
Abstract
Background
Schneiderian papillomas (SP) are aggressive sinonasal tumors that occasionally extend into areas that are surgically unresectable.
Objective
evaluate the signifcance of cyclo-oxygenase-2 (COX-2) expression in SP.
Methods
Immunohistochemistry for COX-2 was performed on SP samples and middle turbinates from chronic rhinosinusitis without nasal polyps controls obtained during surgical resection between 2009–2017. A positive stain was defined as having 10% or more cells exhibiting diffuse immunoreactivity. Comparisons were performed using Fisher Exact tests, t-tests, and ANOVA.
Results
The study included 67 tumor samples and 9 controls from two academic institutions. The mean age of the SP group was 55.4 years and 53.2 years in the control group (p = 0.71). Thirty-nine (58.2%) SP patients had previous surgery compared to 1 (11.1%) in the control group (p = 0.01). The most common tumor attachment sites were the maxillary (47.8%) and ethmoid (25.4%) sinuses. Fifteen (22.4%) SP samples stained strongly positive for COX-2 and 24 (35.8%) stained weakly positive compared to no positive stains in the control group (p < 0.01). When stratified by COX-2 intensity, there were no statistically significant differences in gender, smoking history, history of previous sinus surgery, site of attachment, papilloma subtype, or future recurrence between SP samples.
Conclusion
COX-2 was overexpressed in 58.2% of SP cases, and strongly positive in 22.4% of cases, compared to no positive staining among controls. No significant differences in COX-2 expression were observed between SP subtypes or recurrent tumors. Further studies are warranted to evaluate COX-2 as a possible therapeutic target in tumors that overexpress the enzyme.
Keywords
Introduction
Schneiderian papillomas (SPs) are aggressive benign sinonasal tumors. The standard treatment is primarily complete surgical resection due to the tumor’s predilection for recurrence and a well documented potential for some subtypes to undergo neoplastic progression to squamous cell carcinoma.1–4 There are 3 subtypes of SP defined by their papilloma morphologies: inverted, exophytic, and oncocytic. 5 , 6 On average, there is a 4-17% overall rate of malignant transformation for inverted and oncocytic papillomas, while the exophytic subtype is not associated with dysplasia or malignancy. 1 , 6 However, at times the tumor can extend into areas that are surgically unresectable, such as the orbit or skull base. Radiotherapy is an option for the small subset of patients with residual unresectable Schneiderian papilloma, but there is limited data on its efficacy and side effects. 7
There currently is no effective medical therapy for SPs that are unresectable or exhibit aggressive behavior such as repeated recurrences despite extensive surgical resection. Therefore, the investigation of a viable therapeutic target for medical intervention is warranted. Possible adjuvant medical therapies for the inverted papilloma (IP) subtype proposed in the literature include 5-fluorouracil, a thymidine analogue that interferes with DNA synthesis and was demonstrated in a small case series to be associated with a decreased rate of recurrence in patients who required multiple revision surgeries. 8 Cyclo-oxygenase-2 (COX-2) has also been proposed as a possible target due its overexpression in 62% of inverted papilloma specimens. 9
Cyclo-oxygenase enzymes catalyze the rate-limiting step of prostaglandin biosynthesis. The COX-2 isoform has been shown to modulate cell proliferation and apoptosis in both malignant and benign tumors, such as laryngeal papilloma. 10 , 11 Furthermore, COX-2 inhibitors are being studied as a possible adjunct treatment option for colorectal and non-small cell lung cancer. 12 , 13
The objective of this study was to compare COX-2 expression in Schneiderian papillomas to chronic rhinosinusitis controls and identify risk factors associated with COX-2 overexpression.
Methods
The study was approved by the institutional review board at the University of Southern California and the University of California at Los Angeles (UCLA). Tumor and control samples were obtained from patients who underwent endoscopic sinus surgery at UCLA and Keck Medical Center from 2009–2017. Control samples were sinonasal mucosa from chronic sinusitis patients undergoing endoscopic sinus surgery with no evidence of SP on the final pathology report.
Immunohistochemistry for COX-2 was performed on tumor and control samples using the same protocol. Samples were fixed in 10% buffered formalin, paraffin-embedded and processed by conventional methods. Slides of the samples were incubated with the COX229 monoclonal anti-Cox-2 antibody from Zymed (Grand Island, New York, USA) at an optimized concentration following epitope retrieval in citrate buffer. Visualization was achieved with the Bond Polymer Refine Detection Kit (Leica Biosystems, Buffalo Grove, Illinois, USA) and the slides were counterstained with hematoxylin. The intensity of staining was evaluated by 2 head and neck pathologists blinded to the clinical history. A positive stain was defined as having 10% or more of tumor cells exhibiting diffuse immunoreactivity. If positive, the intensity was then categorized as weak (+) or strong (++). A negative stain was defined as having less than 10% of cells exhibiting diffuse immunoreactivity. Discordance between the scores of 2 pathologists was mediated by a 3rd pathologist who classified the slide as negative, +, or ++ for COX-2 expression.
Sociodemographic information (age and gender) as well as medical history for each specimen was obtained from health records. Statistical significance of each difference between groups was determined using Chi-square or Fisher Exact test for categorical variables, and ANOVA or t-test for continuous variables. A test statistic with a p-value <0.05 was considered significant.
Results
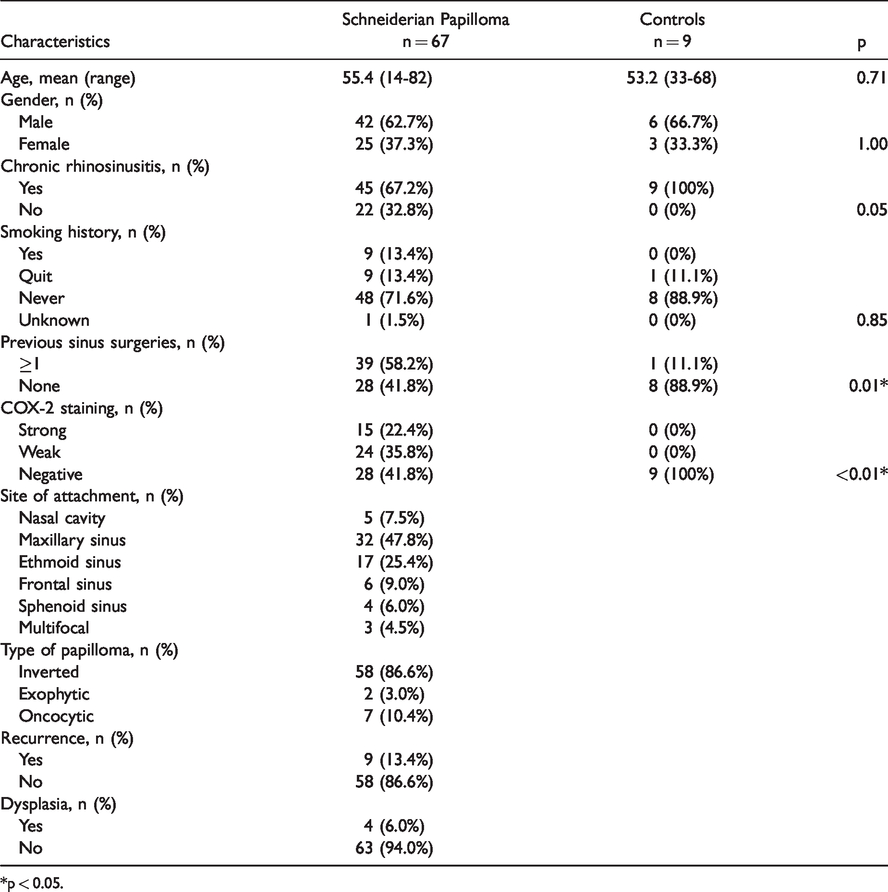
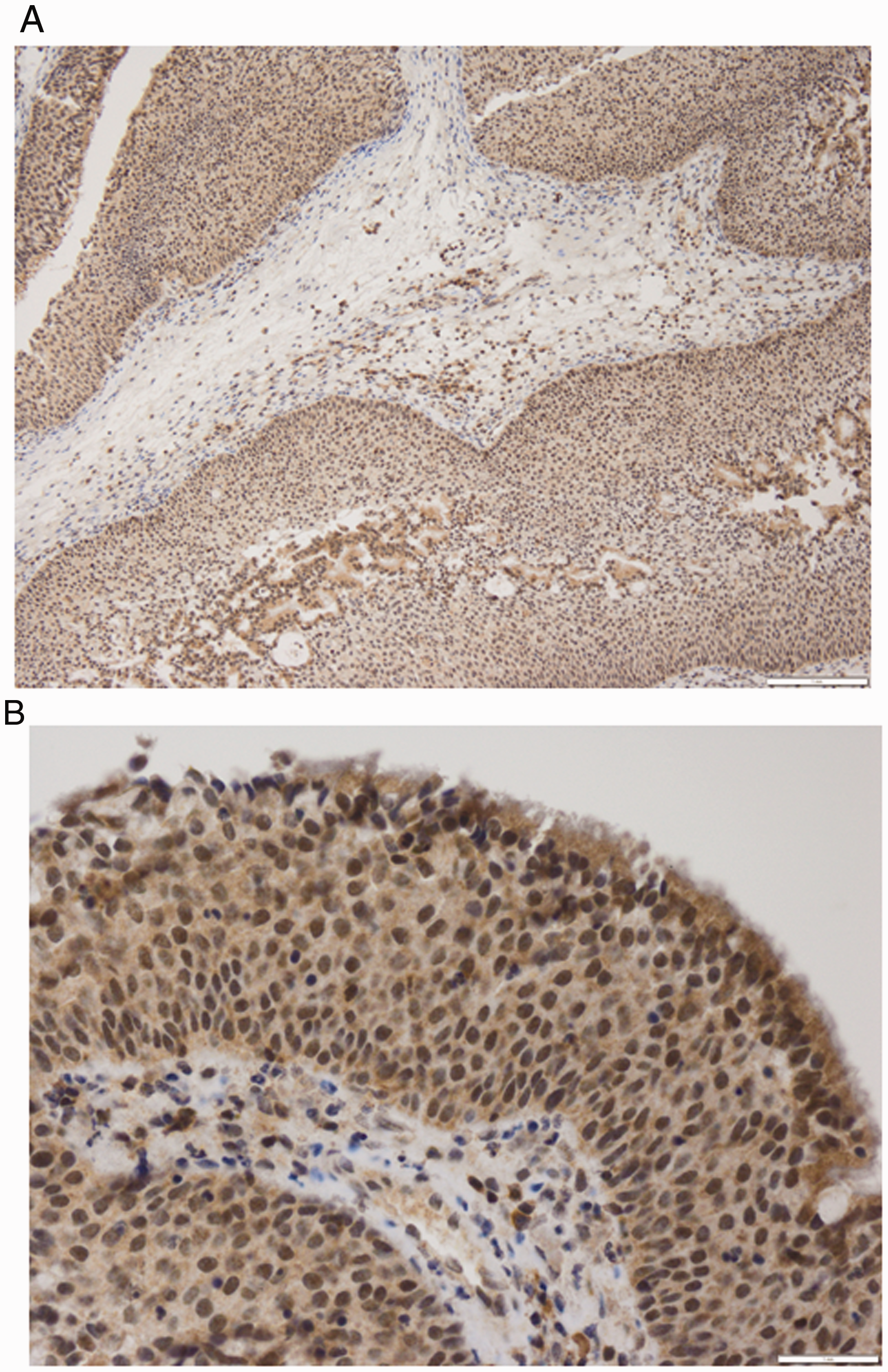
The study included 67 tumor samples and 9 controls from two academic institutions. Characteristics of the two groups are listed in Table 1. The mean age of the SP group was 55.4 years, 62.7% were male, and 13.4% had a history of smoking. In the control group, the mean age was 53.2 years, 66.7% were male, and none were current smokers. Forty-five (67.2%) patients had a history of chronic rhinosinusitis compared to 9 (100%) in the control group (p = 0.05). None of the patients in the control group had nasal polyps. Thirty-nine (58.2%) SP patients had previous sinus surgeries compared to 1 (11.1%) in the control group (p = 0.01). The most common tumor attachment sites were the maxillary (47.8%) and ethmoid (25.4%) sinuses. The majority of SPs were inverted papillomas (86.6%) followed by oncocytic (10.4%) and exophytic (3.0%) subtypes. Future recurrence occurred in 13.4% of patients and dysplasia was noted in 6.0% of samples, but there was no transformation to carcinoma or carcinoma in situ identified in any of the samples. Fifteen (22.4%) SP samples stained strongly positive (Figure 1) for COX-2 and 24 (35.8%) stained weakly positive compared to no positive stains in the control group (Figure 2) (p < 0.01).
Schneiderian Papilloma and Control Group Characteristics.
*p < 0.05.
(A) 10X and (B) 40X. Schneiderian papilloma, inverted type, exhibiting strong COX-2 staining of the epithelium.

(A) 10X and (B) 40X. Ciliated sinonasal mucosa and glands with negative COX-2 staining.
When stratified by COX-2 intensity (Table 2), there were no statistically significant differences in gender, smoking history, history of previous sinus surgery, site of attachment, papilloma subtype, or future recurrence between SP samples.
Characteristics of Schneiderian Papilloma Stratified by COX-2 Intensity.

Discussion
This is the first study in the literature to evaluate the immunohistochemical expression of COX-2 in Schneiderian papillomas versus control samples of sinonasal mucosa. We also evaluated for possible risk factors for overexpression of COX-2 in SPs.
Only a few case series have investigated COX-2 expression in the IP subtype with the rate of COX-2 expression ranging from 5.4% to 61% in the limited literature. 9 , 14 , 15 Despite similar protocols in immunohistochemical staining, the lack of a control group and small sample sizes in all previous studies likely contributed to the wide variability in reported rates of COX-2 overexpression. We did not identify any studies investigating COX-2 expression in the exophytic or oncocytic subtypes of SP.
The role COX-2 plays in the pathophysiology of Schneiderian papilloma is unclear with limited research on the topic. However, COX-2 expression has been well established to be involved in the development of head and neck cancer through its role in cell proliferation, angiogenesis, and antiapoptosis. 10 , 16 , 17 Moreover, COX-2 overexpression has been described as well in recurrent respiratory papilloma, a benign upper airway disease that has a similar predilection for recurrence. Recurrent respiratory papilloma (RRP) is characterized by multiple recurrences of airway papillomas and is strongly associated with human papillomavirus (HPV) 6 and 11 infection. Robinson et al. reported that COX-2 mRNA levels quantified with in-situ hybridization and reverse transcription polymerase chain reaction were found to be 13-fold greater than those measured in normal respiratory mucosa. 11 Molecular studies have shown that the overexpression of COX-2 is a consequence of EGFR signaling leading to Rac1 upregulation, which is a member of the Rho family of GTPases. 18 Also, the use of a selective COX-2 inhibitor in RRP to maintain or extend remission time after surgical debridement has been described in 2 case reports with remarkable clinical reponse in achieving extended remissions. 19 , 20 The growing research on a likely therapeutic pathway through COX-2 inhibition in RRP suggests a possible similar pathophysiologic mechanism in Schneiderian papillomas, which is being explored. For example, positive immunostaining of the EGFR protein and upregulation of EGFR mRNA has been described in the sinonasal inverted papilloma subtype, consistent with results for RRP. 21
While RRP is widely accepted to be caused by HPV infection in respiratory tissue, there is still debate regarding the association between HPV and Schneiderian papillomas. Detection rates of HPV in the IP subtype, which has been the most studied, have varied widely in the literature from 0 to 72%.22–24 Why there is such considerable variation is unclear, though it has been hypothesized that the histologic composition of the cohorts in each study may vary significantly which leads to different detection rates. 24 Since dysplastic and malignant inverted papillomas have been reported to have increasing rates of HPV detection respectively, cohorts with a higher percentage of dysplastic or malignant IP will have higher rates of HPV detection. 25 HPV infection in other SP subtypes has been considerably less studied, but HPV appears to be associated with the formation of exophytic SP and not oncocytic SP. 6 In our study, HPV infection was not tested for, which may be a factor in why only 22.4% of SP samples stained strongly positive for COX-2.
Similarly, there appears to be an upregulation of COX-2 expression correlated with histologic grade and stage of transformation from a benign inverted subtype to squamous cell carcinoma. One study reported that the rate of COX-2 expression in IP samples increased from 9.4% to 38.9% in IPs with squamous cell carcinoma and 41.2% in 17 primary sinonasal squamous cell cancer samples. 15 Lee et al. also reported a stepwise increase in COX-2 expression depending on the histologic grade of IP with 9.4% of grade 1 IP samples expressing COX-2 compared to 80% of grade 4 IP samples. 14 The association of increased expression of COX-2 in IPs that undergo malignant transformation is consistent with the established role of COX-2 in the pathogenesis of head and neck cancer. In our study cohort, only 4 samples had dysplastic findings and none had malignant features. Therefore, we were unable to evaluate the association beetween COX-2 expression and malignant transformation.
The only adjunctive medical treatment for SP reported in the literature is a case series of 18 patients (5 primary and 13 revision) where 5-fluorouracil (5-FU) was applied following endoscopic resection of the inverted papilloma subtype. 5-FU was applied where it was difficult to ascertain whether mucoperichondrium or mucoperiostium was completely removed during the operation, which was usually in anatomical locations where further debridment would lead to significant morbidity. Only 1 patient (5.6%) had a recurrence and one patient had transient periorbital swelling. There were no major complications. 8 It is important to note that the study was a retrospective case series with no control group and evaluated only the IP subtype. Based on our study’s results, COX-2 may be another promising therapeutic target for adjunctive medical therapy.
In this study, we also found no correlation between the expression of COX-2 and risk factors such as age, smoking history, site of attachment, previous sinus surgeries, papilloma subtype, and history of recurrence. The major limitation of our analysis was the limited number of SP samples with dysplasia or SP subtypes other than IP which raises the risk of being underpowered to detect a significant difference between those groups. Also, there may be other risk factors associated with COX-2 expression that were not measured in this study such as HPV infection.
Conclusion
COX-2 was overexpressed in 58.2% of Schneiderian papilloma cases, and strongly positive in 22.4% of cases, compared to controls. No significant differences in COX-2 expression were observed between Schneideiran papilloma subtypes or recurrent tumors. Further studies are warranted to evaluate COX-2 as a possible therapeutic target in tumors that overexpress the enzyme.
Footnotes
Authors’ Note
Presented as an oral presentation at the ARS spring meeting in National Harbor, MD on April 20, 2018.
Ethical Approval
This study was approved by our institutional review board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a Southern California Clinical & Translational Science Institute (SC-CTSI) grant.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.