
Abstract
Three complementary approaches for managing physical and psychological symptoms related to chemotherapy-induced peripheral neuropathy were evaluated against an education-only control arm. This study included 26 participants who were randomly assigned to weekly, hour-long sessions of yoga, Reiki, meditation, or an educational control experience for 6 weeks. Each participant completed pre–post measures of neurotoxicity, quality of life, psychological distress, and mindfulness. Descriptive analysis of the data indicated that all experimental group participants demonstrated improved within-group scores on quality of life and neurotoxicity outcomes following intervention; however, the improvements were not statistically significant. Neurotoxicity worsened significantly in the control group, but there were no pre–post changes with respect to quality of life, psychological distress, or mindfulness. Effect sizes were large with respect to meditation and mindfulness and with Reiki and psychological distress. Moderate effect sizes with respect to yoga and neurotoxicity and quality of life offer promise for all 3 interventions in managing chemotherapy-induced peripheral neuropathy.
Chemotherapy-induced peripheral neuropathy is a side effect that occurs with many of the most common chemotherapeutic agents used to treat cancer. 1,2 It is the result of damage caused to the peripheral nervous system by chemotherapy and can affect sensory, motor, and autonomic neurons. 3,4 Chemotherapy-induced peripheral neuropathy can produce sensory symptoms that range from bothersome to disabling tingling, burning, numbness, loss of balance, pain, and loss of motor function that can include weakness in muscles in the upper and lower extremities. 5 Although the actual prevalence of chemotherapy-induced peripheral neuropathy is unknown, it is generally estimated at 30% to 40% in patients who have received the classes of chemotherapeutic agents used to treat breast, colon, and lung cancers, and lymphomas. 1,6 –8 Typically, symptoms of chemotherapy-induced peripheral neuropathy are considered along with other pain symptoms and treated with opioids and analgesics. 9 However, these options yield limited results. With few alternatives for attenuating the symptoms of unremitting chemotherapy-induced peripheral neuropathy, people living with them have few options other than to endure them.
Massage, yoga, and other complementary and alternative medical modalities have proven successful with pain and quality-of-life issues related to cancer and its treatment. 10 –13 Given the limited effectiveness of allopathic intervention, the purpose of this pilot study was to determine the feasibility of using 3 complementary interventions in relieving the physical and emotional symptoms associated with chemotherapy-induced peripheral neuropathy while increasing capacity for mindfulness or self-focused attention. Of specific interest in this proposed study are 1 putative energy field or biofield 14 approach and 2 complementary mind–body approaches that include Reiki, yoga, and meditation, respectively.
Reiki
Reiki is a Japanese biofield or energy technique used for stress reduction, relaxation, and the promotion of physical healing. As an integrative approach, Reiki is considered to be a low-risk intervention for enhancing the body’s self-healing capacity with few reports of contraindications or adverse events. 15
Limited research findings indicate that Reiki shows promise for relieving pain from a variety of medical and psychiatric conditions that include cancer, surgical pain, chronic back pain, arthritis, depression, and anxiety. 16 –19 Reiki has also produced positive results in people receiving treatment for a variety of local and advanced cancers and has had a significant positive effect on relieving cancer-related fatigue, pain, anxiety, depression, and contributing to quality of life. 20 –22 However, research using Reiki in the treatment of chemotherapy-induced peripheral neuropathy is scant and only one published descriptive article was located in preparation for this study. 23
Yoga
Yoga practice includes muscle stretching and breathing exercises and helps promote stress control, flexibility, balance, sleep, and voluntary control of the autonomic nervous system. 24 –26 Even though the majority of published research involving yoga and cancer has been conducted with breast cancer survivors, 27,28 studies investigating the use of a yoga as a complementary and alternative medicine intervention have reported generally positive physical, psychological, and quality-of-life outcomes. Yoga has proven helpful as an adjuvant to antiemetic therapy 29 ; in the management of menopausal symptoms 30 ; and in diminishing acute and persistent cancer related fatigue, diarrhea, and shortness of breath. 31 –34 Significant positive psychological and quality-of-life outcomes have included decreases in psychological distress, anxiety, and depression. 29,31,35,36
Meditation
Meditation has long been a component of mind–body medicine for its potential to enhance relaxation, reduce stress, and improve general medical symptoms. 37,38 Mindfulness-based stress reduction, developed by Kabat-Zinn, 39 integrates mindfulness meditation with the healing process and the management of medical and psychological issues. Mindfulness meditation strategies, including mindfulness-based stress reduction, have been noted to have a general or nonspecific stress reducing effects that have proven beneficial both to healthy subjects and to those living with heart disease, chronic pain, and emotional disorders. 40 Randomized studies have produced evidence that mindfulness meditation/mindfulness-based stress reduction interventions have significantly reduced pain, sleep disturbances, anxiety, and depression while simultaneously increasing mindfulness and quality of life. 41,42 Within the general cancer population, mindfulness meditation/mindfulness-based stress reduction has produced similar positive results. These have included reduction in treatment-related insomnia, fatigue, psychological distress, and other mood symptoms. 43,44
Rationale for the Study
There can be no doubt that ever-growing numbers of health care consumers are choosing complementary and alternative medicine therapies to address their disease or its effect on quality of life. A study with a large and ethnically diverse random sample of 9187 citizens of California 45 discovered that nearly 66% of the sample had used a complementary and alternative medicine modality, regardless of health status, in the 12 months prior to participation in the study. The use of complementary and alternative medicine treatments as part of an integrated approach to the management of cancer is growing in popularity among people living with cancer-related pain and emotional distress in America and Europe. 46 –49 Furthermore, in a recent study of complementary and alternative medicine use among cancer survivors, 26% of women and 13.7% of men surveyed indicated the use of at least one complementary and alternative medicine modality within the year preceding the study. 50
Despite the availability of a variety of allopathic therapies for managing chemotherapy-induced peripheral neuropathy, complementary and alternative medicine modalities may provide potential options for improving the management of chemotherapy-induced peripheral neuropathy; however, there have been few complementary and alternative medicine studies that specifically address it. Complementary and alternative medicine modalities may provide additional control of residual symptoms of chemotherapy-induced peripheral neuropathy; however, a thorough search of major databases revealed a solitary randomized study that explored the use of acupuncture and another presented an overview of integrative approaches for addressing neuropathic pain. 51,52 Therefore, the current feasibility study evaluated three adjuvant complementary approaches in the management of chemotherapy-induced peripheral neuropathy. Because the focus of the study was to evaluate the strengths of the identified complementary and alternative medicine modalities, it was not designed with sufficient power for producing statistically significant outcomes and responses to study interventions will be described in terms of overall trends.
Design/Methodology
Using a pretest–posttest comparison group design with random assignment, this 4-arm pilot study was undertaken to determine the efficacy of 3 complementary approaches in reducing the signs and symptoms of chemotherapy-induced peripheral neuropathy in contrast to a structured biopsychosocial holistic education reference arm. Outcomes were quantitatively assessed through instruments that measured quality of life, neurotoxicity, psychological distress, and mindfulness.
Participants (N = 36) were recruited for the study through local oncologists’ offices, mailed fliers, an advertisement in the health section of a large metropolitan newspaper, and a general announcement in the monthly newsletter of a large cancer support organization. No financial incentive, other than receiving the complementary and alternative medicine interventions at no charge, was provided. The institutional review boards in the health system through which the study took place and the university where the principal investigator had a faculty appointment approved the study. Following the presentation of study details, written informed consent documents were obtained from each participant prior to being included in the study. The study flow chart is shown in Figure 1.

Study flow diagram
To be eligible for the study, participants had to be 18 years old, have persistent symptoms of chemotherapy-induced peripheral neuropathy lasting 3 months or more, and have completed chemotherapy that included one or more of the taxane, vinca alkaloid, or platinum classes of chemotherapies for a cancer diagnosis at least three months prior to beginning the study. Because the researchers did not have access to participants’ medical records, information about chemotherapy-induced peripheral neuropathy symptoms, diagnosis, and treatment were self-reported. In addition, participants were excluded if they were actively taking part in one of the complementary modalities offered in this pilot study. A further requirement for eligibility required readiness for physical activity as demonstrated by responses to the Physical Activity Readiness Questionnaire for participants aged 18 to 59 years, 53,54 the Revised Physical Activity Readiness Questionnaire for participants aged 60 years and older 55 –57 or the Physical Activity Readiness Medical Examination, conducted by a physician for participants who have physical conditions that required further evaluation. 58 Physical readiness was assessed to ensure safe experiences for participants who may have been randomized into the yoga or meditation conditions that required some measure of movement or sitting for brief periods. Finally, participants were required to have an ability to comfortably speak, read, and understand English, be fully oriented, and possess the capacity to understand and provide informed consent. After meeting eligibility criteria; participants provided signed informed consent and completed baseline outcomes measures. It should be noted that participants who were taking medications for symptoms of chemotherapy-induced peripheral neuropathy were encouraged to continue doing so and to alert the researchers if there were changes or additions to their regimens.
Randomization
After completing pretest instruments, participants were assigned a case number and randomly assigned to 1 of the 3 intervention groups or the holistic education group. Randomization was not masked. However, efforts to conceal allocation included the use of case numbers and a computer-generated random numbers table by the lead researcher. Coresearchers did not take part in the randomization process. Initially, there were 9 participants in each arm.
Interventions
To minimize the extraneous effects of time, interventions began within one month of recruitment. Participants took part in Reiki, yoga, meditation, or education 1 hour per week for 6 weeks. In addition to the formal outcomes measures, participants were also asked to keep a log of their symptom severity, time spent in home practice of their intervention modality, and to make note of experiences that tended to ameliorate or exacerbate their physical or emotional states. The holistic education group was used as a control group.
Reiki
Five Reiki masters who shared the same training and used similar approaches provided Reiki sessions. The sessions took place in a quiet room where up to 5 sessions could be conducted simultaneously. Each session was initiated with a brief conversation between the participant and the Reiki master to establish rapport and set goals for the session. Following the conversation, the participant would lie on a massage table, fully clothed, in a supine position. Working from the head toward the feet, the practitioner placed their hands either on or above the participant; pausing for a few moments at 7 designated locations, reflecting the chakras, to channel energy from their hands to the client. After reaching the feet, the participant was asked to roll into a prone position and the process was repeated. On reaching the feet for a second time, the session was concluded. Participants were encouraged to record their symptoms in their journals.
Yoga Intervention
Each weekly session involved gradual movement from one posture or asana, to another in ways that allowed the participants to move at an individual and safe pace. A registered yoga teacher trained in Hatha Yoga guided all sessions. The 3 stages of the intervention involved use of breathing and body scanning to relax the body before beginning movement, then proceeded from breathing to assuming postures that enabled gentle stretching. The conclusion of the sessions was composed of 10 minutes of relaxation. Participants maintained a supine position on the floor or sat comfortably while the yoga teacher guided them in relaxed breathing systematic muscle relaxation. As the session concluded, participants were encouraged to practice yoga each day and record their practice in their journals.
Meditation Intervention
Meditation sessions followed a weekly protocol. The meditation instructor provided a brief overview of what would be taught during the session as well as addressing participants’ questions, or feedback about their meditative experiences during the preceding week. The remainder of the hour was devoted to developing meditative skills using a mindfulness meditation practice. Participants focused on developing attention to the breath while learning to recognize, acknowledge, accept the presence of physical sensations or emotions, then to step back, release the thought or sensation, and refocus attention toward the breath. Meditative experiences were expanded to include meditation while walking and eating. At the conclusion of each meeting, the meditation instructor encouraged participants to engage in daily meditation practices and to document their practice experiences in the practice journal.
Holistic Education
Each week during the study, participants took part in a 1-hour class that focused on the biological, psychological, and social components of chemotherapy-induced peripheral neuropathy. Topics for each session were presented by an oncology nurse educator, oncology social worker, or registered dietician. During the first three weeks of the group, participants were presented with basic information about neuroanatomy, effects of chemotherapy on the peripheral nervous system, and medications typically used in the management of chemotherapy-induced peripheral neuropathy. During weeks 4 and 5, participants received information about the use of nutrition and complementary modalities for managing symptoms of chemotherapy-induced peripheral neuropathy. During the final meeting of the group, coping strategies for managing the impact of chemotherapy-induced peripheral neuropathy on self-image, relationships with others and abilities to perform activities at home and were presented.
Measures
Psychological distress
The outcome measure for psychological distress was the Brief Symptom Inventory–18. 59 This is an 18-item screening instrument that measures distress on 3 subscales that include somatization, depression, and anxiety. When combined, the subscales produce a global severity index. It is the global severity index that provides an overall measure of psychological distress. A score of 10 and above for men or 13 and above for women indicates psychological distress. The Brief Symptom Inventory–18 has been found to have good internal reliability (Cronbach’s α = .89), was written to be understood at a sixth-grade reading level, and takes approximately 4 minutes to complete. 60
Quality of life and neurotoxicity
The outcome measurement instrument for quality of life was the Functional Assessment of Cancer Therapies—Gynecologic Oncology Group–Neurotoxicity scale. 61 This is a 38-item scale composed of 27 general questions that comprise an instrument known as the Functional Assessment of Cancer Therapies–General. The questions explore general dimensions of life quality with respect to physical, functional, emotional, social, and family well-being. The Functional Assessment of Cancer Therapies—Gynecologic Oncology Group–Neurotoxicity scale combines these questions with 11 questions regarding symptoms of neurotoxicity to form a neurotoxicity subscale. Using a 5-item Likert-type scale, respondents rate the degrees to which items were important to them during the past 7 days. Ratings of experiences range from not at all to very much. This instrument has high test–retest reliability, consistently high convergent/divergent validity coefficients, and is sensitive to respondent performance status rating. 61 Although originally developed within the context of gynecological cancers, this instrument has been used to measure the side effects of taxane therapy and in colon cancers with both men and women. 62,63 Cronbach’s coefficient for each item on this scale has been demonstrated at .70 or higher, and the instrument is sensitive to respondent changes over time. 64
Mindfulness
As a component of general well-being, the construct of mindfulness was measured with a scale known as the Mindful Attention Awareness scale. 65 The Mindful Attention Awareness Scale is a 15-item scale that is self-administered, requires no assistance to complete, and can be taken in 5 minutes or less. Internal reliability of items on the Mindful Attention Awareness Scale has been established with Cronbach’s α coefficients at .80 or higher per item, 65 and there are no differences in performance on the Mindful Attention Awareness Scale between men and women. 66 The Mindful Attention Awareness Scale has demonstrable construct validity across cancer populations with reliability coefficients of .80 or greater. 67
In addition to the above measures, the participants provided data from a brief sociodemographic data and health history questionnaire. This information included the participant’s age, gender, marital status, number of children, and current work status. In addition, the questionnaire asked about cancer history, including type of cancer, stage of cancer, time since initial diagnosis, types of cancer treatments received, and last date of cancer treatment. With the exception of the sociodemographic data and health form, which was administered once; participants completed study instruments prior to the first experience in both intervention or control conditions and immediately following their last experience with the study.
Data Analysis
Descriptive analyses were used to articulate demographic and health characteristics of the study participants, attrition rate, and adherence to study protocol. One-way analysis of variance (ANOVA) was used to test for differences between the intervention and control groups. Because the data were collected using random assignment, paired samples t tests were used to assess within-group differences for the whole sample as well as within intervention and control groups. All participants who completed posttest instruments, regardless of adherence to the study protocol, were included in the analysis to yield treatment effects that are reflective of real-world conditions. 68 Because the sample size was small, missing values were replaced with the series mean for the variable. 69,70 A P value <.05 was considered statistically significant.
Results
Sample
Thirty-six participants were initially recruited and randomized into the study and 31 were present at the first intervention sessions. Five of the initial 36 participants were unable to participate. Two of these reported that their cancer had recurred and required further treatment; making them ineligible to participate. One participant decided to withdraw from the study following a family emergency and another, after randomization to the yoga intervention, withdrew on medical advice. Two participants in the meditation arm began the study but stopped attending after 2 or 3 meetings. One reported that it had become difficult to attend an evening group and the other gave no reason for discontinuing. Two additional participants in the control arm dropped out of the study and did not provide a reason or respond to attempts at contact. One member in the Reiki arm withdrew from the study and reported that her work schedule did not allow for continued participation. The data were analyzed using one-way ANOVA for assessing between-group comparisons at pretest and posttest. Comparisons of demographic, health, and outcomes measures revealed no significant differences between participants who completed the study and those who did not. At the conclusion of the intervention phase of the study, 26 participants remained in the study and completed posttesting following their participation in 1 of the 4 arms that included meditation (n = 5), Reiki (n = 7), yoga (n = 7), or education (n = 7).
Demographic and clinical characteristics
Of those who elected to remain in and complete the study, 23 were women (88.5%) and 3 were men (11.5%) with a median age of 60 years (range = 38-72 years; Table 1). Nearly 81% of the participants self-identified as European American or white (n = 21; 80.8%) and more than three quarters of participants indicated that they were married (n = 20; 76.9%). Most participants reported having received bachelor’s and advanced degrees (n = 23; 88.5%). The most frequently reported cancer diagnoses included breast (n = 17; 65.4%), ovarian (n = 2; 7.7%), and non-Hodgkin lymphoma (n =2; 7.7%; Table 2). More than two thirds of participants reported the onset of symptoms of neuropathy during the course of their chemotherapy treatment (n = 18; 69.2%) with one third reporting the onset of symptoms following treatment (n = 8; 30.8%; Table 2). More than one third of participants (n = 10; 38.5%) reported having symptoms of chemotherapy-induced peripheral neuropathy for more than 2 years, whereas 7 (26.9%) had experienced symptoms for 13 to 24 months, and 9 (34.6%) described having symptoms for 12 months or less (Table 3). A one-way ANOVA was used to test for differences between intervention groups. There were no significant differences between the groups with respect to demographic or medical characteristics for the preintervention-dependent measures for psychological distress, neurotoxicity, quality of life, or mindfulness.
Demographic Variables (N = 26)

Protocol adherence
All 26 participants attended at least one session of the intervention to which they had been assigned. Twelve participants (40%) attended all 6 sessions, 8 (26.7%) attended 5 sessions, 5 (16.7%) attended 4 sessions, 1 (3.3%) attended 3 sessions, 2 (6.7%) attended 2 sessions, and 2 (6.7%) attended only 1 session. In the meditation arm, 1 participant (20%) attended all 6 sessions, 3 (60%) attended 5 sessions, and 1 (20%) attended 4 sessions. Four members (57.1%) in the Reiki arm attended all 6 sessions, 2 (28.6%) attended 5 sessions, and 1 (14.3%) completed 4 sessions. In the yoga arm, 2 participants (28.6%) were present for all 6 sessions, 2 (28.6%) attended 5 sessions, 2 (28.6%) attended 4 sessions, and 1 participant (14.3%) attended only 1 session. In the control condition, which consisted of holistic education, 5 participants (71.4%) attended all 6 sessions and 2 (28.6%) attended 5 sessions.
Psychological Distress
At pretest, the full-sample mean for psychological distress was 13.84 with 56.5% (n = 13) of women participants scoring within the clinical range (Table 4). None of the men scored within the clinical range for psychological distress. At posttest, the full sample mean for the Brief Symptom Inventory–18 was diminished to 11.65 (P = .226). A one-way ANOVA was conducted to compare the effect of each of the interventions on levels of psychological distress, F(3, 22) = 1.15, P = .351. There was no significant effect of any of the interventions at the P ≤ .05 level on psychological distress.
Health Variables

Months Living With Chemotherapy-Induced Peripheral Neuropathy Symptoms

Psychological Distress: Brief Symptom Inventory–18 Global Severity Index
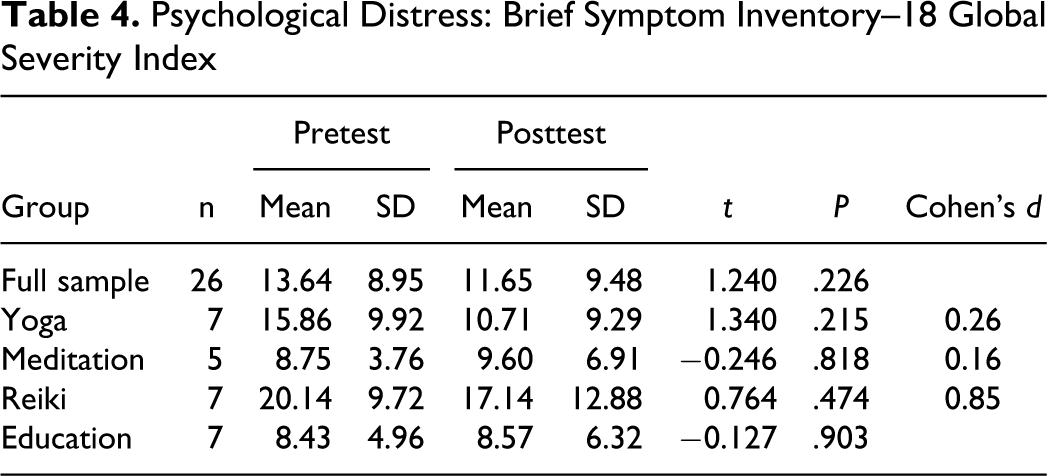
Scores on the Brief Symptom Inventory–18 were diminished for participants in the yoga (P = .215) and Reiki arms (P = .474), but increased in the meditation (P = .818) and education/control (P = .903) arms. It should be noted, however, that although scores increased in the 2 groups, neither group had clinically significant scores. Effect sizes for yoga and meditation conditions indicated a small effect. However, the magnitude of treatment effect was large in the Reiki condition. Converting Cohen’s d to r 2 shows that 15% of the variation was attributable to the Reiki intervention.
Neurotoxicity and Quality of Life
Symptoms of neurotoxicity improved, as indicated by higher scores, only slightly in the full sample from 28.43 to 28.96 (Table 5). However, a one-way ANOVA indicated that there was no significant effect of any of the interventions on symptoms of neurotoxicity, F(3, 22) = 0.76, P = .529. With the exception of the control group, no statistically significant differences were found within groups in any of the study arms with respect to neurotoxicity or quality of life. Cohen’s d for meditation and Reiki was small; however, a moderate effect size was found in the yoga intervention. Converting Cohen’s d to r 2 shows that 8.7% of the variation was attributable to the yoga intervention. Although each study arm demonstrated improvement on the neurotoxicity subscale, the control arm demonstrated a significantly poorer pre–post result from 31.14 to 27.86 (P = .034).
Neurotoxicity Scale: Functional Assessment of Cancer Therapies—Gynecologic Oncology Group–Neurotoxicity

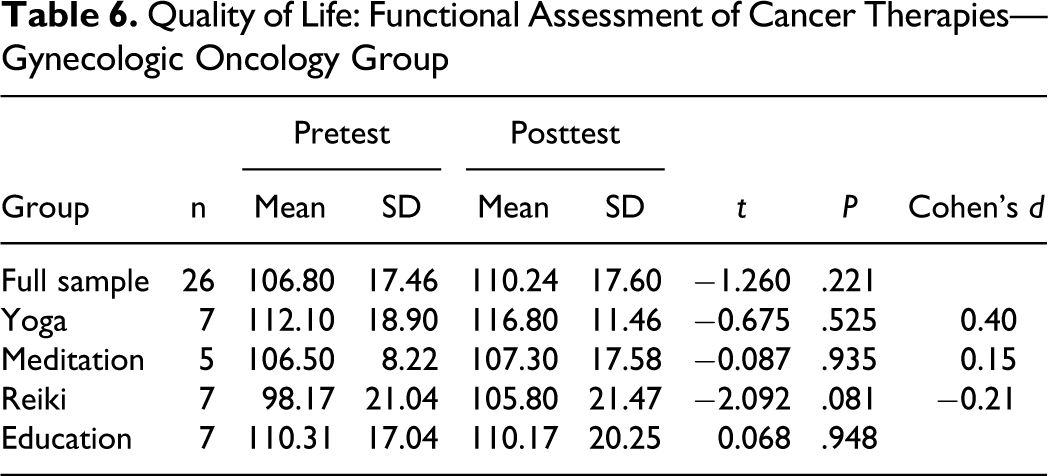
The mean Functional Assessment of Cancer Therapies—Gynecologic Oncology Group–Neurotoxicity scale score on quality-of-life items for the full sample at pretest was 106.8 and this score improved at posttest to 110.24 (Table 6). In each arm, with the exception of the control arm, improvement was noted. One-way ANOVA revealed that no significant effect on quality of life at the P < .05 level for any of the 3 study interventions, F(3, 22) = 0.490, P = .693. Paired samples t-test results for within-group results revealed that, although scores were improved, they were not statistically significant. A weak to moderate effect size was noted in the yoga intervention, but when Cohen’s d was converted to r 2 , only 3.9% of the variance was attributable to the intervention. Pre–post change in the control arm was negligible.
Quality of Life: Functional Assessment of Cancer Therapies—Gynecologic Oncology Group
Mindfulness
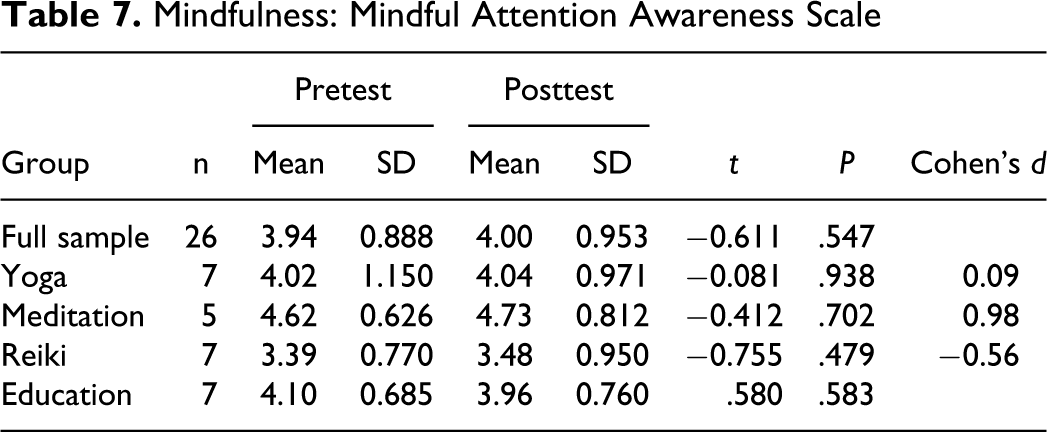
One-way ANOVA revealed that none of the interventions appears to have had a statistically significant effect on mindfulness or capacity to attend to events in the present moment as a method for self-regulation, F(3, 22) = 1.966, P = .149. Little change was noted in the full sample mean between pretest (3.96) and posttest (4.05; Table 7). The within-group scores reflected similar results. Effect size for the meditation arm indicated that the magnitude of the treatment effect was large. Converting Cohen’s d to r 2 shows that 19.3% of the variation was attributable to the meditation intervention.
Mindfulness: Mindful Attention Awareness Scale
Compliance at Home
Per study protocol, participants were asked to maintain a daily log of the time spent practicing the intervention they were learning. Practicing was defined for participants as engaging in an activity learned while taking part in their intervention. Participants could practice yoga postures, engage in meditation, remember a positive experience during Reiki, or review class materials presented in the education/control condition. Twenty-four of the 26 participants submitted logs for analysis. In the full sample, total days of practice ranged from 0 to 36 days yielding a mean of 10.58 days. Similarly, actual minutes of practice ranged from 0 to 1301 minutes yielding an average of 313.68 minutes of practice, or less than 10 minutes per day, over the course of the 6-week study. All participants in the meditation intervention (n = 5) reported practicing meditation during the study with a mean of 22.2 days of practice for 25 minutes per day. Similarly, 5 members of the yoga intervention (n = 7) engaged in daily practice with a mean of 18 days of practice for an average of 14 minutes per day. Although participants in the Reiki condition (n = 7) did not learn a specific symptom management technique, 3 engaged in reflections about their experiences in the study for 5 days on average during the study for 17 minutes each day. Perhaps not surprisingly, only one member in the education/control condition reported review of class materials on 4 days during the study and for less than 2 minutes per day.
Discussion
In the current pilot study, 3 complementary and alternative medicine modalities that included Reiki, yoga, and meditation were evaluated for their feasibility in managing the physical and psychological sequelae of chemotherapy-induced peripheral neuropathy. From the review of existing literature, each of the modalities examined for this study had been shown to have beneficial outcomes with respect to symptom management in people living with cancer and chronic illness. Although this pilot study did not produce results that identified greater effectiveness among the interventions studied; it yielded promising results suggesting that complementary and alternative medicine modalities may improve patient outcomes with respect to psychological distress, quality of life, and neurotoxicity in people living with chemotherapy-induced peripheral neuropathy. In addition, the primary findings included (a) reduction of levels of psychological distress in participants in the yoga and meditation interventions, (b) increased quality of life in all intervention arms, and (c) reduction of neurotoxicity symptoms in all intervention arms with significant worsening of symptoms within the control arm.
Following an extensive review of the literature, we have concluded that this pilot study may be the first to examine the use of Reiki, yoga, or meditation in the chemotherapy-induced peripheral neuropathy population. Furthermore, the findings of this study are consistent with reviews of other controlled studies involving the use of Reiki, yoga, or mindfulness meditation. 27,28,71
A thorough examination of 66 peer-reviewed studies involving Reiki and other biofield therapies in the treatment of a variety of physical conditions found moderate to strong support for evidence that demonstrated the reduction of pain intensity; however, evidence for improvement of quality of life and amelioration of fatigue was much weaker. 72 Within the cancer population, a review of 10 studies that included 6 randomized controlled trials found that following yoga-based interventions participants experienced improvements in stress, quality of life, and sleep. 28 A thoroughgoing meta-analysis of 10 randomized controlled trials by Lin et al 27 mirrored the aforementioned study with significant improvement reported following yoga interventions in cancer populations with respect to levels of anxiety, depression, stress, and distress. However, the effectiveness of the yoga interventions in both reviews could not be determined as a result of variability between the studies and methodological issues. 27,28 Finally, in a well-crafted review of 52 randomized controlled trials studies that examined the neurobiological, biochemical, and clinical effects of meditation, Chiesa and Serretti 40 found that, in addition to neurobiological changes, meditation helped ameliorate the symptoms of physical and mental conditions from hypertension and fibromyalgia to depression and substance dependence.
The study has strengths and limitations that must be acknowledged. Particularly strong components of this study included the diligent attention to design and monitoring of the study, process for random assignment of participants, inclusion of an educational control group, use of trained practitioners, and selection of instruments that were well validated and reflected the targeted outcomes.
Limitations of the study included issues related to sample size and related methodological issues. Recruitment was slow and time constraints prevented development of a larger sample. In addition temporal issues, notably conducting the study in late spring, may have had an impact in adherence as participants began scheduling holidays in lieu of participation. Several positive results emerged from this study; however, the small sample size of just 26 participants and the concomitant lack of power limits the extent to which any of the modalities studied can be regarded as effective for managing the physical and psychological symptoms associated with chemotherapy-induced peripheral neuropathy. Furthermore, the limited sample size also restricted options for complex research design strategies. Thus, in retrospect, we might have considered limiting the number of interventions to 2 rather than 3 interventions and a control group. This might have improved our outcomes.
Conclusion
Chemotherapy-induced peripheral neuropathy is difficult to manage and allopathic treatment options rarely provide total relief from symptoms that interfere with physical and emotional functioning. Complementary and alternative medicine options may provide complementary or adjuvant alternatives to traditional models of treatment for chemotherapy-induced peripheral neuropathy.
Research exploring the use of complementary and alternative medicine interventions in the amelioration of cancer-related physical and psychological distress is in its beginning stages. However, findings within the body of research have been positive and, combined with the findings of this pilot study, indicate that there is an appropriate role for Reiki, yoga, and meditation in the management of chemotherapy-induced peripheral neuropathy. The potentially beneficial physical and psychological changes that emerged from this study warrant further well-defined clinical investigation.
Footnotes
Acknowledgments
The authors would like to acknowledge the George Mason University Center of Consciousness and Transformation for their support of this study.
Author Contributions
All authors have read and approved the manuscript. In addition, each author has played a role in the conceptual development of the research, design of the study and the writing or editing of the manuscript. PGC was involved in all phases of the study and developed the first draft of the manuscript. GCJ participated in the conception, design, implementation of the study, and writing phases of the project. EC participated in the conception, design, and implementation of the study as well as revision of the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research funding for this study was provided by the George Mason University Center for Consciousness and Transformation.
Ethical Approval
The Institutional Review Boards at the Inova Health System and George Mason University approved the study. Both institutions are in Fairfax, Virginia. Trial Registration: U.S. National Institutes of Health – ClinicalTrials.gov Identifier- NCT01569269.