
Abstract
Paranasal sinus mucoceles are benign, expansive, cystic lesions which arise from retention of mucus secretions. They arise primarily in the setting of cystic degeneration of the sinus mucosa or secondarily in the setting of obstruction of the sinus ostium due to mucosal trauma or chronic inflammation. Septal mucoceles are rare. Only 10 cases to our knowledge have previously been reported. Patients are exclusively male, in their middle years, usually with a history of nasal trauma or nasal surgery. Nasal obstruction followed by headache present for 3 months to a year are the most common presenting symptoms. Here, we present a case of septal mucocele with dystrophic bone formation in a 57-year-old man arising 35 years after open septorhinoplasty treated successfully with total excision via an endoscopic, endoseptal approach. A review of the available literature was conducted to provide a consolidated update on diagnosis and management.
Introduction
Paranasal sinus mucoceles are benign, expansive, cystic lesions which arise from retention of mucus secretions. Mucoceles typically occur in the frontal, ethmoid, and maxillary sinuses.1–3 Septal mucoceles are very rare. There are only 10 cases reported in the literature (Table 1). Patients are typically male, in their middle years, usually with a history of nasal trauma or nasal surgery. Nasal obstruction followed by headache present for 3 months to a year are the most common presenting symptoms. Endoscopic partial excision with marsupialization or complete excision are the mainstays of treatment with no reported recurrences.1–7 Here, we report our case of a septal mucocele treated with complete excision using an endoscopic transnasal approach. This is the first reported case of a septal mucocele arising as a complication to septorhinoplasty, and it is unclear if it occurred as a result of his revision surgery or as a long-term complication of septal hematoma incision and drainage. A review of the available literature was conducted to provide a consolidated update on diagnosis and management. Because this article represents a single case report and literature review, institutional review board (IRB) approval was waived as per the standing policy of the IRB of the University of Texas Medical Branch (Galveston, TX).
Summary of Previously Reported Septal Mucoceles.

Abbreviations: M, male; F, female; FB, foreign body; FESS, functional endoscopic sinus surgery; HA, headache; n/a, not applicable.
Case Report
Patient CK is a 57-year-old man with a medical history of allergic rhinitis and obstructive sleep apnea who presented to clinic in May 2017 with nasal obstruction of 3 years’ duration which was refractory to medical management with nasal steroids and saline. He was a former boxer and reported a history of 3 open septorhinoplasties to correct trauma-related nasal defects and 1 incision and drainage of a septal hematoma following the last open rhinoplasty in 1982. On examination, a soft compressible mass was observed filling the anterior nasal cavity bilaterally arising from the anterior septum. The rest of the examination was normal. The patient presented with a prior needle aspiration revealing respiratory epithelium, confirming mucocele. To assess for interval changes prior to surgery, we obtained an updated computed tomography (CT) sinus scan revealing a 2.4 cm × 2.0 cm × 2.0 cm cystic mass in the anterior septum with dystrophic calcification particularly of the right wall of the cyst (Figures 1 and 2). He was taken to the operating room, and 6 cc of a thick gelatinous material was aspirated from the mass and sent for culture. Transnasal endoscopic approach was performed after making a modified Killian incision just anterior to the curvature of the mass on the right side. Three layers of tissue were noted with the superficial layer being the septal flap followed by a fibrous and boney layer with the mucosal lining of the cyst being noted most medially (Figures 3 and 4). At the end of the case, all the mucous membrane lining was removed along with the dystrophic bone, and the right and left septal flaps were re-approximated with quilting suture. Doyle splints were placed at the end of the case and left in place for 3 weeks. Final pathology for the case reflected bone and respiratory epithelium consistent with a mucocele. At the first postoperative visit, the splints were removed and nasal endoscopy examination revealed flat septal flaps without crusting or swelling. The patient reported significant improvements in nasal airflow.

CT sinus fusion protocol, axial view. Midline septal mass and notable right-sided dystrophic bone formation are seen.
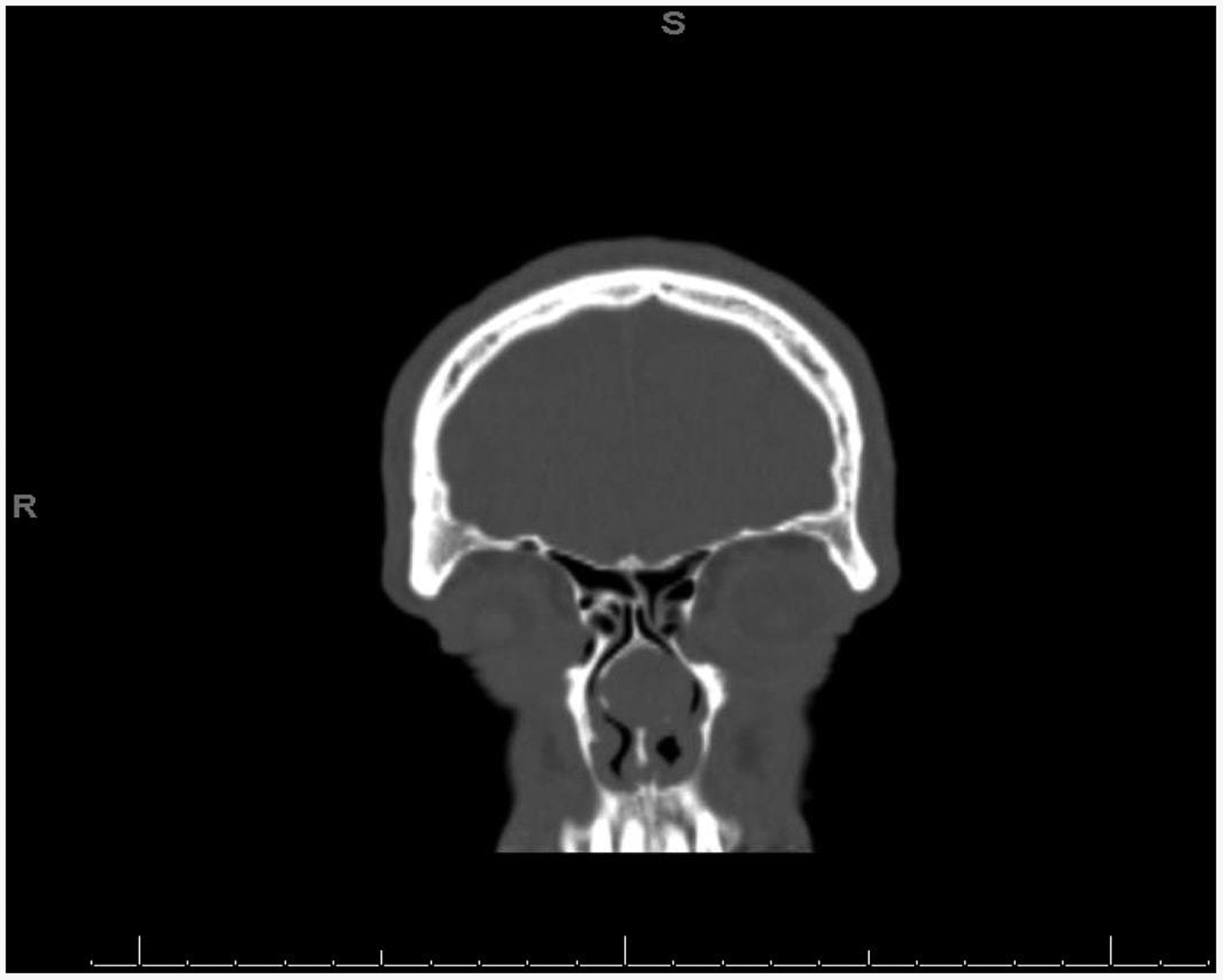
CT sinus fusion protocol, coronal view. Note that mass does not communicate with skull base.

Endoscopic view per right-sided septal incision into the mucocele. Note that mucoperichondrial flap is on the far right and mucocele mucosa is being removed. The opposite mucocele lining is on the left.

Endoscopic view per right-sided septal incision into the mucocele. Note that mucoperichondrial flap is on the far right. Fractured dystrophic bone is on the left and is being removed with Blakesley forceps.
Discussion
Mucoceles are thought to result from the blockage of sinus ostia with either scar band after trauma or possibly due to blockage of minor salivary gland ducts within the mucosa.1,2 Previous nasal surgery, facial trauma, recurrent infections, pneumatized nasal septa, and allergies have all been linked as etiological factors to mucocele development within the paranasal sinuses. 4 They are expansile and locally induce bony remodeling and can destroy surrounding structures. They are most commonly found in the frontal sinuses (60%–65%). Ethmoid mucoceles make up 20%–30% of cases followed by maxillary mucoceles at 10%. Sphenoid mucoceles are rarer and make up 2%–3% of cases.1–4 They sometimes occur as a complication of the use of a nasal septal flap for closure of skull base defects.8,9 Mucoceles have been described in the nasolacrimal duct, intersinus cells, pterygomaxillary space, orbital floor, root of the nose, and within a concha bullosa.2,3,7 Symptom development relates to the location of the mucocele and the degree of bony remodeling by the mucocele matrix as it expands stimulating local cytokine release. Occasionally, mucoceles may become disfiguring, especially if they are located in the periorbital region.1,4
While paranasal sinus mucoceles are more common, nasal septal mucoceles are rarely reported in the literature. Only 10 cases have been reported based on a thorough literature search using PubMed and Ovid. The reported patients are typically male presenting usually in their middle years. One case reported on septal mucocele in a 52-year-old woman with no history of nasal trauma or surgery. 11 The oldest patient was 62 years old, and the youngest was 13 years old. Our patient, a 57-year-old man fits this clinical picture. Several hypotheses have been presented to explain the generation of septal mucoceles ranging from involution of nasal mucosa into the septum during surgery, as a result of a traumatic event or as a result of obstruction of a pneumatized perpendicular plate. 6 One septal mucocele presented as an infected highly destructive mucopyocele with destruction of nearby sinuses and lateral nasal wall. 4 Three of the 10 cases noted the involvement of the perpendicular plate. Four of the 10 cases noted a history of nasal trauma. Six of the 10 cases reported a history of nasal surgery. To our knowledge, this is the first reported case of septal mucocele arising as a complication to open septorhinoplasty 35 years postoperatively.
Differential diagnoses for septal mucoceles include meningocele, encephalocele, neurofibroma, angiofibroma, lymphoma, inverted papilloma, adenoid cystic carcinoma, plasmacytoma, dermoid cyst, intraseptal abscess, and nasal foreign body.1,2,4 CT can help define calcifications, cartilage involvement, and degree of extension and bony destruction. Classically on CT, mucoceles are smooth, fluid-filled, rounded structures with well-defined borders causing bony remodeling.1,2,4 One author advocated for the use of cone beam CT over multidetector CT given the ability of cone beam computed tomography to produce images with superior resolution compared to conventional CT. 1 Halawani and Banjar echoed this opinion and recommended high-resolution CT as the preferred initial diagnostic modality. Magnetic resonance imaging with contrast helps to define lesion margins and neural involvement, and it is necessary to rule out intracranial extension and dural involvement along with other similar appearing lesions such as meningocele, rhabdomyosarcoma, hemangioma, and neuroblastoma.1,3
Histopathologically, these cysts are filled with mucoid fluid and lined by a pseudostratified ciliated columnar or cuboidal epithelium with cellular infiltrates comprising neutrophils, lymphocytes, plasma cells, and eosinophils.3,4 Occasionally, woven and lamellar bone may be found. 3
Treatment consists of surgical excision with either complete removal of the cyst or partial excision. Both external and endoscopic approaches have been used, and recurrence rates are low. Endoscopic marsupialization or excision of septal mucoceles has gained recent popularity due to its low risk of complications, low mortality, ease of use, and excellent visualization. 11 Many authors consider it to be the gold-standard treatment for paranasal sinus mucoceles.10,11 Har-El et al. performed a retrospective review of 108 paranasal sinus mucoceles treated with endoscopic marsupialization with 1 case of recurrence of a frontal sinus mucocele (0.9%). To our knowledge, there have been no previous reports of recurrence of septal mucocele after endoscopic marsupialization or total excision. In our case, the patient’s chief complaint was nasal obstruction. Given the bony remodeling within the mucocele wall, simple marsupialization would not have relieved this. Surgical complications include need for revision, postoperative hemorrhage, septal hematoma, vascular injury, septal perforation, mucosal tears, anosmia, and skull base injury causing cerebrospinal fluid leak. 12 Still, complication rates remain low for endoscopic repair, and we agree that it should be regarded as the treatment of choice for nasal septal mucoceles.
Footnotes
Acknowledgments
The authors acknowledge Triological Society for accepting our project for poster presentation at the 2018 Combined Otolaryngology Spring Meetings, Washington, DC, April 18–22, 2018.
Ethical Approval
IRB approval was waived by our institutional committee.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Department of Otolaryngology at the University of Texas Medical Branch in Galveston, TX.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.