cardiac arrest (7/30) was low.
Finally, one interesting preliminary finding is worth mentioning. Mindfulness scores were higher in patients who exercised at least once a week compared with patients who did not (62.5, SD = 5.5 vs 56.0, SD = 8.3; P = .08; Figure 1). Physical exercise in the form of light yoga exercises is a component of the Mindfulness Based Stress Reduction program,6,33 the most popular and world-renowned mindfulness-based intervention. Self-reported yoga practice has been associated with positive changes in mindfulness during Mindfulness Based Stress Reduction training. 34 If physical activity is positively associated with mindfulness levels, it might contribute to the increase in mindfulness observed at the end of such training, which in turn could exert its beneficial effects on psychological and physical well-being.15,35,36 An alternative explanation is that these patients could have paid close attention (been mindful) to their bodily sensations while they were exercising because of the underlying heart conditions. However, this association was of borderline statistical significance, and it deserves further investigation in larger populations.
The most notable strength of this preliminary study is that this is the first study describing the characteristics of dispositional mindfulness in patients with severe cardiovascular disease. Second, the study sample was selected from a “real-life” diverse population of consecutive candidates to implantable cardioverter defibrillator procedures and/or with implantable cardioverter defibrillator shocks and, thus, very different from the highly educated, high-socioeconomic-status, and mostly female population usually accessing mind–body programs. 37 However, there are also several limitations. First, because of the small sample size, this study was not powered to detect associations with less frequent events such as previous cardiac arrest or shocks and to examine associations with the specific facets of mindfulness measured by the Five Facets of Mindfulness questionnaire. Second, we studied a highly selected population, and the study findings cannot be generalized to patients with other diseases. Third, although the study was proposed to all consecutive implantable cardioverter defibrillator candidates, it cannot be excluded that only highly motivated participants joined the study and that because of social desirability or other factors, they may be more prone to report higher or different levels of mindfulness compared with patients who did not participate. Fourth, dispositional mindfulness was self-reported. This is a common limitation of studies assessing the effect of mindfulness training. In fact, despite recent evidence that mindfulness is an important mediator of the effect of mindfulness interventions on anxiety and other psychological outcomes,15,35,36 adequate definitions of mindfulness are often not provided, and when provided, they are either inconsistent or overlapping across studies. 38 Objective criteria for the measurement of mindfulness are currently unavailable, and although several self-report instruments were developed to measure this construct,13,19,20,39,40 correlations across different scales are modest, 41 further complicating the comparison of results across studies. It is likely that the meaning of some items in mindfulness inventories (including the one used for this study) may have quite a different meaning in mindfulness-trained participants and in patients such as the ones enrolled in this study who were never exposed to mindfulness training. 38
Finally, because this was a cross-sectional analysis, the direction of the association could not be established—that is, whether enhanced dispositional mindfulness leads to an improved emotional well-being or if the mind’s absorption in the powerful struggles and emotions accompanying anxiety and depression is limiting its natural capacity of attending to the present.
In conclusion, current psychological well-being and prior psychological morbidity, and not indicators of disease severity such as prior cardiac arrest or shocks, appear to be more strongly associated with dispositional mindfulness in patients with implantable cardioverter defibrillators who did not receive previous mindfulness training. Further research in larger populations is needed to confirm these findings, which may help shed further light on the mechanism of the beneficial effects of mindfulness training on health outcomes.
Footnotes
Acknowledgments
This study was partially supported by a grant of the National Center of Complementary and Alternative Medicine (F32AT005048). We would like to thank Mary Stanley, MS, NP, and Karen Rose, MS, NP, for their help with recruitment.
Elena Salmoirago-Blotcher designed the study, collected the data, conducted the data analysis, and wrote the manuscript draft; Sybil Crawford provided statistical advice and revised the manuscript; James Carmody contributed to the study design and the interpretation of the data and revised the manuscript; Ira Ockene and Lawrence Rosenthal contributed to the study conception and revised the manuscript. All authors approved the final version of the manuscript for publication.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Elena Salmoirago-Blotcher is supported by a grant of the National Center of Complementary and Alternative Medicine (F32AT005048).
The study protocol and all study materials were approved by the Committee for the Protection of Human Subjects at the University of Massachusetts Medical School (Docket H-13078).