
Abstract
Background
Endoscopic sinus surgery is a common surgery, in which the uncinate process of the ethmoid is removed as the first surgical step. There are multiple techniques for uncinectomy. Herein we describe a new and simple uncinectomy technique.
Methods
We performed a randomised controlled trial with blinded assessors. Eight cadaveric heads were used to compare the new technique to the commonly used technique; retrograde uncinectomy. The procedures were performed by 2 rhinologists, and the findings were evaluated by 2 senior rhinologists blinded to the technique and the surgeon who did. They assessed the final view of the procedure and the complications. Thereafter, they assessed the procedure for the duration and ease of each technique for teaching purposes.
Results
Fifteen uncinectomies were performed, 7 using the retrograde technique, and 8 using the new technique. The mean durations were 5.64 min using the seeker uncinectomy and 7.57 min using the retrograde uncinectomy, p-value = 0.017. The completion was better in seeker uncinectomy; however, not significant statistically, p > 0.05. The complications with the new technique were inferior turbinate injury in 12.5% and natural ostium non-identification in 12.5%, p > 0.05. With retrograde uncinectomy, lacrimal injury occurred in 14.3%, p > 0.05. The ease of teaching scores was higher for the seeker uncinectomy.
Conclusion
Based on this cadaveric trial, seeker uncinectomy seems to be a safe and easy to perform technique. However, injury to the inferior turbinate and missing the natural ostium must be taken into consideration. These warrant further studies on the clinical application of this procedure.
Keywords
Introduction
Uncinectomy is the first step performed in most endoscopic sinus surgeries. 1 There are two commonly described techniques of uncinectomy, antegrade and the retrograde technique.1–3 The key surgical principles of both techniques are to remove the uncinate process, identify the natural ostium of the maxillary sinus, and to avoid going blindly to the ostium itself. Herein we describe a new technique aimed at directly going to the maxillary ostium using a maxillary sinus seeker. The goals of this new technique are to ease uncinectomy teaching for physicians in training, shorten the time of this step, and minimise the risk of lacrimal system injury. In this trial we aimed to comparatively assess the differences in safety and duration between the new technique, seeker uncinectomy, and retrograde uncinectomy using a back-biter on cadaveric heads.
Materials and Methods
Eight fresh frozen cadaveric heads were simply randomised between 2 rhinologists. They performed seeker uncinectomy in 2 heads and retrograde uncinectomy in 2 heads each and each technique was performed in both sides. The procedure of seeker uncinectomy consists of palpating the inferior turbinate (IT) in an upward manner and the frontal process of the maxilla in a retrograde manner to identify the infero-anterior part of the philtrum between these structures and the uncinate. The uncinate is then punctured in the infero-lateral direction and extended posteriorly. The horizontal uncinate is then cut from the IT with a scissor, removing it with the 4 mm 0° degree powered shaver, and finally, the upper uncinate is removed with angled forceps at 90° (see Figure 1). On the other hand, retrograde uncinectomy is performed by back-biting the uncinate process at the junction between its vertical and horizontal portions using 0° degree endoscope. The upper part is then removed with angled forceps. With a 30° degree endoscope, the natural ostium is identified and removal of the horizontal portion is done with a side biting instrument widening the ostium posteroinferiorly (see Figure 2). 3 , 4 The outcome measures included the duration of each technique, the completion of the uncinectomy, and complications such as lacrimal injury, orbital injury, IT injury, and missed natural ostium. In addition, those who rated these outcome measures were asked to give a score on the ease of teaching for both techniques from 1 to 5, where 1 represents impossible to teach and 5 represents very easy to teach. The final view of the uncinectomy was assessed by 2 blinded senior rhinologists. They were blinded to the technique used and to the surgeons who performed them. The first author, a senior rhinologists, has described this new technique and demonstrated it on a separate cadaveric head that was not included in the study. He was not involved neither in the execution of the study procedure or the assessment of the study variables. Data were analysed using the Statistical Package for the Social Sciences (SPSS v 22; IBM Corp., New York, USA), chi-squared test for categorical variables, and one-way analysis of variance for continuous variables. We considered P-value < 0.05 a statistically significant difference.

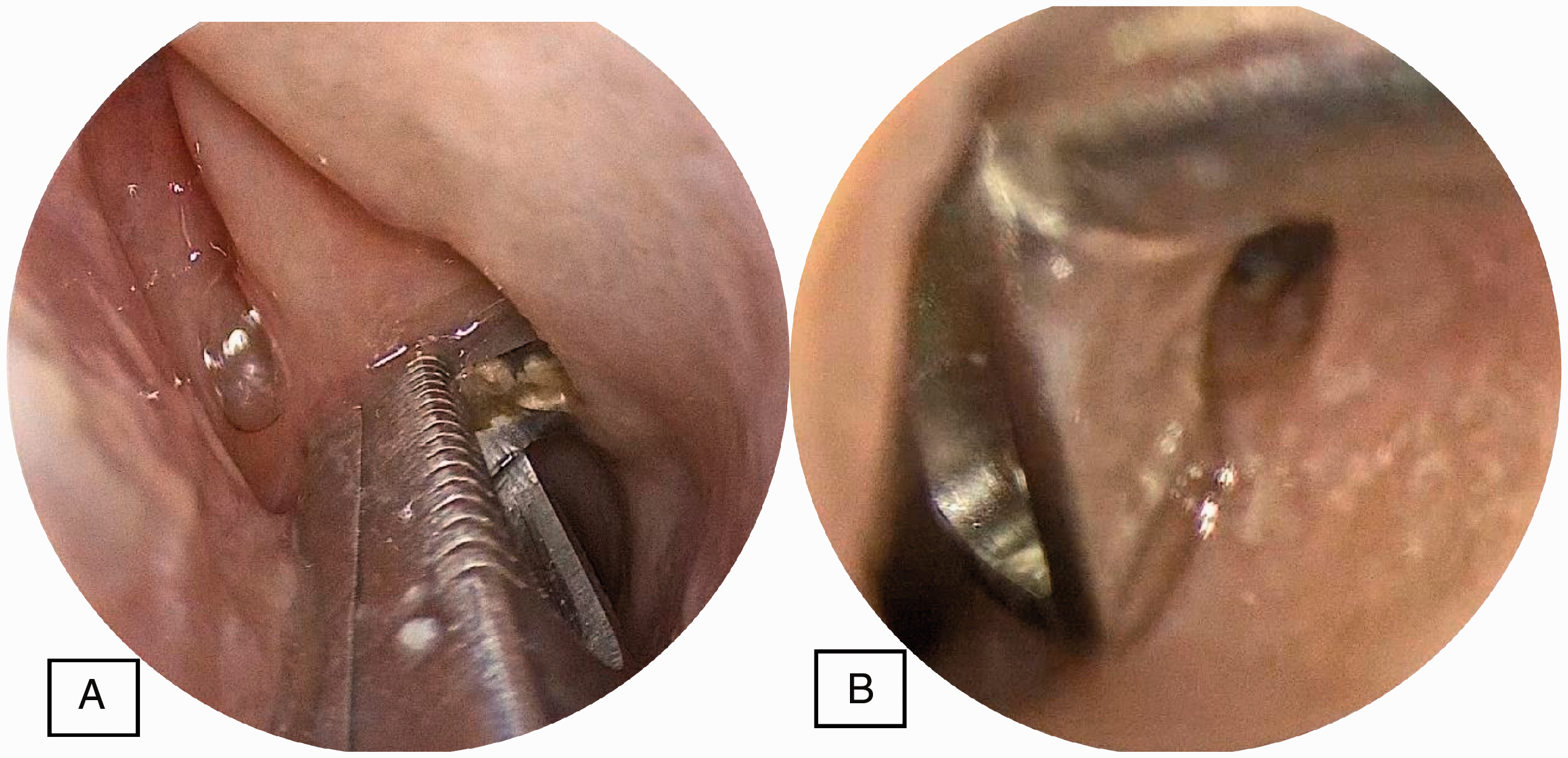
Seeker uncinectomy on the left side. A, Puncturing the anteroinferior part of the philtrum with the seeker probe in an inferolateral direction. B, Widening the opening. C, Cutting inferior attachment of the uncinate process with scissors. D and E, Removing the horizontal part of the uncinate process with the straight powered shaver. F and G, Removing the upper part of the uncinate process with 90° degree up-biting forceps. H, final view with 0° degree endoscope. I, Final view with a 90° endoscope.
Results
Eight cadaveric heads and 15 sides were included in the study. One side was excluded as there was previous facial trauma involving the orbit and sinuses. The mean time for seeker uncinectomy was 6.22 min for surgeon 1 and 5.06 min for surgeon 2. The mean time for retrograde uncinectomy was 7.55 min for surgeon 1 and 7.56 min for surgeon 2. The overall mean durations of the two techniques were 5.64 min using the seeker uncinectomy technique and 7.57 min using the retrograde uncinectomy technique, p-value = 0.017. Complete uncinectomy was successfully achieved in 14 out of 15 sides. In one out of the 15 sides, using the seeker uncinectomy technique, the natural ostium was missed. The complications were as follows: lacrimal injury with the retrograde technique in one out of the 15 sides, IT injury, and wrongful opening of the inferior meatus instead of the natural ostium with the seeker technique in one out of the 15 sides. These complications were not in the hand of the same surgeon. No orbital injury or other complications were encountered. The average ease to teach score 3.93/5 for the seeker uncinectomy and 3.28/5 for backbiter uncinectomy, p-value = 0.133 (see Table 1).
The Study Findings Comparing Retrograde Uncinectomy and the New Seeker Uncinectomy.

Note. Boldface indicates significant difference.
Discussion
Our trial demonstrates a novel technique for uncinectomy and shows that it is as safe as the known techniques, with a significantly lesser duration, and is apparently easier to learn. However, a learning curve study needs to be done for junior residents.
Uncinectomy is usually the first surgical step in sinus surgery. 1 There are two famous techniques described to conduct a safe and successful uncinectomy: the Stammberger’s antegrade technique and the retrograde swing-door technique.1–3 The learning curve for the ability to perform these procedures independently is relatively slow. 5 , 6
Few studies have compared these two techniques in subjective and objective approaches. Puranik et al. conducted a survey of 585 practising British otorhinolaryngologists to assess the surgeons’ preferences, knowledge about the incidence of complications, and ease of the procedure. They found comparable results in both techniques. However, this was a very subjective study. 7 In another study, Singhania et al. evaluated the complications of classical antegrade uncinectomy versus the retrograde swing door technique on 480 uncinectomies and found that the incidence of orbital penetration, incomplete removal, ethmoid complex injury, and natural ostium non-identification were significantly lesser in the back-biter swing door technique, but it was associated with a higher incidence of lacrimal injuries. 8
Our novel technique, seeker uncinectomy, is expected to combine the advantages of both techniques, being easier to teach, having a lesser risk of injury to the orbit, lacrimal system, and ethmoid complex. However, non-identification of the natural ostium and penetration into the inferior meatus are expected, and have to be taken into consideration.
This trial mainly aimed to assess the safety of the new technique. However, this trial is limited by the fact that it was a cadaveric study, had a small sample size, and was performed by rhinologists. These warrant further studies to assess the learning curve using this novel technique, and evaluate its pros and cons in a prospective trial of sinusitis patients.
Conclusion
This cadaveric evaluation of the new uncinectomy technique, the seeker uncinectomy, showed that it is as effective as the retrograde technique. However, it is a new technique and the trial was performed by rhinology fellows, the duration was a significantly less than the retrograde technique. This technique seems to be safe and much easier to teach. The associated complications were relatively minor, but should not be neglected. Further clinical studies are to be done to assess the learning curve and the safety.
Footnotes
Acknowledgments
The authors extend their thanks and gratitude to the Saudi Association of Neurological Surgery (SANS) for offering the cadaveric heads to conduct the study as part of the skull base surgeries course.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by our institutional review board. This study was conducted in part of the annual endoscopic skull base surgery course in King Saud University.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.