
Abstract
A 15-minute, single-intervention, individually guided, Vedanta-based meditation was evaluated for acute effects on vital signs and mood indices. This study included 99 volunteers. Subjects were led in meditations incorporating breathing techniques, relaxation exercises, mental imagery, and silent mantra repetition. Pre- and post-intervention vital signs and mood indices were assessed, including heart rate, respiratory rate, blood pressure, temperature, Beck Depression Inventory (BDI), and Likert scales for mood. The meditation was shown to have statistically significant effects in the immediate improvement of vital signs and mood indices. The most substantial effects occurred for blood pressure, respiratory rate, Beck Depression Inventory, depression, anxiousness, happiness, and peacefulness. Also, males experienced greater physiological benefit whereas females experienced greater psychological benefit. The results of this study could be useful in developing gender-specific meditations to improve vital signs and mood indices in acute settings.
Keywords
Introduction
Meditation can decrease depression, anxiety, and hostility in addition to medical symptoms. 1 The positive effects of meditation have been linked to greater psychological and physiological well-being.2–8
Our study explored meditation to improve the quality of medical encounters. The acute effects of a 15-minute, single-intervention, individually guided, Vedanta-based meditation on vital signs and mood indices were examined for this purpose. A secondary goal of the analysis was to determine whether gender differences exist in the acute effects of meditation. A Vedanta-based meditation was chosen because of its appropriateness for a single intervention.
Some studies have reported that meditation and other complementary and alternative medicine (CAM) practices are generally used by women more than men. Researchers have published such findings for Americans,9–12 Israelis, 13 and Brazilians. 14 In one study, female physicians were more likely than male physicians to use meditation and other mind–body medicine for themselves and their patients. 15 However, another study reported that complementary and alternative medicine utilization did not differ by gender for persons with chronic pain. 16
Few rigorous studies have examined gender differences in the effects of meditation. Furthermore, the existing studies have observed inconsistent findings with respect to gender differences in the effects of meditation on physiological and psychological outcomes.
Some studies have shown that meditation effects on self-reported health outcomes were independent of gender.17,18 For cancer outpatients effects of meditation on self-reported mood did not differ by gender. 19 In another study, meditation effects on self-reported physiological and psychological symptoms were independent of gender. 20 A meta-analysis concluded that gender did not significantly influence the effect size on anxiety from meditation and other relaxation techniques. 21
Although the aforementioned studies did not find gender differences in the effects of meditation, the following studies have found significant physiological and psychological differences. When subjects used meditation as part of combined yoga practice, women achieved greater reduction than men in their basal metabolic rates adjusted for weight. 22 Women had greater reduction than men in systolic blood pressure, but not diastolic blood pressure, when using meditation and other relaxation techniques. 23 In another study, meditation and meditation plus biofeedback improved somatopsychic symptoms in females but not in males. 24
A different group examined the effects of an acute stressor on blood pressure, respiration, electrocardiographic variables, and self-reported emotional state in subjects with and without social phobia. 25 Women with social phobia demonstrated greater physiological and psychological changes than women without social phobia whereas men with social phobia demonstrated greater psychological changes alone, without greater physiological changes, compared with men without social phobia. 25 Our literature review suggests that gender differences are likely to exist in the effects of meditation, but the trends are neither clear nor consistent.
Materials and Methods
Eligible subjects were 18 years of age or older. A total of 99 volunteers participated in the study, which included 53 males and 46 females. All subjects provided verbal informed consent. The volunteers were recruited from public beaches and personal contacts of the principal investigator. The meditations were conducted at public beaches, in campus buildings, or at private residences. The Institutional Review Board of the University of Pennsylvania approved the study protocol.
Subjects anonymously completed surveys indicating gender, age, race, religion, and highest education completed or in progress. Subjects also indicated current medical problems and diagnoses and medications, current psychiatric problems and diagnoses and medications, diagnoses of high blood pressure, meditation experience, yoga experience, and spiritual or philosophical orientation.
Pre- and post-meditation subjects completed the Beck Depression Inventory (BDI) 26 and Likert scales, from 0 to 10, for 28 emotional adjectives in random order from the following mood categories: (a) depression (depressed, miserable, unhappy, sad, down, disheartened, cheerless); (b) anxiousness (anxious, nervous, worried, restless, stressed, strained, tense); (c) happiness (happy, content, pleased, glad, joyful, cheerful, blissful); (d) peacefulness (peaceful, calm, tranquil, composed, relaxed, serene, comfortable). Mood category scores represent the sum of the 7 Likert ratings within each of the 4 categories (range 0-70).
Immediately before and after the meditation, vital signs were measured, including heart rate, respiratory rate, blood pressure, and temperature. Blood pressure and heart rate were measured using the ReliOn Digital Blood Pressure Monitor 741CREL (Omron Healthcare, Bannockburn, IL; accuracy: pressure ±3 mm Hg or 2% of reading; pulse ±5% of reading). The temperature was measured using the ReliOn 510REL ear thermometer (accuracy: ±0.5°F). The respiratory rate was determined by counting the frequency of the rise and fall of the chest. All vital signs were assessed by the same medical student in his fourth and final year of school.
Instructions were given regarding breathing techniques and mantra selection prior to the guided meditation. The 15-minute single-intervention, individually guided, Vedanta-based meditation involved guided breathing techniques, guided relaxation exercises, guided mental imagery, and silent mantra repetition. Based on their preferences the subjects chose whether to be seated on the ground, to be seated on a chair, or to be lying on their backs. Instructions and sample recordings can be found at http://www.brindala.com/jebcam.html.
After the meditation and after assessment of vital signs and mood indices, the subjects completed a “yes” or “no” answer to the following questions: (a) Do you believe this meditation will allow you to feel better prior to a medical procedure? (b) Do you believe this meditation will allow you to feel better prior to surgery? (c) Do you believe this meditation will allow you to feel better prior to an encounter with a physician who will care for your health? (d) Do you believe this meditation will allow you to feel better prior to an encounter with a mental health professional who will care for your mental health?
All analyses were performed using R (http://www.r-project.org). Changes in mood and vital signs (before versus after meditation) were assessed using paired t tests. Differences in the response between males and females were assessed using Welch’s (unequal variance) 2-sample t test. In testing for an overall trend across the mood and vital sign responses, the differences in mood categories were added (depression + anxiousness − happiness − peacefulness) to produce an aggregate measure for mood change. For vital signs, the changes for each vital sign were ranked, and then the ranks added across vital sign to produce an aggregate measure of vital sign change. Differences in these aggregate measures were assessed using Welch’s 2-sample t test.
Results
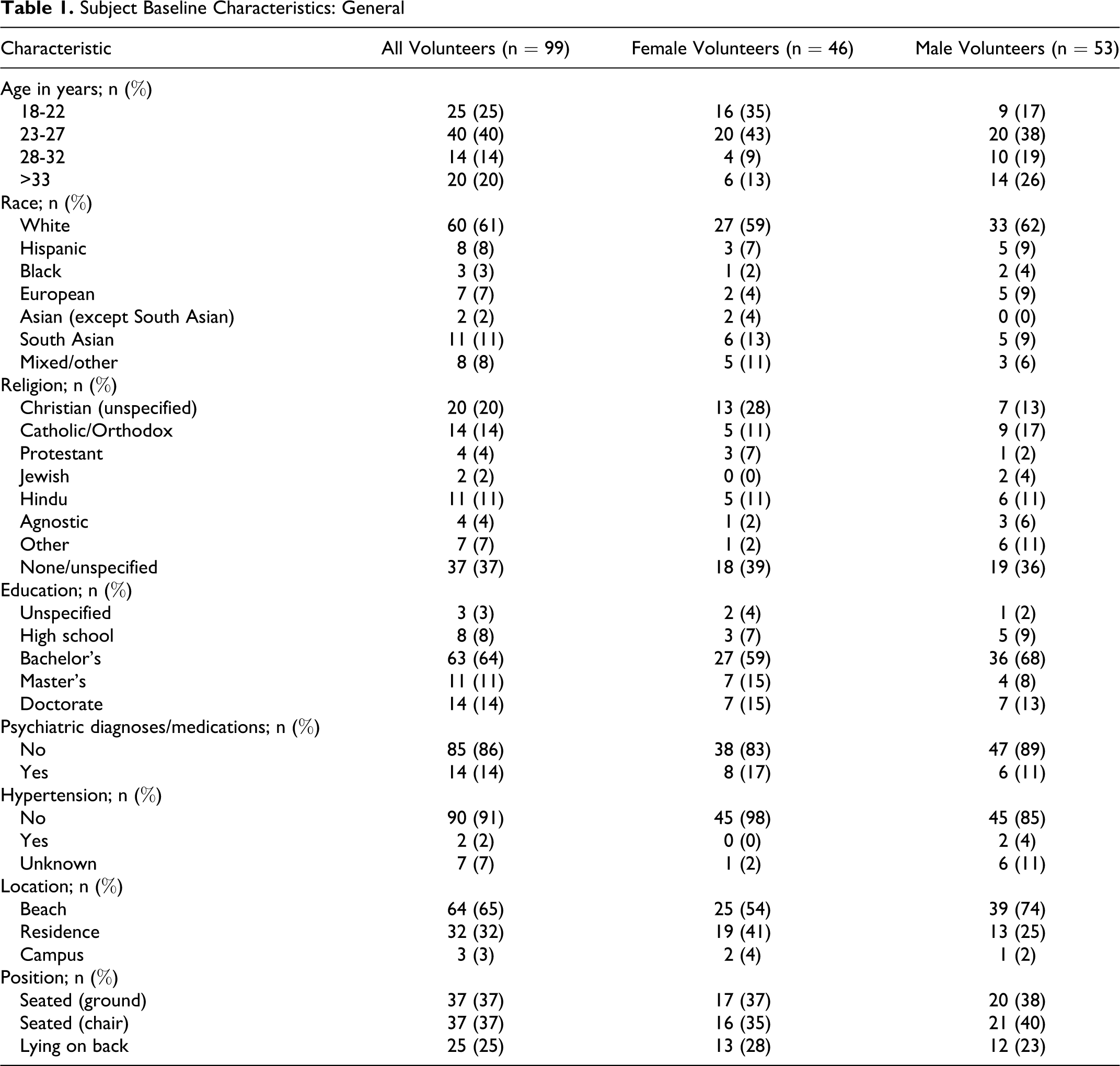
The study included 99 volunteers. The temperature readings from 2 volunteers and the blood pressure readings from 1 volunteer were unavailable because of equipment malfunction. The baseline characteristics are summarized in Tables 1, 2, and 3, which include information on demographics, psychiatric attributes, hypertension diagnoses, meditation experiences, and yoga experiences. Table 1 also includes the locations for the interventions and the positions of the subjects during the meditations. Table 4 includes the before and after values for vital signs and mood indices by gender.
Subject Baseline Characteristics: General
Subject Baseline Characteristics: Meditation Experience

a Meditation scores (0-10) were calculated by the sum of all characteristics with the following values: Previous meditations 0 (value 0); 1 (value 1); 2-5 (value 2); 6-20 (value 3); 21-100 (value 4); >100 (value 5). Weeks of experience 0-9 (value 0); 10-49 (value 1); 50+ (value 2). Regular frequency none (value 0); monthly (value 1); weekly (value 2); daily+ (value 3).
Subject Baseline Characteristics: Yoga Experience

a Yoga scores (0-10) were calculated by the sum of all characteristics with the following values: Previous yoga sessions 0 (value 0); 1 (value 1); 2-5 (value 2); 6-20 (value 3); 21-100 (value 4); >100 (value 5). Weeks of experience 0-9 (value 0); 10-49 (value 1); 50+ (value 2). Regular frequency none (value 0); monthly (value 1); weekly (value 2); daily+ (value 3).
Improvement in Vital Signs and Mood Indices From Meditation a

Abbreviations: SBP, systolic blood pressure in mm Hg; DBP, diastolic blood pressure in mm Hg; HR, heart rate in beats per minute; RR, respiratory rate in breaths per minute; Temp, temperature in °F; BDI, Beck Depression Inventory.
a Vital signs and mood indices were assessed immediately before and immediately after the meditation. Peacefulness, happiness, depression, and anxiousness each represent composite mood category ratings based on Likert scales. +/− indicates standard deviation.
Heart rate was reduced by 1.36 beats per minute (n = 99, 95% confidence interval [CI] = 0.10-2.63, P = .03). Respiratory rate was reduced by 4.78 breaths per minute (n = 99, 95% CI = 4.14-5.43, P < .0001). Systolic blood pressure was reduced by 4.80 mm Hg (n = 98, 95% CI = 2.76-6.83, P < .0001). Diastolic blood pressure was reduced by 2.26 mm Hg (n = 98, 95% CI = 0.70-3.83, P = .01). Temperature was reduced by 0.24°F (n = 97, 95% CI = 0.08-0.39, P = .003). Data are summarized in Figure 1 .

Improvement in vital signs and mood indices from meditation
Beck Depression Inventory score was reduced by 3.07 (95% CI = 2.35-3.79, P < .0001). Depression mood category score was reduced by 5.99 (95% CI = 4.76-7.22, P < .0001). Anxiousness mood category score was reduced by 10.40 (95% CI = 8.54-12.25, P < .0001). Happiness mood category score increased by 5.80 (95% CI = 4.09-7.51, P < .0001). Peacefulness mood category score increased by 11.26 (95% CI = 9.45-13.07, P < .0001). Data are summarized in Figure 1.
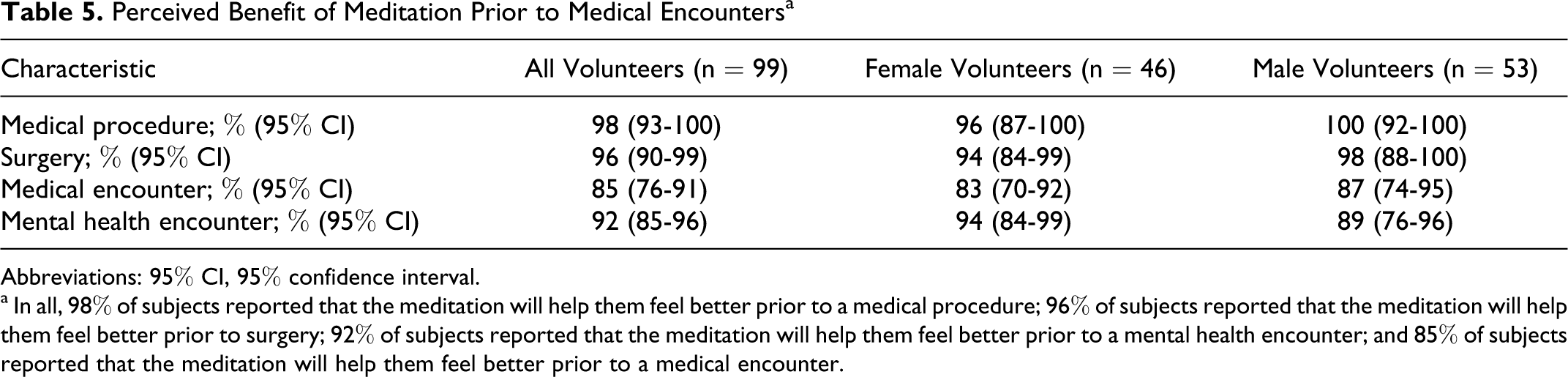
In all, 98% of volunteers answered “yes” to the question, “Do you believe this meditation will allow you to feel better prior to a medical procedure?”; 96% of volunteers answered “yes” to the question, “Do you believe this meditation will allow you to feel better prior to surgery?”; 92% of volunteers answered “yes” to the question, “Do you believe this meditation will allow you to feel better prior to an encounter with a mental health professional who will care for your mental health?”; and 85% of volunteers answered “yes” to the question, “Do you believe this meditation will allow you to feel better prior to an encounter with a physician who will care for your health?” Data for perceived benefit are represented in Table 5 .
Perceived Benefit of Meditation Prior to Medical Encounters a
Abbreviations: 95% CI, 95% confidence interval.
a In all, 98% of subjects reported that the meditation will help them feel better prior to a medical procedure; 96% of subjects reported that the meditation will help them feel better prior to surgery; 92% of subjects reported that the meditation will help them feel better prior to a mental health encounter; and 85% of subjects reported that the meditation will help them feel better prior to a medical encounter.
Heart rate reduction was greater in males by 0.39 beats per minute (95% CI = −2.12 to 2.91, P = .76) though not statistically significant. Respiratory rate reduction was greater in males by 0.26 breaths per minute (95% CI = −1.03 to 1.55, P = .69), though not statistically significant. Systolic blood pressure reduction was greater in males by 4.62 mm Hg (95% CI = 0.71 to 8.52, P = .02). Diastolic blood pressure reduction was greater in males by 2.16 mm Hg (95% CI = −0.89 to 5.20, P = .16), though not statistically significant. A test for whether the change in aggregate vital sign measure differs across gender yields a P value of .06 with males having greater reduction in vital signs, though not statistically significant.
Beck Depression Inventory score reduction was greater in females by 0.31 (95% CI = −1.11 to 1.74, P = .66), though not statistically significant. Depression mood category score reduction was greater in females by 0.34 (95% CI = −2.15 to 2.83, P = .78), though not statistically significant. Anxiousness mood category score reduction was greater in females by 2.69 (95% CI = −1.04 to 6.41, P = .16), though not statistically significant. Happiness mood category score improvement was greater in females by 3.18 (95% CI = −0.25 to 6.61, P = .07), though not statistically significant. Peacefulness mood category score improvement was greater in females by 3.85 (95% CI = 0.27 to 7.44, P = .04). A test for whether the change in aggregate mood score differs across gender yields a P value of .03 with females having greater improvement in mood. The data for gender subgroups are represented in Figure 2 .
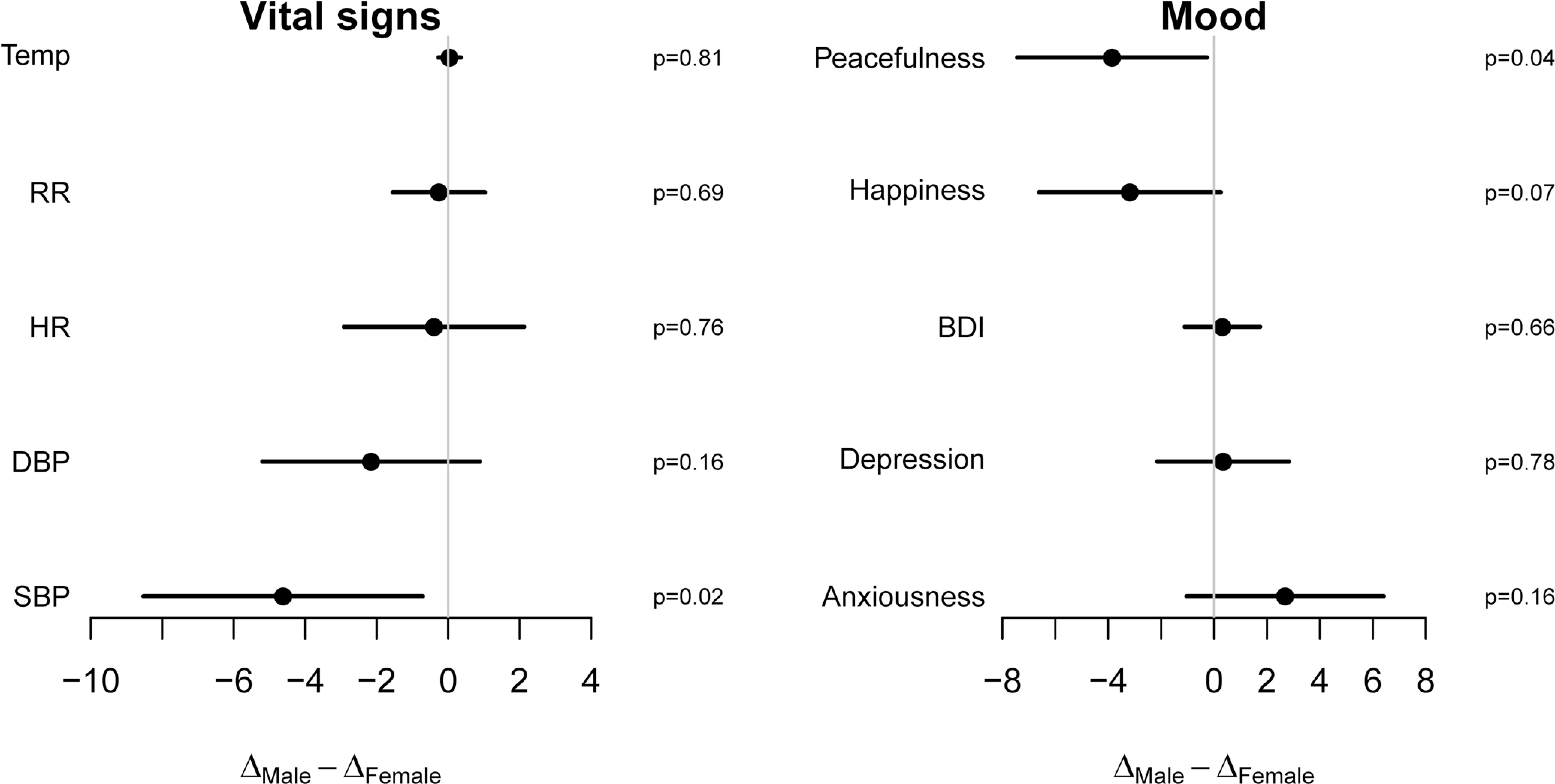
Gender differences of improvement in vital signs and mood indices from meditation
Secondary statistical analyses demonstrated no significant differences in outcomes between subgroups based on the characteristics summarized in Tables 1-3 or between random volunteers and personal contacts of the principal investigator.
As suggested by Table 4, Beck Depression Inventory, depression mood category, and anxiousness mood category are all rather skewed to the right, that is, most people have values close to 0, and some people have very high values. Consequently, we explored the use of nonparametric methods to analyze these outcomes, but they did not substantially alter any of our conclusions.
Discussion
After the 15-minute, single-intervention, individually guided, Vedanta-based meditation, an improvement in all vital signs occurred for the study population. Heart rate, respiratory rate, systolic blood pressure, diastolic blood pressure, and temperature all decreased after the meditation. The respiratory rate and blood pressure were most substantially reduced. The guided breathing techniques involved conscious slowing of inhalations and exhalations. However, the respiratory rate remained slower immediately after the meditation was complete and the guided breathing techniques had concluded.
The shift in vital signs potentially represents a stimulation of the parasympathetic nervous system. Increased parasympathetic drive has been proposed as a mechanism for mood improvement from yogic breathing techniques. 27 Also, lower temperatures have been observed in control subjects compared to depressed patients, 28 and average temperatures were lower on days with lower ratings of self-reported depression. 29 The results of this study corroborate these previous findings. In future studies, it will be interesting to assess potential mechanisms of parasympathetic stimulation through utilization of brain imaging techniques and analyses of various neurotransmitters, hormones, endorphins, and other factors.
In addition to the rapid reduction in all vital signs, mood improvement was remarkable across the subject population for all indices measured. The Beck Depression Inventory is perhaps the most well validated mood index, and there was a clear, significant reduction in Beck Depression Inventory after the meditation. Beck Depression Inventory is primarily used to assess mood changes over longer time periods such as days, weeks, or months. To have any reduction in Beck Depression Inventory in 15 minutes indicates an important finding. Therefore, the Beck Depression Inventory results alone suggest that the meditation had a strong effect on mood improvement. The Likert mood category results further suggest reduction in depression and anxiousness with improvement in happiness and peacefulness.
Also, baseline mood ratings for the study population were quite good prior to the meditation. Therefore, the potential range for mood improvement was limited by the nature of the mood scales as well as the baseline characteristics of the subjects. Hence, the improvement in mood ratings could potentially be underestimated in this study. Perhaps, in a population with worse baseline mood ratings even more significant improvement in mood could be observed.
Subjects answered questions to indicate whether they thought the meditation in this study would be useful in different medical settings. It was clear that a large number of the subjects perceived benefit prior to interactions with health care providers, particularly in settings of procedures or surgeries in which there could be greater stress and/or anxiety. People can generally attribute less stress and/or anxiety to general medical encounters and mental health encounters, which could explain why subjects perceived less benefit in those settings compared with procedures and surgeries.
Nonetheless, a very high percentage of subjects indicated that the meditation would allow them to feel better prior to all of the medical situations described. Improved mood and vital signs could prove to be helpful for quality improvement of medical interactions, procedures, and surgeries. Better interactions could even lead to increased compliance, fewer complications, and improved outcomes. The subjects' perceptions about meditation prior to medical encounters suggest that such an intervention could represent great potential for quality improvement.
Males achieved greater reduction in systolic blood pressure following the meditation whereas females experienced greater improvement in the peacefulness mood category score. Though the other outcomes were not statistically significant, all the differences across the genders illustrate a greater physiological improvement for males and a greater psychological improvement for females. These findings add to the literature reviewed about gender differences in the effects of meditation. More research comparing gender differences will be necessary to determine the robustness of the trends observed.
The baseline characteristics appear to be similar for male and female subjects as summarized in Tables 1-3. Therefore, the differences are more likely to be due to gender than some other confounding factor which might have mediated the differences. It is important to note that the meditation leader for all the interventions was a young, male medical student. In future studies it would be interesting to examine whether the gender or appearance of the meditation leader has any bearing on the effects of the meditation across gender.
Important limitations of this study include selection bias, lack of comparison groups, possible placebo effects, some unvalidated mood scales, and accuracy of instruments for vital signs. Nonetheless, each subject did serve as their own internal control, and the secondary analysis of gender subgroups did involve comparison groups. Furthermore, the results of the well-validated Beck Depression Inventory represent important findings notwithstanding the results of the unvalidated Likert scales.
Conclusions
This study illustrated that a 15-minute, single-intervention, individually guided, Vedanta-based meditation rapidly improved both vital signs and mood indices. The most substantial improvements were effects on blood pressure, respiratory rate, Beck Depression Inventory, depression, anxiousness, happiness, and peacefulness. A few statistically significant differences existed across gender subgroups, which potentially suggest greater physiologic effects on males and greater psychological effects on females. Such a meditation has profound ramifications for the improvement of interactions in various medical settings, and the perceptions of the subjects endorsed this potential benefit. Further study of meditation in this context can ultimately demonstrate the ability to achieve quality improvement in medical encounters and their resulting health outcomes.
Footnotes
Acknowledgments
The authors are deeply indebted to Albert Stunkard, MD, University of Pennsylvania, for serving as the original research advisor for the design of the study and the collection of the data. The authors would like to thank Jacques Barber, PhD, University of Pennsylvania, for offering initial guidance for the data analysis. The authors would also like to thank Michael Posner, PhD, and Ryan Kelly, Villanova University, for offering preliminary statistical guidance and conducting preliminary statistical tests, respectively. The authors would like to recognize the following University of Kentucky faculty members for their assistance with article preparation: F. Douglas Scutchfield, MD, Rice Leach, MD, and Subbarao Bondada, PhD.
JS designed the study, collected the data, conducted the analysis, and wrote the paper. PJB offered analytical support, completed statistical calculations, and provided the contents for tables and figures.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
This study was supported by a fellowship from an NIH-funded Short Term Training Grant awarded to Jayaram Srinivasan as a medical student at the University of Pennsylvania. Bryan A. Wolf, MD, PhD, University of Pennsylvania, secured the overall grant funding, which was sponsored by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK).
The Institutional Review Board of the University of Pennsylvania approved the study protocol.