
Abstract
Adolescents and young adults (AYAs) aged 15–39 with cancer face distinct challenges during treatment, with eating consistently emerging as one of the most distressing and underrecognized concerns. At a critical life stage, AYAs must navigate illness-related consequences that profoundly affect well-being. Eating reflects these broader challenges and is identified as a key issue requiring health care attention. To address this, we synthesized evidence on AYAs’ eating experiences and well-being during mealtime-related activities to inform health care practice. Qualitative and mixed-method studies were identified through searches across CINAHL, Embase, PubMed, Scopus, and Web of Science for studies published up to May 2025, supplemented by snowball searches. Of 3214 records, 74 full-text articles were reviewed, and 18 met the inclusion criteria. These represented 302 AYAs, 73 relatives, and 88 health care professionals. Studies were analyzed using Joanna Briggs Institute review methods and GRADE-CERQual to support clinical interpretability. The meta-synthesis identified one core theme: “Eating as an embodied struggle and act of agency,” with three subthemes: (a) living through physical and sensory disruption, (b) carrying the weight of new emotions and shifting relations, and (c) finding ways through gaps in support. Eating emerged as a disrupted, emotionally charged, yet agentic act requiring sensitive, individualized approaches. Thirteen evidence-informed recommendations were developed to guide clinical application. These emphasize early nutritional screening, dietetic support, flexible meal options, respectful family involvement, and psychosocially attuned care. Future research should codevelop and evaluate tailored interventions that address AYAs’ embodied, emotional, and social needs to improve eating-related quality of life during cancer treatment.
Keywords
Introduction
The adolescent and young adult (AYA) cancer population, defined as individuals ages 15–39,1,2 is steadily increasing due to advances in treatment and improved survival rates. 3 This life stage is marked by intense physical, cognitive, and emotional development and represents a transitional period between childhood and adulthood. 4 It is also a time of growing independence, pursuit of education and career goals, and the formation of meaningful relationships.4,5 A cancer diagnosis during this critical stage can severely disrupt normal development, with both disease- and treatment-related side effects hindering social participation, peer integration, and emotional stability. 6
AYAs face unique vulnerabilities shaped by evolving decision-making skills and a strong drive for independence. The emotional burden of cancer is often exacerbated by changes in appearance and body image, functional impairments, and the loss of normalcy.7–9 Consequently, many experience disruptions to their developmental trajectory and emotional well-being.10–12 Research has consistently shown that AYAs report poorer health-related quality of life than other age groups undergoing cancer treatment, largely due to their distinct psychosocial and physical challenges.13,14 Although evidence on AYA needs and experiences is steadily expanding through both quantitative15–18 and qualitative studies11,19–24 that underscore emotional well-being, the impact of cancer on eating behaviors during treatment, rather than only in survivorship, remains insufficiently explored. 25
Like all patients with cancer undergoing treatment, AYAs experience substantial changes in food intake.26,27 Eating, a fundamental necessity of life, is often taken for granted until it becomes a complex and demanding process during cancer therapy. 23 High-emetogenic chemotherapy and other intensive treatments introduce a range of side effects, including appetite loss, dry mouth, nausea, vomiting, and pain, which can drastically diminish nutritional intake and reduce the desire to eat. These disruptions affect overall well-being and energy levels in addition to increasing the risk of nutritional deficiencies, malnutrition, and obesity.28–31
A recent review of AYA health records (n = 93) revealed that nearly half (44%) of AYAs experienced weight loss exceeding 5% during cancer treatment, with the prevalence of underweight increasing by 16% between diagnosis and active treatment. 32 Conversely, treatment with steroids and metabolic changes can induce excessive hunger and weight gain, creating additional barriers to weight management. 33 These fluctuations in weight and nutritional status not only pose physical health risks but also contribute to heightened emotional distress, compounding the already significant burden of cancer on AYAs.
Beyond its physiological role, eating carries deep social, psychological, and cultural meaning. For AYAs, food is not merely sustenance but a central part of social life, pleasure, and identity.24,27 Disruption of normal eating behaviors may thus have wide-reaching consequences on emotional and social well-being. Many AYAs report eating-related challenges as among the most pervasive and distressing challenges during treatment, requiring both personal adjustments and professional support. 34 These eating-related challenges also affect their families and caregivers, who shoulder the practical and emotional burdens of meal planning, nutritional management, and chemotherapy-induced symptoms.35,36
AYAs with cancer experience complex eating difficulties that profoundly influence their physical health, psychological well-being, and social relationships. Yet existing research remains fragmented, with limited integration of perspectives from patients, relatives, and health care professionals to guide responsive and individualized care. Moreover, while barriers to AYA participation in clinical research have been explored, far less is known about their personal preferences, motivations, and decision-making processes. This represents a critical gap, particularly within symptom management research, where meaningful patient engagement is essential to the development of targeted support strategies, personalized interventions, and enhanced professional awareness. Therefore, the aim of this systematic review and meta-synthesis was to synthesize qualitative evidence on adolescents’ and young adults’ (aged 15–39 years) experiences of eating during cancer treatment to inform age-appropriate, person-centered nutritional care.
Materials and Methods
Design
This study is a systematic review of qualitative research findings, using thematic synthesis. The methodology followed the Joanna Briggs Institute (JBI) guidelines for qualitative evidence synthesis. 37 To ensure rigor and transparency, reporting adhered to both Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ).38,39 Particular attention was given to preserving the richness and contextual depth of the original qualitative data, as advocated by Tong et al., 39 while offering a coherent and interpretive analysis. 40 The review protocol was registered in PROSPERO (CRD42024591679).
Search strategy
A comprehensive systematic search was conducted in CINAHL, Embase, PubMed, Scopus, and Web of Science. Search strategies combined free-text terms and controlled vocabulary (e.g., MeSH), tailored to each database’s indexing system, and applied Boolean operators (AND, OR) for effective term combination. The use of exploded subject headings ensured comprehensive inclusion of all relevant cancer types. The initial search revealed challenges due to limited literature and inadequate terminology tagging on the topic. To improve coverage, reference lists of included studies were screened (backward citation tracking), and Google Scholar was used for forward citation tracking to identify additional relevant studies citing key articles.41,42 Authors of included studies were also contacted in June 2025 to identify potential additional sources.
Type of studies
All studies included were original research published in peer-reviewed journals, comprising qualitative studies and mixed-methods studies in which the qualitative data could be analyzed independently of the quantitative components. Search terms were identified and structured according to the PICOTS framework, an abbreviation for population (P), issue of interest (I), context (C), outcome (O), time (T), and study design (S).
Population (P): The primary target group was AYAs, defined as individuals ages 15–39 years. We included mixed-age studies only when AYA perspectives were clearly separable (e.g., age-labeled quotations or stratified analyses) and extracted exclusively data from participants aged 15–39. Studies exploring the perspectives of family members or health care professionals were also included when their insights contributed to a deeper understanding of AYAs’ eating difficulties. Relevant terms included AYAs, health care professionals, family, next-of-kin, and relatives. Issue of Interest (I): As this was a qualitative meta-synthesis, the “issue of interest” was conceptualized broadly to encompass experiences, challenges, needs, and alleviating factors related to eating and nutritional intake during cancer treatment. Search terms included appetite, eating, feeding, food aversion, malnutrition, nausea, nutritional intake, swallowing, and vomiting. To ensure sufficient depth for meaningful synthesis, included studies were required to present at least 100 words. This threshold was set to exclude studies where eating was mentioned only superficially, thereby safeguarding analytic richness, comparability, and interpretive validity. Context (C): Studies conducted during active cancer treatment were included, regardless of setting (e.g., hospital or home). Relevant treatment-related terms included cancer, chemotherapy, high-emetogenic therapy, medication, neoplasms, oncology, and radiation. Outcome (O): The primary outcome of interest was the identification of barriers and facilitators to eating during active cancer treatment, along with factors that health care professionals could influence through enhanced understanding of patients’ lived experiences.
Prior to the final search, we reviewed previous systematic reviews on related topics43–45 and carried out exploratory searches. These preliminary steps underscored the need for broad search terms to capture the full scope of relevant literature. The final strategy, including tailored search strings and database-specific adaptations, was refined and validated in collaboration with a health care librarian. The final search strategy is shown in Table 1.
Search Strategy with Database-Specific Adaptations
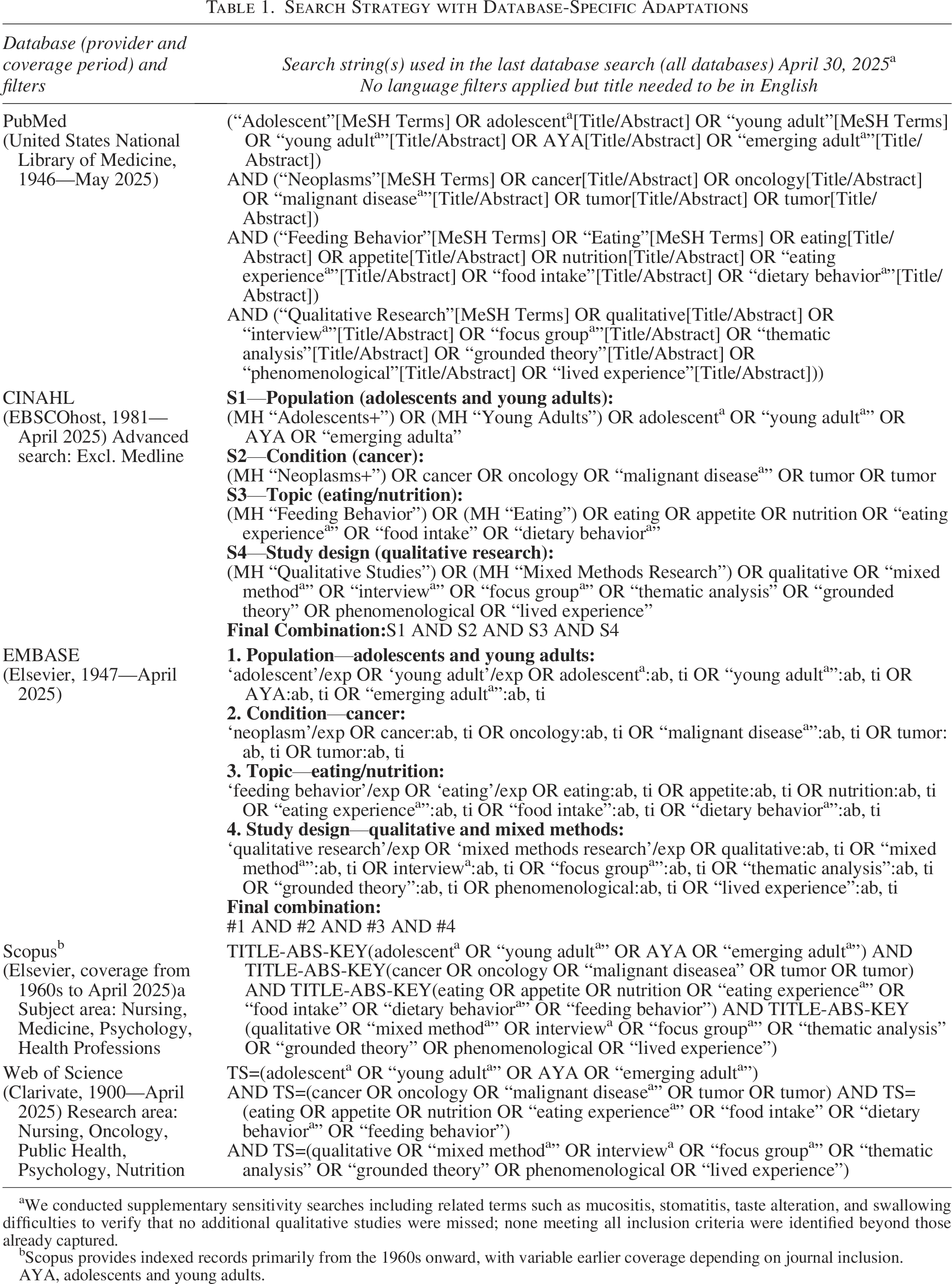
We conducted supplementary sensitivity searches including related terms such as mucositis, stomatitis, taste alteration, and swallowing difficulties to verify that no additional qualitative studies were missed; none meeting all inclusion criteria were identified beyond those already captured.
Scopus provides indexed records primarily from the 1960s onward, with variable earlier coverage depending on journal inclusion.
AYA, adolescents and young adults.
Study inclusion
Titles and abstracts identified through the search strategy were imported into Covidence and independently screened by the two primary authors (MEC and MEK). Full-text screening was conducted by all authors. 46 Discrepancies were resolved by discussion with additional coauthors when needed to reach consensus.
Risk of bias (quality) assessment
In accordance with the ENTREQ guidelines, at least two reviewers (MEC and SSS or RBJ) independently assessed the methodological quality and risk of bias of the included studies using the JBI Critical Appraisal Checklist for Qualitative Research. 37 Discrepancies were addressed through discussion, and a third reviewer (MEK) was involved when necessary to achieve consensus. The appraisal results informed the interpretation and synthesis of the findings by highlighting variations in credibility, methodological rigor, and transferability across studies.
Data synthesis
Qualitative data were synthesized thematically. Extraction followed the elements from Thomas and Harden 47 and was conducted independently by two reviewers (MEC and MEK). Consensus on key statements was reached through larger group discussions. A summary table described study characteristics (author, year, design, participants, methods, and main themes) (see Table 2).
Characteristics of Included Studies Reflecting AYAs’ Eating Experiences
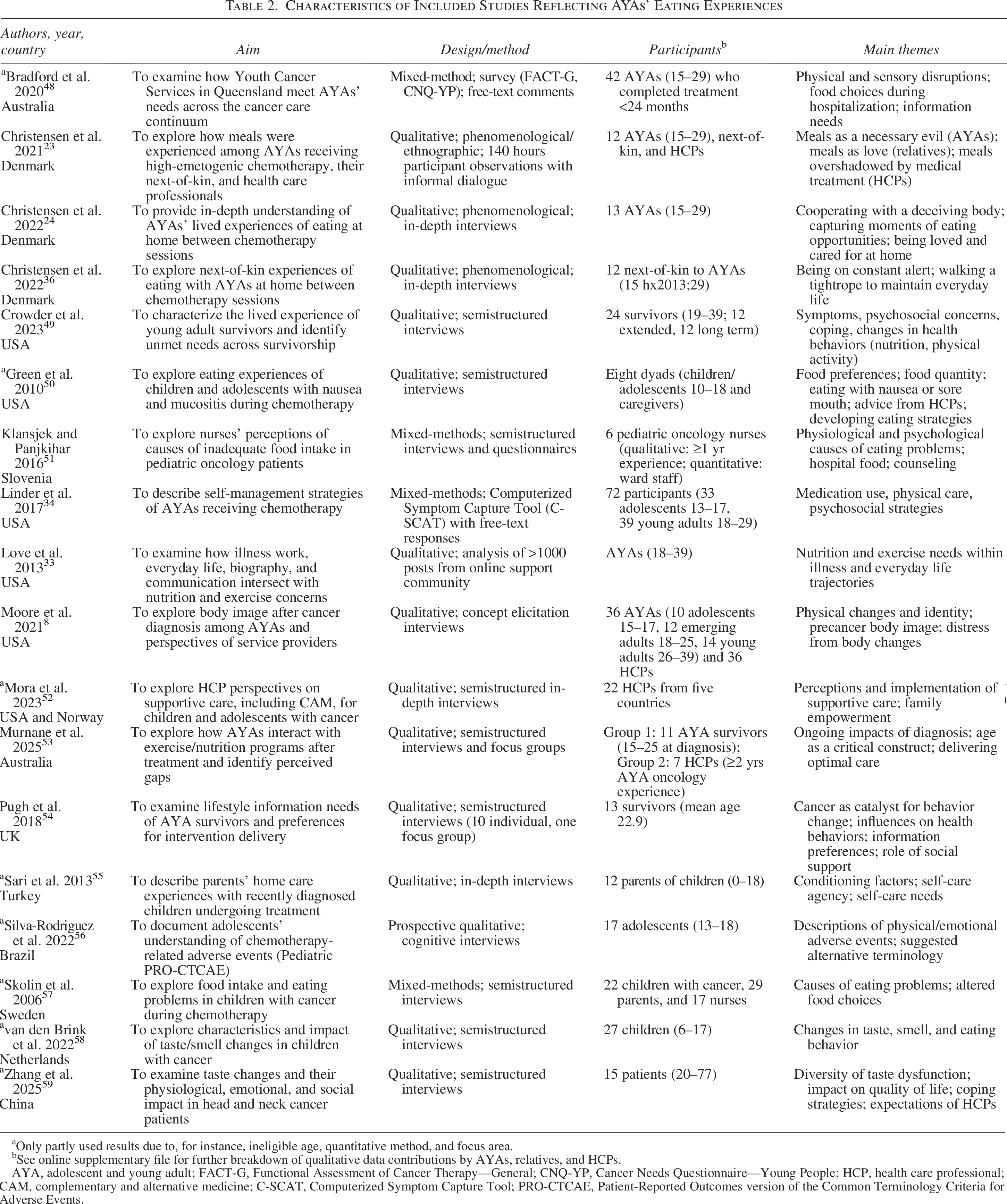
Only partly used results due to, for instance, ineligible age, quantitative method, and focus area.
See online supplementary file for further breakdown of qualitative data contributions by AYAs, relatives, and HCPs.
AYA, adolescent and young adult; FACT-G, Functional Assessment of Cancer Therapy—General; CNQ-YP, Cancer Needs Questionnaire—Young People; HCP, health care professional; CAM, complementary and alternative medicine; C-SCAT, Computerized Symptom Capture Tool; PRO-CTCAE, Patient-Reported Outcomes version of the Common Terminology Criteria for Adverse Events.
Data were coded inductively, with recurring concepts labeled descriptively and grouped into higher-order categories to build a cohesive synthesis. The analysis was guided by Thorne’s 40 interpretive description and inspired by phenomenological concepts of embodiment and lived experience, 60 allowing for deep, iterative engagement with the data. All authors independently reviewed the included articles against the synthesis to ensure that it accurately reflected the original studies’ intent and meaning.
To support clinical translation, findings were assessed using GRADE-CERQual, which evaluates methodological limitations, coherence, adequacy, and relevance of clinical recommendations.61,62 Each finding was assigned a confidence rating (high, moderate, or low). Practical suggestions for clinical incorporation were developed through interpretive synthesis and refined through review team discussions. Author’s expertise in cancer care (MEC, MEK), qualitative methods (MEC, MEK, RBJ), and eating-related challenges (MEC, MEK, SSS) contributed to the depth and applicability of the final synthesis.
Results
Included studies and their main characteristics
A total of 3214 records were identified through database searches, and an additional four studies were located through snowball and citation tracking. After screening 74 full-text articles, 18 studies met the inclusion criteria and were included in the final analysis.8,23,24,33,34,36,48–59 The selection process is illustrated in the PRISMA flowchart in Figure 1.
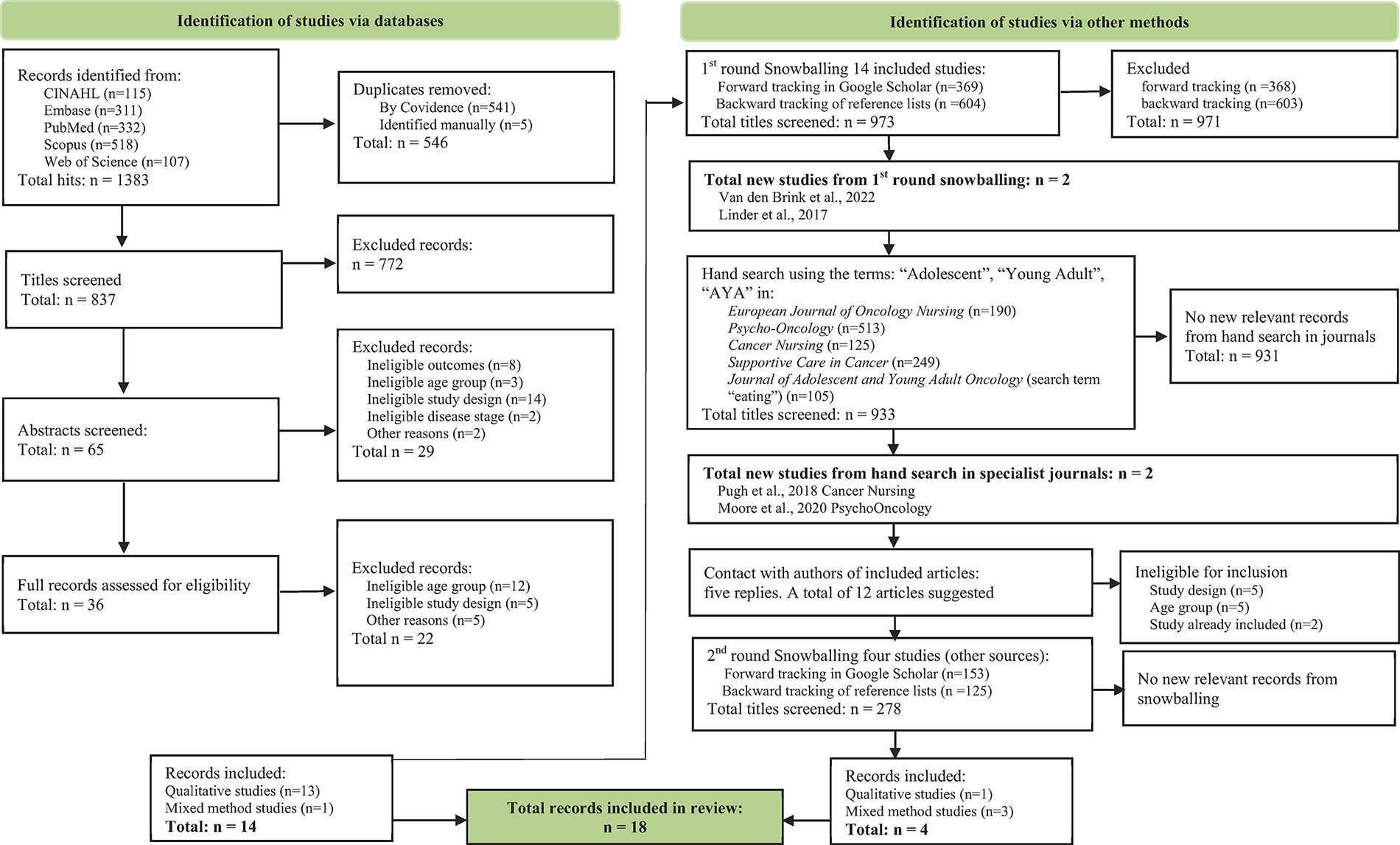
PRISMA flow diagram illustrating the process of study identification, screening, eligibility assessment, and final inclusion in the review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
The 18 included studies were published between 2006 and 2025, covering a wide geographical range across 11 countries. Most studies originated from the USA (n = 6), followed by Denmark (n = 3) and Australia (n = 2), with single studies from Brazil, Turkey, Slovenia, the Netherlands, Sweden, the UK, China, and Norway. Eight studies only partially addressed the topic,48,50,52,55–59 whereas 10 studies investigated it as their primary focus.8,23,24,33,34,36,49,51,53,54 Most participants were undergoing or had recently completed chemotherapy for a range of solid and hematological malignancies, as reflected across the included studies. Common diagnoses included leukemia, lymphoma, sarcoma, and head and neck cancers, where specified. Each of the articles scored between 7 and 10 on methodological quality; see Table 3. The most frequent limitation was limited reflexivity reporting.
Quality Appraisal of the Included Reviews According to JBI Critical Appraisal Tool
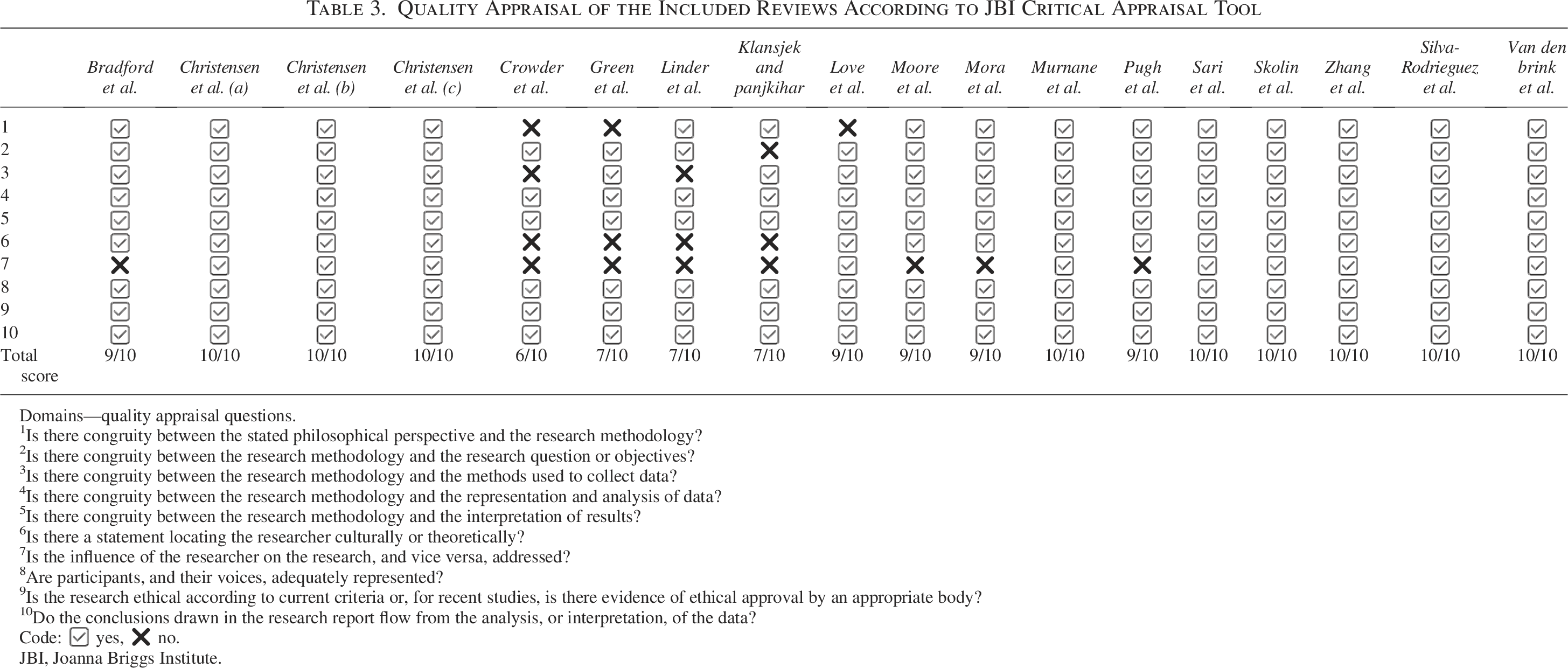
Domains—quality appraisal questions.
1Is there congruity between the stated philosophical perspective and the research methodology?
2Is there congruity between the research methodology and the research question or objectives?
3Is there congruity between the research methodology and the methods used to collect data?
4Is there congruity between the research methodology and the representation and analysis of data?
5Is there congruity between the research methodology and the interpretation of results?
6Is there a statement locating the researcher culturally or theoretically?
7Is the influence of the researcher on the research, and vice versa, addressed?
8Are participants, and their voices, adequately represented?
9Is the research ethical according to current criteria or, for recent studies, is there evidence of ethical approval by an appropriate body?
10Do the conclusions drawn in the research report flow from the analysis, or interpretation, of the data?
Code: ✅ yes, ❌ no.
JBI, Joanna Briggs Institute.
Altogether, qualitative data were provided by 302 AYAs, 73 relatives, and 88 health care professionals. For extracted significant statements across articles, codes, and interpretations informing the synthesis (see Table 4).
Synthesized and Condensed Statements and Thematic Content Associated with the Eating Experience of AYAs
For significant sentences and statements in each included article, see online supplementary file S1, S2 and S3.
AYA, Adolescents and young adults.
Meta-synthesis of qualitative data
We identified one core theme: “Eating as a site of embodied disruption and agency in AYA cancer care.” Eating during cancer treatment was not merely a nutritional task but a disrupted and complex experience shaped by embodied disorientation, relational dynamics, and struggles for agency. Three interconnected subthemes captured this: (a) eating as a physical and sensory struggle, (b) the emotional and relational burden of eating, and (c) coping strategies and support gaps. Cutting across these subthemes, the deeper existential ramifications elucidate how eating during cancer treatment becomes a site of embodied tension and existential negotiation, reflecting both the disruption of illness and the struggle for agency.
Eating as a physical and sensory struggle
Eating was not a routine necessity but a physically and sensorially distressing experience, shaped by treatment-related side effects that disrupted how food was perceived, tolerated, and desired. Taste and smell alterations were especially disruptive, with food often described as metallic, synthetic, overly sweet, or completely bland. These distortions frequently provoked nausea, particularly triggered by smell, and could make even the anticipation of eating intolerable. Over time, such aversions became deeply embedded in daily life, leading many AYAs to avoid specific foods, textures, or eating environments altogether.
Appetite fluctuations and food aversions further compounded the challenges. AYAs reported extreme and unpredictable shifts in appetite, ranging from intense cravings to complete aversion, often occurring within short time frames. These fluctuations were influenced by a complex interplay of factors, including treatment cycles, medication effects (e.g., corticosteroids), and psychological states such as anxiety and depression. The resulting unpredictability made meal planning and food intake a source of frustration, distress, and mental fatigue. In addition, treatment side effects such as mucositis, nausea, and fatigue posed significant physical barriers. Eating was frequently described as painful, exhausting, or both, turning the act of nourishment into a clinical task rather than a source of pleasure or comfort. Many AYAs described forcing themselves to eat simply because they had to, not because they wanted to.
Hospital food rarely alleviated these difficulties. It was often perceived as unfamiliar, unappetizing, and poorly suited to individual preferences, further discouraging intake. In contrast, familiar food from home was highly valued and sometimes the only acceptable source of nutrition. This created a dynamic in which relatives played a pivotal role, responding to sensory and physical needs by preparing or delivering home-cooked meals, adjusting textures, and offering foods that aligned with the AYAs’ shifting preferences. These efforts were both practically helpful and emotionally supportive, though often guided by trial and error.
Health care professionals (HCPs), by contrast, tended to focus on clinical symptom management. Their approach to eating-related challenges was largely pharmacological, prescribing antiemetics or appetite stimulants, with limited attention to sensory, emotional, or contextual dimensions of eating. AYAs and their families noted the absence of personalized or holistic strategies, highlighting disconnect between biomedical care and the lived experience of eating during treatment.
Overall, the physical and sensory challenges related to food were central to AYAs’ daily coping during cancer treatment. These difficulties extended beyond nutritional intake, significantly impacting emotional well-being and family dynamics. This underscores the urgent need for more integrated, patient-centered, and sensory-aware approaches within health care systems. Table 5 outlines recommendations for health care practice, with confidence ratings based on GRADE-CERQual. 61
Implications of “Eating as a Physical and Sensory Struggle” for Health Care
AYA, Adolescents and young adults.
The emotional and relational burden of eating
While the physical challenges of eating during cancer treatment were considerable, the emotional and relational dimensions were equally profound. Eating was an emotionally charged and socially complex experience shaped by power dynamics, care expectations, and shifting family roles. AYAs often described eating as emotionally exhausting; what was once pleasurable and spontaneous became a task they had to force themselves to do, often under pressure from family members or HCPs. Meals carried a sense of obligation and, at times, quiet resentment, making it mentally draining and compounding the physical and emotional fatigue of treatment.
A central emotional theme was the loss of control with routines and choices largely dictated by medical protocols, and thus, food became one of the few remaining domains where AYAs could assert personal agency. Choosing not to eat, or deciding what and when to eat, emerged as symbolic acts of self-determination. For some, refusing food was not merely a response to appetite but a conscious effort to reclaim autonomy within an otherwise tightly controlled existence. This assertion of control, however, often clashed with the intentions of relatives, who typically saw food as an act of care and concern. Families, especially parents, took on the emotional weight of trying to ensure nutritional intake, motivated by both love and fear. When AYAs resisted eating, relatives reported feelings of helplessness, guilt, and frustration. Many described a sense of failing in their caregiving role, especially when food was perceived as one of the few ways they could contribute to their loved one’s well-being. As a result, meal situations frequently became conflict-laden. Tensions arose when encouragement to eat crossed the line into perceived coercion or nagging. AYAs felt misunderstood or pressured, while relatives struggled to balance support with respect for autonomy. This dynamic was marked by mutual emotional strain, with each party navigating the difficult space between care and control.
HCPs were largely peripheral to these relational dynamics. Their involvement was primarily biomedical, focusing on appetite-enhancing medications or symptom control. They rarely engaged with the emotional or interpersonal struggles of eating. This distance left AYAs and families to manage these burdens largely on their own. HCPs did not appear to recognize mealtimes as potential sites of psychological distress or family tension, nor did they provide targeted interventions to support communication or conflict resolution around eating.
Overall, these findings highlight the need to broaden the clinical understanding of eating difficulties beyond symptom management. For AYAs and their families, eating during treatment was intertwined with emotional labor, power dynamics, and relational care, yet these dimensions have received limited recognition and systematic attention within current health care provision. Table 6 outlines recommendations for health care practice, with confidence ratings based on GRADE-CERQual. 61
Implications of “The Emotional and Relational Burden of Eating” for Health Care
AYA, Adolescents and young adults.
Coping strategies and support gaps
Despite substantial sensory, physical, and emotional barriers to eating, AYAs demonstrated resilience and creativity by developing personalized coping strategies. These approaches reflected both a desire for autonomy and the need to adapt eating to the shifting realities of cancer treatment. Individual adaptations were central, with many AYAs constructing flexible, self-guided routines around medication cycles, energy levels, and emotional states. Strategies included experimenting with foods and textures, eating small, frequent meals, and using distractions to make eating more bearable. Learned largely through trial and error, these practices were rooted in a keen awareness of fluctuating tolerance and needs.
Social and environmental modifications played an important complementary role. AYAs reported that eating was significantly easier in informal, relaxed settings, that is, while engaging in casual conversation. Adjustments such as dimming lights, allowing screen time during meals, or reducing portion sizes helped create a more tolerable and less pressured eating experience. Relatives often facilitated these modifications, demonstrating a sensitive awareness of how contextual factors influenced appetite and willingness to eat. Relatives’ practical support was therefore crucial in preparing tailored meals and in creating a more tolerable environment. Their contributions surpassed meal preparation or seeking wished-for foods; they included ongoing observation, experimenting with food presentation and environment, and emotional presence. AYAs valued these efforts when they aligned with their own preferences rather than being experienced as external control. This type of support, however, was largely informal and based on intuition rather than coordinated HCP guidance.
HCPs also acknowledged nutrition as important, but their involvement primarily focused on managing physical symptoms. AYAs and relatives alike noted a lack of practical, emotional, and contextual support from health care staff regarding eating. There was minimal personalization in nutritional advice and little attention to the social or environmental aspects that affected food intake. Furthermore, structured hospital routines often conflicted with the AYAs’ need for individualized, responsive care.
Overall, this theme underscores a critical support gap: while AYAs and their relatives employed meaningful and adaptive coping strategies, these were rarely acknowledged, supported, or integrated into formal care. The findings point to the need for a more holistic and collaborative approach that considers the medical, emotional, relational, and environmental dimensions of eating during cancer treatment. Table 7 outlines recommendations for health care practice, with confidence ratings based on GRADE-CERQual. 61
Implications of “Coping Strategies and Support Gaps” for Health Care
AYA, Adolescents and young adults.
Cutting across themes: disrupted embodiment and the struggle for bodily agency
Findings across themes reveal a profoundly embodied disruption of eating among AYAs with cancer. What was once a natural and pleasurable act became an effortful task. Bodies were experienced as unpredictable, no longer responding reliably to hunger, taste, or satiety. Treatment side effects such as nausea, mucositis, and fatigue disrupted the habitual flow of bodily experience, producing estrangement from one’s own corporeality. The body became an object to be managed rather than a lived source of orientation and pleasure, while smell and taste turned into hostile forces that undermined trust in sensory signals. This reflected a fundamental disintegration of bodily agency and a loss of trust in the body as a reliable medium for engaging with food.
Institutional settings further exacerbated this alienation. Hospital meals, routines, and sterile environments conflicted with the sensory familiarity of everyday life, disrupting the comforting domestic rituals that normally structure eating. In contrast, when AYAs and families recreated relaxed, informal spaces—bringing food from home or eating while watching TV—they attempted to restore spatial belonging and reduce tension.
Eating also unfolded within a distorted sense of time, shaped by treatment regimens and the unpredictability of appetite, cravings, and aversions. Sudden fluctuations created chaos and undermined planning, yet AYAs sought to regain control through personalized routines, timing meals around medications or energy levels. Temporal control thus became central: asserting when and how to eat offered a fragile reclaiming of agency amid the disorientation of illness.
Finally, eating emerged as a relationally charged act. For AYAs, autonomy over food was existential and symbolic, asserting selfhood within the dependencies of illness. For relatives, food embodied love, protection, and the hope of contributing to recovery, while these intentions sometimes collided with AYAs’ need for autonomy. HCPs, meanwhile, remained largely outside these dynamics, focusing on symptom management and giving limited attention to the emotional and interpersonal weight of meals. In this context, eating became a site of identity work, where refusal, selection, or adaptation of food allowed AYAs to defend and express agency, even when the choice not to eat paradoxically became the only available form of control. At the same time, eating permeated everyday life with illness, signifying not only struggle and control but also hope, identity, and the will to live.
Discussion
This systematic review and meta-synthesis provide an integrated understanding of AYAs’ eating experiences during cancer treatment to inform clinical practice. It demonstrates that, for AYAs with cancer, eating is an embodied and relational experience, entangled with identity, autonomy, family dynamics, and existential concerns. Across studies, AYAs described eating as disrupted by treatment-related sensory and physical side effects, emotionally charged within family and social contexts, and insufficiently addressed by health care professionals whose focus often remained on biomedical management. Synthesizing the three subthemes—eating as a physical and sensory struggle, the emotional and relational burden of eating, and coping strategies and support gaps—reveals how eating becomes an existential negotiation of self, relationships, and bodily change. Eating difficulties thus represent a threat to nutritional status and also to agency, social belonging, and identity. These insights underscore the need for care approaches that recognize eating as a lived and relational practice, rather than merely a biomedical problem.
From the synthesis, 13 recommendations were formulated to guide clinical application (Tables 5–7). Although two of these were supported by low-level evidence, this does not diminish their clinical relevance; rather, it underscores the need for greater research focus in these areas. Collectively, the recommendations emphasize the importance of early detection, individualized nutritional support, psychosocial integration, and family involvement, reflecting the central finding that eating is both a challenge and an act of agency for AYAs. Routine nutritional screening is a critical first step, with validated tools such as the Screening Tool for Childhood Cancer (SCAN) and the Patient-Generated Subjective Global Assessment showing strong potential for integration into AYA care pathways to identify and monitor eating difficulties, though further validation in this age group is needed.30,32,63,64 Complementary evidence from an ongoing, prospective, longitudinal, mixed-methods study may further inform the tailoring of such tools for AYAs. 53 Screening must also extend beyond physical symptoms to capture food aversions and psychosocial challenges, thereby positioning eating as a core element of cancer care. This approach aligns with broader calls for holistic AYA symptom assessment that integrates psychological and emotional dimensions to address their most distressing experiences.11,28
Youth-friendly, age-appropriate dietetic support is essential. Evidence shows that AYAs value professionals who use accessible, relatable language and address the emotional as well as physical dimensions of eating.24,65,66 Interdisciplinary teams that integrate dietetic, psychological, and nursing expertise can deliver more holistic care and counter AYAs’ perception that eating difficulties are reduced to mere appetite or nausea management. Another important theme was the need for flexibility around meals. Allowing AYAs to personalize meals, bring food from home, or order snacks outside structured mealtimes supports autonomy and reduces distress tied to hospital routines. This aligns with research emphasizing autonomy and agency as central to AYA resilience and to maintaining connection with family and home life during treatment.4,20 Some authors advice that specialized nutritional counseling should even start before initiation of active cancer treatment. 67
Social eating spaces represent a promising avenue for supportive care. Creating environments where AYAs can share meals with peers or family fosters normalcy, belonging, and identity. Mealtimes carry strong relational meaning, and eating together was often described as comforting and identity-affirming. Prior research highlights the importance of peer connection in reducing isolation and distress, 25 suggesting that mealtimes can be structured opportunities for social support. Designing appealing hospital dining spaces located separately from treatment areas and enhanced with homelike, aesthetic features may further improve the eating experience and reduce negative associations. 66
Addressing emotional and body image concerns is essential. Weight fluctuations, feeding tubes, and steroid-induced changes were described as deeply distressing, consistent with evidence linking body image to psychosocial well-being in AYAs.8,68 Embedding psychosocial support into nutritional care through psychologists, nurses, or peer mentors can help AYAs voice and manage these challenges rather than endure them in silence.
Innovative approaches, such as telehealth and mobile apps for food tracking or meal inspiration, may empower AYAs, but they require careful design to avoid reinforcing disordered eating. 27 Evidence indicates that digital and social media-based interventions are most effective when codesigned with AYAs, providing tailored support for symptom management and engagement.48,67–69 Yet technology cannot substitute for the relational dimensions of care, underscoring the need to support families in their caregiving role. Across studies, family involvement was both indispensable and, at times, a source of tension: caregivers struggled to balance encouragement with respect for autonomy. Targeted education that distinguishes support from pressure may reduce relational strain. Consistent with this, evidence supports family-centered, multidimensional interventions that strengthen coping while preserving AYA independence.10,70,71
Finally, health care professionals need to ask the right questions. Simple, open-ended inquiries such as “What foods sound good to you right now?” or “Are there times when eating feels easier or harder?” invite AYAs to articulate their preferences and experiences. This approach reflects broader recommendations for shared decision-making and the use of patient-centered communication tailored to AYAs’ developmental stage, providing space to express evolving needs.19,65
Collectively, our findings emphasize the importance of tailoring interventions to the unique developmental and psychosocial needs of AYAs. For instance, involving families in mealtime routines may be particularly beneficial for younger AYAs, while promoting autonomy in meal planning might be more suitable for older AYAs. This distinction is required for enhancing the relevance and effectiveness of nutritional support during cancer treatment across the AYA age spectrum. Future priorities include codesigned interventions with AYAs and families, longitudinal research to capture changing needs across the cancer trajectory, and implementation studies to integrate age-appropriate nutritional support into routine oncology care. Institutional policy adoption of nutritional screening and ensuring access to youth-trained dietitians may further strengthen translation into practice.
Strengths and limitations
A key strength of this review is its comprehensive, multilayered search strategy, which combined structured database searches with snowballing, hand-searches, and author contact. This approach minimized the risk of missing relevant studies and captured diverse perspectives in a relatively underexplored field. Transparency was enhanced by using established review frameworks and applying GRADE-CERQual to provide clinical interpretation of findings. Challenges arose from inconsistent indexing and terminology; for instance, Bradford et al. 48 was not initially retrieved due to the absence of eating- or nutrition-related terms and a title that obscured its scope. This underscores both the limitations of keyword-based searches and the responsibility of authors and journals to ensure accurate indexing and precise keywords. While including qualitative and mixed-methods studies enriched the synthesis, variability in design, cultural context, and reporting depth may limit transferability. The strong convergence of themes across studies reinforces confidence in the findings, while the fact that several studies addressed eating only tangentially highlights the need for more targeted research in this area.
Conclusion
Findings highlight the need for holistic, youth-centered, and flexible nutritional support in oncology. Care should integrate sensory adaptation, respect for autonomy, and recognition of the emotional and relational significance of eating. Families require guidance to balance caregiving roles with AYA independence, while health care professionals must move beyond symptom management to address psychosocial and environmental dimensions through individualized strategies. Reframing eating as both a struggle and an act of agency underscores the importance of embedding eating-related support into routine cancer care. Practical measures that reduce distress, foster autonomy, and strengthen mealtime experiences can enhance well-being. By incorporating embodied, emotional, and social dimensions into care, food may be reclaimed not only as sustenance but also as a source of resilience, connection, and quality of life for AYAs during treatment.
Authors’ Contributions
M.E.C.: Conceptualization, methodology, formal analysis, investigation, validation, resources, data curation, writing—original draft, writing—review and editing, visualization, and project administration. R.B.J.: Formal analysis and writing—review and editing. S.S.S.: Formal analysis and writing—review and editing. M.E.K.: Conceptualization, methodology, formal analysis, investigation, validation, resources, data curation, writing—original draft, writing—review and editing, visualization, and supervision.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Ethics Statement
This study is a systematic review and meta-synthesis of previously published research and did not involve the collection of new data from human participants. No identifiable personal data were used. Accordingly, institutional ethics approval and informed consent were not required.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.