
Abstract
Background
Chronic rhinitis impacts 60 million Americans and is associated with significant costs for patients. Although medical treatments are first line, some patients require surgical intervention such as vidian or posterial nasal neurectomy. Previous reviews have investigated the role of surgical management in chronic rhinitis, but none have investigated a longstanding treatment with recent interest: cryotherapy.
Objective
To identify the safety, efficacy, and durability of treatment response of cryotherapy in treating chronic rhinitis.
Methods
A systematic literature review was performed to identify studies that investigated the utility of cryotherapy in chronic rhinitis. Only studies with the primary objective of assessing the efficacy of cryotherapy on chronic rhinitis were included. Patients were classified as allergic rhinitis, nonallergic rhinitis (vasomotor rhinitis), or mixed rhinitis using the original author’s criteria. Data were extracted regarding reported complications, treatment efficacy, and length of follow-up.
Results
A total of 110 abstracts were identified, of which 15 were included in this review. Epistaxis and nasal obstruction were commonly reported complications. No serious adverse events were reported. For obstructive symptoms, “reduced” symptoms were reported in 63.4% to 100% of patients. In regard to rhinorrhea, reports of reduced symptoms were experienced from 77% to 100% of patients. Seven studies used only patient-reported improvements without stratifying results based on symptom type; general improvements ranged from 67% to 100%. Nine studies noted symptom improvement in nonallergic cohorts ranging from 67% to 97.5% of patients. Four studies noted improvement in allergic cohorts ranging from 63.4% to 80% of patients. Two studies noted improvement in patients with mixed pictures ranging from 92.5% to 100%.
Conclusions
Although cryotherapy appears safe and efficacious, heterogeneous past investigations with low-quality evidence make strong, evidence-based recommendations difficult to make. Further study with validated metrics and controlled populations is certainly warranted and should be encouraged.
Keywords
Introduction
Chronic rhinitis impacts roughly 60 million Americans and includes allergic rhinitis, nonallergic rhinitis, and mixed subtypes. Although clinical presentation may vary, watery rhinorrhea and nasal congestion are dominant symptoms which may negatively impact a patient’s quality of life 1 and drive patients to seek treatment. Medical treatments for chronic rhinitis are considered first line and account for the majority of economic costs, which have been estimated at over $600 per patient per year. 2 However, not all patients respond adequately to available medical treatments and may require procedural or operative intervention for recalcitrant chronic rhinitis.
Classically, vidian neurectomy is the procedure of choice for refractory rhinitis, whereas relatively more recent technical studies have described the role of the posterior nasal neurectomy.3–9 Several recent systematic reviews have explored the evidence base for the surgical treatment of chronic rhinitis. Marshak et al. focused on procedures that divide the vidian nerve, concluding that a role exists for endoscopic vidian neurectomy to improve rhinorrhea. 4 Meanwhile, Halderman and Sindwani performed a similar review, concluding that endoscopic techniques appear less morbid than an open, transantral approach. 10 Although vidian neurectomy appears efficacious, there are several downsides including the potential nasal and ocular morbidities as well as increased health-care costs and resources associated with general anesthesia and operative intervention.
The pathophysiology of chronic rhinitis is complex and involves both sensory and autonomic nerve pathways. Sensory pathways detect specific allergens or irritants which stimulate a parasympathetic response via the vidian nerve. 11 Procedures such as a vidian neurectomy have been shown to reduce symptoms of chronic rhinitis. 12 However, side effects such as dry eyes due to ablation of parasympathetic innervation to the lacrimal gland have been noted. 13 Ablation of the posterior nasal has been hypothesized to reduce the side effects of dry eyes experienced with a vidian neurectomy. 10 Therefore, targeted therapies to this region may offer relief of chronic rhinitis symptoms with limited side effects are desired. Due to the simple, office-based nature, cryotherapy has gained interest. Cryotherapy utilizes liquid nitrogen to ablate posterior nasal tissue. Through extremely low temperature, cryotherapy forms ice crystals and induces cellular contraction to ultimately lyse cells. 14
Despite several decades of intermittent descriptions of the use of cryotherapy as a treatment for chronic rhinitis, this technique is not widely utilized. Historically, several cryotherapy devices have been utilized for chronic rhinitis.15–17 The most recent investigation of cryotherapy in the treatment of chronic rhinitis was a small clinical trial employing a device designed to ablate the posterior nasal nerve. Given the lack of utilization of this treatment modality for chronic rhinitis, the goal of this study was to review the evidence surrounding the use of cryotherapy for the treatment of chronic rhinitis. Specifically, we were interested in performing a systemic review exploring the efficacy, safety, and durability of treatment response of cryotherapy.
Methods
A comprehensive literature search was performed on February 3, 2018. Articles were identified in PubMed, Cochrane Database, and Scopus using the search strategy: “(cryotherapy or cryosurgery) and (vasomotor rhinitis or nonallergic rhinitis or allergic rhinitis or rhinorrhea or nasal obstruction).” The Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement was used throughout this systematic review. 18
Abstracts were independently reviewed by 2 reviewers (A.R.K. and T.A.J.). Only studies with the primary objective of assessing the efficacy of cryotherapy on chronic rhinitis were included. The full texts of identified abstracts were reviewed for all available studies. Case reports, review articles, and nonhuman studies were excluded. In addition, studies describing the use of cryotherapy for medical diseases other than chronic rhinitis were excluded. Finally, studies not in English that could not be translated were excluded. References from all included studies were reviewed in order to identify any additional studies. Patients were classified as allergic rhinitis, nonallergic rhinitis (vasomotor rhinitis), or mixed using the original author’s criteria. Data were extracted regarding reported complications, treatment efficacy, and length of follow-up. Level of evidence for each included article was performed using Oxford Center for Evidence-Based Medicine (OCEBM). 19
Assessment of Risk of Bias
The risk of bias was assessed according to the Cochrane Handbook for Systematic Reviews of Interventions. The latest version of this tool was updated in March 2011, version 5.1.0. 20 Two authors assessed the risk of bias according to this tool. All disagreements were resolved by the way of discussion. Risk of bias items included the following: incompleteness bias, reporting of success metrics bias, and other biases.
Statistical Methods
Given the expected heterogeneity in outcome metrics, no meta-analysis or statistical tests were performed.
Results
The initial literature review yielded a total of 110 abstracts. A review of potential abstracts identified 36 articles that described cryotherapy for chronic rhinitis. Of these articles, 17 were unable to be translated into English and 4 were duplicates. The remaining 15 met inclusion and exclusion criteria and were included in final review (Figure 1). Of these studies, 9 included patients with nonallergic rhinitis only, 1 included patients with allergic rhinitis only, 3 included allergic and nonallergic rhinitis cohorts in their studies, and 2 had information on patients with mixed symptoms of allergic and nonallergic rhinitis. In total, data from 1266 patients were available for review (Table 1). The majority of articles were published between 1977 and 1997, with only a single paper published within the last 5 years. The majority of articles were deemed OCEBM level 4 with 1 article being level 2c.15–17,21–30
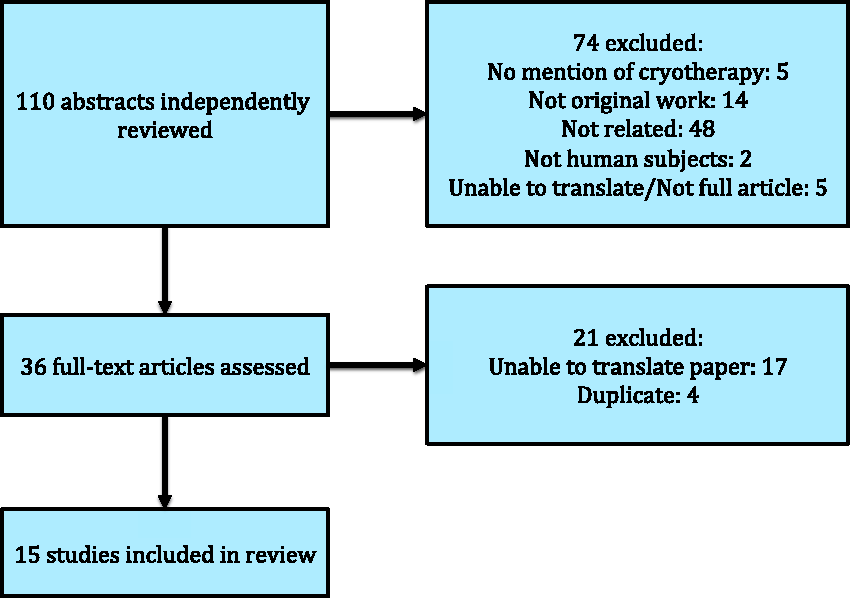
Preferred Reporting Items for Systematic Reviews and Meta-Analysis diagram describing the article selection.
Study Background and Patient Demographics.
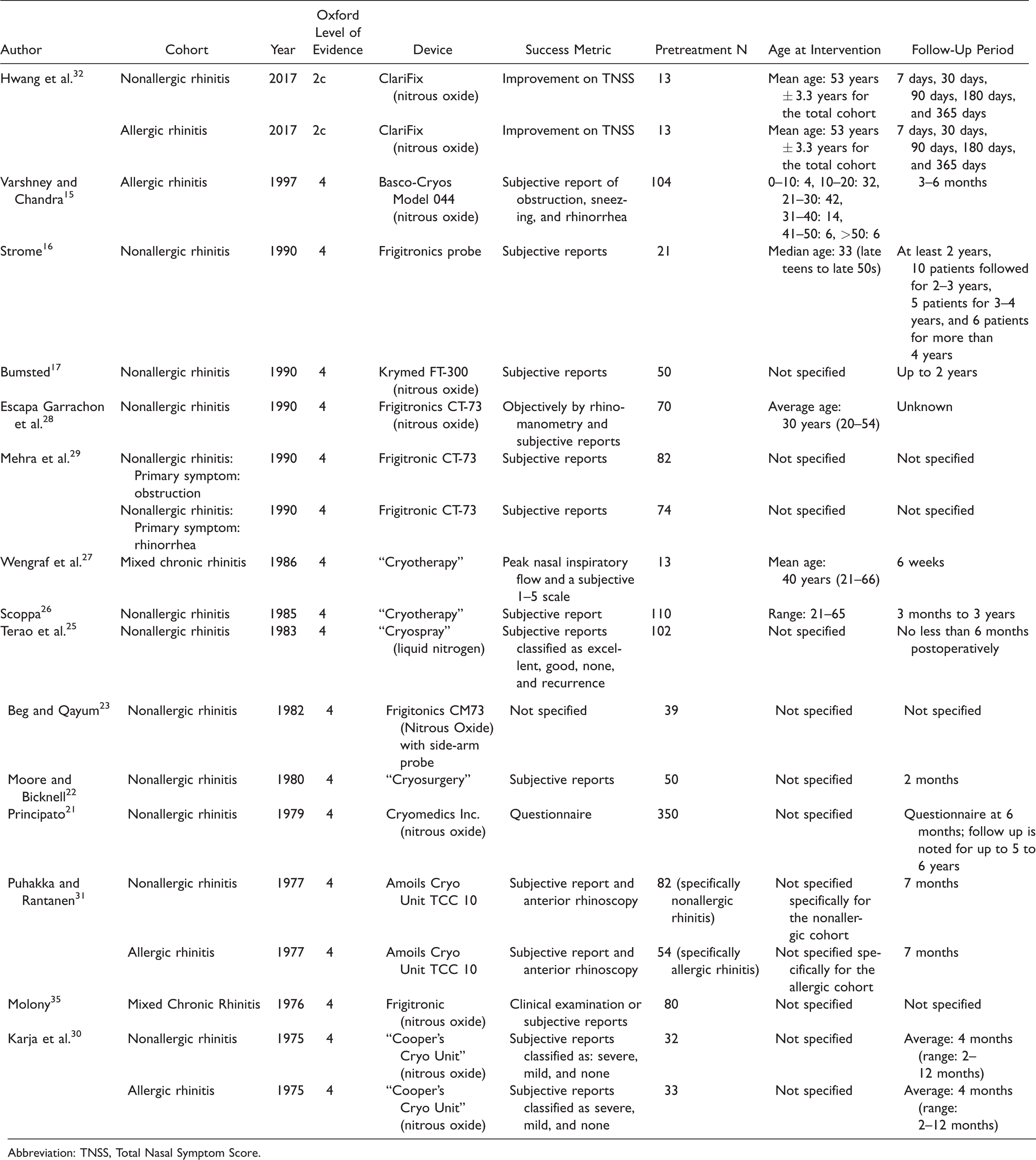
Abbreviation: TNSS, Total Nasal Symptom Score.
There was little consistency in duration of therapy or devices used. Duration of therapy ranged from 5 to 8 seconds to 2 to 3 minutes.15,25 Only 1 study investigated the role for repeat applications. 31 The majority of studies utilized Frigitronics probes (Cooper Surgical, Trumbull, CT). Device comparison was further limited by 3 studies referencing “cryotherapy” without addressing the device used. Only the most recent study investigated an U.S. Food and Drug Administration (FDA)-cleared device. Temperatures were more consistent, varying between −75°C and −90°C.15,31
Cryotherapy Reduces Obstructive Symptoms and Rhinorrhea
Five studies separated subjective reports based on obstructive symptoms and rhinorrhea.17,28,29,32,33 Although the studies did not use verified quality of life questionnaires, all studies asked patients to gauge the success of the therapy. For obstructive symptoms, “reduced” symptoms were reported in 63.4% to 100% of patients. In regard to rhinorrhea, reports of reduced symptoms were experienced from 77% to 100% of patients. Seven studies used only patient-reported improvements without stratifying results based on symptom type; general improvements ranged from 67% to 100% (Table 2). A widely accepted measurement of symptoms, the Total Nasal Symptom Score (TNSS), 34 was used in 1 study (Table 2). 32 The authors noted significant reduction in TNSS from baseline (6.2 ± 0.5) to 30 days (2.6 ± 0.3), 90 days (2.7 ± 0.4), 180 days (2.3 ± 0.5), and 365 days (1.9 ± 0.3) (P < .001). Furthermore, patient-reported obstruction was reduced from 1.9 ± 0.2 to 0.5 ± 0.2, and rhinorrhea was reduced from 2.4 ± 0.8 to 1.2 ± 0.2.
Outcomes of Cryotherapy in Allergic and Nonallergic Cohorts.
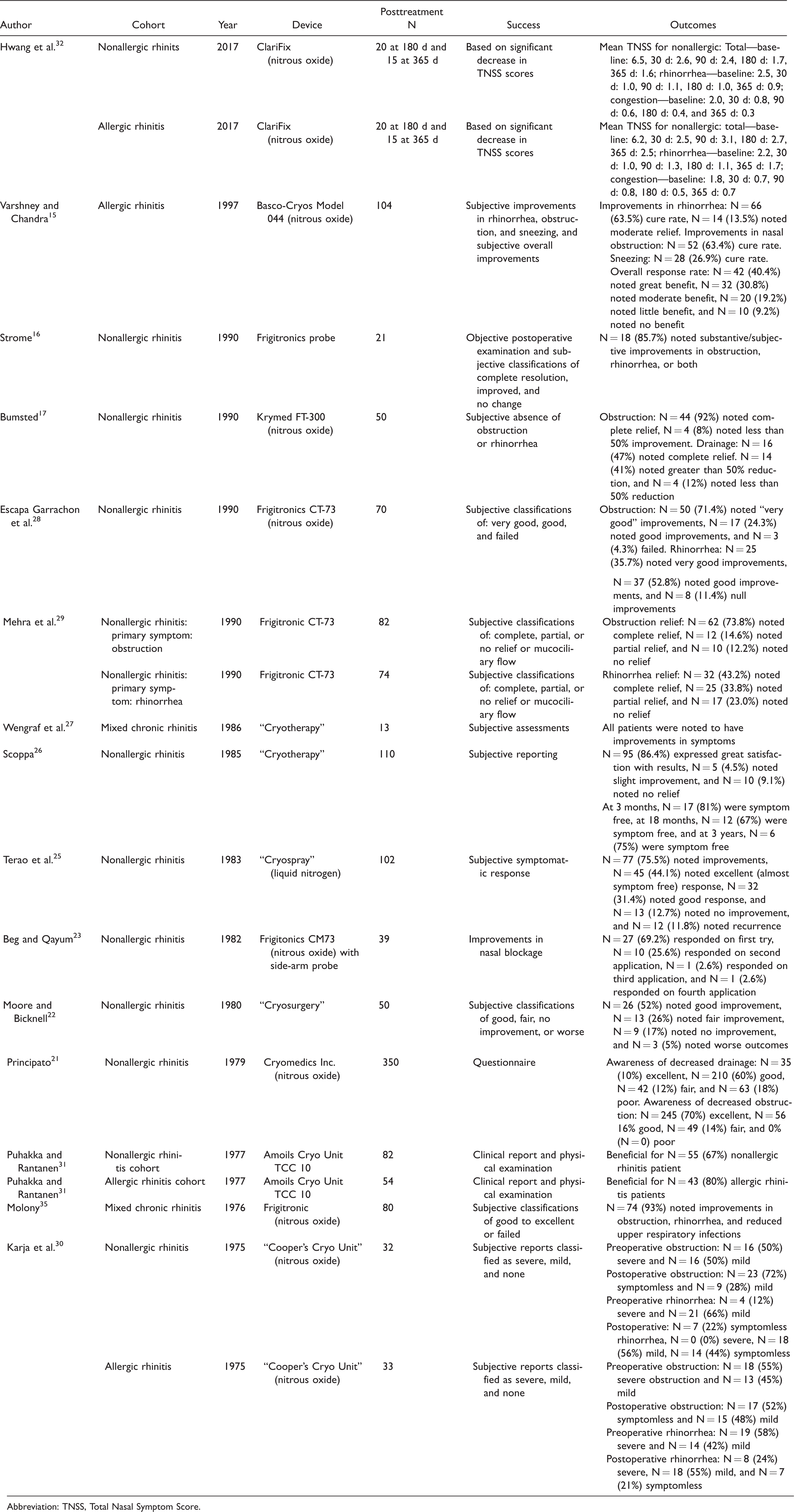
Abbreviation: TNSS, Total Nasal Symptom Score.
Effectiveness of Cryotherapy for Nonallergic, Allergic, and Mixed Chronic Rhinitis
Nine studies specifically examined the role of cryotherapy for the treatment of nonallergic rhinitis. Improvement of overall symptoms was found in 67% to 95.7% of patients with nonallergic rhinitis (Table 2). In 1977, Puhakka and Rantanen reported the smallest improvement in overall patient reported symptom control in 67% of their patients with nonallergic rhinitis. 30 Meanwhile in 1975, Karja et al. reported decrease in obstructive symptoms in 100% of their nonallergic cohort. 31 The recent study by Hwang et al. demonstrated statistically significant differences in TNSS scores from baseline that were maintained at 30, 90, 180, and 365 days posttreatment (6.5 ± 0.7 to 1.6 ± 0.4 at P < .01). Furthermore, the authors analyzed individual domains of the TNSS and demonstrated a decrease in rhinorrhea scores from 2.5 to 0.9 and a decrease in obstructive symptoms from 2.0 to 0.3 in 9 patients but did not note the statistical significance of these reductions. 32
Four studies examined allergic cohorts, with overall symptom improvement ranging from 63.4% to 80% of patients (Table 2). Hwang et al. demonstrated statistically significant decreases in TNSS scores at 30, 90, and 365 days (6.2 ± 0.7 to 2.5 ± 0.6 at 365 days P < .05) though greater than half of the allergic cohort was lost to follow-up at 1 year. These authors also reported a decrease in obstructive scores from 1.8 to 0.7 and a decrease in rhinorrhea scores from 2.2 to 1.7 at 365 days but did not note the statistical significance of these reductions. Meanwhile, Puhakka and Rantanen found that 80% of allergic rhinitis patients reported a decrease in overall symptoms. 31 Karja et al. demonstrated a decrease in obstructive symptoms in 100% of allergic patients while 76% of patients noticed decreases in rhinorrhea. 30
Finally, 2 studies specifically examined patients with a mixed clinical picture. In this patient population, 92.5% to 100% noted a decrease in overall symptom burden. In 1986, Wengraf et al. investigated 13 patients with mixed chronic rhinitis and reported subjective improvement in overall symptoms in all patients by using a 1- to 5-point Likert-type scale. 27 Using subjective classifications of “good to excellent” or “failed,” Molony et al. reported that 74 (93%) patients experienced improvements in obstruction, rhinorrhea, and frequency of upper respiratory infections. 35
Safety of Cryotherapy
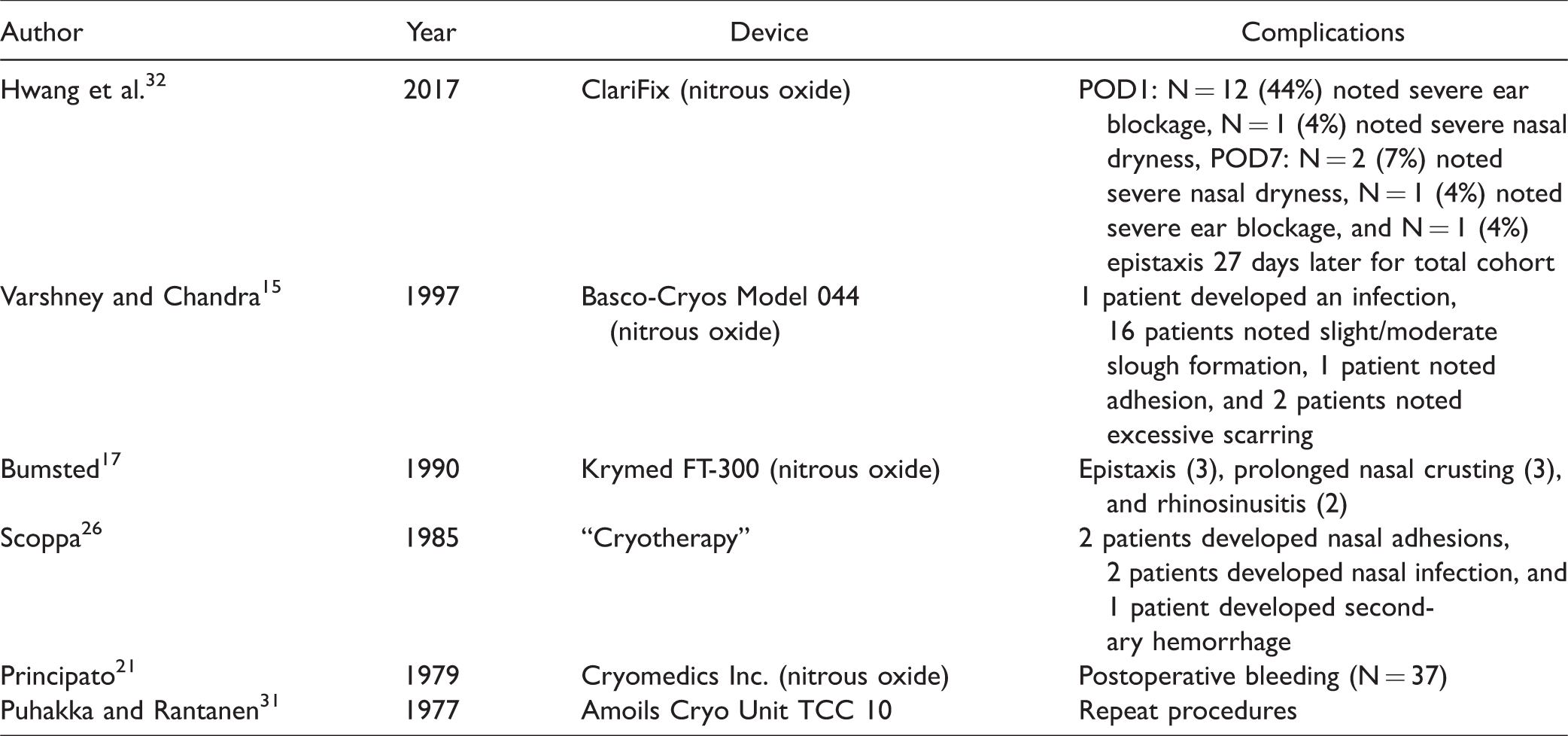
Six studies, encompassing a total of 641 patients, investigated the complications associated with cryotherapy. The most common reported complications were epistaxis and nasal obstruction or crusting (Table 3). In 1979, Principato noted that 37 of the 350 (10.6%) patients had bleeding during the procedure, but this resolved with topical adrenaline immediately after the procedure for all patients. 21 Two studies reported epistaxis following cryotherapy in 4 of the 76 (0.8%) patients, with 1 requiring electrocautery at the procedure site.15,32 Meanwhile, obstruction and crusting were reported in 3 studies and occurred in a total of 8 (3.0%) patients. Postoperative infections were reported in a total of 3 patients (0.5%) in 2 separate studies. All infections responded to antibiotics. No severe adverse events were reported across all 6 studies.
Safety and Complications Associated With Cryotherapy.
Discussion
Chronic rhinitis is an incredibly common diagnosis that may originate from either nonallergic or allergic causes. 36 With the recent development of a novel cryotherapy delivery device with promising results, there has been renewed interest in surgical intervention for chronic rhinitis, specifically the use of cryotherapy. 32 This review details the safety, efficacy, and durability of treatment response of cryotherapy as a treatment strategy for chronic rhinitis. Beyond the apparent low risk of cryotherapy for chronic rhinitis, the heterogeneity of data makes treatment-related outcomes difficult to objectively ascertain. First, the majority of publications investigating the role of cryotherapy for chronic rhinitis are outdated, as most were published between 1977 and 1997;15–17,21–30 a period of time prior to which the field of rhinology has undergone substantial advances. Although these investigations are relatively remote, the results are promising as all studies demonstrated improvement in symptoms with 63% to 95.7% of patients noting improvement in overall symptoms. Obstructive symptoms improved in 63.4% to 100% and rhinorrhea improved in 77% to 100% of patients. Endoscopic vidian neurectomy has also been shown to significantly reduce obstructive symptoms and rhinorrhea, but currently no evidence is available to compare outcomes between the 2 procedures. 4 Currently, literature comparing posterior nasal neurectomy to endoscopic vidian neurectomy or cryotherapy is sparse. Halderman and Sindwani noted only 5 studies that investigated this technique. 10
The overall safety profile of cryotherapy is favorable. Six studies in this review noted complications of cryotherapy.15,17,21,26,31,32 Across the 6 studies with reported complications, a total of 55 (8.6%) patients experienced complications. Common complications included epistaxis, nasal obstruction, nasal crusting, or ear blockage, none of which were reported to be serious. Postoperative bleeding, the most prevalent complication, was readily managed postprocedurally with topical therapies in most cases. In contrast, a study of 85 patients with chronic rhinitis who underwent vidian neurectomy reported that 26 (30.6%) patients developed xerophthalmia lasting for a month, and 8 (9.4%) patients developed numbness of the lip and palate. 37 In our review, epistaxis was reported in 0.8% (4 of the 76) of patients who were treated with cryotherapy. In an extensive review of vidian neurectomy for rhinitis, epistaxis occurred in 1.75% (8 of the 457) of patients. 4 In addition to increased risk of dry eyes or paresthesias, vidian neurectomy incurs a direct increased cost of therapy and an increased operative risk associated with the use of general anesthesia. 6 Currently, there are no randomized control trials demonstrating the safety or efficacy of cryotherapy for the treatment of chronic rhinitis compared to other surgical interventions; however, the overall safety profile with the lack of potential serious side effects is encouraging.
Although literature on the long-term durability of cryotherapy is limited, 2 studies mentioned results at a year postoperatively or longer. Most studies investigated time points within 1 year. However, Hwang et al. reported that for the 9 nonallergic rhinitis and 6 allergic rhinitis patients followed up for 1 year, TNSS was significantly lower than baseline (6.2 ± 0.5 to 1.9 ± 0.3, P < .001). 32 Obstruction (1.9 ± 0.2 to 0.5 ± 0.2) and rhinorrhea (2.4 ± 0.8 to 1.2 ± 0.2) domains were noted to have the most significant improvements from baseline at 1 year. Strome noted that 18 of the 21 patients had noted improvement in at least 2 years. 16
Despite encouraging results, these studies do have significant weaknesses, which limit the strength of conclusions that can be drawn. One of the most substantial weaknesses is the lack of rigor in diagnostic criteria for chronic rhinitis and differentiation of rhinitis subtypes. Another drawback is the lack of validated, patient-reported outcome metrics. Only 1 article used the TNSS making comparison of clinical improvement difficult. These weaknesses make assessments of true effect sizes difficult and make comparisons across studies challenging. Finally, and most importantly, none of the reported studies included control groups.
Currently, only 1 FDA-cleared cryotherapy device is available for the treatment of chronic rhinitis in adults. 38 Recent investigation of this device applied cryotherapy, via nitrous oxide, delivered to the posterior nasal nerves along the nasal mucosa. With the use of this novel cryotherapy device, Hwang et al. demonstrated improved patient-reported outcomes regardless of atopic status. 32 This device, such as other cryotherapy devices, benefits from the lack of overhead procedural costs associated with other surgical interventions and can be performed in-office. Although it may be assumed that this device is effective for the treatment of chronic rhinitis, future controlled trials to validate Hwang et al.’s conclusions should be encouraged.
Conclusion
Chronic rhinitis is a common disease most often treated with medical therapy; however, for a subset of patients, surgical intervention may be necessary. Although surgical procedures such as vidian neurectomy have been the predominate intervention, cryotherapy has been utilized for the treatment of chronic rhinitis since the 1970s. A recent report of a new FDA-cleared device suggests that cryotherapy is safe and corroborates earlier reports suggesting efficacy. Although this procedure appears safe and recent results are promising, heterogeneous past investigations with low-quality evidence make strong, evidence-based recommendations difficult to make. Further study with validated metrics, accepted symptom scales such as the TNSS, and controlled populations is certainly warranted and should be encouraged. Despite these obvious limitations, cryotherapy shows promise as a useful tool for the management of chronic rhinitis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.