
Abstract
The Naturopathic Patient Database is a data management tool developed by the Canadian College of Naturopathic Medicine to collect patient data from its teaching clinic, the Robert Schad Naturopathic Clinic. This study investigated how type 2 diabetes mellitus was managed at the Robert Schad Naturopathic Clinic from May 2009 to February 2011. Cases of type 2 diabetes mellitus from the Robert Schad Naturopathic Clinic reported in the Naturopathic Patient Database were extracted based on an International Classification of Diseases, 10th revision code assessment of E11 (non-insulin-dependent diabetes mellitus) and files were audited. The American Diabetes Association 2010 standards of medical care in diabetes were used as guidelines for the audit. Multiple categories in diagnosis, physical exam, laboratory tests, and management were graded on a 0 to 2 scale. The average audit score was 55.5/90. The most common interventions being used are diet and aerobic exercise, followed by supplements (omega-3 fatty acids) and botanicals. These data suggest that the American Diabetes Association standards of care for type 2 diabetes mellitus are not followed stringently. Education and creation of a naturopathic standard of care may improve audit performance and patient outcomes.
Type 2 diabetes mellitus is a multifactorial disease, primarily characterized by a decreased response to insulin. The World Health Organization (WHO) calculated the worldwide prevalence of diabetes in 2000 to be 2.8% and anticipates that this number will double in the next decades. 1 The World Health Organization has also affirmed that diabetes causes approximately 5% of all deaths globally each year. 2 In Canada alone, the cost associated with type 2 diabetes mellitus in 2000 was more than CAD $4 billion dollars, 3 and it was almost CAD $6 billion dollars in 2005. 4 Because of the rapidly rising prevalence of type 2 diabetes mellitus, the Canadian Diabetes Association estimates that by 2020, diabetes will cost the Canadian health care system more than CAD $16 billion dollars. 5 The total burden caused by diabetes also inflicts additional costs because of lost productivity, lost work days, mortality, and permanent disability. 6
The largest contributing factors that increase the risk of type 2 diabetes mellitus are excessive caloric intake and a sedentary lifestyle, leading to obesity. 7 The interventions that reverse or improve these factors, including weight loss through diet and exercise, have been demonstrated to have a beneficial effect in the treatment of type 2 diabetes mellitus. 8 For this reason, these interventions are advocated by the American Diabetes Association as first-line therapies in all diabetes management plans. 9 However, several studies indicate that many patients with type 2 diabetes mellitus still do not receive the recommended care. 10 Structured self-monitoring of blood glucose and patient self-management behaviors improves metabolic outcomes in patients with type 2 diabetes mellitus. 11 Because effective care for type 2 diabetes mellitus requires that certain habits be maintained for long-term periods, self-care is a continuous challenge. The physician’s ability to provide memorable information has been shown to improve self-care habits, even after controlling for patient socioeconomic status and medical condition. 12 However, physician time is costly, and a cost-effective solution might be to encourage patient referrals to alternative providers for evaluation, treatment, and management.
In 1 study, more than 60% of all physicians had made referrals to alternate providers at least once in the preceding year, and 38% had referred in the preceding month. 13 The demand for complementary and alternative medicine among people with diabetes is high. Most referrals are based on patient requests or the failure of conventional treatments. Many studies have shown that a high proportion of diabetes patients use complementary and alternative medicine, ranging from one third 14 to more than 70% in some studies. 15
One type of complementary and alternative medicine therapy that patients with type 2 diabetes mellitus use is naturopathic medicine, but the quality of the care being provided is not well documented. Naturopathic medicine is a distinct whole-system approach to medicine that blends classic healing traditions with current scientific research. 16 Common therapies used include diet, nutritional/botanical supplementation, counseling, health and disease education, acupuncture, physical medicine, hydrotherapy, and homeopathy. Many naturopathic treatments have shown benefit in the treatment of diabetes. 17 Some naturopathic treatments have also shown promise for comorbidities associated with diabetes, such as α-lipoic acid in the treatment of peripheral neuropathy. 18 There are limited studies on the safety of naturopathic medicine as a whole, but standards have been set for the education, training, licensing, and regulating of naturopathic doctors, at least in Ontario, Canada. 19 In Canada, 5 provinces are regulated, and in the United States, 15 states are regulated. 20 Safety has also been demonstrated in the context of specific pathologies, including anxiety, 21 multiple sclerosis, 22 and menopausal symptoms. 23 There are also limited studies on the comparative cost of naturopathic medicine, but those that are available suggest that naturopathic medicine is cost-effective, at least for certain conditions.24,25
Clinical audits and feedback are useful tools for improving the quality of care in professional practice. 26 When baseline adherence to recommended practice is low, the effectiveness of audits increases. For the management of diabetes in particular, audits have been shown to improve rates of laboratory testing such as glycated hemoglobin and lipid profiles, enquiries about smoking, eye screening rates, foot examinations, and prescription rates. 27 Once the audit results were provided for the doctors, more patients achieved targets for blood pressure, glycated hemoglobin, and low-density lipoprotein cholesterol.
The Naturopathic Patient Database is a data management tool developed by the Canadian College of Naturopathic Medicine to collect patient data from its teaching clinic, the Robert Schad Naturopathic Clinic. Patient care is delivered by student interns in their fourth and final year of the Naturopathic Doctor program, and overseen by experienced, licensed naturopathic doctors. This database was created in 2006 and has evolved to meet the various academic and research needs of the Canadian College of Naturopathic Medicine. This study investigated how type 2 diabetes mellitus is managed at the Robert Schad Naturopathic Clinic for the purposes of auditing clinical care provided in the context of a teaching clinic and ultimately improving patient care. This is the first audit done at the Robert Schad Naturopathic Clinic that has focused on type 2 diabetes mellitus.
Materials and Methods
Setting
The audit was performed in the Robert Schad Naturopathic Clinic, which operates clinic shifts for 8 to 10 hours a day, 6 days a week. Approximately 130 fourth-year naturopathic interns directly see patients in 1-on-1 settings. These clinic interns are supervised by 45 licensed naturopathic doctors. Located in the Greater Toronto Area, the Robert Schad Naturopathic Clinic provides health care for a large and diverse patient population and services approximately 25 000 patient visits annually. The clinic houses approximately 40 treatment rooms, including a hydrotherapy suite that contains peat baths and sauna rooms. The Robert Schad Naturopathic Clinic is advertised as a primary care clinic but also operates 3 focus shifts for sports medicine, pediatrics, and cancer care. The prevalence of diabetes in the patient population of Robert Schad Naturopathic Clinic is unclear; this is one of the rationales for ongoing development of the Naturopathic Patient Database. The Naturopathic Patient Database provides a snapshot of patient encounters, and based on files that were entered in the Naturopathic Patient Database, patients with type 2 diabetes mellitus represent approximately 3% of all patients seen at the Robert Schad Naturopathic Clinic.
Methods
The Research Ethics Board of the Canadian College of Naturopathic Medicine provided ethical oversight of this project. A core audit form was created and pilot tested to assess the quality of naturopathic care for patients with type 2 diabetes mellitus in the Robert Schad Naturopathic Clinic. The American Diabetes Association 2010 standards of medical care in diabetes were used as guidelines, 28 this being the most recent and comprehensive guideline at the time of the audit. The American Diabetes Association guidelines are similar to the Canadian Diabetes Association guidelines that were released in 2008. 29 However, the American Diabetes Association guidelines are better suited for a clinical audit because the association is accountable to a much larger comparable population and has synthesized the clinical targets used by other audits, allowing for a comparison of results. 30
Multiple categories in diagnosis, physical exam, lab tests, and management were graded on a 0 to 2 scale. Criteria being assessed that were applicable to all cases included but were not limited to inquiring about current medications, obtaining a detailed history of complications, measuring blood pressure, palpating the thyroid, performing fundoscopy, doing a foot exam, obtaining laboratory test results for glycated hemoglobin and lipid profiles, providing referrals to medical doctors, setting appropriate treatment goals, and using evidence-based prescriptions. Additional American Diabetes Association guidelines only apply to specific patient populations, and as such, audit criteria were adapted to be used when applicable. These included but were not limited to referral for bariatric surgery if body mass index was more than 35, recommendation for statin therapy if the patient was older than 40 years with at least 1 cardiovascular risk factor, and recommendation for insulin therapy if the fasting plasma glucose level was more than 10 mmol/L.
Finally, audit criteria that focused on naturopathic interventions and their doses were also assessed. These included the recommendations for various supplements, botanicals, physical medicine, homeopathy, traditional Chinese medicine, or therapeutic counseling. The Measure Yourself Medical Outcome Profile was used as a universal outcome measure of effectiveness of individualized patient-defined symptoms in addition to these audits. 31
Patient data in the Naturopathic Patient Database are entered by clinic interns only when they have seen a patient for at least 3 visits at the Robert Schad Naturopathic Clinic. The information entered in the Naturopathic Patient Database contains comprehensive clinical information from the patient’s chart, divided into 4 areas: subjective, objective, assessment, and plan. However, because of delays in transcribing information from the patient chart into the Naturopathic Patient Database, a gap can exist between the more up-to-date chart and the repository of historical patient data in the Naturopathic Patient Database.
One auditor conducted a search of the Naturopathic Patient Database from May 2009 to February 2011 to identify patients assessed with type 2 diabetes mellitus. The assessment section of the Naturopathic Patient Database contains a column for diagnosis that uses the International Classification of Diseases, 10th revision coding system. 32 The inclusion criteria were such that all patients assessed with type 2 diabetes mellitus could be included, so that the audit could also capture a realistic representation of naturopathic care for those with comorbidities, as is often the case in patients with type 2 diabetes mellitus. 33 The International Classification of Diseases, 10th revision code for type 2 diabetes mellitus (E11) was used and was able to capture 37 patient cases out of a total of 1419 cases in this time frame. Audit scores were tabulated. A second auditor tabulated audit scores independently for 9 randomly selected cases as a quality control measure. The overall interrater agreement (κ value) was 0.78, indicating satisfactory agreement between auditors.
Results
Patient Characteristics
Figure 1 outlines results of the process for case selection for the audit. Of the 37 patient cases captured by the Naturopathic Patient Database, 8 cases (21.6%) lacked patient file number identifiers and so were unable to be acquired for audit purposes. The remaining 29 cases were obtained, and the patient files were critically appraised. The mean patient age was 60.6 years (±10.5 years), and female gender was more common (62%). None of the patients were smokers. Patients had, on average, 4 comorbidities (±1.7) as assessed by International Classification of Diseases, 10th revision coding. The most common comorbidities were hypertension, hyperlipidemia, and obesity. The average onset of type 2 diabetes mellitus was 8 years prior to the date of chart review, and based on available lab reports, the mean glycated hemoglobin at the start of the assessment period was 8.2% (±2.1). The mean duration of care that was directly assessed was 4.2 (±2.9) months. From an overall qualitative assessment, care being provided was predominantly adjunctive care rather than primary care.

Process for case selection for audit
Core Audit Scores
The mean core audit score was 55.5 (±15.0) out of a possible total of 90. There was no cutoff score used to determine what was considered adequate care. All audit items were placed into 1 of 6 categories and analyzed together to comment on major areas of clinical interaction. Table 1 outlines the criteria and raw data for each of the 6 core categories, Figures 2 , 3, and 4 are graphical representations of scores on the core and additional audit criteria. Figure 5 and Table 2 outline doses of the most commonly prescribed natural health products (ie, supplements).
Major Audit Categories and Scores

Abbreviation: HbA1c, glycated hemoglobin.
Mean Daily Doses and Standard Deviations for Common Prescriptions

Abbreviations: ALA, α lipoic acid; CoQ-10, coenzyme Q10.
a Unable to differentiate between Cinnamomum zeylanicum and C cassia.
Additional Audit Items
The additional audit items specific to the use of naturopathic treatments were scored individually. Over the duration of assessed care, the mean number of therapeutic interventions or therapeutic recommendations was 6.6 (±1.8). Other common therapies that were used that were not tracked in the additional audit were vitamin B12, bitter melon (Momordica charantia), and fenugreek (Trigonella foenum-graecum).
Traditional Chinese medicine and acupuncture were used in 4 patient cases to directly treat diabetes or the patient as a whole. Half of these cases used a traditional Chinese medicine diagnosis of Liver and Kidney Qi and Yin deficiencies. The other half of these cases did not specify a traditional Chinese medicine diagnosis. The most common acupuncture points used were SP6, ST36, KD3, and LV3. Within a given treatment, 5 to 10 points bilaterally were used. The mean number of treatments was 3.8 (±1.5), and treatments usually occurred once a week or once every 2 weeks, depending on the individual patient’s visit frequency. Only a single Chinese patent formula was prescribed (Jade Source Formula).
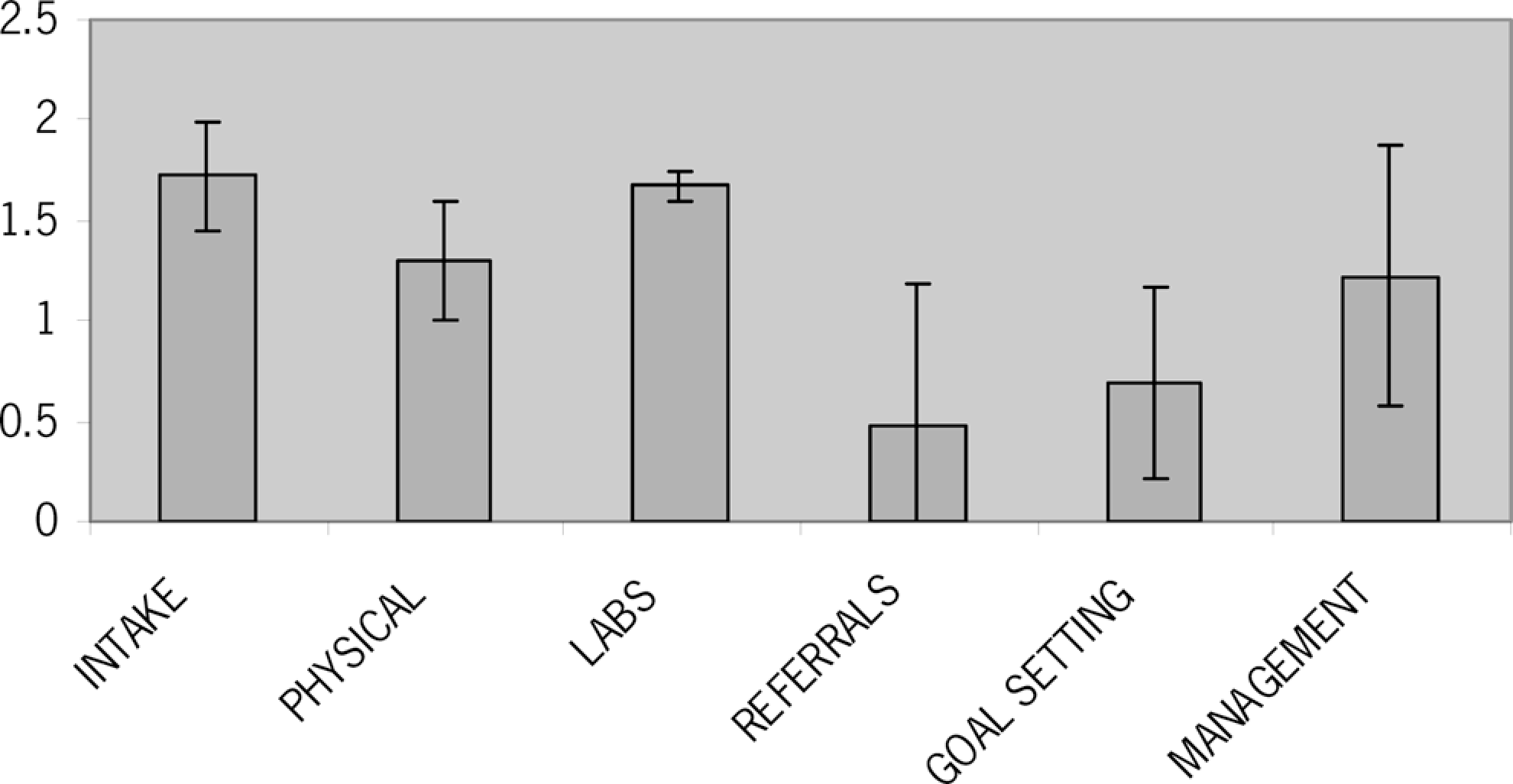
Average audit scores for major audit categories

Percentage of cases in which a therapy was prescribed

Percentage of cases in which specific supplements or botanicals were prescribed
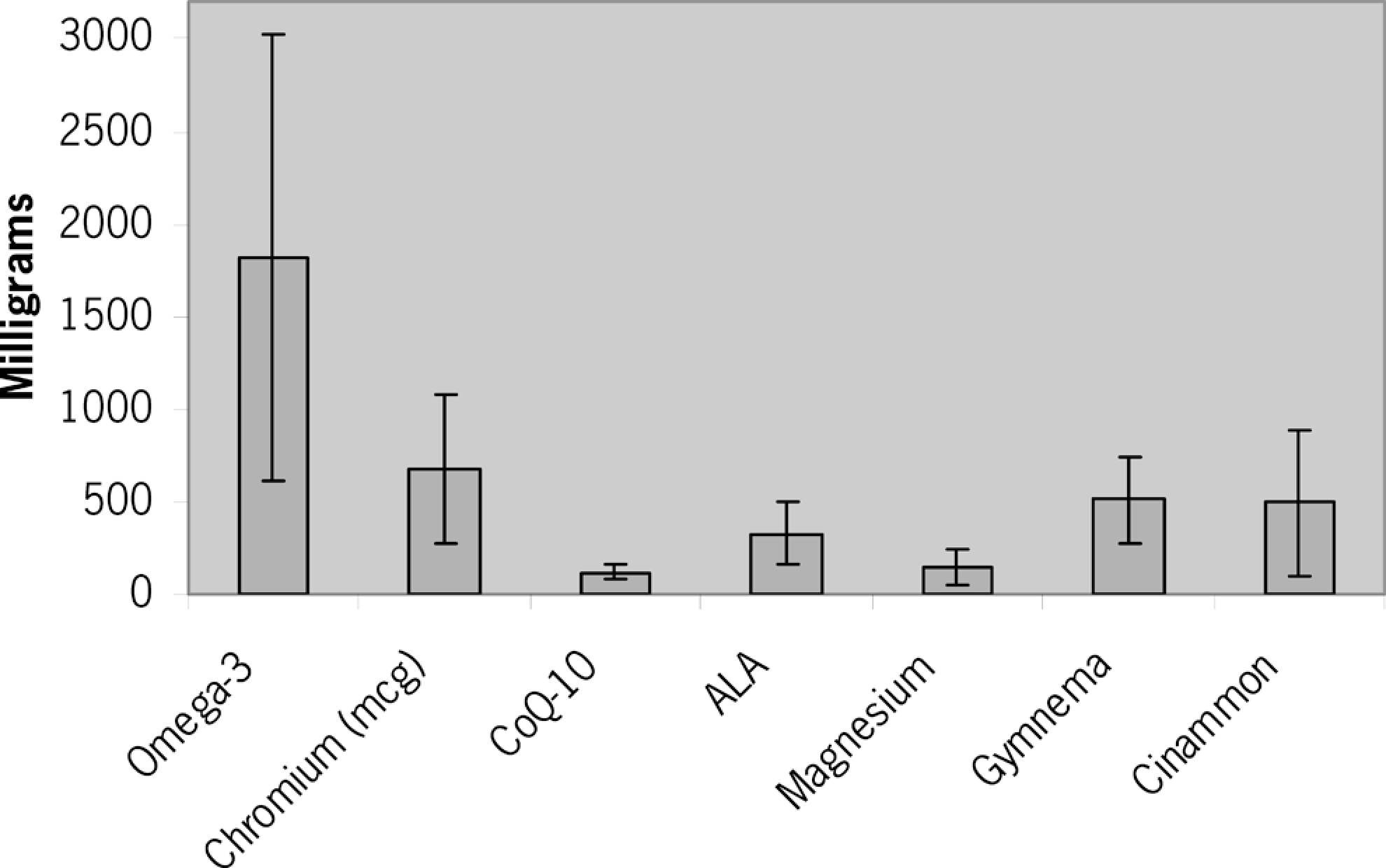
Daily doses used for common prescriptions
Naturopathic Patient Database Visits Omitted
An analysis was done looking at the amount of visits omitted in the Naturopathic Patient Database compared with the corresponding audit scores. The average number of visits omitted was 2.5. The audit scores remained relatively unchanged by the number of visits omitted (r 2 = 0.0007; Figure 6).

Audit score versus naturopathic patient database visits omitted
Lab Results
The mean number of lab reports available within a file over the duration of assessed care was 1.2 (±1.1). Of the patients assessed, 75.9% had at least 1 lab report available; 17.2% of patient files had no lab reports available and also contained no requests for lab work. When lab reports were not available, sometimes, other data were available, such as the patient’s self-monitored fasting glucose results.
In all, 7 patients had results available for more than 1 glycated hemoglobin level, allowing for a calculation of net change in glycated hemoglobin over the duration of care. For these patients, the mean change in glycated hemoglobin was a drop of 1.3% (±1.8). After the treatment period, 3 of these 7 patients (42.9%) could be reclassified as having achieved glucose control.
Measure Yourself Medical Outcome Profile Results
Only 7 files contained greater than 1 Measure Yourself Medical Outcome Profile questionnaire to allow for the tracking of subjective outcomes. A lower Measure Yourself Medical Outcome Profile value indicates a more desirable outcome. The symptoms that are tracked are subjective and generated by each individual patient. For the purposes of this study, only type 2 diabetes mellitus, a diabetic symptom, or a diabetic complication was tracked for Measure Yourself Medical Outcome Profile purposes. There were a total of 9 separate items tracked in these 7 cases. Examples included the tracking of “diabetes,” “blood sugar,” or “fatigue.” When comparing the first and last Measure Yourself Medical Outcome Profile scores for the applicable items, 6 items improved, 2 did not change, and 1 worsened (Table 3 ). The mean change for all items was an improvement of 2 points on the Measure Yourself Medical Outcome Profile Scale.
MYMOP Original and Final Values

Abbreviation: MYMOP, Measure Yourself Medical Outcome Profile.
Feedback
To facilitate dissemination, education, and improvement, audit findings were presented to clinical supervisors and to current interns at the earliest available time following analysis of results. A checklist was created to help guide interns in their first 3 visits with a diabetic patient and made available in both print and electronic format. An additional Grand Rounds presentation on diabetes 3 months following the initial education components included a breakdown and a reminder of the findings of the audit.
The 3 areas that were emphasized as needing improvement were the following: Physical exam: frequency of charting and presumably conduct of various aspects could be improved, including body mass index (BMI) calculation, fundoscopy, thyroid palpation, skin and foot exams, and measuring blood pressure at every visit. Patient referral: despite current limitations in the ability to formally refer (in other words, other health care providers are not obligated to accept the referrals), the documentation of recommendations to consult with other care providers (eg, optometrist, dentist, or medical doctor) when warranted could be improved. Goals: specific treatment goals (eg, glycated hemoglobin <7% or systolic blood pressure <130 mm Hg) are not being set, monitored, and reported in the chart.
Even though the management category scored lower than the physical exam category, it was not emphasized as needing much improvement. This choice was made because data on patient outcomes were extremely limited and because management had a larger standard deviation, whereas the physical exams were more consistently low scoring. It is also important to note that some of the subcategories within management included physical exams, which tended to score poorly. Thus, an improvement in physical exam scores would have more widespread implications.
Discussion
Core Audit
The audit scores evaluating patient intake were high (1.71 ± 0.27). Naturopathic interns spend up to 1 hour per visit with patients, resulting in ample opportunity to accumulate information. Additionally, the holistic style practiced by naturopathic doctors, which is emphasized by the academic institution, lends itself toward collection of comprehensive patient information. 34
The audit scores for lab tests were also high (1.67 ± 0.07), although this may be an artifact of how scoring criteria were adapted for these components of the American Diabetes Association guidelines. Currently, in Ontario, Canada, naturopathic doctors face difficulties in directly requisitioning lab tests that would normally be funded within the public health care system. Naturopathic doctors can usually obtain laboratory testing when their patients are comanaged by a medical doctor, and in these situations, patients must sometimes pay for the laboratory tests out-of-pocket. This creates a barrier for obtaining outcome measurements and for tracking patient progress. As a result, many patients choose to use the health care services of other providers, rather than absorbing the financial load of the laboratory tests. In light of this limitation, credit was given in the audit if an intern requested lab work from the patient or communicated directly with the patient’s medical provider using a release of records or medical note. Often, consistent laboratory test results were not captured, but the scoring criteria adapted for the audit did not penalize for this.
The 4 lowest scoring categories in the audit were a thorough physical exam, referring patient care, setting specific treatment goals, and patient management. The Robert Schad Naturopathic Clinic’s general screening form does not incorporate some of the physical exam recommendations recommended by the American Diabetes Association for type 2 diabetes mellitus. As such, interns may have been less likely to complete those elements of the physical exam that are tailored to type 2 diabetes mellitus patients.
Referring patient care scored poorly, in part, because in Ontario, naturopathic doctors do not have the ability to directly refer to other health care providers because they are not yet incorporated with other health care practitioners into the Regulated Health Practitioners Act. 35 This leads to an increased reliance on informal referrals, which may or may not service the needs of patients. Also, according to the American Diabetes Association, patients must be referred to many health care practitioners whose capabilities often overlap with those of naturopathic doctors. Naturopathic doctors have a wide scope of practice that includes nutritional counseling, and a large part of naturopathic treatment involves a focus on patient education. 36 The delivery of this type of information likely overlaps with many recommendations made by registered dieticians or obtained through a diabetes self-management education program. At the Robert Schad Naturopathic Clinic, patients are often seen on a frequent basis, thus improving the ability of naturopathic doctors to reinforce and clarify any educational prescriptions. As such, submitting naturopathic doctors to American Diabetes Association guidelines for these particular referrals may not be appropriate. In addition, it may not be cost-effective to use referrals in some circumstances. For example, in lower-risk patients, less-frequent eye screenings provide almost the same benefit as annual ones at a lower cost. 37
Setting specific treatment goals likely scored poorly, partly because the patients who are seen are often not identifying diabetes control as their primary concern. It may also relate to the fact that it is difficult to measure goals for which the outcomes are challenging to collect and monitor.
Additional Audit of Naturopathic Interventions
The most highly used therapies are diet (96.6%), supplements (93.1%), and aerobic exercise (82.8%). Diet and exercise are therapies that have been shown to be extremely beneficial for patients with type 2 diabetes mellitus. 38 Naturopathic dietary recommendations align with those that other providers would be prescribing (including low-carbohydrate or low-glycemic-index diets). 39 Nutritional and botanical supplements are useful prescriptions because they often combine many different vitamins, minerals, and herbs together in a single capsule or tablet. Keeping oral prescriptions simple tends to increase patient compliance. 40 Omega-3 fatty acids were frequently used (72.4%) for type 2 diabetes mellitus because they have been shown to lower triglycerides and very-low-density lipoprotein cholesterol in these patients. 41 Chromium was frequently used (58.6%) because it can cause a decrease in fasting glucose and improve insulin sensitivity for individuals with type 2 diabetes mellitus who have more elevated fasting glucose and glycated hemoglobin levels. 42
Therapies within the general scope of practice of naturopathic doctors that were seldom used were resistance training (20.7%), physical medicine (3.4%), homeopathy (3.4%), traditional Chinese medicine (13.8%), and counseling (3.4%). Resistance training was not prescribed at a high frequency possibly because of the high prescription rates of aerobic exercise (82.8%). Although speculative, patients or practitioners with a goal of weight loss may have operated with the understanding that aerobic exercise would use more calories or have a more immediate effect on reducing blood sugar or lipid levels. The rest of the naturopathic therapies might have been used at a lower frequency because there is less evidence (traditional and/or scientific) specific to the immediate health needs and implications for people with an endocrine disease like type 2 diabetes mellitus. An analysis of the gap between information contained in the Naturopathic Patient Database and that within the chart revealed that an audit score is generally determined within the first 3 visits and that there was congruence between the Naturopathic Patient Database and patient chart in providing information needed to obtain a reliable audit score.
Outcomes
Availability of laboratory findings was limited because only 24.1% (n = 7) of patients had greater than 1 report for glycated hemoglobin, for example. The majority of these patients experienced a modest drop in glycated hemoglobin levels. After the treatment period, 42.8% (n = 3) of the patients for whom consecutive lab tests were available could be reclassified as having achieved glucose control. Although patient compliance with prescription medications is unclear, it is possible that these effects were affected by comanagement. However, the results suggest that there is value in naturopathic care.
Measure Yourself Medical Outcome Profile scores indicate the patients' subjective perception of their disease and symptoms. A 2-point improvement on the Measure Yourself Medical Outcome Profile Scale corresponds to a 28% improvement. Given the limited number of Measure Yourself Medical Outcome Profile forms completed with this patient population (20.7%) and that these results are highly nonspecific, they are of limited value. However, they attest to the idea that self-selecting patients choosing to report do report success from a subjective perspective.
Study Limitations
The American Diabetes Association standards of medical care may not be a valid model to use in evaluating the care provided by naturopathic doctors. Particular audit items were identified that did not necessarily fit logically with the practicalities of naturopathic care in Ontario. Two of these items related to services of other health care providers (a referral to a registered dietician and to diabetes management self-education) but were being therapeutically accomplished by naturopathic doctors directly, potentially eliminating the need for referral for delivery of these health care services. Another possibly inappropriate audit item was evaluating the measurement of blood pressure at every visit. The similarity of visit frequencies between medical doctors following the American Diabetes Association guidelines and naturopathic doctor interns at a teaching clinic is unclear. Patients at the Robert Schad Naturopathic Clinic can be seen, initially, as frequently as once per week, which could have implications for the practical validity of this audit point. The audit items promoting vaccination are also a point of contention. Not a single clinician in this audit had recommended vaccines, possibly as a result of 1 or a combination of 3 possible factors: (1) many alternative medicine practitioners have preconceptions about vaccines that are difficult to change, 43 (2) patients using naturopathic doctor services may have preconceptions about vaccines that are hard to change, and (3) currently, naturopathic doctors do not have the ability to prescribe or deliver vaccinations in Ontario.
A teaching clinic might not be representative of practicing naturopathic doctors. Specific academic requirements and structure inherent in the administrative operations of the Robert Schad Naturopathic Clinic as well as the patient population attending a teaching clinic can influence treatment of the type 2 diabetes mellitus patient. Clinical supervisors also have academic duties, such as education of the students; this can at times be at odds with providing care similar to that of the naturopathic profession. These factors and the knowledge that patients are seen more frequently in the teaching clinic can alter the rate of delivery and quality of care.
Another limitation is that the audit was performed on a subsection of identifiable patients using the Naturopathic Patient Database based on International Classification of Diseases, 10th revision coding. Even though the majority of patients are entered into the Naturopathic Patient Database, it is not comprehensive. Cases of type 2 diabetes mellitus might not have been captured because they were not entered into the Naturopathic Patient Database correctly (ie, 8 cases lacked file identifiers) or because requirements to implement International Classification of Diseases, 10th revision coding were not in place at the inception of the Naturopathic Patient Database.
The data available on outcome measures was limited. Objective outcome measures such as consecutive glycated hemoglobin results were only available in 24.1% of cases. Subjective outcome measures (Measure Yourself Medical Outcome Profile) were only available in 20.7% of cases. It is important to note that these were observational data and that no control group was assessed. These factors make it difficult to draw any broad conclusions.
Finally, the patient expectations for the naturopathic doctor significantly dictated the role the clinician may have played as a primary care provider. Most patients presented with multiple comorbidities and did not indicate diabetes as a primary concern. This created a challenging scenario where clinicians treated multiple other concerns while attempting to simultaneously manage type 2 diabetes mellitus thoroughly. Consequently, many treatments provided for type 2 diabetes mellitus would be considered adjunctive rather than primary health care.
Conclusion
In this study, the Naturopathic Patient Database was useful in capturing cases of type 2 diabetes mellitus within the teaching clinic of the Canadian College of Naturopathic Medicine. Reliable audit criteria were successfully generated based on the American Diabetes Association standards of medical care, and 29 files were audited. The average audit score was 55.5/90. The most common interventions being used are diet and aerobic exercise, followed by supplements (omega-3 fatty acids and chromium) and botanicals. These data suggest that the American Diabetes Association standards of care for type 2 diabetes mellitus are not followed stringently, particularly with regard to thorough physical exams, appropriate referrals, and goal setting, in part because of systemic and regulatory limitations surrounding delivery of care. This was an observational study, and no attempt was made to assess a control group. Objective and subjective data on outcomes was limited. Patient outcomes improved in some cases. This study supports the idea that naturopathic care can improve outcomes in patients with type 2 diabetes mellitus, as has been previously shown in other studies. 44 Educational talks and reference sheets assisted in providing feedback to clinicians and students regarding measures to improve care. We expect these steps to result in practice improvement when the audit is repeated within the course of the next academic year. Further education and the creation of a naturopathic standard of care may improve audit performance and patient outcomes at this teaching institution.
Footnotes
Acknowledgments
The authors would like to acknowledge the Lotte and John Hecht Foundation and the Diabetes Action Research and Education Foundation for their generous support.
All authors contributed to the design of the project. CH and MS contributed to the acquisition of data and to the conduct of the project. CH and KC contributed to the analysis of the project. CH and KC generated the initial draft of the manuscript. All authors read and approved the final manuscript.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by grants from the Lotte and John Hecht Foundation and the Diabetes Action Research and Education Foundation.
Ethical approval for this project was provided by the Research Ethics Board of The Canadian College of Naturopathic Medicine.