
Abstract
Objectives
Ethnicity is a well-established factor in criminal justice decisions, but its impact on forensic psychiatric evaluations—particularly in assessments of competency to stand trial (CST) and mental state at the time of the offense (MSO)—has received limited attention. While clinical and legal predictors are well documented, the role of ethnic background remains unclear, with existing findings often inconsistent, especially between CST and MSO outcomes. This study examines whether defendants’ ethnicity (Jewish vs. Arab) is associated with different CST and MSO outcomes in evaluations conducted at the Jerusalem Mental Health Center.
Method
Archival data from 248 Jewish and Arab defendants evaluated at the Jerusalem Mental Health Center were coded and analyzed. Logistic regression models were used to examine the relationship between ethnicity and CST and MSO outcomes, controlling for criminal history and clinical symptoms. The final dataset included 168 cases for CST and 157 for MSO.
Findings
For MSO decisions, Arab defendants were more likely than Jewish defendants to be assessed as not criminally responsible, while no significant ethnic differences were found in CST outcomes.
Conclusions
These findings highlight the potential influence of ethnicity on forensic psychiatric decisions, particularly in assessments of criminal responsibility. They also shed light on the inconsistent findings in previous research and support theoretical claims regarding attribution processes and intergroup bias—where minority defendants may be perceived either as morally culpable or as psychiatrically dangerous. The results underscore the importance of evaluating how ethnic stereotypes and attributional frameworks shape psychiatric-legal judgments.
Keywords
Introduction
Ethno-racial bias in criminal justice decision-making has been studied extensively in the United States (Berk et al., 2005; MacDonald & Donnelly, 2019; Mitchell, 2005) and Israel (see Rahav et al. (2015) for a review). Scholars explain these disparities through frameworks including social identity and attribution processes (Pettigrew, 1979; Tajfel & Turner, 1979), perceptions of threat (Avni et al., 2024; Feldmeyer & Cochran, 2018; Stephan & Stephan, 1996; Stephan et al., 1999), structural barriers to access to justice (Gutterman, 2022; Lucy, 2020), and broader institutional logics that classify minorities as deviant (Foucault, 2006).
Research on ethnic bias in forensic psychiatry evaluations—particularly competency to stand trial (CST) and mental state at the time of the offense (MSO)—has yielded inconsistent findings (Gonzalez, 2019; Harris & Weiss, 2018). Outside the CJS, however, minority defendants are disproportionately diagnosed with psychotic disorders (Feinstein & Holloway, 2002; Hicks, 2004; Sadock et al., 2015; Thompson, 2010), which are associated both with incompetence and non-responsibility (Gonzalez, 2019; Warren et al., 2006) and with perceptions of dangerousness (Sadock et al., 2015; Thompson, 2010). This paradox challenges the assumptions of Integrated Threat Theory (ITT), which would predict more uniform patterns of bias. Because both possible outcomes—“criminal” for competence and responsibility or “insane” for incompetence and non-responsibility—are negative, it remains unclear how ITT applies in this context.
The complexity deepens when considering CST and MSO assessments. Although often conducted simultaneously (Chauhan et al., 2015; Kois et al., 2017), they differ substantially: CST evaluates current and typically temporary functioning, whereas MSO entails a retrospective judgment about past mental state and its connection to the offense (Gowensmith et al., 2013; Packer, 2013; Svensson et al., 2022; Zapf et al., 2004).
The present study examines ethnic bias in both CST and MSO evaluation outcomes, drawing on the files of Jewish and Arab criminal defendants referred to the Jerusalem Mental Health Center (JMHC). Each evaluation type was analyzed separately, using logistic regression to test whether ethnicity was significantly associated with the outcomes while controlling for different factors.
Ethnicity in the Criminal Justice System: An Overview
Decision-making processes in the CJS are subject to both systematic biases and non-systematic noise, resulting in significant variability in outcomes (Kahneman et al., 2021). Noise may arise from random factors such as fatigue, mood, or time of day (e.g., Danziger et al., 2011), while biases reflect deeper cognitive patterns shaped by social identities and cultural frameworks. Within this context, numerous studies have documented disparities in the treatment of ethnic minority defendants, who face higher rates of arrest, stricter risk assessments, and harsher sentencing compared to majority group members (Baldus et al., 1998; Bridges & Steen, 1998; Hunt, 2015; Kochel et al., 2011; MacDonald & Donnelly, 2019; Rahav et al., 2015).
Several theoretical frameworks help explain this phenomenon. Social Identity Theory posits that individuals favor members of their own group (in-group) while discriminating against members of other groups (out-group), especially when social boundaries are salient (Hodson et al., 2013; Tajfel & Turner, 1979). Building on this, ITT suggests that perceived threats—demographic, economic, or criminal—posed by the out-group intensify hostility and fear toward its members (Feldmeyer & Cochran, 2018; Stephan & Stephan, 1996). These emotional responses can in turn influence how individuals interpret and evaluate others’ behavior.
A key cognitive mechanism underlying such biases is Attribution Theory, which examines how people explain the causes of behavior. In legal settings, attributions can shape perceptions of intent, responsibility, and risk (Albonetti, 1991; Dripps, 2003). Crucially, Ultimate Attribution Error (Pettigrew, 1979) refers to the tendency to attribute negative behaviors of out-group members to internal and stable traits (e.g., aggression, immorality), while interpreting similar behaviors by in-group members as caused by external, situational factors (Chatman & Von Hippel, 2001). This distortion not only perpetuates stereotypes but also impairs objective judgment. Empirical research supports the idea that such biases are embedded in the judicial decision-making process (Beckman & Rodriguez, 2021; Bridges & Steen, 1998; Yamamoto & Maeder, 2017).
In addition to cognitive and perceptual biases, access to justice highlights structural sources of inequality. It refers not just to legal representation or hearing schedules, but to whether defendants can participate fairly and whether institutions uphold legitimacy (Gutterman, 2022; Lucy, 2020). In practice, economic, bureaucratic, linguistic, and cultural barriers continue to limit minority defendants’ ability to exercise their rights (Avnaim-Pesso & Guetzkow, 2025; Lucy, 2020; MacDonald, 1992). Furthermore, legal decision-making is shaped not only by situational biases or barriers to justice but also by deeper classificatory logics—categories of “normal” and “abnormal” that, as Foucault (2006) argued, are historically and institutionally produced and disproportionately mark minority groups as deviant.
Forensic Psychiatry and Ethnicity: A Critical Intersection
One important context for examining these dynamics is forensic psychiatric evaluation, where forensic clinicians are tasked with assessing defendants’ CST and MSO. Both cognitive biases and structural barriers may shape these pivotal determinations. CST concerns the defendant's current ability to understand and participate in legal proceedings, while MSO addresses whether the defendant was legally responsible at the time of the offense, often relating to a potential insanity defense (Adjorlolo et al., 2019; Pirelli et al., 2011).
In the United States, approximately 20–30% of defendants are referred for forensic psychiatric evaluations—a proportion that fluctuates but reflects an overall upward trend in CST referrals. In contrast, MSO evaluations remain comparatively rare (see, e.g., Kois et al., 2021; Morris et al., 2021; Murrie et al., 2023; Warren et al., 2006). A substantial body of literature has explored CST and MSO evaluations, emphasizing their conceptual complexity and proposing improvements to reduce noise and enhance the reliability of decision-making (Acklin & Fuger, 2016; Acklin & Velasquez, 2021; Cheng, 2020; Cole Jr, 2010; Drogin & Kelley, 2020; Fogel et al., 2013; Løvgren et al., 2022; Rogers & Johansson-Love, 2009). While normative research addresses legal standards and assessment protocols (Appelbaum, 2007; Neal & Grisso, 2014), empirical studies have focused on the prevalence and predictors of CST and MSO outcomes. Findings suggest that incompetence is determined in 18–30% of CST cases, and lack of criminal responsibility in 8–12% of MSO cases, based on studies conducted primarily in the United States and Canada (Cochrane et al., 2001; Lawrence et al., 2021; Nicholson & Kugler, 1991).
Predictors of CST and MSO Outcomes
Psychotic and cognitive disorders 1 are consistently identified as the strongest predictors of both incompetence and non-responsibility (Cochrane et al., 2001; Colwell & Gianesini, 2011; Crocker et al., 2002; Gay et al., 2015, 2017; Gonzalez, 2019; Johnson et al., 1990; Johnston, 2022; Pirelli et al., 2011; Rogers et al., 1984; Van Es et al., 2020; Warren et al., 2006; Yaron-Antar et al., 2020). In contrast, substance use has been shown to reduce the likelihood of such findings (Kois et al., 2017; Gowensmith et al., 2013; Rogers et al., 1984).
Demographic and legal variables play a meaningful role in CST evaluations across diverse jurisdictions, including the United States, Canada, and Europe. Female defendants have been found more likely to be deemed incompetent compared to male defendants (Crocker et al., 2002; Pirelli et al., 2011, in Canadian samples). Regarding age, several studies have reported that older defendants exhibit higher rates of incompetence (Cox & Zapf, 2004; Crocker et al., 2002; Warren et al., 2006). However, a large meta-analysis by Pirelli et al. (2011) did not identify a consistent age effect across studies, suggesting that the association may be sample- or context-dependent. Unemployment is another robust predictor of incompetence (Cox & Zapf, 2004; Pirelli et al., 2011), and never having been married has also been linked to incompetence in some samples (Cox & Zapf, 2004; Pirelli et al., 2011). Regarding offense type, findings have been somewhat inconsistent: in some studies, violent offenses were associated with higher rates of incompetence (e.g., Crocker et al., 2002), whereas in others, violent, sexual, or drug-related charges were linked to higher rates of competency (Cox & Zapf, 2004; Pirelli et al., 2011; Warren et al., 2006).
In MSO evaluations, several demographic and legal variables have been shown to influence responsibility outcomes, though findings are not always consistent across studies. Older defendants were more likely to receive insanity or diminished responsibility determinations in some samples (Warren et al., 2004), while very young defendants (under 20) were less likely to succeed with an insanity plea (Cirincione et al., 1995). Female defendants were repeatedly associated with higher rates of insanity or diminished responsibility judgements (Cirincione et al., 1995; Mandarelli et al., 2019; Warren et al., 2004). Education showed mixed effects: higher education was linked to greater likelihood of insanity acquittals in the United States (Cirincione et al., 1995), whereas lower education was associated with diminished responsibility in Italian cases (Mandarelli et al., 2019). The absence of prior arrests or convictions increased the likelihood of insanity (Cirincione et al., 1995; Mandarelli et al., 2019; Warren et al., 2004). Less severe crimes, including certain violent offenses involving known victims, were more often linked to insanity outcomes (Cirincione et al., 1995; Warren et al., 2004), and drug-related offenses were negatively associated with such findings (Warren et al., 2004). In contrast, Johnson et al. (1990) found that defendants judged not responsible were more often involved in serious offenses compared to those judged responsible.
Ethnicity as a Predictor of Forensic Psychiatric Outcomes
The role of ethnicity in CST and MSO evaluations has received less systematic attention, and findings remain inconsistent. In CST evaluations, minority defendants—such as African-Americans in US samples and immigrant defendants in Canadian samples—have been found more likely to be assessed as incompetent (Cox & Zapf, 2004; Crocker et al., 2002; Johnson et al., 1990; McCallum et al., 2015; Pirelli et al., 2011; Warren et al., 2006). In MSO assessments, results are mixed: some studies suggest minorities are more likely to be found not responsible (Warren et al., 2004), others indicate the opposite (Cirincione et al., 1995; Yaron-Antar, 2023), and some report no significant group differences (Daniel et al., 1984; Johnson et al., 1990; Kois et al., 2017).
This variation underscores the importance of context in shaping forensic decisions. Theoretically, these inconsistencies reflect the dual perception of minority defendants as both more dangerous (and therefore responsible) and more psychiatrically impaired (and thus not responsible). Outside the courtroom, minorities are disproportionately diagnosed with psychotic disorders and associated with psychiatric dangerousness (Feinstein & Holloway, 2002; Hicks, 2004; Sadock et al., 2015; Thompson, 2010). In legal evaluations, this creates an interpretive ambiguity: CST and MSO assessments do not offer a straightforward “positive” or “negative” outcome—rather, both findings may reflect forms of perceived threat, either criminal or clinical. In both cases, minority defendants may be viewed as deviating from the “normal” social order (Foucault, 2006), whether through criminal dangerousness or psychiatric instability.
In addition, although CST and MSO are often evaluated simultaneously (Chauhan et al., 2015; Kois et al., 2017), they differ in important ways: CST concerns present and temporary functioning, whereas MSO involves a retrospective and often permanent judgment tied directly to the offense (Gowensmith et al., 2013; Packer, 2013; Svensson et al., 2022; Zapf et al., 2004). These distinctions suggest that evaluators may apply different interpretive frameworks in each context, which in turn may help explain divergent outcomes. Yet, despite the practical overlap between the two assessments, few studies have systematically examined how ethnicity operates across both simultaneously.
Forensic Psychiatry in Israel: Legal and Clinical Implications
In recent years, the relationship between the Criminal Justice System (CJS) and the Mental Health System in Israel has significantly strengthened (Elizur, 2010). Israeli law, drawing on the 19th-century M'Naghten rules, establishes that the presence of a mental illness or intellectual disability is a necessary condition for negating criminal responsibility. However, such a condition alone is not sufficient: exemption from responsibility applies only if, due to the disorder, the defendant was unable to understand the nature of their actions or to refrain from committing them, as stipulated in Section 34-H of the Israeli Penal Code. Moreover, the Israel Mental Health Act of 1991 provides the framework for court-ordered psychiatric assessments and possible hospitalization.
These evaluations are typically conducted in governmental psychiatric hospitals, and—as shown in research from Israel and internationally—the courts tend to accept their recommendations regarding CST and MSO (e.g., Yaron-Antar, 2025; Zapf et al., 2004). Defendants deemed unfit to stand trial or not criminally responsible due to mental disorder may be hospitalized or placed under compulsory outpatient treatment. Recent guidelines issued by the State Attorney's Office in 2024 emphasize the need for forensic reports to explicitly connect clinical findings with legal criteria, enhancing transparency for judicial decision-making. Nonetheless, no binding oversight mechanism currently regulates the precise scope or content of such reports, potentially resulting in variability in practice.
Several studies have examined forensic psychiatric decision-making in Israel. One study explored defendants with psychotic disorders, primarily schizophrenia, who were found not guilty by reason of insanity (NGRI), and highlighted their prior diagnoses of schizophrenia, repeated hospitalizations, and poor treatment compliance (Yaron-Antar et al., 2020). Later studies examined differences between Jewish and Arab defendants in CST and MSO evaluations, finding that Jewish defendants were more often deemed incompetent and not responsible compared to Arab defendants (Yaron-Antar, 2023, 2025). While these studies provide valuable insights, they focused exclusively on homicide cases, limiting their applicability to other types of offenses. This highlights the need for further investigation in Israel, a culturally diverse and divided society (Hasisi & Weitzer, 2007).
The Current Study
The present study investigates how defendant ethnicity (Arab or Jewish) influences the outcomes of forensic psychiatric evaluations in Israel, specifically those assessing CST and MSO. Importantly, in the Israeli context the Arab minority is not only ethnically distinct but also in ongoing conflict with the Jewish majority (Lamont et al., 2016). This enduring intergroup tension, coupled with entrenched perceptions of the “other” as threatening, makes Israel a particularly meaningful setting for examining how ethnicity shapes psychiatric-legal decision-making through dynamics of perceived threat, institutional structures, and cultural divisions (Avni et al., 2024; Hasisi & Weitzer, 2007).
Although prior research has examined ethnicity as a factor in CST or MSO evaluations—primarily in the United States—there is a lack of research directly comparing how the two types of assessments vary by defendants’ ethnicity. In particular, no research has systematically addressed this question in Israel across defendants charged with different types of offenses. The present study therefore builds on the theoretical and empirical insights outlined above to explore this gap within the Israeli forensic context.
The study is guided by two key hypotheses:
First, it is hypothesized that evaluation outcomes will differ by ethnicity, such that Arab and Jewish defendants will be evaluated differently. However, given the theoretical ambiguity—where minority group members may be viewed either as more dangerous and therefore more responsible, or as more psychiatrically impaired and thus less responsible—no specific direction is predicted.
Second, it is hypothesized that ethnic disparities will be more pronounced in MSO evaluations than in CST evaluations. As noted above, the two assessments differ in fundamental ways: MSO involves retrospective judgments concerning the defendant's mental state during the offense and often carries moral and legal significance, while CST focuses on present abilities and is generally more procedural. These differences may affect how evaluators interpret and apply attributional reasoning and group-based perceptions across decision types.
Methods
Data
To examine our hypotheses, we conducted a study at the JMHC in Israel. Ethics approval was obtained from the Helsinki committee of the JMHC and the IRB committee of the Institute of Criminology at the Hebrew University. The JMHC coordinates psychiatric evaluations for the Jerusalem District Criminal Courts. Each file includes the details of the legal and medical procedure (physical and mental) and the opinion of the forensic psychiatrist appointed by court order to examine the CST and MSO, which is the primary document used for data collection.
The opinion consists of several parts: The first part includes technical details of the diagnosed and the diagnosis. The second part refers to the anamnesis, that is, details provided by the diagnosed, and if necessary, by his relatives regarding his past as far as the information exists and is available. This part may include information on development, marital status, education, employment, psychiatric and physiological history, social conditions and criminal background (arrests, charges, etc.). The third part includes the findings of the psychiatric evaluation. Finally, in the fourth part, there is a discussion summarizing what is written in the previous three parts, the decision that was reached (competent/incompetent, responsible/not responsible, or no decision reached), sometimes accompanied by an explanation of its basis, and a recommendation regarding the continuation of the treatment of the case.
Sample
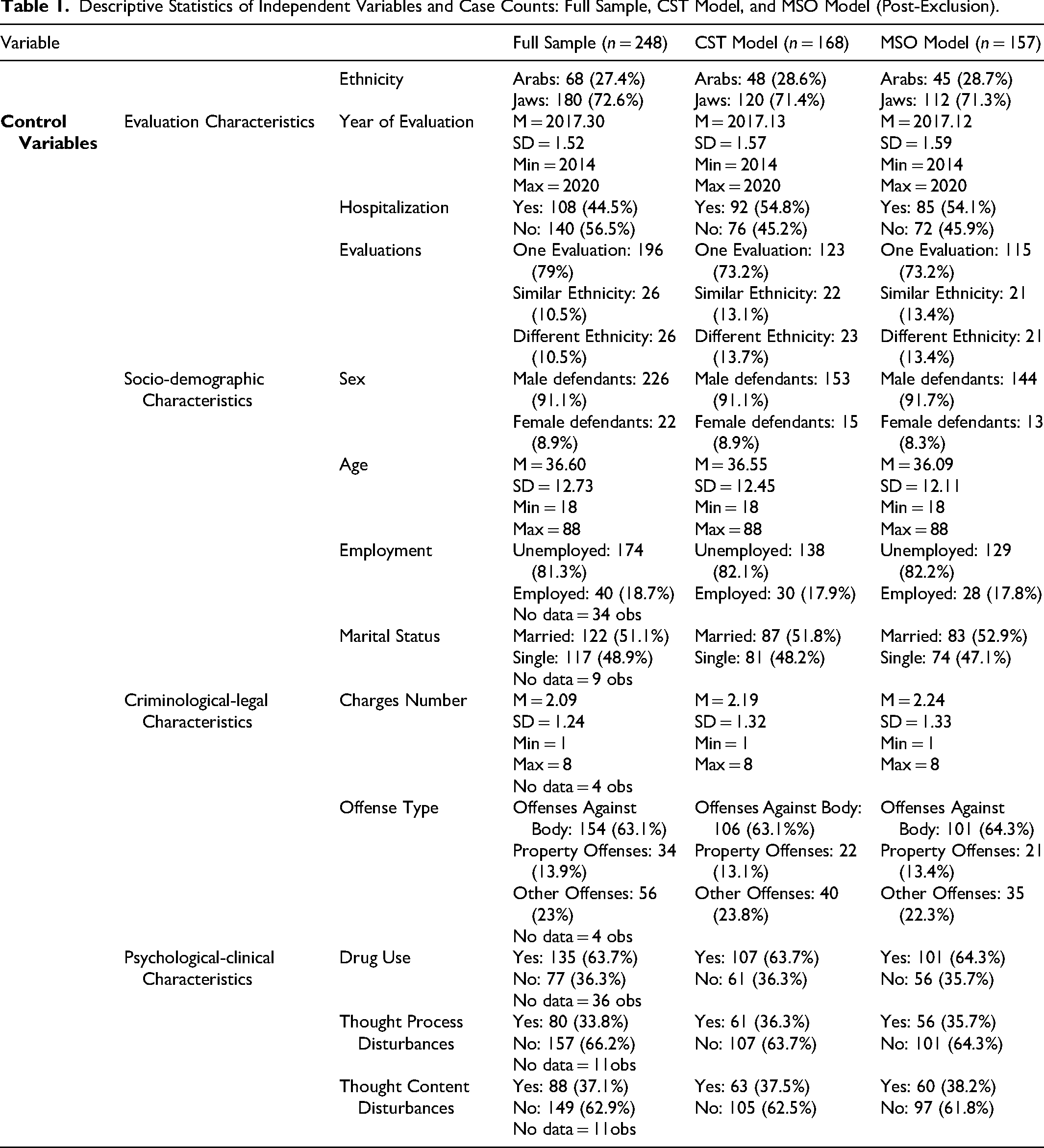
On average, approximately 160 cases per year undergo such evaluations at the JMHC. We identified 1,118 defendants evaluated from 2014–2020 (68% Jewish and 32% Arab), from which we randomly sampled 248 cases. Of these, 180 (73%) were Jewish, and 68 (27%) were Arab, similar to the ratio in the general population in that district. In some cases, either no decision or only a partial one was made, so there was no dependent variable, in which case it was excluded from the data analysis. This includes 14 observations for decisions regarding CST and 27 for decisions regarding MSO. Additional cases were excluded due to missing data on independent variables, resulting in final samples of 168 for CST and 157 for MSO. The proportion of Jewish and Arab defendants remained largely consistent across the final samples for both models (see Table 1).
Descriptive Statistics of Independent Variables and Case Counts: Full Sample, CST Model, and MSO Model (Post-Exclusion).
Coding Process and Variables
Coding proceeded in two stages. In the first stage, we identified and collected information on variables related to sociodemographic, psychiatric, and criminological-legal characteristics, as well as technical aspects of the evaluation. Sociodemographic characteristics included, for example, marital status and employment history. Psychiatric characteristics referred to diagnostic categories and clinical symptoms. In the psychiatric evaluations analyzed in this study, the examiners consistently distinguished between disturbances in the thought process (e.g., disorganized or incoherent thinking, reflecting the flow or structure of thought) and disturbances in thought content and perception (e.g., delusions of persecution or grandeur, auditory or visual hallucinations). This clear and consistent clinical distinction guided our coding process and was reviewed in consultation with a forensic psychiatrist to ensure accuracy. Criminological-legal characteristics included the type of offense (e.g., assault) and prior arrests or convictions. Technical aspects of the evaluation captured factors such as whether the assessment was conducted under inpatient or outpatient conditions and whether a single psychiatrist or a panel performed it.
The text from the opinions with the relevant information was copied directly in order to record the information most accurately. When no reference to these aspects was found in the documents or stated that there was no information regarding a specific figure, it was marked as “no information.” In the second stage, we conducted an inductive content analysis to identify themes and patterns emerging from the text and from this created different categories (Elo & Kyngäs, 2008; Forman & Damschroder, 2007; Grbich, 2007; Mayring, 2004; Pope et al., 2000).
The analysis included an in-depth examination of the opinion, the organization of the information into different variables, and the categorization of those variables. For example, consider the coding process for the clinical feature “symptoms of thought disturbances in the process of thinking.” These disturbances manifested as disruptions in the continuity or pace of thought, such as expressions of disorganized thinking, including associative looseness, word salad, and over-elaboration (American Psychiatric Association, 2013). All of these indicate behaviors that reflect impaired judgment or clinically and legally defective reality testing. During the content analysis, it was found that this is indeed an important element noted by the examiners. Initially, this variable was coded into three categories: the first category included cases where the psychiatrist concluded that there were no symptoms of thought disturbances. Sometimes, the psychiatrist stated this directly and clearly: “No symptoms of thought disturbances observed,” and sometimes it could be inferred: “Organized thinking”/“Organized and speaking coherently.”
The second and third categories included cases where the psychiatrist concluded that there were symptoms of thought disturbances. In the second category, the focus was on the manner of speech: “Tendency toward over-elaboration” or “Impoverished thinking, with no disturbance in pace or flow,” while the third category focused on the nature of the thought process, as reflected in the patient's behavior and speech: “Associative looseness” or “Word salad.” Following exploratory analyses showing no significant difference between the second and third categories, they were merged, resulting in a binary variable with two categories (absence or presence of symptoms of thought disturbances).
A similar coding process was conducted for “symptoms of thought content and perception,” focusing on the presence of delusions, hallucinations, or both. Delusions reflect fixed false beliefs that are resistant to contrary evidence (e.g., delusions of persecution or grandeur), whereas hallucinations involve perceptual experiences in the absence of external stimuli (e.g., auditory or visual hallucinations) (American Psychiatric Association, 2013). In line with the psychiatric evaluations analyzed in this study, examiners consistently classified both delusional thinking and auditory or visual hallucinations as disturbances of thought content, rather than disturbances of thought process. Initially, this variable was coded into distinct categories to differentiate between the types of disturbances (e.g., delusions only, hallucinations only, or both). Following the initial coding, these categories were collapsed into a binary variable reflecting the presence or absence of thought content disturbances. This process ensured consistency with the coding of thought process disturbances, aligning with the goal of capturing clinically significant elements noted in the evaluations.
After coding, we used two dependent variables and 13 independent variables, most of which have been discussed in the literature and had enough observations for the analysis. The dependent variables were the outcome of the assessment: CST (competence/incompetence); MSO (responsible/not responsible). The main independent variable was the defendant's ethnicity (Arab or Jewish). In addition, we controlled for variables tested in previous studies, such as sex, age (Kois & Chauhan, 2018; Mandarelli et al., 2019; Pirelli et al., 2011), and psychiatric characteristics (Gay et al., 2015, 2017), or variables that may have an effect as found in studies that deal with decision-making in the CJS. For example, a mixed composition of judges (black and white) was a moderating factor of discrimination against minority group members in sentencing (Kastellec, 2021). Therefore, in the current study, we controlled for the identity of the evaluator in cases where more than one evaluator was involved and when at least one of them was Jewish and at least one Arab. Notably, there were no cases evaluated solely by Arab psychiatrists. In the final analytic sample, a small number of cases involved mixed evaluation teams (Jewish and Arab psychiatrists together), while most were conducted by Jewish psychiatrists only.
Overall, in each model, the sociodemographic variables were sex (male defendants/female defendants), age (years), employment (yes/no), and marital status (single/married); the psychiatric characteristics were drug use (yes/no), symptoms of thought content and perception (yes/no), and symptoms of disturbances in the thought process (yes/no); the criminological-legal characteristics were charges number, and the type of offense (property, assault and other); and technical characteristics were the year of diagnosis, examination under hospitalization conditions (yes/no), and the composition and ethnic origin of the psychiatrists were coded into three categories: (a) a single psychiatrist (always Jewish); (b) several psychiatrists of the same background (all Jewish); or (c) mixed teams of psychiatrists from different ethnic backgrounds (Jewish and Arab together). As mentioned, no evaluations were conducted solely by Arab psychiatrists, whether by a single evaluator or by a team of the same background. While this distribution reflects the cases included in our analytic sample, it does not necessarily mirror the full range of forensic psychiatric practice in Israel, where it is reasonable to assume that some evaluations are conducted exclusively by Arab psychiatrists. Their absence in our dataset likely reflects their relatively small proportion within the broader system, rather than their complete absence in practice.
Data Analysis
We performed two logistic regression analyses: one for CST (competence = 0, incompetence = 1) and a second for MSO (responsible = 0, not responsible = 1). As mentioned, we controlled clinical, criminological, and sociodemographic variables, as shown in the equation below. The reference category for psychiatrists’ composition was “one psychiatrist,” and for the type of offense, “other offenses.” As mentioned, after removing cases with missing data in the dependent and independent variables for each model, 168 cases remained in the CST analysis and 157 cases in the MSO analysis.
As shown in Table 1, we compared evaluation, sociodemographic, clinical, and criminological characteristics across the full sample and the subsets included in the CST and MSO models. Overall, the descriptive statistics were very similar across these groups, suggesting no meaningful differences in the composition of the analysis samples. The main divergence concerned hospitalization status: among the cases retained for regression, a higher proportion involved inpatient evaluations, whereas in the full dataset outpatient evaluations were more common. This shift is likely to reflect the greater availability and completeness of information in files generated under inpatient conditions, making such cases more likely to be included in the final analyses.
For all analyses, the significance level was set at 5% (α=0.05), and we used two programs: StataSE 16 and JASP 0.16.3.0. Below is the regression equation:
Results
Table 1 presents the descriptive statistics of the sampled cases, all of which involved defendants referred for forensic psychiatric evaluation. In both CST and MSO subsamples, most defendants were male, single, and unemployed. Drug use was relatively common, while disturbances in thought process and content were largely absent. The most frequent type of offense was assault. These characteristics provide a general profile of the evaluation files analyzed. As noted in the data analysis section, the final analytic samples included proportionally more inpatient evaluations, likely because such files contained more complete information, whereas outpatient evaluations were more often excluded due to missing data. This also aligns with the nature of the offenses, which typically spanned a range of violent crimes—some of them more severe—cases that are more frequently referred for inpatient assessment and tend to generate more comprehensive documentation. In addition, while multiple psychiatrists conducted some evaluations, the majority involved a single evaluator. Among the smaller set of multi-evaluator cases, the distribution was nearly identical between teams composed solely of Jewish psychiatrists and mixed teams including both Jewish and Arab psychiatrists.
In addition, we examined whether there was an association between ethnicity and psychiatric characteristics, specifically disturbances in the content of thinking, symptoms of thought disorder, and drug use. Separate chi-square tests were conducted for the cases included in the CST model and for those included in the MSO model. Among defendants included in the CST analysis, no significant ethnic differences were observed in rates of drug use (χ2(1, n = 168) = 0.023, p = .879), symptoms of thought disorder (χ2(1, n = 168) = 0.257, p = .612), or disturbances in the content of thinking (χ2(1, n = 168) = 0.000, p = 1.00). Similarly, among defendants included in the MSO analysis, none of these characteristics differed significantly between Jewish and Arab defendants (drug use: (χ2 (1, n = 157) = 0.0004, p = .985); symptoms of thought disorder: (χ2(1, n = 157) = 0.149, p = .699); disturbances in the content of thinking: (χ2(1, n = 157) = 0.189, p = .664).
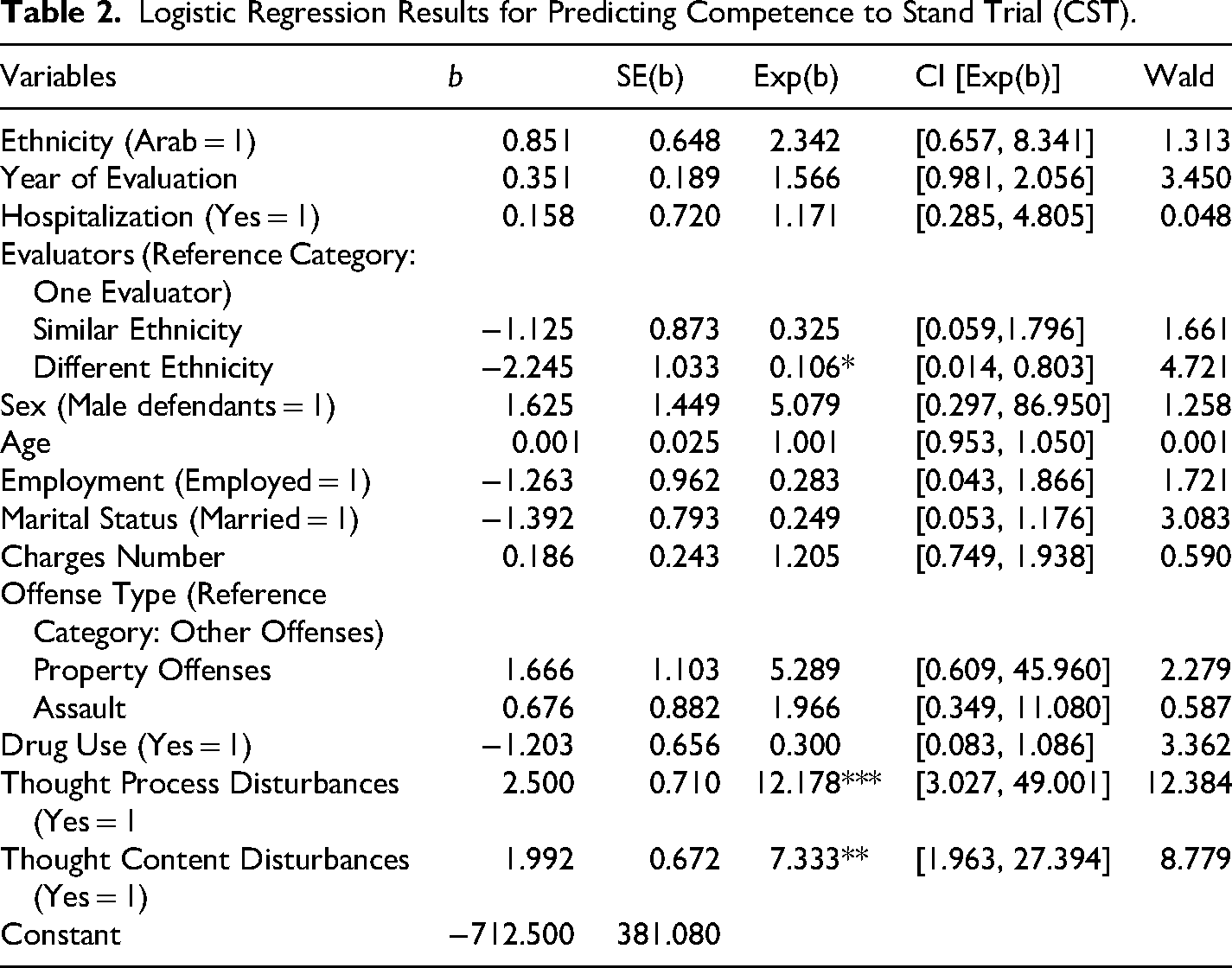
The research findings are presented in Tables 2 and 3. First, we examined the association between ethnicity and CST evaluation outcomes (Table 2). Although the odds ratio is greater than one, which would indicate that Arab defendants’ chances of being found incompetent is higher than Jewish defendants, this difference is not significant. The results do indicate that when there is evidence of disturbances in defendants’ thought processes, the chances of being found incompetent significantly increases by 1,117.8% compared to the absence of those symptoms (χ2(1, n = 168) = 12.384, p < .001). When there is evidence of disturbances in the content of thinking, the chance of being found incompetent significantly increases by 633.3% compared to the absence of those symptoms (χ2(1, n = 168) = 8.779, p = .003). In addition, the chance of being found incompetent significantly decreases by 89.4% when the case includes a group of diagnosticians of different ethnic origins compared to a case that includes a single diagnostician (χ2(1, n = 168) = 4.721, p = .030).
Logistic Regression Results for Predicting Competence to Stand Trial (CST).
Logistic Regression Results for Predicting Mental State at the Time of the Offense (MSO).
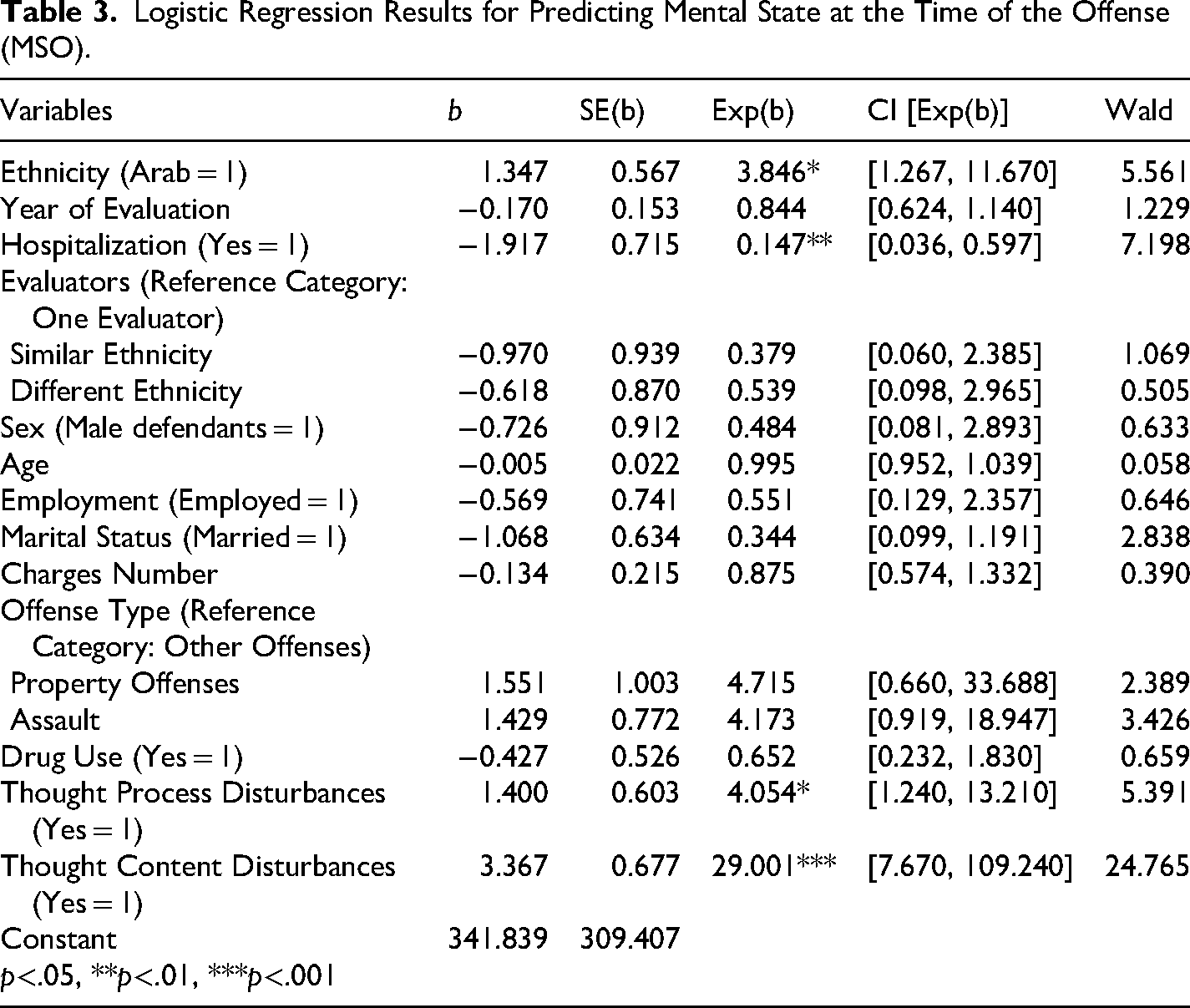
In the second analysis, we examined the association between ethnicity and MSO evaluation outcomes (Table 3). The chance of Arab defendants being found not responsible for their actions was 284.6% higher than the chance of Jews being found not responsible, which was statistically significantly (χ2(1, n = 157) = 5.561, p = .017). Regarding the psychiatric characteristics, when there is evidence of disorders in the content of thinking, the chance of being found not responsible significantly increases by 2,800.1% compared to the absence of those symptoms (χ2(1, n = 157) = 24.765, p < .001). Similarly, when evidence of disturbances in defendants’ thought processes was present, the odds of being found incompetent were 305.4% higher compared to cases in which such symptoms were absent (χ2(1, n = 157) = 5.391, p = .020). In addition, when the diagnosis was made in hospital conditions, the chance of being found not responsible significantly decreases by 85.3% (χ2(1, n = 157) = 7.198, p = .007).
Discussion
This study examined potential ethnic bias in forensic psychiatric decision-making across two evaluations: CST and MSO. In both, outcomes are not inherently “positive”: findings of competence or responsibility mark the defendant as criminal, while findings of incompetence or nonresponsibility mark the defendant as psychiatrically impaired. This duality creates ambiguity distinct from binary legal judgments (e.g., guilty vs. innocent).
Empirically, CST outcomes did not differ by ethnicity, whereas Arab defendants were significantly more likely to be deemed not responsible in MSO evaluations. Theoretically, this pattern reflects the complexity predicted by in-group/out-group frameworks: minority defendants may be perceived as threatening either through presumed criminality or psychiatric instability (two stigmatizing “threats”). MSO's retrospective, offense-tied judgment likely amplifies such biases more than the more procedural, present-focused CST. This pattern also resonates with Ultimate Attribution Error (Pettigrew, 1979): given the distinct features of CST and MSO evaluations (e.g., present and temporary versus retrospective and offense-related), attributions of out-group behavior to internal deficits may operate differently in each context.
Beyond perceptions, structural conditions intersect with these processes. Barriers to access to justice and the under-resourcing of mental-health services for Israel’s Arab population can yield more severe clinical presentations at referral, shaping both psychiatric findings and legal outcomes. Together, these dynamics underscore the need to probe how evaluators reach decisions in ethnically divided contexts. Importantly, such disparities may also compromise the realization of justice for minority defendants, as unequal access to treatment and fairness in evaluation can translate into unequal outcomes in the legal system.
On the practical level, this study highlights the need to improve forensic psychiatric practice in Israel. We observed wide variability in the length and content of evaluation reports, pointing to the value of standardized guidelines that could enhance consistency and reliability. Structured professional judgment tools, shown to reduce bias by ensuring evaluators apply clear criteria, could be integrated into practice to mitigate potential ethnic disparities (Mossman et al., 2007).
Equally important is cultural competence training, which may help evaluators recognize differences in mental health expression, criminal behavior, and risk perception across groups—particularly relevant in a multicultural society like Israel. Clear protocols for documenting evaluators’ reasoning, including supporting evidence, could further reduce variability and enhance fairness. Encouraging evaluators to reflect explicitly on potential biases would strengthen both the accuracy and legitimacy of their assessments. Together, these steps align with principles of access to justice by ensuring not only the formal availability of forensic evaluations but also defendants’ meaningful ability to participate equitably in CST and MSO assessments.
This study has several limitations that also suggest directions for future research. First, the sample was relatively small (248 cases, with about 80 missing key information), limiting the scope of analysis. Future work should expand the number of cases, ideally examining the full population, to allow more robust analyses and descriptive comparisons. Second, missing data may not only reduce statistical power but also systematically bias results. Gaps in documentation could reflect disparities in how information is recorded for different defendants, potentially linked to ethnicity or other factors. Future studies should therefore analyze missingness itself as a source of bias, as it may obscure real differences and highlight barriers to access to justice.
Future research should also examine additional factors that may substantially influence forensic psychiatric decisions. One such factor is the ethnic background of the evaluator, which—although controlled in this study at the level of mixed versus homogeneous teams—warrants a more detailed analysis given its potential to shape interpretations of defendants’ mental states. Another important dimension concerns the ethnicity of the victim, which may be relevant to judicial decision-making from multiple angles. Prior criminological research has emphasized that victim identity can shape how cases are interpreted and processed within the legal system (see, e.g., Factor & Gur-Arye, 2020), and this issue has also been examined in the specific context of CST and MSO evaluations (Yaron-Antar, 2025). This variable, though unavailable in the current dataset, may prove crucial in understanding how intergroup dynamics operate within forensic decision-making.
A further direction is to analyze predictive variables within each ethnic group separately. Subgroup analyses could clarify whether the same clinical, criminological, or contextual predictors operate similarly for Jewish and Arab defendants, or whether distinct patterns emerge. Such an approach would deepen our understanding of how ethnicity intersects with other factors in shaping CST and MSO outcomes, providing a more nuanced view of forensic psychiatric judgments.
Finally, a more systematic exploration of offense types may shed additional light on these findings. Our study encompassed a broad range of offenses, whereas other Israeli research, such as Yaron-Antar (2023, 2025), focused on homicide cases. Interestingly, both our study and Yaron-Antar's study (2023) found an association between defendants’ ethnicity and determinations of criminal responsibility, though in opposite directions: in our data, Arab defendants were more often found not responsible, whereas Yaron-Antar reported that Jewish defendants were more frequently found not responsible. Also, Yaron-Antar's later study (2025) found that Arab defendants were more often deemed competent to stand trial, whereas we found no ethnic differences in competency outcomes. This divergence may reflect the different offense profiles under study, suggesting that the relationship between ethnicity and responsibility determinations is not uniform but may vary depending on the type and of the offense. Although we did not find any differences across offense severity, analysis of a larger sample might reveal systematic differences. Future research would also benefit from considering factors such as the number of injured or fatalities associated with the offense, where such data are available.
A separate limitation relates to generalizability across regions. The results cannot necessarily be generalized to other regions of Israel outside of the Jerusalem district. Collecting information from psychiatric hospitals in other areas may help us examine whether the findings can be generalized or if this phenomenon is unique to a socially and ethnically complex area like Jerusalem. This limitation is particularly salient given the distinctive status of East Jerusalem, where many Arab defendants reside under unique legal and civil arrangements. These conditions may influence both referral patterns and evaluators’ perceptions, making the Jerusalem sample different from other regions. Notably, our dataset did not include information on whether defendants originated from East Jerusalem or other areas. While such information is typically considered as part of the evaluation context, it was not systematically available for analysis in this study. Future research should therefore explore how defendants’ place of residence and corresponding legal status may shape both referral decisions and forensic outcomes.
Conclusions
The study examined biases based on ethnicity in the decision regarding CST and MSO assessments. We found that Arab defendants were more likely than Jewish defendants to be assessed as not responsible for their actions, but there is no clear difference between Arab and Jewish defendants in the likelihood of being found competent to stand trial. The findings provide additional information on the decision-making process among forensic psychiatrists in Israel, a divided society where minority group members may be perceived as dangerous. As mentioned, although the study is not without limitations, mostly related to the sample size, it is essential to thoroughly examine the evaluations of forensic psychiatry from a theoretical and practical point of view. Follow-up studies may also provide more information about the diagnostic procedure and the influence of other factors and shed some light on this critical “black box” of the CJS.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.