
Abstract
Background
Various graft materials that are classified as autografts, xenografts, and allografts based on their origin have been used to endoscopically repair skull base defects. Tutoplast® (Tutogen Medical GmbH), an allogeneic natural collagen matrix, is processed through chemical sterilization that preserves tissue biocompatibility and structural integrity.
Objective
To study the safety and efficacy of Tutoplast Fascia Lata and Tutoplast Temporalis Fascia® as primary graft materials in the endoscopic reconstruction of skull base defects of different sizes and etiologies and to compare the outcomes with those of other traditional graft materials based on our experience.
Methods
This is a multi-center retrospective chart review of patients who underwent cerebrospinal fluid leak (CSF) endoscopic reconstruction with Tutoplast Fascia Lata or Tutoplast Temporalis Fascia as either a stand-alone reconstruction material or a part of a multilayer reconstruction depending on the defect at Prince Sultan Military Medical City and King Faisal Specialist Hospital and Research Center in Riyadh, Saudi Arabia, between 2017 and 2020. Our inclusion criteria were CSF leak repair with Tutoplast and a transnasal endoscopic approach. We reviewed demographic data, intraoperative and postoperative complications, repair materials, repair failure, defect size and location.
Results
Tutoplast® was used as the primary graft material in 33 cases. Our main outcome was repair success with lack of post operative CSF leak, observed in 30 cases (90.9%). There was no significant association between postoperative CSF leaks and factors including different defect sizes, defect sites, demographic data, hospitalization duration, or postoperative radiation in oncological cases.
Conclusion
Tutoplast alone or in combination with other materials can be used safely and effectively for skull base defects repair.
Keywords
Introduction
Significant advancements have been made in rhinology and endoscopic skull base surgery over the last 2 decades. These advances are attributed to a number of factors, such as the introduction of angle scopes, navigation systems, and high-definition cameras. This is in addition to the improved understanding of sinonasal and ventral skull base anatomy. Consequently, rhinologists have become more confident in expanding the field in order to address issues associated with different pathologies of the base of the skull.1,2
Wigand described the first endoscopic transnasal skull base repair procedure in 1983. 3 The same principle applied in cerebrospinal fluid (CSF) leak repair was subsequently utilized for skull base reconstruction following tumor resection. 4 In 2006, the use of a vascularized septal flap was described. These flaps allowed for the successful reconstruction of larger defects following the resection of different parts of the base of the skull in order to approach or resect different types of tumors.4–6
Autografts have traditionally been the first choice for skull base repair. These grafts are readily available. Given that the graft is obtained from the same host, it is tolerated without the risks of immune reactions. Despite these advantages, there are some limitations associated with the use of autografts. A separate donor site may be needed to obtain the grafts resulting in additional risks, such as infection, hematoma or seroma formation, and a longer operation time, which are related to additional procedures. Another limitation is the size and availability of the graft, especially in post-oncological resection.7–9
Over the years, different dural substitutes have been used to address the limitations of using autografts. Based on their origin, grafts can be classified as homografts, xenografts, allografts, or alloplastic grafts. Tutoplast® (Tutogen Medical GmbH) is an allogeneic natural collagen matrix that is processed through a chemical sterilization process that preserves tissue biocompatibility and structural integrity.
The objectives of this study were to review our experience in the endoscopic reconstruction of skull base defects of different sizes and etiologies using either Tutoplast Fascia Lata or Tutoplast Temoralis Fascia as a primary reconstructive material and to compare the outcomes with those of other traditional graft materials.
Materials and Methods
This study was approved by the King Faisal Specialist Hospital & Research Center Institutional Review Board. We conducted a retrospective chart review of cases involving CSF leak repair procedures that were performed at Prince Sultan Military Medical City (PSMMC) and at King Faisal Specialist Hospital and Research Center (KFSHRC) between 2017 and 2019 in Riyadh, Saudi Arabia.
The primary outcome measured was the success of the repair. All the procedures were performed by the primary investigator (G. Alokby). The data variables included in this study were patient demographics, diagnosis, location and size of the defect, type and techniques of repair (monolayer or multilayers), materials used in the repair (Tutoplast, vascularized flap, fat), need for transfusion, operative and postoperative complications, use of a lumbar drain, hospitalization period, postoperative CSF leak (graft failure), need for revision, need for postoperative radiotherapy in oncology cases, and follow-up period. In our study, we defined and categorized the defect sizes as small (<1 cm), intermediate (1–2 cm), and large (>2 cm).
Statistical Methods
Statistical analyses were performed using the IMB SPSS version 20 software by the KFSCRC biostatistics department. Continues data are summarized as mean and standard deviation whereas categorical data are summarized as frequencies and percentages. Data comparisons were performed using Chi-square, Fisher’s exact test and t-tests. The results were considered significant if P value was < 0.05.
Surgical Technique
During the repair, we used Tutoplast as a stand-alone layer or as part of a multilayer repair. Regardless of the type of repair, the technique for the application of Tutoplast was as follows.
The first step was to ensure the appropriate exposure of the defect. In this step, the bony edges of the defect should be stripped from the mucosa. The dura was elevated by applying saline-soaked neurosurgical pledgets over the exposed dura and then gently elevating the dura. The Tutoplast graft was fashioned after the dura was elevated so that it was larger than the size of the dural defect. Further, it should be noted that 2 cm should be added on each side of the defect to estimate the size of the graft. It was then hydrated by soaking it in saline. It was placed such that it doubled back on itself over the bony edges of the defect, thereby creating a pocket circumferentially. Oxidized cellulose (Surgicel; Ethicon, Somerville, NJ, USA) was wrapped around a plug of dry Gelfoam (Pfizer, New York, New York) to form cigarette-like wedges that were wedged into these pockets to keep the graft in place and to maintain a circumferential watertight seal around the bony defect. The intranasal ends of the graft were allowed to fold back and make contact with the bone circumferentially, and they were anchored circumferentially by Gelfoam. This technique for skull base repair using an acellular dermal graft was first described by Germani. 10
The graft should be compressed against the bony surfaces. No blood or air should be present between the graft and bone circumferentially. If a vascularized flap is being used, it should be laid over the graft at this point. It is important to note that watertight closure should be achieved prior to placing the flap as the flap may not provide watertight closure; however, it facilitates early healing and epithelization. In our series, Tutoplast was used as the primary reconstructive material to achieve this watertight closure in all the cases.
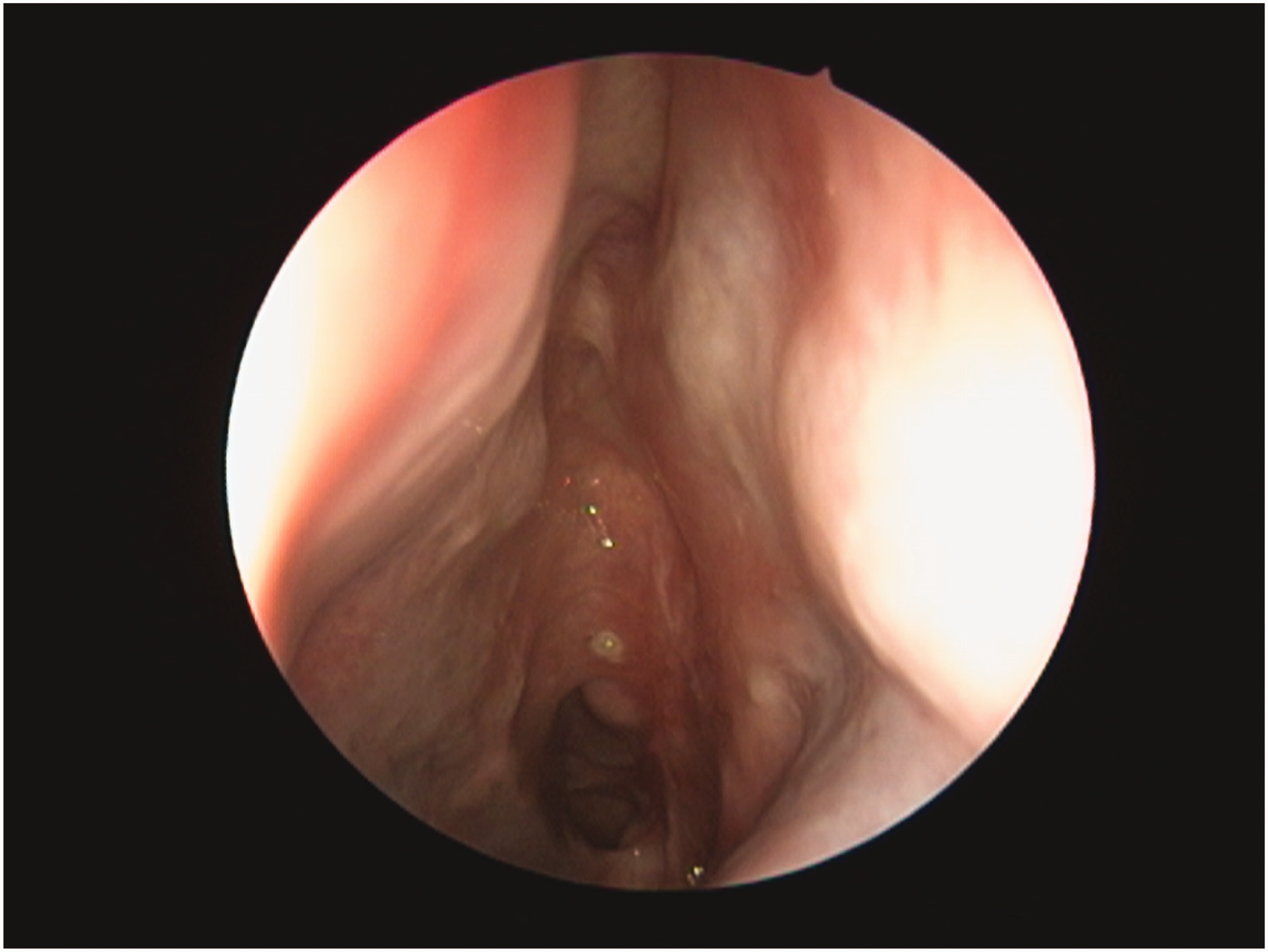
The repair was then covered with Gelfoam, and a merocel pack was compressed against it to keep it in place. The merocel pack should be removed in the clinic after 1 week. Lumbar drain was never used initially at the time of surgery. Figures 1-3 shows the endoscopic appearance of the repair following the application of Tutoplast. Figure 4 shows an endoscopic post operative view after healing.
Results
Among the 44 patients who underwent CSF leak repair procedures within the duration of the study, a total of 33 patients who underwent endoscopic skull base repair involving the use of Tutoplast as the primary graft material were included, and 11 cases were excluded as the repair procedures did not involve Tutoplast. Of these patients, 48.5% were female, and 51.5% were male. The age group was between 17–74 years old, and the mean and SD were 40.15 + 15.27.
The mean number of hospitalization days was 20.75 days. If cases that involved if cases that involved tumor resection or invasive fungal sinusitis wee excluded, the mean number of hospitalizations would drop to 4.3 days. The longer duration of hospitalization for the whole cohort was related to factors other than the skull base repair such as the management of diabetes insipidus or for the long-term systemic antifungal in case of invasive fungal sinusitis rather than for the management of the cerebrospinal fluid leak. All the patients were followed up postoperatively for a minimum of 3 months in the outpatient clinics, with a median follow-up period of 7.95 months.
In 14 cases, the defect was repaired using Tutoplast with a vascularized flap used as an on-lay layer. In nine cases, the defect was repaired using Tutoplast in addition to a free mucosal graft as an on-lay layer. In two cases, we used Tutoplast combined with a vascular flap and fat. In one case, we used fat in addition to Tutoplast, and in another case, we used Tutoplast in addition to Duragen (Integra) as an in-lay layer. In seven cases, the defect was repaired using Tutoplast alone. In all cases, the application of tutoplast was done using the technique described above and it achieved watertight closure when challenged with Valsalva maneuver. The use of vascularized flap was limited to cases with high flow leak or to cases with large defects. The main purpose of using fat was to obliterate dead space such as following clival tumor resection.
Regarding the defect sizes, small defects were identified in seven (21.2%) patients, intermediate defects were found in 16 (48.5%) patients, and large defects were found in 10 (30.3%) patients. We used Tutoplast Temporalis Fascia for small defects and Tutoplast Fascia Lata for intermediate and large defects as Tutoplast Temporalis Fascia comes in a size of 2 × 3 cm whereas Tutoplast Facia Lata comes in a larger size of 4 × 5 cm and 6 × 8 cm
The etiologies that lead to the skull base defects are presented in Table 1. Table 2 presents the locations of the defects.
Etiology of CSF Leak in the case series.

Location of the skull base defect in the case series.

The primary outcome of this study was to determine if a Tutoplast graft could be used as a safe and effective option for successful skull base repair, and success was defined as the absence of postoperative CSF leakage. The defects in 30 (90.91%) cases were successfully repaired with Tutoplast. On the other hand, three (9.09%) patients developed a postoperative CSF leak.
Two of the three cases involved obese patients who had a high flow leak. Both these cases were managed with a lumber drain alone, and they did not require a revision procedure; The defect sizes were intermediate and large, respectively. One of the graft failure cases required revision as the leak did not stop following a lumbar drain. In this case, the recurrence of CSF rhinorrhea occurred within 1 month of the initial repair.postoperative complications were observed in one patient who developed postoperative pulmonary embolism on the 3rd post operative day.
Seventeen patients (51.5%) and five patients (15.2%) were obese and extremely obese, respectively. There was no significant correlation between the body mass index (BMI) and graft failure (p = 0.335). There was also no statistically significant link between the occurrence of a postoperative CSF leak and other factors, including different defect sizes (small p = 0.9, medium p = 0.9, large p = 0.22) defect sites, gender (p = 0.6), age (P = 0.98) revision cases (p = 0.99), the use of vascularized flap (p = 0.067) or postoperative radiation in oncological cases (p = 0.23).

View by 70 degree nasal endoscope of reconstruction of skull base using Tutoplast Fascia late after anterior skull base resection.

View by 30 nasal endoscope after repair of large skull base defect involving the left cribriform plate and fovea ethmoidalis using Tutoplast Temoralis facia.

View by 30 nasal endoscope after repair of large seller defect after the resection of giant pituitary adenoma using Tutoplast Facia late.
View by a 30 degree nasal endoscope showing a completely healed left sided skull base defect that was repaired using Tutoplast Facia Lata.
Discussion
Different materials have been successfully used for skull base repair. It is important for any external material that is implanted in a patient to be well tolerated by the host without causing a foreign body reaction and to integrate with the surrounding tissues. 2 The implant needs to have good handling properties so that it can be well positioned at the defect site, and it must have sufficient strength to form a watertight barrier.1,2,6 Although the use of a synthetic dural substitute results in additional expanse, it is counteracted by the shorter operative time. 10
Different materials have been used over the years as dural substitutes. These include allografts, xenografts, and other synthetic materials. In the mid-1900s, polymer-derived materials, such as Dacron and Orlon, were popular. However, high infection rates, the inability of the material to integrate with the surrounding dura, and foreign body encapsulation were commonly encountered and eventually lead to the discontinuation of their use. 2
Since then, different materials have been introduced and have been demonstrated to be well tolerated and effective in repairing skull base defects.4,5 The main principles for skull base repair remain constant, and they are applicable regardless of the material being used. It is important to be able to effectively visualize the defect. Any herniating meningocele must be cauterized and removed so that all the edges of the defect are seen. The bony edges of the defect should be identified and smoothed. This may make the defect larger. However, having a well-defined defect with smooth edges helps in laying the graft down against the bony margins. All the mucosa around the defect should be removed so that the graft lays against the bare bone, and the formation of a mucocele is avoided. This step will help the graft stay in its place without the secretory mucosa moving it or forming a mucocele at a later time.7,8 A watertight closure should be achieved. This is accomplished by using a meticulous surgical technique and via the use of a reconstructive material that can withstand the harsh nasal environment 6 with the use of a vascularized flap reserved for cases with a high risk of a postoperative CSF leak.6,9,11
On applying these principles, different dural substitutes have been shown to produce an outcome similar to that of autografts.4,10,12,13
Tutoplast® Fascia Lata and Tutoplast Temporalis Fascia (Tutogen Medical GmbH) are allogeneic natural collagen matrices that are processed through a chemical sterilization process that preserves tissue biocompatibility and structural integrity.
In our case series, both have been proven to be suitable options for facilitating watertight closure that is well tolerated by the host. It is noted that since Tutoplast Fascia Lata is large in size, it is more suitable for larger defects that may result from oncological resection.
In this article, we have reported our experiences in using Tutoplast Fascia Lata or Tutoplast Temoralis Fascia for skull base repair. To our knowledge, this report includes the largest series of cases involving the use of this material in a purely endoscopic nasal approach. We have also reported on the successful repair of defects in different subsets of the ventral skull base and in the case of different types of defects, including large defects and defects with high flow CSF leaks.
Cavallo et al. published a report regarding their experience in using Tutoplast Pericardium. Tutoplast Pericardium is a homograft that undergoes the same Tutoplast sterilization process as Tutoplast Facia Lata and Facia Temporalis. It has a thickness of 0.3 – 0.5 mm and comes in a variety of sizes. Cavallo et al. series included 21 patients with suprasellar lesions, and skull base reconstruction was performed using a multilayer repair procedure involving an allogeneic pericardium that was placed intra- or extradurally and another layer of solid support provided by the bone substitute material, Lactosorb (Walter Lorenz Surgical). The CSF leak rate was 9.5%. No patients in the series developed meningitis. 14
Divitiis et al. published a report that included a series of 11 patients diagnosed with meningioma who underwent transnasal endoscopic resection. The anterior cranial floor was reconstructed in a multilayered fashion with a collagen sponge matrix, Tutoplast, and a resorbable solid material (Lactosorb). Three patients developed a postoperative CSF leak that was successfully repaired by a revision surgery. 15 In another series, Cavallo et al. used the same technique in the repair of the skull base following resection in 21 patients diagnosed with craniopharyngioma. The postoperative CSF leak rate was 16.7%. 16
In a recent multicenter observational cohort study that included a total of 187 cases that underwent skull base reconstruction following resection of skull base tumors, Tutoplast Facia Lata was used in one case. However, the study does not state if that case had intraoperative CSF rhinorrhea or not. In that study no adverse reaction was reported with the use of Tutoplast. 17
In our experince, there was no statistically significant association between post-operative CSF leak and the different variables studied. It is worth mentioning that other studies has found an association between CSF leak and a number of variables including elevated BMI, defect size, defect location and high flow leak. 17 This could be attributed to the population size which is one of the limitations of this study.
Conclusion
Tutoplast can be safely and effectively used as a primary graft material for skull base defect repair either as a stand alone layer or as part of a multilayer repair. The incidence of a postoperative CSF leak with the use of Tutoplast is at least within the same range as that of other materials.
Footnotes
Authors’ Note
Poster Presentation at the American Rhinologic Society annual meeting, held on September 2020.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed that they did not receive financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.