
Abstract
Background
Cryoablation of the posterior nasal nerve at the middle meatus has been shown to successfully treat nasal obstruction and symptoms of chronic rhinitis. Cryoablation of both the middle and inferior meatus has not yet been studied.
Objectives
To evaluate the safety and feasibility of cryoablation of the posterior nasal nerve at both the middle and inferior meatus locations to treat chronic rhinitis.
Methods
Participants underwent bilateral cryoablation of the posterior nasal nerve at both the middle meatus and inferior meatus and were assessed through 3 months post treatment. The primary endpoint is the change from baseline to 3-month follow-up in the reflective Total Nasal Symptom Score (rTNSS). Other assessments include additional patient-reported outcomes, physician assessment, and independent review and scoring of imaging.
Results
Thirty participants were enrolled at 3 US centers. There was a significant improvement from baseline in the median rTNSS (–4.0, P < .001) at 3 months. Statistically significant improvements from baseline (P < .001) were also observed with the Nasal Obstruction Symptom Score (NOSE), nasal symptom visual analog scale (VAS), Sino-Nasal Outcomes Score (SNOT-22), and mini Rhinoconjunctivitis Quality of Life Questionnaire (mini RQLQ). Clinical Global Impression – Improvement (CGI-I) indicated that 89.7% (26/29) of participants experienced improvement at 3 months. No serious adverse events were reported.
Conclusion
Cryoablation at both the middle meatus and inferior meatus appears to be a safe and feasible option for treatment of chronic rhinitis. In this feasibility study, there is significant improvement in symptoms post treatment. Adverse events are minor and transient.
Introduction
Approximately 60 million people in the United States are affected by chronic rhinitis. 1 Rhinitis symptoms – rhinorrhea, congestion, itching, sneezing – significantly impact the quality of life and productivity. 2
Although pharmacological treatments are the first line of treatment, they do not always provide an adequate response or are not tolerated by all patients. In such cases, surgical techniques can be used to treat rhinitis. Interruption of the posterior nasal nerve at the middle meatus using cryoablation has demonstrated a response rate of ∼80% with reductions in rhinorrhea and congestion symptoms by approximately 50%. 1 , 3 , 4 Since parasympathetic nerve fibers innervate the nasal cavity within the inferior meatus as well as the middle meatus, 5 , 6 adding cryotherapy treatment at the inferior meatus may improve the symptom reduction and/or response rate in patients with chronic rhinitis. The purpose of this study was to evaluate the safety and feasibility of cryoablation of the posterior nasal nerve at both the middle and inferior meatus locations to treat chronic rhinitis.
Materials and Methods
Study Design and Population
This is a prospective, nonrandomized, interventional, postmarket feasibility study conducted at 3 centers in the US. Advarra IRB (Columbia, MD) approved the study for all 3 centers and written informed consent was obtained from all participants. The study is registered on www.clinicaltrials.gov (NCT03791489). The STROBE guidelines were applied to the study reporting. 7
Participants were adults (≥18 years) with moderate to severe rhinorrhea and mild to severe nasal congestion lasting at least 3 months. All participants were required to have had an allergy test within the past 10 years or undergo one during the study period.
Participants were excluded from the study if they had significant anatomic obstructions limiting access to the posterior nose (eg, severe septal deviation, nasal polyps, sinonasal tumor); previous sinonasal surgery significantly altering the posterior nose anatomy (previous cryoablation was allowed); moderate to severe ocular symptoms; a history of epistaxis in the past 3 months; a history of rhinitis medicamentosa; previous head or neck irradiation; active or chronic nasal or sinus infection; an allergy or intolerance to anesthetic agents; cryoglobulinemia, paroxysmal cold hemoglobinuria, cold urticaria, Raynaud’s disease, and/or, open or infected wounds at or near the target tissue; were pregnant; or were participating in another clinical research study.
All participants underwent in-office bilateral cryoablation of the posterior nasal nerve with the ClariFix device (Arrinex, now part of Stryker ENT, Plymouth, Minnesota 55447) at both the middle meatus and inferior meatus. The FDA-cleared cryosurgical device is indicated for the destruction of unwanted tissue during surgical procedures, including in adults with chronic rhinitis. Details of the cryotherapy procedure have been described previously. 3 , 4 Figure 1 depicts the treatment sites used in this study. Each cryoablation treatment was approximately 30 seconds in duration; an additional 30-second treatment was permitted at each location, at the investigator’s discretion, if necessary.

ClariFix treatment sites. Cryotherapy treatment sites included the posterior nasal nerve branches at the middle meatus (A) and the inferior meatus (B).
Participants were required to discontinue use of ipratropium bromide (ie, Atrovent) at least 3 days before treatment and for the duration of the study.
Assessments
Data were collected at baseline and at the 1- and 3-month follow-up visits. Assessments included a series of patient-reported outcome (PRO) assessments, a physician assessment, and independent review and scoring of imaging. Procedure characteristics and adverse events are also reported.
The primary endpoint is the change from baseline to 3-month follow-up in the reflective Total Nasal Symptom Score (rTNSS), which is a validated PRO that rates 4 nasal symptoms on a scale of 0 (no symptoms) to 3 (severe symptoms). The scores are summed to provide a total rTNSS with a possible range of 0 to 12. 8 The minimal clinically important difference (MCID) for the rTNSS is –1.0 points. 8
Other PRO efficacy outcomes include the changes from baseline in the Nasal Obstruction Symptom Evaluation (NOSE) score, Sino-Nasal Outcome Test (SNOT-22), nasal symptoms visual analog scale (VAS), and mini Rhinoconjunctivitis Quality of Life Questionnaire (mini RQLQ).
The NOSE is a validated PRO questionnaire of 5 nasal symptoms that are rated on a scale of 0 (no problem) to 4 (severe problem) and the sum of the symptom scores is multiplied by 5 to provide a total score that can range from 0 to 100. 9 The following classification scheme for total NOSE scores has been developed: mild 5–25, moderate 30–50, severe 55–75, and extreme 80–100. 10 A NOSE responder is defined as a participant who had at least 1 NOSE class improvement or at least 20% NOSE score reduction from baseline.
The SNOT-22 is a validated PRO questionnaire consisting of 22 items scored using a 5-point Likert scale from 0 (no problem) to 5 (problem as bad as it can be). 11 The total SNOT-22 score is the sum of the responses, producing a total possible score of 0 to 110, with higher scores indicating worse symptoms. The MCID for the total SNOT-22 is –8.9 points. 11
A 100-mm visual analog scale (VAS) is used to evaluate nasal symptoms of rhinorrhea and congestion on a continuum over the previous week, with 0-mm representing no symptoms and 100-mm marking representing severe symptoms.
The mini RQLQ is a validated 14-item PRO measuring impairments in 5 domains (activities, practical problems, nose symptoms, eye symptoms, and other symptoms). 12 Each item is rated on a 7-point scale from 0 (no impairment) to 6 (maximum impairment) and the overall mini RQLQ score is the mean of the 14 items. The MCID for the mini RQLQ is 0.4 points. 13
The Clinical Global Impression-Improvement (CGI-I) is a clinician-completed assessment evaluating the clinician’s impression of a patient’s response to treatment based on their clinical observations. The CGI-I is a 7-point Likert scale that ranges from 1 (very much improved) to 7 (very much worse). The CGI-I was completed by the physicians at follow-up visits to evaluate the physicians’ impression of participant improvement over baseline.
Bilateral endoscopic images were taken from videos of the head of the inferior turbinates at baseline and follow-up visits. The images were deidentified and put in randomized order by the study sponsor for evaluation by an independent, blinded physician reviewer (DC). Each location was evaluated for inferior turbinate sizing using a validated 4-level scale with intervals of 25% (1 = 0–25%; 2 = 26–50%; 3 = 51 = 75%; 4 = 76–100%). 14
Procedure pain scores for each location were collected by verbal response of the participant immediately after treatment. Additionally, an overall posttreatment pain score was collected before the participant left the clinic. Both procedure and posttreatment pain scores were rated on a scale of 0 (no pain) to 10 (severe pain).
All serious adverse events, device- and/or procedure-related adverse events, and adverse events associated with the head, ears, nose, throat, or lungs were reported from treatment through the 3-month follow-up. All adverse events were adjudicated for relationship to the device and/or procedure by an independent physician.
Statistical Analysis
Since this was a feasibility study, no formal power or sample size calculations were performed. The sample size was selected to be comparable to those in other trials of this nature in this field. All statistical analyses were performed using 2-sided hypothesis tests and P < .05 was considered statistically significant. No adjustments for multiplicity were performed, so inference is valid for the primary endpoint of 3-month change in rTNSS only.
Continuous data are summarized using descriptive statistics: n, mean ± standard deviation (SD) or median [interquartile range (IQR)]. Categorical variables are summarized using frequency counts and percentages. Ordinal-scaled variables are summarized using the frequency and percentage of observations within a category.
Change from baseline for participant-reported assessments are evaluated using a paired t-test. For data that are not normally distributed, Wilcoxon signed rank tests are used to evaluate the difference in paired observations from baseline to follow-up in place of the t-test. Normality is assessed by the Shapiro-Wilk test, where a P value <.05 was interpreted as evidence of nonnormality of the data. All analyses are based on available data; no imputation for missing data was performed. Statistical analyses were performed by an independent statistician using SAS version 9.4.
Results
Participants
A total of 30 participants were enrolled at 3 US centers from December 2018 to April 2019. All 30 participants received bilateral cryoablation treatment of both the inferior meatus and middle meatus. One participant missed the 1-month visit. The NOSE, SNOT-22, and CGI-I were not completed by 1 participant at the 3-month visit. Five participants (16.7%) had undergone previous cryoablation of the middle meatus without adequate symptom resolution. Demographics and other baseline data are presented in Table 1.
Demographics and Baseline Characteristics (30 Participants).

Abbreviations: IQR, Interquartile range; mini RQLQ, mini Rhinoconjunctivitis Quality of Life Questionnaire; NOSE, Nasal Obstruction Symptom Evaluation; rTNSS, reflective Total Nasal Symptom Score; SD, standard deviation; SNOT-22, Sino-Nasal Outcome Test; VAS, visual analog scale.
aRhinitis type was not specified for 2 participants (N = 28).
Procedure Characteristics
One-hundred-thirty-two treatments were administered in the 30 participants. Most participants underwent a single treatment at each location (mean number of treatments per location 1.1). Location means were 1.3 for the left middle meatus, 1.1 for the right middle meatus, and 1.0 for both the left and right inferior meatus.
Forty percent of participants experienced some level of pain during the treatment with the mean (SD) pain score during the treatment of 1.0 (2.0) on a scale of 0 to 10. No treatments were discontinued due to pain or discomfort. Sixty percent of participants experienced some posttreatment pain or discomfort with a mean (SD) posttreatment pain score of 4.1 (3.9).
Patient-Reported Outcomes
The primary endpoint of the change from baseline in the rTNSS demonstrated statistically significant improvement at the 1-month and 3-month follow-ups (Table 2). Twenty-six of the 30 participants (86.7%) experienced a 1-point or more improvement in the total rTNSS, and the median change in each of the 4 individual rTNSS subscales showed significant improvement over baseline (P < .001) at the 3-month follow-up (Figure 2). All participants who had undergone previous cryoablation experienced ≥1-point reductions in the total rTNSS at 3 months post treatment.
Change From Baseline in rTNSS at 1 and 3 Months.

Abbreviation: rTNSS, reflective Total Nasal Symptom Score.
Results are presented as median [IQR] or % (n/N).
aThe rTNSS has a range of 0 (no symptoms) to 12 (severe symptoms). A change from baseline of ≥1 point is considered the minimal clinically important difference (MCID).
bP value is based on the Wilcoxon signed rank test.
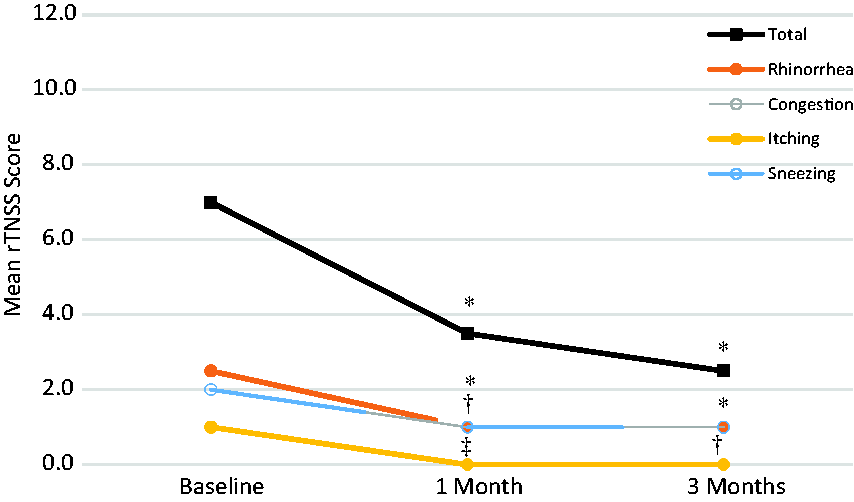
Change in median rTNSS total score and subscores over time. Statistical significance is indicated by * for P < .0001 for total, rhinorrhea, and congestion scores at 1 and 3 months and sneezing at 3 months; †P < .01 for sneezing at 1 month and itching at 3 months; and ‡ P < .05 for itching at 1 month.
The change from baseline to 3-month follow-up for the secondary PRO assessments are shown in Table 3. At the 3-month visit, 89.7% (26/29) of the participants were considered NOSE responders (1 assessment was not done). The change in the mean NOSE scores over time is shown in Figure 3. Twenty-two of 29 participants (75.9%) achieved the MCID of –8.9 points for the overall SNOT-22 score at 3-months post treatment (1 assessment not done).
Change From Baseline to 3-Month Follow-up in Secondary Patient-Reported Outcomes.

Abbreviations: mini RQLQ, mini Rhinoconjunctivitis Quality of Life Questionnaire; NOSE, Nasal Obstruction Symptom Evaluation; SNOT-22, Sino-Nasal Outcome Test; VAS, visual analog scale.
Results are reported as mean ± SD or median [IQR]. Negative changes indicate improvement.
aP values are based on paired t-tests.
bOne participant each inadvertently did not complete the NOSE and SNOT-22 assessments at the 3-month visit.

Change in mean nasal obstruction symptom evaluation (NOSE) scores over time. NOSE scores were inadvertently missed at the 1-month visit for 15 participants due to an administrative error: baseline and 3 months n = 30; 1 month n = 15 (baseline score is 46.3 ± 24.7 when restricted to these participants). Statistical significance is indicated by *P < .05 and †P < .001 for comparison to baseline. Error bars indicate standard deviations.
The median change in total score and each of the 5 subscale scores of the mini RQLQ showed statistically significant improvement over baseline at the 3-month follow-up (P < .0001 for total, activities, practical problems, nasal symptoms, and other symptoms; P = .023 for eye symptoms). Twenty-six of the 30 participants (86.7%) achieved the MCID of –0.4 points for the total mini RQLQ score at 3 months.
Physicians’ evaluations of participant improvement, using the CGI-I, indicated that 89.7% (26/29) of participants experienced improvement at 3-months post treatment. Two participants experienced no change, 1 was considered worse, and 1 did not have an assessment completed.
Imaging Analysis
At 3 months post procedure, 36% of inferior turbinate images were observed to have reduced congestion (improvement) by 1 or more grades, while 64% of the inferior turbinate images were not observed to have improvement in congestion.
Adverse Events
There were no serious adverse events reported. A total of 40 nonserious adverse events were reported in 24 participants. One adverse event was not considered related to either the device or procedure (sinusitis). The most common events related to the device and/or procedure were headache (12/30, 40.0%), postprocedure pain or discomfort (facial, jaw, tooth, occipital, treatment site, unspecified; 10/30, 33.3%), and palate numbness (8/30, 26.7%). The events required no to minimal (over the counter medication) intervention and typically resolved the same day as the procedure. All related events were transient and resolved before the 3-month visit.
Discussion
Cryoablation of the posterior nasal nerve at the middle meatus for treatment of chronic rhinitis has been demonstrated to be safe and effective. 3 , 4 To our knowledge, this is the first report of cryoablation treatment including the inferior meatus.
Our findings suggest that including the inferior meatus as a secondary cryotherapy treatment site is safe and as effective as treatment at the middle meatus only. We demonstrate a significant change from baseline (-4.0) in the median rTNSS. Our rTNSS change from baseline is slightly greater than the 3-month changes reported by Hwang et al. 3 in 27 participants (-3.3) and by Chang et al. 4 in 98 participants (-3.1). Our population had slightly higher baseline scores than either of the other studies (7.0 vs 6.2 and 6.1, respectively) due to a higher score on the sneezing subscale (2.0 vs 1.2 and 1.0, respectively). Cryoablation of the inferior meatus is effective but does not appear additive to treatment of the middle meatus treatment at 3 months. It is unknown if treatment of the inferior meatus may be additive at longer follow-up with a larger sample size.
The most common adverse event reported with cryoablation of the posterior nasal nerve is post treatment pain/discomfort. We reported 60.0% of participants experienced post treatment pain/discomfort. These findings agree with the results reported by Chang et al in which 77.8% of participants reported some level of post treatment pain/discomfort. 4 Hwang reported that 26.0% of their participants experienced more than mild post treatment pain/discomfort. 3 This suggests that cryoablation of the inferior meatus does not cause more pain/discomfort over ablation of the middle meatus alone. Although pain/discomfort is common, it is transient (typically resolved the day of procedure) and does not require intervention beyond over the counter pain medications.
Independent assessment of imaging indicated that 36% of inferior turbinates showed reduced edema after treatment. The methodology is intended for direct observation to evaluate the percent of space that the inferior turbinate head occupies. We made this assessment from still video images and feel that evaluation of the 2-D cross-sectional area was highly dependent on the exact position and angle of the still image captured within the nasal valve. Additionally, to reduce observer bias, we deidentified and uncoupled the pre and post treatment images and were, therefore, unable to compare the treatment effect within each patient. Ultimately, this methodology may have been too restrictive and led to a result that was less than we anticipated.
Strengths of the current study include the follow-up of all 30 participants through the 3-month visit for the primary endpoints, and the inclusion of additional PROs such as the NOSE, VAS, and SNOT-22 to evaluate the broader impact of the cryotherapy treatment on patients. The results of these assessments were very consistent; each assessment demonstrated greater than 86% responder rates or MCID achievement.
Limitations of this study include the small sample size, lack of a control arm, and short-term follow-up. These limitations were intentional, as this was designed as a pilot study. The results of this study can be used to direct the design of future studies that can evaluate larger populations with appropriate controls and longer follow-up.
Conclusion
Cryoablation of the middle and inferior meatus appears to be a safe and feasible option for treatment of chronic rhinitis. In this feasibility study, there was significant improvement in rhinitis symptoms post treatment that are comparable to previous studies. Adverse events are nonserious and transient in nature.
Footnotes
Acknowledgments
The authors thank April Slee of New Arch Consulting for the statistical analysis. The authors also thank the following study coordinators and office staff: David Campbell and Mary Anne Martini of Bethlehem ENT; Wendy Zhu of San Francisco Otolaryngology Medical Group; and Santana Eppler, Katie Lee, and Sandra Hoerster of the office of Tracy Byerly, MD.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D. Y. is a consultant for Stryker ENT and E. M. O. is an employee of Stryker ENT. The other authors have no conflicting interests to declare.
Ethical Approval
Advarra IRB approved the study protocol (Pro00030820) and informed consent documents for all participating centers.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research for this study was funded by Arrinex, now part of Stryker ENT.
Statement of Human and Animal Rights
The study adhered to good clinical practices and ethical standards. The STROBE reporting guidelines for cohort studies were applied.
Statement of Informed Consent
Written informed consent was obtained from all participants.