
Abstract
Background
Inverted papillomas (IPs) are benign, locally aggressive neoplasms with a high recurrence rate that most commonly arise from the lateral nasal wall. Rarely, IP can originate from the lacrimal sac and/or nasolacrimal duct (NLD) system. A 58-year-old man presented with chronic epiphora and an enlarging mass inferior to his left medial canthal tendon (MCT) for 2 years.
Objective
The patients’ clinical presentation and surgical management are described. A literature review on IP of the lacrimal sac and NLD system was conducted.
Methods
Case report.
Results
We present a case of an IP that arose primarily from the lacrimal sac and grew below the MCT rather than extending above it. This is one of few published case reports detailing the use of a combined endoscopic and external approach for the resection of an IP of the lacrimal sac.
Conclusion
Combined endoscopic and external resection is a viable approach for complete removal of extensive IP of the lacrimal sac and NLD system. IP arising from the lacrimal sac may grow below the MCT or extend above it as previously reported.
Keywords
Introduction
Lacrimal sac tumors are exceedingly rare but can be life threatening with a 55% malignancy rate.1–3 The majority arise as primary tumors of epithelial origin (60%–94%). 4 Among benign epithelial lacrimal sac tumors, papillomas are most common, occurring 36% of the time, with growth patterns including exophytic, endophytic/inverted, or mixed. 1 Inverted papillomas (IPs) are benign, locally aggressive neoplasms with a high recurrence rate.5,6 IP most commonly arises from the lateral nasal wall or paranasal sinuses and much less frequently from the lacrimal system.7,8 Only a few cases of IP originating primarily from the lacrimal sac have previously been reported.3,6,9 In addition, pathology arising within the lacrimal sac with extension above the medial canthal tendon (MCT) has traditionally been considered worrisome and indicative of a possible neoplasm. On the other hand, pathology arising within the sac that remains or grows below the MCT is considered less worrisome.10–13 We report a case of a lacrimal sac IP that initially presented with growth below the MCT and was removed in a combined endonasal and external approach by both otolaryngology and oculoplastics.
Methods
The authors describe a case report and review of the literature on IP of the lacrimal sac and nasolacrimal duct (NLD) system. Institutional review board approval was not required at our institution for reporting of individual cases. Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.
Case Report
A 58-year-old African male from Liberia initially presented to the Wills Eye Emergency Room with a 2-year history of a progressively enlarging mass inferior to the left MCT (Figure 1(A)). The patient endorsed a pressure-like sensation around the mass, constant tearing, and 1 episode of epistaxis prior to presentation. He denied pain, hemolacria, rhinorrhea, diplopia, or pain with extraocular movements. He also denied any systemic symptoms including fevers, chills, or weight loss. His medical history was notable for hypertension; he had no past surgical or ocular history. He did not take any medications. Social history was significant for being a current smoker with a 3 pack-year smoking history and a former heavy alcohol user. Family history was noncontributory. Review of systems was otherwise negative.

A, Preoperative external photograph of a 58-year-old man from Liberia who presented with a progressively enlarging mass below his left medial canthus for 2 years. B, Postoperative external photograph after an inverted papilloma was removed in a combined endoscopic and external approach.
On ophthalmologic exam, uncorrected visual acuity was 20/20 in both eyes, pupils were equally round and reactive to light and accommodation, intraocular pressures were normal, extraocular movements were intact, and color plates were full. Visual fields demonstrated an inferonasal defect in the left eye. Hertel exophthalmometry was even bilaterally, and cranial nerves II–XII were intact. External examination was significant for a 3.3 cm × 2.5 cm × 2 cm nonfluctuant, firm mass located inferior to the MCT on the left. There was nonaxial superotemporal displacement of the left globe with 1 to 2 mm of hyperglobus. The mass was nontender and nonerythematous. With massage, no purulent material was able to be expressed from the punctae. There was medial canthal dystopia but no madarosis or ulceration of the left upper or lower eyelids. Anterior segment and dilated fundus examination were otherwise normal in both eyes.
The patient underwent computed tomography (CT) of the orbits which demonstrated a 3.4 cm (transverse) × 3.1 cm (anteroposterior) × 3.4 cm (craniocaudal) enhancing mass centered in the medial canthus and lacrimal sac of the medial left orbit (Figure 2(A)). The mass extended along the osseous canal of the NLD causing its bony expansion (Figure 2(B) and (C)) and was most consistent with a lacrimal sac tumor. Given the extent of the mass, the patient was referred to both the oculoplastics and otolaryngology clinics for further evaluation. Endoscopic, endonasal biopsy was performed in the office with histopathology revealing an IP (Figure 3(A) and (B)). The patient subsequently underwent magnetic resonance imaging (MRI) of the sinuses for surgical planning. MRI redemonstrated a T1 and T2 isointense mass measuring 4.0 cm × 2.6 cm in axial dimension centered in the left medial canthus (Figure 2(D)), extending inferiorly through the NLD, and exiting the inferior meatus into the inferior nasal cavity (Figure 2(E) and (F)).

A, Axial CT scan demonstrating a mass centered in the left lacrimal sac with erosion of the lacrimal fossa and nasal bones. B, Axial CT scan demonstrating a widened NLD secondary to tumor extension. C, Coronal CT scan demonstrating a left lacrimal sac mass eroding the lacrimal fossa and extending down the NLD causing its expansion. D, Axial T1 postcontrast MRI redemonstrating a large well circumscribed mass at the medial canthus with anterior extension and compression of the medial orbit. E, Axial T1 postcontrast MRI redemonstrating extension of tumor inferiorly within a widened NLD. F, Coronal T1 postcontrast MRI redemonstrating a mass at the lacrimal fossa extending into the NLD.
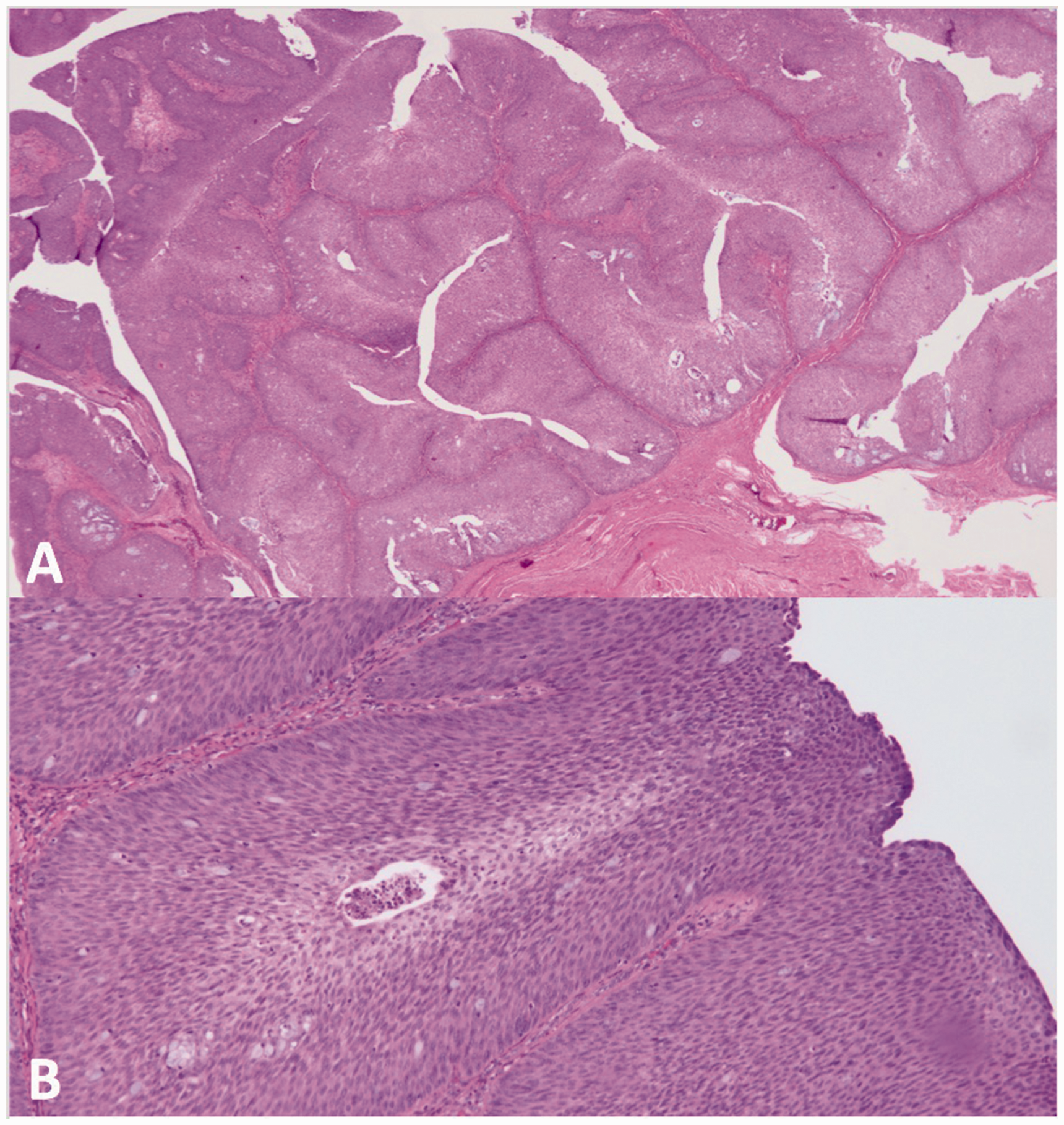
Pathologic findings, endoscopic biopsy. A, Nonkeratinizing stratified squamous epithelium growing inward toward the stroma consistent with inverted papilloma. B, Lobules of polarized epithelium composed of cells with elongated nuclei and cytoplasm reminiscent of transitional epithelium with few foci of neutrophils. No nuclear atypia or mitotic figures are present, consistent with a diagnosis of inverted papilloma without dysplasia.
A combined endonasal and external approach was employed. Endonasally, there was a papillomatous-appearing mass emanating from below the left inferior turbinate. An endoscopic medial maxillectomy was first performed. The lesion was visualized in the NLD and removed piecemeal by endoscopic resection. However, there was no endonasal attachment point of the tumor identified, and tumor was noted to continue superiorly into the lacrimal fossa and sac. Given the lack of an endonasal attachment point of the tumor, the oculoplastics team then proceeded with external orbitotomy.
An orbital malar crease incision was made with dissection into the subcutaneous plane to demarcate and mobilize the entire lower eyelid lesion anterior to the orbital septum. Orbitotomy with extensive exploration was then performed. The tumor was noted to be extremely adherent to the junction between the inferior orbital rim and the excavated NLD, so a modified Lynch incision was performed sparing the skin through the same incision as noted earlier. This was extended into a standard external dacryocystorhinostomy (DCR) incision of the nasal periosteum and the medial canthus was avulsed, which aided in disinsertion of the orbital tumor from the medial orbital wall without damaging the medial rectus or inferior oblique. The tumor was dissected from fascial attachments and noted to have a firm attachment point to the anterior lacrimal crest region. It was disinserted and the bony attachment was burred to ensure no rests of tissue remained. The entire orbital lesion was isolated and was noted to involve the lacrimal sac which was diffusely infiltrated by the IP and removed in its entirety. The entire specimen was removed via an external approach using loupes from the lacrimal sac fossa, inferior orbit, orbital rim, and the eyelid as well as about 1 cm of lesion prolapsing into the lacrimal duct. The NLD was noted to be severely widened secondary to tumor growth (Figure 4). A standard DCR was completed using Crawford tubes. Endoscopically, the common canaliculus was noted to be uninvolved. The skin incision was closed with an inferomedial to superolateral flap closure so as to avoid cicatricial ectropion and further lagophthalmos or exophthalmos given the extent of the lesion removed.

Intraoperative photograph during combined endoscopic and external resection of an inverted papilloma of the lacrimal sac demonstrating severe dilation of the NLD system superiorly secondary to tumor growth (solid arrow) and a large defect in the lateral nasal side wall (dotted arrow).
The patient healed well postoperatively (Figure 1(B)). He was noted to develop a small 0.5 cm left naso-cutaneous fistula 3 weeks postoperatively at the medial aspect of the fascial incision, which self-resolved 1.5 months after the procedure. He remained recurrence free at 3-months status-post tumor resection and was subsequently lost to follow-up thereafter.
Discussion
Given the high recurrence rate of IP (27%–71%) and 10% chance of malignant transformation, complete excision with clear tumor margins is of critical importance.7,14–16 In the past, local resection of lacrimal drainage apparatus (LDA) tumors with dacryocystectomy was employed, but this approach often resulted in lack of tumor margin clearance and a mortality rate as high as 47.5% at 5 years.3,11,17 More recently, en bloc resection of LDA tumors and the surrounding bony structures has been utilized for better tumor margin clearance with adjunct radiation and/or chemotherapy depending on tumor histopathology. 18 The use of a combined endonasal and external approach for complete excision of LDA papillomas has rarely been reported in the literature.7,19
Four prior cases detailing a combined approach were reported with initial exposure via external DCR and subsequent confirmation of diagnosis on frozen sections of lacrimal sac lumen biopsies. 19 Complete excision then proceeded first via dissection of the superior LDA from an external approach and then by dissection of the lower end of the NLD endoscopically, with ultimate removal of the entire specimen through the external wound. 19 Other joint approaches between otolaryngology and oculoplastics have included external en bloc resection of LDA tumors using combined external medial maxillectomy and medial orbitotomy with simultaneous reconstruction of resulting bony defects with titanium mesh or a T-plate. 17
We report a combined endoscopic and external approach to resection of a lacrimal IP. In addition, we report occurrence of a lacrimal sac IP presenting as a mass arising and growing below the MCT. Previously, LDA tumors have been reported to present as hard, fixed masses that extend above the MCT in more than half of cases.10–14 Papillomas have also been reported to present as lacrimal sac mucoceles confirmed on CT imaging, though this was not the case in our report. 10 Of 17 reported cases of IP arising from the lacrimal sac in the literature, only 1 report specified the mass extending both above and below the MCT, while other reports did not designate specific extension pattern.1,6,7,9,20–25 In this case, the patient presented with a firm, fixed mass arising and extending below the MCT. This should alert otolaryngologists and ophthalmologists to the fact that extension above or below the MCT does not necessarily differentiate neoplastic versus nonneoplastic processes.
In conclusion, the authors report a successful combined endonasal and external approach for the resection of an IP arising primarily from the lacrimal sac. This case demonstrates that lacrimal sac IP can arise and extend below the MCT as well as above it as previously reported. An interdisciplinary approach to surgical resection is of the utmost importance to ensure complete removal when tumor growth is extensive.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Institutional review board approval was not required at our institution for reporting of individual cases.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.