
Abstract
Objectives:
The main sites, clinical symptoms, and causal elements linked with pseudomeningoceles at the cranial base are sought by this thorough study. Apart from organizing present data to support therapeutic decision-making, it aims to evaluate diagnostic techniques and the appropriate course of action.
Methods:
Using the terms “skull base” AND/OR “pseudomeningocele,” a thorough search was done in the MEDLINE, PubMed, and Cochrane databases. Articles offering explicit data on the localization and management of pseudomeningocele published in English, French, or Spanish were taken into consideration. Review papers, case studies, and case reports were taken into consideration; reviews, conference abstracts, and papers lacking enough or inaccessible data were turned away. Data gathered covered demographics, location, cause, presentation, diagnosis tools, management strategies, and results.
Results:
Twenty 29-person trials were examined. The primary location of pseudomeningocele development was the sphenoid bone (31%), followed by the posterior cerebral fossa (44.8%). At 42.9%, the main etiology was iatrogenic; traumatic reasons came second at 34.5%. Mostly post-surgical, these factors were blamed. Magnetic resonance imaging was the main imaging modality in 79.3% of cases; computed tomography was used in 62.1% of those cases. Though for most individuals, surgical intervention proved to be the definitive cure, initial conservative treatment was tried. There was limited follow-up data; most patients showed neither morbidity nor mortality. Mostly, preventing problems depends on fast diagnosis and suitable intervention.
Conclusion:
Skull base pseudomeningoceles are rare events that are sometimes missed due to their uncertain appearance and diagnostic difficulties. This study emphasizes how important quick imaging and improved clinical awareness are to guide management decisions. Although traditional methods are usually used, in complicated or unresolved cases, surgical intervention is usually justified. These findings highlight the need for raising awareness and thorough documentation in order to enhance the results for the impacted individuals.
Keywords
Introduction
Although meningoceles are heavily studied in the literature, their prefixed counterpart is rarely addressed. The term “pseudomeningocele” is a term used to describe a non-arachnoid-lined collection of extravasated cerebrospinal fluid (CSF) arising from a dural tear. 1 The etiology of pseudomeningocele formation can be classified into 3 main categories: iatrogenic, congenital, and traumatic. Our review aims to provide a multifaceted review of anterior skull base pseudomeningoceles. A deeper understanding of this phenomenon will provide the infrastructure for better clinical outcomes through earlier detection and better management.
The clinical presentation of pseudomeningoceles varies depending on the site and can range from headache, nausea, and vomiting to more serious neurological manifestations affecting hearing and vision.2 -4 Some articles reported retropharyngeal pseudomeningoceles in which patients presented with dysphagia and neck mass.3,5,6
In the literature, several studies reported that patients are asymptomatic and diagnosed incidentally.7,8 Magnetic resonance imaging (MRI) and/or computed tomography (CT) scans are essential radiological modalities to establish the diagnosis, locate the origin and extension of a pseudomeningocele, and guide the physician toward finding a suitable approach for treatment.7 -9
Based on evidence in the literature, the treatment of pseudomeningoceles is initially conservative and includes lumbar drains. However, surgical intervention is considered the definitive treatment.4,7,9
The main objective of this scoping review is to determine the most common sites of pseudomeningoceles, their clinical presentation, and the main etiology that contributes to their formation, as well as to evaluate the optimal management that can be used to treat such lesions.
Materials and Methods
Study Design and Search Strategy
This comprehensive literature review was performed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guideline through major databases such as MEDLINE, PubMed, Cochrane, and Google Scholar articles, using the terms “skull base” (OR)/(AND) “pseudomeningocele.”
Selection Criteria and Screening Process
Two authors (Naif Alotaibi and Kholoud Alamari) performed an independent review of the titles and abstracts of the articles, selected relevant articles, and obtained their full texts. The articles investigated were limited to human studies only.
The inclusion criteria included all published articles related to the site and the management of pseudomeningoceles in English, French, and Spanish, with no restriction based on age or ethnicity.
The exclusion criteria included duplicates, reviews, editorial articles, unpublished data, conference abstracts, materials inaccessible due to language restrictions, and studies with missing data on the site and management of pseudomeningoceles.
The review contains retrieved and screened articles that meet the eligibility criteria, as well as a reference list of selected articles scanned for additional studies.
Data Extraction and Synthesis of Result
A total of 141 articles were reviewed, and 75 articles were included after excluding duplication. Of the 31 full-text articles that were obtained and reviewed, 19 articles met our inclusion criteria, and 1 article met the inclusion criteria for cross-reference.
The 2 researchers independently extracted data from the included studies using a standardized Excel extraction spreadsheet containing baseline characteristics such as author’s name, country, year of publication, sample size, and demographic data; further details included the site, etiology, and clinical presentation of pseudomeningoceles; then, the approach to diagnosis, treatment, and the follow-up duration; and finally, the data of outcomes, morbidities, and mortality.
Epidemiology
This review includes a total of 20 studies: 14/20 (70%) case reports, 5/20 (25%) case series, and 1/20 (5%) retrospective review. Most of the articles were published in the USA (7/20), followed by India (3/20), the UK, and Turkey jointly (2/20), as well as single studies (1/20) from Australia, Belgium, Japan, South Korea, Pakistan, and Spain. Almost all articles (19/20 or 95%) were obtained from a single center, and only 1 case series (1/20 or 5%) was from a multicenter. 10 The sample size included 29 patients, among whom were 51.7% (15/29) males, 37.9% (11/29) females, and 10.3% (3/29) persons of unspecified gender. High variability in the sample age was observed, ranging from <1 to 70 years, with 6.9% (2/29) in which patient age was not mentioned. Table 1 shows a summary of the included articles.
Summary of the cases reported in the literature.
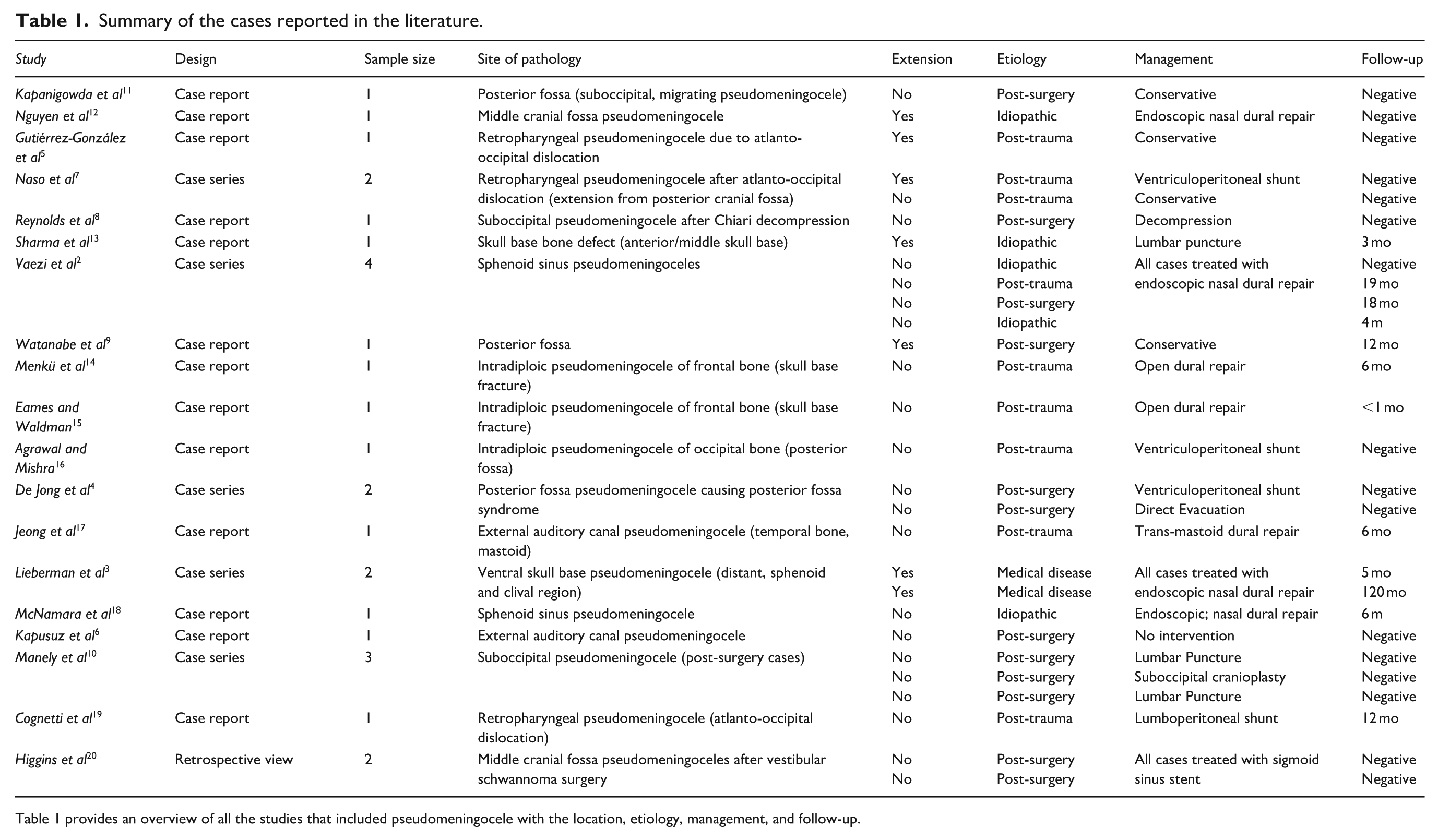
Table 1 provides an overview of all the studies that included pseudomeningocele with the location, etiology, management, and follow-up.
Etiology
Most of the reported etiologies of pseudomeningoceles found in the literature were classified as iatrogenic, congenital, or traumatic. 9 This is reflected in the result of our review, showing that the most reported etiology of pseudomeningocele formation is iatrogenic, accounting for 42.9% of total cases. Furthermore, the incidence of pseudomeningocele formation is reported to increase by up to 40% after posterior cranial fossa surgery and spinal surgery, accounting for 41.4% of all cases.2 -5,9,10,14,20 Iatrogenic, after posterior cranial fossa surgery and spinal surgery, is by far the most commonly reported cause, 9 (41.4%),2,5,7 -10,20 followed by post-trauma (34.5%),2,4,7,14 -16,21 idiopathic cases (5/29 or 17.2%), and medical disease-related cases (such as recurrent meningitis and CSF rhinorrhea; 2/29 or 6.8%). 9
Pathophysiology
In the literature, different theories are found that relate to the nature of the pathophysiology of pseudomeningocele formation. Several authors state that the reason is poor wound closure, while others suggest that it may be due to factors such as subarachnoid scarring and hydrocephalus. 22 Another theory is that dural tears can cause a persistent decrease in intracranial pressure, leading to symptoms of low cranial pressure, such as pseudomeningoceles. 23 Furthermore, numerous case reports correlated hydrocephalus and pseudomeningoceles. 3
Preventive Operative Techniques
Since postoperative complications are the most common cause of pseudomeningocele formation, the authors propose prevention measures that can help reduce postoperative complications of the postoperative CSF complications.22 -24 Insufficient bony reconstruction can lead to the formation of pseudomeningoceles or CSF fistulas. Therefore, the implementation of a bone flap prevents the formation of dead space and limits the collection of CSF in the space. 25 There was a study researching the effectiveness of arachnoid membrane suturing after posterior fossa surgery in preventing pseudomeningocele formation involving 2 groups. The first group consisted of 38 patients who had undergone suturing of the arachnoid membrane; the results showed that only 1/38 patients (2.6%) developed pseudomeningocele. In the second group, consisting of 32 patients without arachnoid membrane suturing, 11/32 patients (34.4%) developed pseudomeningocele. 24 This proves that suturing the arachnoid membrane creates an additional barrier and may reduce the risk of a postoperative pseudomeningocele and an incisional CSF leak. 4 There is also a study by Slot et al reported a decrease in the incidence of pseudomeningoceles with complete reconstruction of the suboccipital cranial defect. The method of dural reconstruction involves the use of a synthetic dural substitute or pericranium. 25 The watertight closure of the dura mater is indeed a crucial procedure to prevent pseudomeningocele formation; To ensure tightness, a direct closure of the dura mater is made using a fat or fascia lata graft. 14 There is also a paper reporting the repair of a pseudomeningocele with muscle graft placement and TISSEEL fibrin sealant. At 9 months of follow-up, the magnetic resonance findings showed total resolution of the meningocele. The results were reassuring, and the patient showed improved symptoms with satisfactory speech and swallowing functions. 6 Furthermore, 1 study discussed the replacement of the bone flap created after the detachment of muscles in the suboccipital region and supports their reattachment to the replaced bone flap. That would decrease the dead space so that CSF collection in this space is limited and pseudomeningocele is prevented. 19
Clinical Presentation and Symptom Initiation
Table 2 shows the signs and symptoms described in the literature, headache being the most common symptom, followed by neurological symptoms, including, but not limited to, cerebellar signs of severe disequilibrium, progressive headaches, gait disturbances, and dysarthria; the third common group of symptoms involves orbital complications, including a long history of progressive proptosis, irritation, pressure sensation behind the left eye, and vision loss. Other, less frequent signs and symptoms are listed in Table 2.
Summary of the reported symptoms.
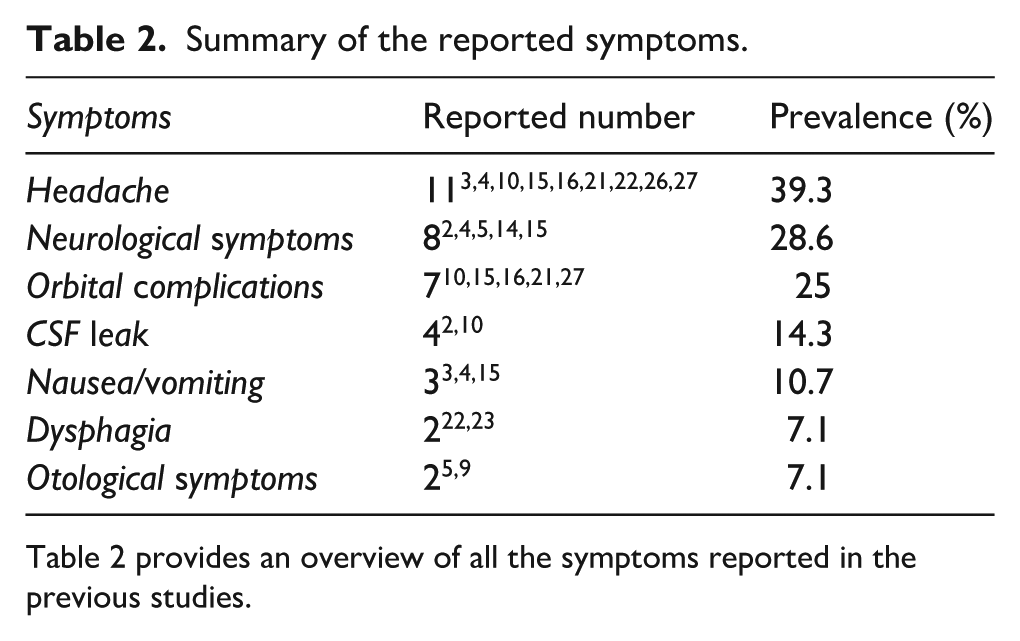
Table 2 provides an overview of all the symptoms reported in the previous studies.
The symptoms of pseudomeningocele appear for multiple reasons. There is a model that connects headaches and CSF leaks in a medical condition known as idiopathic intracranial hypertension. The main symptoms of this condition are headaches and visual disturbances. 16 In the event of visual disturbances, including diplopia, it has been established that trauma to the orbital walls can cause swelling of the soft tissues and retroocular edema, resulting in vascular congestion, which subsequently leads to increased intraorbital pressure propelling the eyeball forward. Stretching of the extra-ocular muscles and nerves and compressing of the draining veins result in proptosis. 28 At the same time, dysphagia is known to be directly related to the mass effect involving disruption of the airway and swallowing. 6 Finally, the formation of pseudomeningoceles causes tinnitus, which implies a defect in the dura that allows the CSF to escape into the middle ear or the subcutaneous tissue, causing the symptoms. 16
The onset of symptoms varied significantly amongst the patients—<1 month for 2/29 patients,3,28 between 1 and 3 months for 7/29 patients,2,5,8 -10,20 between 4 and 6 months for 3/29 patients,3,15,21 between 7 and 12 months for 1/29 patient, 26 and more than 12 months for 4/29 patients4,10,19,27; while 5 years (60 months), 9 10 years (120 months), 10 and 40 years (480 months) 2 were reported in 1 case each. This high variability might be attributed to the difference in the locations where the pseudomeningocele lesion develops.
Site and Extension
Pseudomeningoceles are present in various locations in the skull. For categorization reasons, we may combine similar divisions based on the anatomy of the cranial fossa. The most common site of pseudomeningoceles is reported to be the posterior cranial fossa (13/29 or 44.8%),2,5,12,14 -16,18,20,27 followed by the sphenoid bone (9/29 or 31%).7 -10,19
Regarding the extension of pseudomeningoceles to surrounding areas, three-quarters of the total cases reported no extension (22/29 or 75.9%), and only one-quarter of the cases (7/29 or 24.1%) reported extension to the nearby structures.3,7,9,14,19
In general, according to the analyzed literature and the results of our review, anterior pseudomeningoceles are less common than both middle and posterior cranial fossa pseudomeningoceles. First, gravitational forces affect pseudomeningocele formation: there is a patient whose pseudomeningocele was reported to be formed and growing progressively due to a lack of bone support exacerbated by gravity. 19 Therefore, gravity may be a significant factor in pseudomeningocele formation within the skull base.
Diagnostic Methods
In case pseudomeningoceles are formed and CSF accumulates in local soft tissue behind the paranasal sinus mucosa, some of these cases may be clinically associated with CSF rhinorrhea. However, in the absence of CSF rhinorrhea, a pseudomeningocele can be radiographically difficult to distinguish from a mucocele, resulting in an increased rate of misdiagnosis in the absence of clinical manifestations. 10
In terms of diagnostic modalities, CT and MRI techniques were used in almost every reported case; most patients underwent both modalities during their diagnosis process. MRI was used in 79.3% of the cases (23/29),2 -5,7,9,10,12,14,15,18,20,21,26,28 while CT was used in 62.1% of the cases (18/29).3 -5,7,8,10,14,15,18,26 -28 Other imaging technologies included audiology 4 and lateral skull X-ray. 19
It should be noted that a biopsy is not performed as a diagnostic method because it is performed only in the operating room following the removal of the lesion. In most cases (25/29 or 86.2%), a biopsy was not performed.
The diagnosis of pseudomeningocele depends primarily on imaging, as proposed by Steinbok et al in a published study involving 53 cases of pseudomeningocele, 13 of which (24.5%) reported no clinical symptoms and were only diagnosed by imaging. 28
The results showed that 100% of the patients underwent at least 1 diagnostic imaging modality. Radiographically, a pseudomeningocele is described as a localized collection of low-density fluid related to intracranial CSF. 29 On MRI, an extradural collection represents the radiological characteristics of CSF manifested as low signal intensity on T1 and high signal intensity on T2. 29 Although MRI can identify dural defects and the degree of communication, CT is used to visualize the exact location of the lesion. 29 The diagnostic tool of choice is currently MRI due to its increased sensitivity to soft tissue, in contrast to CT, which is used to locate the lesion more accurately, as it can produce an image of the bone in the case of erosion or calcification. Study findings conclude that MRI was used in 79.3% of the cases, while CT was used in 62.1%. Therefore, it is believed that both imaging modalities are supportive and complementary to each other.
Management and Follow-Up
Different management options exist in the literature. Most of the patients (23/29) underwent surgical treatment, which is considered the definitive treatment of pseudomeningoceles; a few patients (5/29) underwent multiple treatment options; 1 patient (1/29) refused surgery. 4
The postoperative follow-up period varied among the patients. No follow-up period was reported in 51.7% of cases (15/29); other than that, 3 to 6 months was the most reported period (6/29 or 20.7%).8 -10,19,21,28 The longest reported follow-up period was 120 months (1/29 or 3.4%). 9 A patient was still undergoing the follow-up (19), and 1 patient was reported lost during the follow-up. 10
No morbidity outcomes were documented in most patients (25/29 or 86.2%). However, the reports include 2/3 patients (6.9%) with disease recurrence,9,15 and 1/29 patients (3.4%) who had complications during the surgery. 26 A reported case (1/9 or 3.4%) was misdiagnosed as a calcified chronic subdural hematoma; A burrhole evacuation was performed, which led to a communicative type of hydrocephalus, which is associated with pseudomeningocele. 27 As with morbidity, no mortality is reported in most cases (27/29 or 93.1%), only 6.9% of cases (2/29) resulted in mortality related to a pseudomeningocele.3,5 A low percentage of reported morbidity and mortality could be attributed to a lack of follow-up data in the published literature.
The initial treatment of pseudomeningoceles is conservative, including several measures such as bed rest, elevation of the bed head, and administration of acetazolamide as the drug of choice in the absence of contraindication. 5 There is a study consisting of 17 patients with postoperative complications of a pseudomeningocele; 14 of them (82.4%) improved with conservative treatment involving pressure dressing and bed rest, and 3 of them (17.6%) required subsequent lumbar spinal drainage. 30 In addition to conservative management, there is an alternative CSF shunting method that resolves the lesion with a high success rate among the surviving patients.5,31 Ventriculoperitoneal shunts are indicated in the presence of hydrocephalus, 32 while lumbo-peritoneal shunts are the method of choice in the absence of hydrocephalus.
The reviewed literature reports cases of conservative management failure and consequential serious complications. Furthermore, surgical treatment is generally considered the definitive treatment of pseudomeningoceles. 29 The indications for surgical intervention include failure of conservative management or the presence of progressive signs and symptoms of neurological injury. 33
Surgical intervention can vary from a simple incision and drainage to more complicated operations. The main objective of the surgery is to maintain watertight dural closure to prevent CSF re-accumulation. 24 Although surgical removal of the pseudomeningocele and direct dural defect repair is suggested in the literature, more exploration of surgical techniques is still needed. 6 Surgical repair of pseudomeningocele can be challenging for the following reasons: first, it can be difficult to approach the defect site; second, there is an increased risk of developing meningitis; finally, there is a likelihood of severe morbidities, such as poor neurological function. Another study reported 2 cases of iatrogenic postoperative cranial pseudomeningocele that failed conservative management. Subgaleal shunt placement was used with successful resolution in both cases. 34
Recommendations include a set of steps that must be followed to ensure the best possible outcome: first, it is necessary to accurately establish the diagnosis, etiology, and mechanism of the leak before surgery; second, the graft material should be discussed and chosen before surgery; third, a short-term lumbar drainage might be considered in case of a small high-pressure leak; finally, it is believed that engaging a multidisciplinary team including a neurosurgeon guarantees the best outcome.
We suggest exploring the definitive surgical techniques more deeply and continuing observation of patients during the follow-up period to analyze morbidity and mortality.
Conclusion
The objective of this study was to provide a comprehensive overview of the skull base pseudomeningocele published in the literature. Research shows that pseudomeningoceles at the skull base pseudomeningoceles are considered rare; however, as the most common etiology behind their formation is postsurgical, it is believed that early diagnosis through imaging modalities is essential to prevent complications. Pseudomeningoceles can be initially treated with conservative measures, while surgery is considered the definitive treatment. This scoping review about pseudomeningoceles provides an additional level of evidence, as most of the published articles were case reports and case series. Hence, the authors of this study conducted this comprehensive review of the literature to gather and report all the existing findings and evidence on the presentation, diagnosis, and treatment of pseudomeningocele.
Limitations and Recommendations
Due to the rarity of the condition, this comprehensive review is limited by the predominance of case reports and small case series, which undermines the strength of the evidence and hinders generalizability. Furthermore, several studies lacked thorough demographic data, precise anatomical localization, and prolonged follow-up, leading to variability that obstructs meaningful comparisons. The inconsistent reporting of outcomes and the exclusion of papers in languages other than English, French, and Spanish may exacerbate bias.
Future research should focus on multicenter prospective studies with standardized reporting to clarify diagnostic criteria, treatment approaches, and long-term outcomes. Clinicians should maintain an elevated level of suspicion, particularly in post-surgical and post-traumatic patients, and utilize MRI and CT for accurate diagnosis. Initially, conservative approaches are advised; nevertheless, surgical intervention should be contemplated if symptoms persist or complications arise.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data supporting the findings of this study are included within the article and its supplementary files.