
Abstract
Background
Pediatric patients presenting with a nasal mass is uncommon and a high index of suspicion for it to be a meningoencephalocele is essential. Majority of these are congenital and require early intervention owing to the risk of meningitis. Surgery in these cases is very challenging because of the risk of anesthesia and limited space.
Objective
This study aimed to describe our technique and experience in managing pediatric meningoencephaloceles.
Methods
A retrospective study of 19 pediatric patients (age ranging from 40-day-old infants to 11.5-year-old children) was conducted at our tertiary care center from January 2012 to February 2017. Patients presenting with an intranasal meningoencephalocele were treated by endoscopic approach, using otological microinstruments. After detailed imaging and clinical evaluation, a tailored repair, using fat/fascia/cartilage, a multilayer closure, was carried out in all cases.
Results
All patients had a successful repair and recovery, except for one death following an episode of convulsion. There was a minor circumferential narrowing of the nasal vestibule and synechia formation in 2 of our cases.
Conclusion
Transnasal endoscopic repair of meningoencephalocele is minimally invasive. It avoids permanent anosmia and is cosmetic. A combination of miniaturized instruments and a 4-mm 0° nasal endoscope gives excellent visual field and an adequate working space. Owing to the larger defects in congenital meningoencephaloceles, a multilayer repair provides excellent outcomes.
Keywords
Introduction
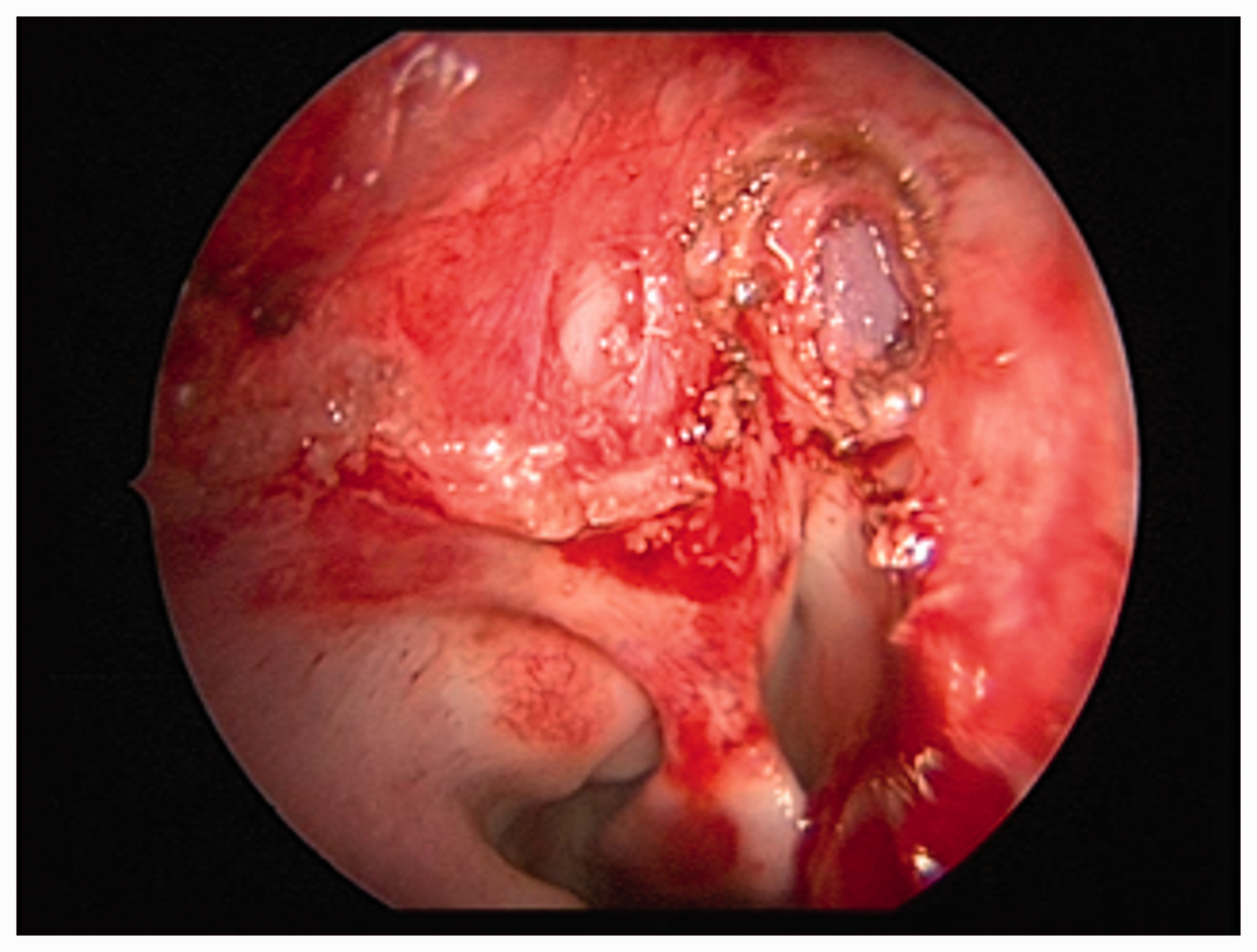
Congenital meningoencephaloceles (MEC) are rare, occurring in 1 of 3000–5000 live births, and of these, 1 of 10 present in the nose. 1 Congenital lesions tend to arise from a defect in the developing anterior neuropore in the region of foramen cecum. Majority of these nasal mass lesions are present medial to the middle turbinate (Figure 1); however, one can encounter a MEC lateral to the middle turbinate too. Occasionally, they may present as an external swelling or a nasal mass with fullness, and these cases may require a combined approach with neurosurgeons.

Right-sided congenital MEC in a 2-year-old child, medial to middle turbinate.
Transcranial approaches were traditionally used for the management of MEC, but following the first report by Wigand in 1981, 2 the endonasal endoscopic approach for skull base repair has evolved tremendously. Using the combination of otological microinstruments and the routine 4-mm 0° nasal endoscope, we have described our technique of repair.
Methods
The retrospective study was approved by the institutional review board of King Edward Memorial hospital and Seth Gordhandas Sunderdas Medical College. It included 19 patients, in the age-group of 40-day-old infants to 11.5-year-old children, presenting with intranasal MEC. All the cases were treated by an endonasal, endoscopic approach, with a multilayer closure of the defect at our center over a period of 5 years. The follow-up period ranged from a minimum of 6 months to 2 years.
Patient Evaluation
A detailed history and clinical examination with specific pediatric evaluation to rule out any associated malformations was done for all our patients. An attempt to examine the nose with an otoscope was made in our outpatient department.
Imaging of brain and paranasal sinuses by a computed tomography (CT) (Figure 2) and magnetic resonance imaging (MRI) (Figure 3) was done. MRI was not done only in one case where it was not possible to sedate the patient due to airway obstruction. The scans helped us to localize the defect in the skull base, to decide the surgical exposure necessary, and to rule out any associated pathologies. The defect size was measured by imaging and graded as follows: 1—small: 2 to 10 mm; 2—medium: 11 to 20 mm; 3—large: more than 20 mm (as per the largest length in a single dimension).

CT of the paranasal sinuses with brain showing a right-sided MEC.
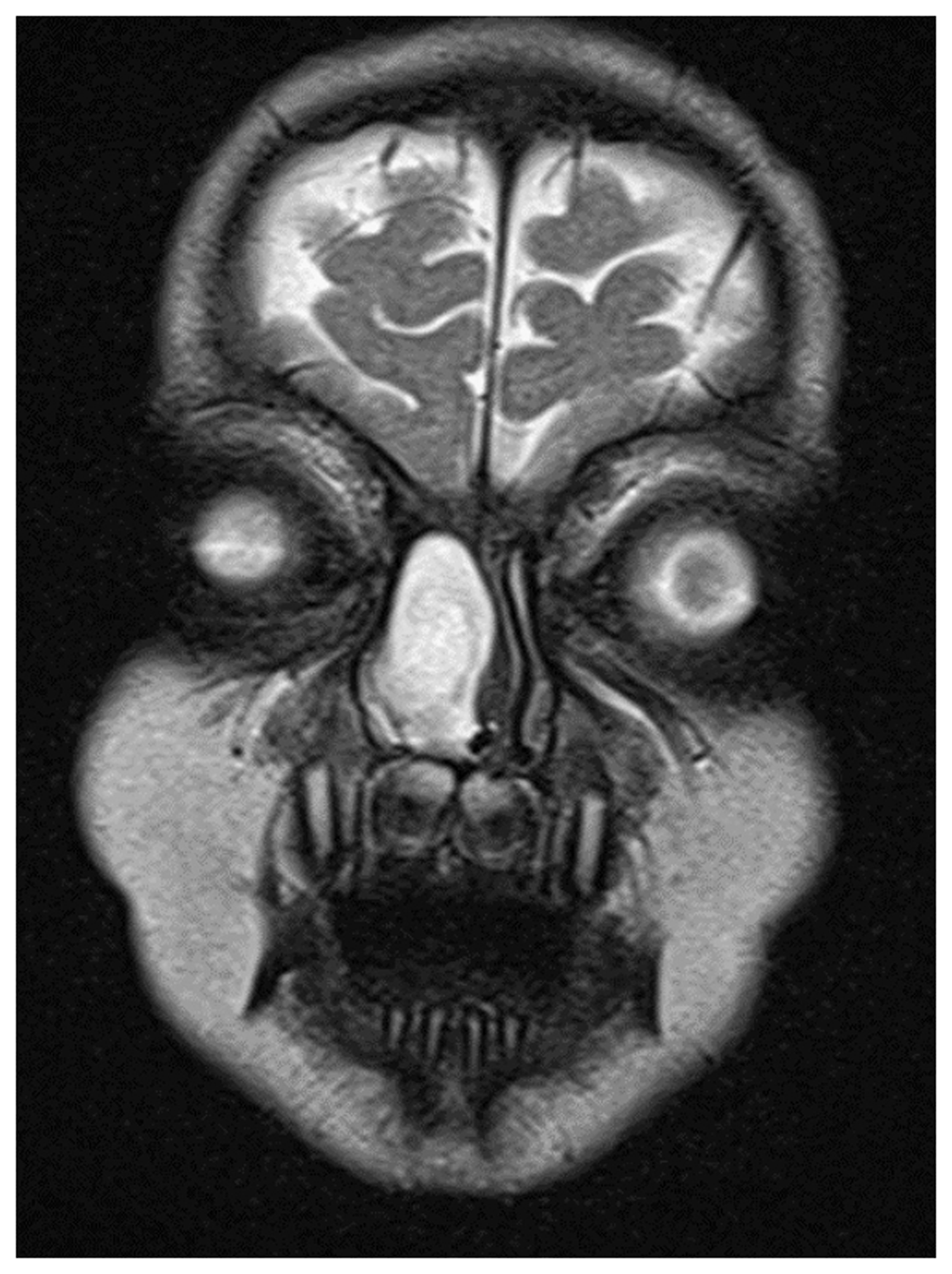
T2-weighted MRI showing a right-sided MEC in a 2-year-old child.
Following a fitness for general anesthesia and consent of the child’s guardian, an endoscopic repair was planned. The children were placed under an antibiotic cover 1 day prior to surgery.
Surgical Procedure
The repair was carried out under general anesthesia. The nasal cavity was adequately decongested using adrenaline-soaked patties. The goal was to gradually release the nasal mass from all its attachments and reach its neck at the skull base with minimal mucosal trauma and blood loss.
After decongestion and local infiltration, an insulated ball point cautery and a microscissor were used to release the mucosal adhesions of the MEC to lateral nasal wall and nasal septum. The mass was dissected all around and reduced using bipolar cautery with precision. Once the bony defect was delineated, the surrounding mucosa was made raw. The repair was then customized based on the size of the defect and the intraoperative scenario. A detailed patient-wise description of the repair in our series is shown in Table 1.
Details of Patients of MECs in Our Series.
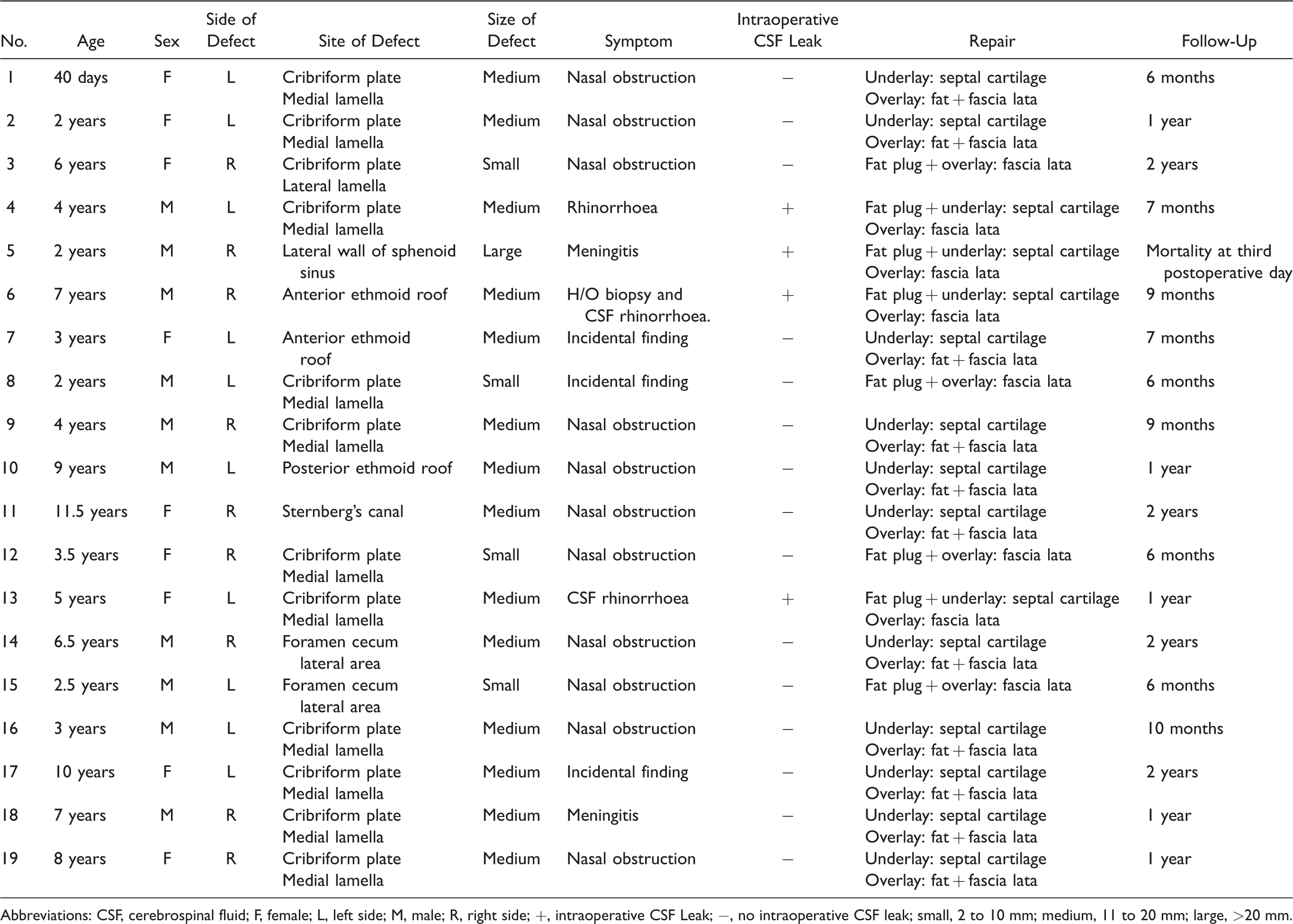
Abbreviations: CSF, cerebrospinal fluid; F, female; L, left side; M, male; R, right side; +, intraoperative CSF Leak; −, no intraoperative CSF leak; small, 2 to 10 mm; medium, 11 to 20 mm; large, >20 mm.
We harvested septal cartilage in all our cases except for the one patient, where a conchal cartilage graft was used to reinforce the defect. The fashioned cartilage piece was used to cover the large area of defect (Figure 4). Cross-hatching of the cartilage was done to resolve its elasticity and curvature, for ease of placement. The cartilage was then placed using crocodile forceps. This repair was further reinforced using fascia lata (Figure 5). The fat and fascia lata were harvested from the thigh. In few of the cases, active cerebrospinal fluid (CSF) leak had to be sealed using fat (bath plug technique). 3 Fibrin sealent—TISSEEL (Baxter) was then applied over the repair. The repair was supported by Gelfoam pieces and a Merocel pack. Dissolvable nasastent was used in 4 patients to avoid the need for pack removal.
Septal cartilage used to repair the skull base defect.

Fascia lata graft used to reinforce the repair.
Postoperative Care
The children were given intravenous antibiotics for 5 to 7 days. The nasal pack was removed after 5 days in all cases except for 1 child where he pulled out the nasal pack on the second day.
Laxatives, antitussives, and diuretics (acetazolamide) were administered to avoid elevation in intracranial pressure during the phase of primary healing. Banana and coconut water intake was encouraged. None of our patients needed a lumbar drain.
Following the first 7 days, the patients were followed up at 2 weeks, 1 month, 3 months, 6 months, 1 year, and 2 years. On follow-up, they were examined with an otoscope, as endoscopy was not possible in all children. Imaging was reserved only for patients with history of rhinorrhea, meningitis, or seizures in the postoperative period.
Results
No patients in our series had recurrence of MEC or postoperative CSF leak. The repair site was found to be well mucosalized after 2 months postoperatively.
All of our cases had a successful repair except one; the one death in our series was a case who had the MEC arising from the broad-based defect in the basisphenoid. The intraoperative repair with fat and fascia lata was uneventful, but the patient had an episode of convulsion and expired postoperatively. It is suspected that probably there was an increase in pressure over the respiratory center in the region of the repair site, which could have caused the mortality.
One of our cases had circumferential narrowing of the vestibule and the other had synechia formation, but these patients were asymptomatic and did not need further management. None of the children had any complaints regarding anosmia in our series.
Discussion
On the basis of their location, MECs are classified as occipital, cranial vault, fronto-ethmoid or sincipital, and basal MECs. Frontoethmoid and basal are together known as anterior MEC. Basal MECs are further subdivided into transethmoidal, transsphenoidal, sphenoethmoidal, and frontoethmoidal. 4 Majority of the children in our series had a frontoethmoid type of MEC.
MEC is an incidental finding in many cases, while others may have varied presentations. It may present as nasal mass with obstruction or even as an external facial deformity. Less often, the MEC may cause significant breathing and feeding difficulties, failure to thrive, especially in infantile cases. The 40-day-old infant in our series presented with these issues (Figure 6). He was on an orogastric tube for feeding and needed urgent intervention. Infantile MEC repair at this age has not been reported as per our literature search. Sometimes there may be a significant delay in presentation, which may be in the form of meningitis. 5

A, A 40-day-old infant with congenital MEC presenting as a right-sided nasal mass with the orogastric tube. B, CT scan of the infant showing the MEC. C, The excised specimen of the MEC.
As the age advance, the MEC may increase in size due to constant pulsation of brain. It can affect the facial growth and may present as an external deformity. To minimize these effects on the developing craniofacial skeleton, we prefer an endoscopic approach in pediatric patients.
The endoscopic approach unlike external approaches is a procedure without the need for cerebral retraction, and the patients have a faster recovery. Recurrence and anosmia are frequent with transcranial repair, 6 which is not so in the endoscopic technique. Similar experience of reduced morbidity and hospitalization in patients undergoing endoscopic repair has been reported. 7
Imaging in the form of CT and MRI is an useful road map for endoscopic surgery. If MRI is not possible, atleast a CT should be done before the surgery. We have not used fluorescein dye in any of our cases to locate the skull base defect. There are chances of allergy to fluorescein, convulsion, and increased risk of infection. In some cases, the angled endoscope was used for adequate visualization of the skull base.
Surgery is the treatment of choice for all MECs. We recommend that these procedures should be attempted with neurosurgeons and preferably in tertiary care centers. These surgeries are challenging because of the risk of anesthesia, hypothermia, hypovolemia, and hypotension. The working space for an endoscopic approach is extremely limited in pediatric patients.
Congenital pediatric MEC tends to have a relatively larger defect compared to those with traumatic or other etiologies in adults. Hence, we have preferred to use multilayer closure in all our cases.
There have been reports of surgical management of pediatric MEC using powered instruments, 8 but we advise strong caution while using this. Even if used, they must be strictly restricted to debride the lower parts of the MEC only. There is a risk of injury to the intracranial vasculature if used near the skull base. Often the strong suction may cause the lateral wall to collapse during the surgery.
Due to the lack of space, many surgeons use a (2.7 mm) pediatric endoscope, but we feel that this compromises the visual field, which is essential for delineating the site of leak. The use of otological microinstruments with a 4-mm nasal endoscope as described above is advisable. We have also reported the use of these minaturized instruments in our technique of pediatric dacrocystorhinostomy surgery. 9
Various materials such as fat, fascia lata, and cartilage are used for repair of the defect. Although we have used a multilayer repair technique, certain smaller defects can be managed by single-layer repair. We could harvest septal cartilage in most of our cases, except one case where conchal cartilage was used. Synthetic material such as polydioxanone plates for skull base repair has been described, and these materials avoid donor-site morbidity. 10
Nasal packing was done after repair in all cases to provide a tamponade and keep the assembly in place till mucosal healing. We used Merocel in most of our cases and nasastent only in 4 patients. Various dissolvable nasal packing materials such as nasastent can be preferred in children as they do not require removal. One of our patients removed the nasal pack on the second postoperative day, but fortunately, there was no complication. Padding of hands must be done to prevent such incidences.
Conclusion
Transnasal endoscopic repair of anterior skull base meningoencephalocele is a favorable technique in most cases. High index of suspicion is required to diagnose these cases. Meticulous tailored repair using multilayer closure gives excellent results. Working in a narrow space in pediatric patients is challenging, and it definitely has a learning curve.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the institutional review board of King Edward Memorial Hospital.
Statement of Human and Animal Rights
This study was performed in compliance with the Declaration of Helsinki.
Statement of Informed Consent
A full informed consent was obtained from all the participants.