
Abstract
Background
The Taiwan Smell Identification Test (TWSIT) was developed and successfully administered in Taiwanese population since 2015. However, for sanitation reason, the original liquid-jar form of this test is not appropriate. The commercialized TWSIT was then re-designed as “scratch-and-sniff” version: the TIBSIT (Top International Biotech, Taipei, Taiwan). This project aims to investigate the normative value of TIBSIT in different age groups and genders.
Methods
Volunteers aged 20 to 80 with no subjective smell loss were recruited in a rhinology clinic. The participants were given full instructions on using the TIBSIT.
Results
Two hundred and nine healthy subjects (female: male =107: 102) were enrolled into this study. The median TIBSIT score in female and male subjects is 47 and 46, respectively. Subjects were further divided into three age groups: (A) 20∼34 years (n = 77), (B) 35∼54 years (n = 77), and (C) 55∼80 years (n = 55). The TIBSIT scores at the tenth percentile value at each age group of male patients are 43, 42 and 37; while the scores at the tenth percentile value at each age group of female patients are 42, 42 and 41. TIBSIT score was significantly and inversely correlated with age (Spearman rho = − 0.20, p = 0.004.).
Conclusion
We established the normative values of the new TIBSIT in different age groups in Taiwan. Future nation-wide screening is needed for more sophisticated norms establishment.
Keywords
Introduction
The sense of smell is important to human beings. It helps people interact with their surroundings and connect with others. Physiologically, olfactory dysfunction adversely affects appetite and nutrition. Yet there are also substantial psychological effects associated with a diminished sense of smell. 1 The sense of smell is also protective, and in the early detection of environmental hazards like smoke or spoiled food. Recent studies are demonstrating that deterioration in olfactory function may be an early sign of multiple neurodegenerative disorders as well.2–4
Due to the importance of olfaction, objective measures of function are valuable. Numerous smell tests have been created, and when validated can provide useful information regarding the differential diagnosis of disease, posttreatment changes, and olfactory outcome after sinonasal surgeries.5,6 Objective smell tests should be reproducible and therefore are generally considered as more accurate than self-reported smell ability.7–9
An important element of objective smell tests is the need for it to be reliable among the specific test population. Recent data posits that smell identification is not universal; thus, smell identification tests should be culturally and regionally validated.6,10–13 For example, though the University of Pennsylvania smell identification test (UPSIT) has widely used worldwide, certain scents like “dill pickle” were not familiar to Taiwanese subjects in one study. 12 As a result, the traditional Chinese edition of UPSIT (TC-UPSIT) was created and while it was validated among Taiwanese people, there were still some odorants in TC-UPSIT were not as familiar for Taiwanese and thus could consider substitution for more common scents.12,13
The Taiwan smell identification test (TWSIT) was subsequently developed to be more relevant for the Taiwanese population (Shen et al). TWSIT consists of eight liquid odorants, which are diluted with odorless propylene glycol in amber-colored jar. 6 Professionals assist in opening and presenting the jars to the subjects when performing the test. Although the cost of this liquid form of this test is cheap, the TWSIT has several shortcomings: 1. The odorants need to be replaced every six months to maintain freshness. 2. There is potential contamination between subjects. 3. Jars could be a vector of disease. As a result, the Top International Biotech Smell Identification Test (TIBSIT) (Top International Biotech, Taipei, Taiwan) was developed to replace TWSIT (Figure 1).
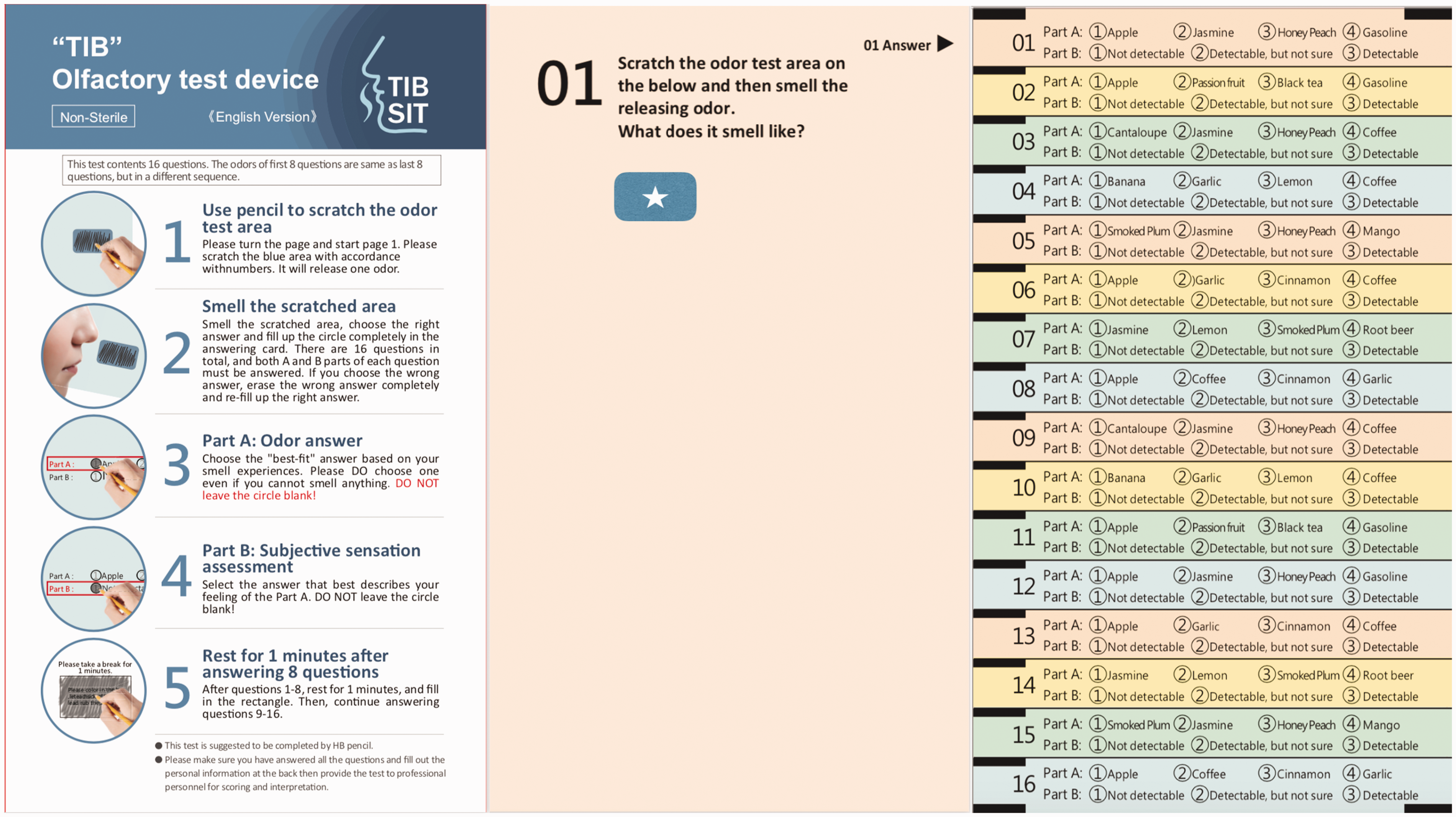
TIB olfactory test device (TIBSIT). The “scratch-and-sniff” with pencil on the sticker (white asterisk). The questionnaire is on the right side.
TIBSIT is a “scratch-and -sniff” form of TWSIT consisting of embedded fragrant microcapsule. The scents of the 8 different odorants are the same as TWSIT, and the format of questionnaire is also the same.
This study aims to establish normative data of the TIBSIT in a healthy Taiwanese population.
Methods
Subjects
This study was approved by the Institutional Review Board of Kuang Tiang General Hospital (#KTGH 10813). Informed consent was obtained from all participants. Taiwanese adult volunteers aged 20 to 80 years with subjectively normal olfaction were recruited from our rhinology clinic. Exclusion criteria included presence of sinonasal diseases, allergy to components of TIBSIT, pregnancy, history of recent head trauma, history of recent upper respiratory tract infection, long term administration of psychiatric agents and drug abusers.
Top International Biotech Smell Identification Test (TIBSIT)
The TIBSIT consists of 16 questions and a questionnaire. The first 8 odorants in question 1–8 are the same as questions 9–16 but in different order. Each page has one “scratch-and-sniff” strip.
The fragrant microcapsule is made of melamine, formaldehyde and fragrant oil by condensation polymerization. This process prevents the fragrant oil from evaporating and thereby allowing storage for 2 years. Then fragrant microcapsules are printed on paper by screen print tech (Figure 2). The subject can complete the test without any assistance by medical personnel by simply scratching the fragrant microcapsules with a pencil and smelling the fragrance released from microcapsules (Figure 1, white asterisk).

The odorant microcapsule and paper printing tech.
After the subject sniffs the odors, they answer the corresponding question to identify it. Each question contains two sub-questions, one is a 4 item multi-choice question where subjects gain 1 point if they chose the correct odorant from the 4 choices; the other is a 3-item question, “not detectable” meaning one can smell nothing at all (0 points)”, “detectable, but not sure” meaning one can smell something but unsure (1 point), and “detectable” meaning one can smell and know exactly what it is (2 points). Thus, a normosmic patient gains 1 point for correctly choosing the odorant and extra 2 points for choosing “detectable” for a maximum score of three points per odorant. However, if the patient chose “detectable” but got the answer wrong, 0 points are scored for this odorant. Hence, there are 48 points in total for 16 questions.
Statistical Analysis
All of the data were recorded as mean values ± standard error of the mean (SEM). Differences were analyzed using independent-samples Mann-Whitney U-test, because TIBSIT score in either male or female group is not normally distributed. The level of significance was set at p < 0.05, and all tests were two tailed. Correlational analyses were performed using Spearman’s rho.
Results
Two hundred and nine subjects with self-reported normal olfactory function were enrolled, including 107 women (mean age: 42.5 ± 3.9 years, range: 21–78 years) and 102 men (mean age: 42.2 ± 4.1 years, range: 20–78 years). The median TIBSIT score in female and male subjects is 47 and 46, respectively. Subjects were further divided into three age groups: (A) 20–34 years (n = 77), (B) 35–54 years (n = 77), and (C) 55–80 years (n = 55). The demographic data, mean TIBSIT score and lower tenth percentile value of each age group are shown in Table 1. The TIBSIT score distribution of each group are shown in Figure 3.
The demographic data, mean TIBSIT score of each age group.
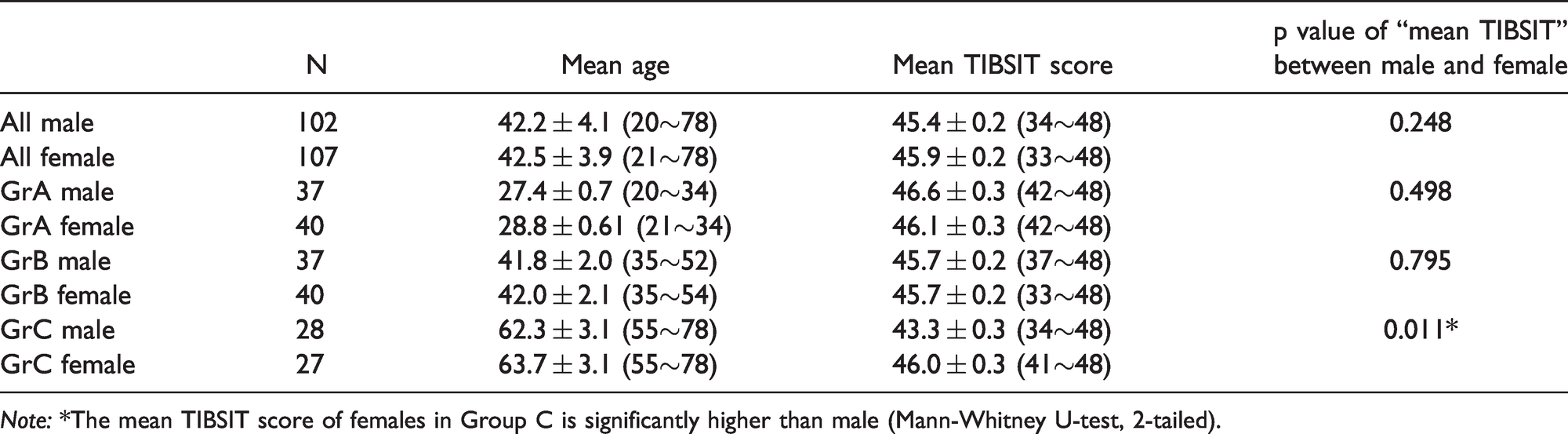
Note: *The mean TIBSIT score of females in Group C is significantly higher than male (Mann-Whitney U-test, 2-tailed).
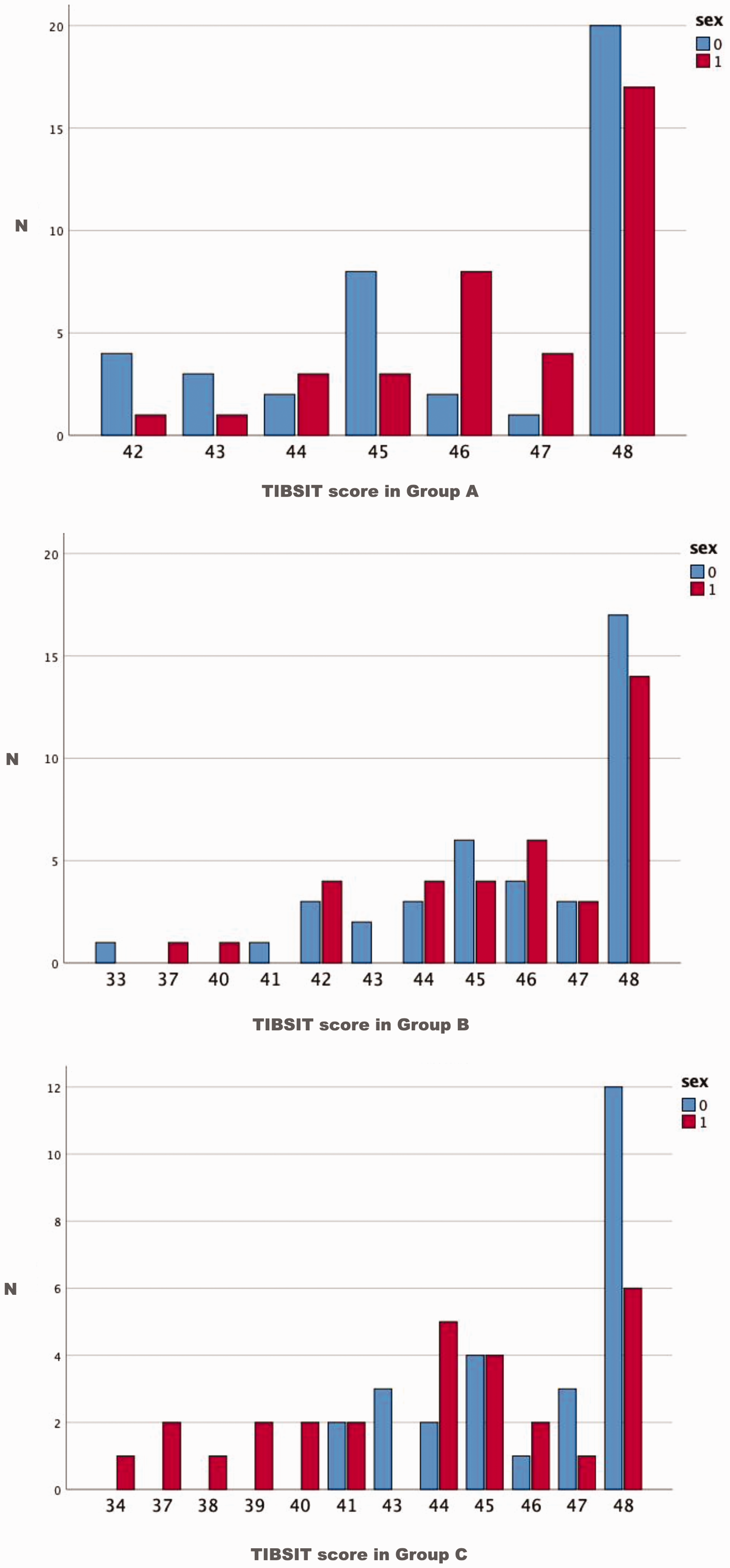
TIBSIT score distribution in Group A (N = 77), Group B(N = 77), Group C(N = 55). (Upper, middle and lower, respectively). Red columns stand for male while blue columns stand for female.
The TIBSIT scores at the tenth percentile value at each age group of male patients are 43, 42 and 37; while the scores at the tenth percentile value at each age group of female patients are 42, 42 and 41. TIBSIT score was significantly and inversely correlated with age (Spearman rho = − 0.20, p = 0.004) (Figure 4, upper part). Male gender was at higher risk for age-related olfactory dysfunction, with a moderate correlation between TIBSIT score and age in male subjects (Spearman rho = –0.31, p = 0.001) (Figure 4, lower part). Older female subjects (Group C) have significantly higher TIBSIT scores than male counterparts (mean: female 46.0 ± 0.3 versus male 43.3 ± 0.3, p = 0.004)

Upper part: TIBSIT score was significantly and inversely correlated with age in all subjects (Spearman rho = − 0.20, p = 0.004.) Lower part: Moderate negative correlation between TIBSIT score and age in male subjects (Spearman rho = –0.31, p = 0.001).
The tenth percentile values of each age group were used to separate the normosmia from the hyposmia subjects.14–16 We define the score range of anosmia by way of binominal distribution probability, the concept was adopted from a previous publication. 6 Hence, we have a normative value table for TIBSIT (Table 2).
The normative data of TIBSIT. Please note that the possibility “zero-points” score in anosmia subjects is extremely low.

Discussion
Many researchers have developed smell tests modified for their own country and region. This is important since a smell test with unfamiliar scents to the test subjects has limited clinical utility.10–13 TWSIT is demonstrated to be as accurate as TC-UPSIT and is cultural-based, time-saving, and easy-to-use in an outpatient clinic as well as in clinical study applications.6,17 The limitations with the re-usable reagents, however, requires modification of this format.
TIBSIT is a commercialized, TWSIT-based smell identification test with the same 8 familiar odorants and questionnaire design as the validated TWSIT. TIBSIT is composed fragrant microcapsules made of melamine, formaldehyde, and fragrant oil that print onto pages of the 16-page booklet and questionnaire. This format is more convenient than the TWSIT without the risk of patient cross contamination and potential disease transmission. Due to the format change, it is necessary to reinvestigate the normative data of the new TIBSIT. Indeed, the normosmic score range of TIBSIT is lower than that of TWSIT which is likely explained by the relatively lower odor intensity of the microcapsules compared with oils in jars. Furthermore, a shortcoming on the literature for the TWIST was the tenth percentile value was not established. The tenth percentile values are widely used in separating the normosmia from the hyposmia subjects, and our results are comparable with other studies in terms of scoring distribution among different smell abilities (e.g normosmia, hyposmia and anosmia).14–16,18
This study also determines the normative value in three age groups based on previous studies.14,16 A decline of smell identification ability is observed with increasing age, and the tenth percentile value in groups A,B,C is 43,42,39 respectively (disregarding gender differences). Though the TIBSIT score was significantly and inversely correlated with age (p = 0.004), the correlation is weak (Spearman rho = − 0.20). Stronger correlation between score and age was found in male gender (Spearman rho = − 0.31, p = 0.001).
The mean TIBSIT score of men and women in Group A and B was not significantly different among these subjects, but men scored lower than women in Group C(p = 0.004). The same phenomenon was not seen in TDI score of aged group using “Sniffin' Sticks” smell test. 14 One possible explanation is that a great number of women smoke in Europe than Asia (19% versus 2%), compared with 38% versus 32% in male counterparts based on WHO: current smoking status. 19 Evidence suggest that smoking impairs the olfactory function; 20 therefore, the higher female smoking prevalence in Europe could decrease their scores to the average of male. The finding in this cohort that women had more keen sense of smell appears to follow the general trend in olfaction research,14,21,22 although there is still some conflicting evidence;23,24 and indeed the absolute numerical differences here are small.
The rationale for determination of an “anosmia” value of this study is based on our previous study. 5 By way of probability calculation or binomial distribution statistical estimation, the chance of obtaining scores more than 11-points for anosmic participants is 0.0285% which is extremely low probability. In our daily practice, either using TWSIT or TIBSIT, anosmic subjects hardly reach scores higher than 11-points. Hence, the threshold of anosmia was set at 11 for all age groups. The score range for hyposmic subjects is between 12-points and the tenth percentile value for that individual’s age and gender.
In summary, the main focus of this study is to determine the normative data of the novel TIBSIT among a Taiwanese population where existing tests like the UPSIT are limited due to cultural differences. This study also is unique in establishing the tenth percentile score of TIBSIT identified, which in this study is similar to other international smell identification tests. Only the aged group had statistically significantly different scores between men and women. The benefits of the TIBSIT make it likely to become more popular in Taiwan, and this normative data aims to assist in clinical practice and research endeavors performed in the Taiwanese population. Similar modifications can likely be made for different cultural and ethnic groups.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by our institutional review board.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.