
Abstract
Introduction
A 79-year-old woman with macular degeneration was referred to the Allergy/Immunology clinic for the evaluation of a potential allergy to anti-vascular endothelial growth factor (anti-VEGF) treatments. The patient developed urticaria and eyelid swelling immediately following a retinal injection of aflibercept, which she had previously tolerated. She previously had allergic reactions following ranibizumab and bevacizumab injections. Injections of anti-VEGF treatments were discontinued given concern for allergy with progression of the patient’s disease.
Objective
To assess the culprit medication(s) responsible for hypersensitivity reactions following anti-VEGF injections for macular degeneration.
Methods
Medication records were reviewed for each retinal injection. All medications used in each procedure, including the anti-VEGF therapy (aflibercept), topical anesthetics (tetracaine and proparacaine hydrochloride), and antiseptic (povidine), were evaluated with skin testing. She was additionally tested for alternative anti-VEGF therapies (ranibizumab and bevacizumab) as she was thought to have allergies to these agents by prior history. A test dose challenge was completed for aflibercept, ranibizumab, and bevacizumab.
Results
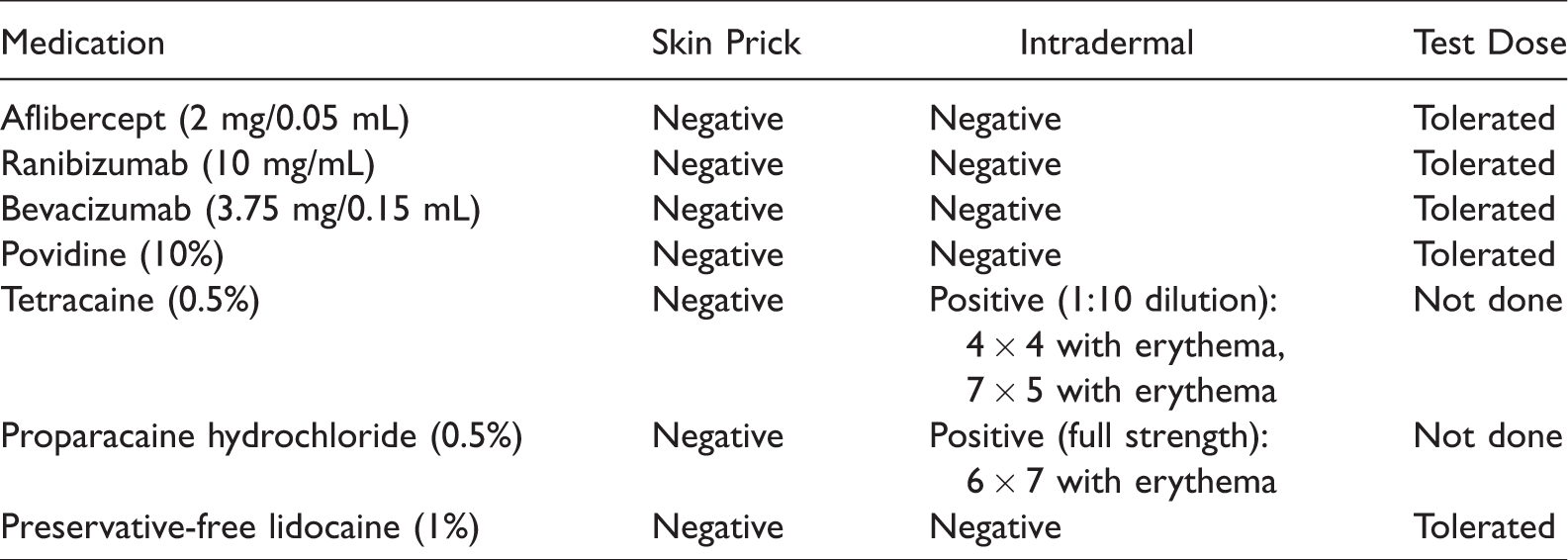
Skin prick and intradermal testing were negative to aflibercept, ranibizumab, bevacizumab, and povidine. Intradermal testing was positive to tetracaine and proparacaine hydrochloride. The patient passed test dose challenges to aflibercept, ranibizumab, and bevacizumab. Due to her positive hypersensitivity testing to 2 ester anesthetics, the patient underwent skin prick and intradermal testing to the amide anesthetic, lidocaine. This was negative and the patient tolerated a graded challenge to lidocaine. She was deemed to have an immunoglobulin E (IgE)-mediated hypersensitivity to ester-type local anesthetics. She successfully resumed anti-VEGF therapy with an amide local anesthetic.
Conclusions
The reason for this consult was the concern for hypersensitivity to a biologic anti-VEGF medication. The culprit allergen, the local anesthetic, could have been overlooked without an assessment of all medications used during the procedure. This case highlights the importance of a thorough allergy evaluation of all medications used during procedures to determine the causative agent.
Keywords
History of Present Illness
A 79-year-old woman with macular degeneration was urgently referred to the Allergy/Immunology clinic from ophthalmology for the evaluation of recurrent allergic reactions following injections of anti-vascular endothelial growth factor (anti-VEGF) treatments for macular degeneration. The patient developed angioedema and an erythematous, pruritic rash approximately 4 hr following a retinal injection with the anti-VEGF treatment aflibercept (Eylea®). She had previously tolerated ophthalmic injections of aflibercept at least 4 times previously. She reported bilateral eyelid, cheek, chin, and lip swelling. The patient denied tongue swelling, throat closure, shortness of breath, and lightheadedness. The red, raised pruritic rash appeared to the patient to be “whelps.” She took diphenhydramine but noted that the “whelps” stayed in the same place for approximately 1 week. When they resolved, her skin was flaky, and she described the area as if she had sunburn. There was no recurrence of the rash after the 1 week. Four years prior, the patient had reported a similar rash with retinal injections of other anti-VEGF treatments, bevacizumab (Avastin®) and ranibizumab (Lucentis®). She had been evaluated by dermatology at that time. Her skin biopsy demonstrated an interface dermatitis concerning for a drug hypersensitivity reaction thought to be secondary to the anti-VEGF therapies. Given her recent reaction of swelling and rash after injection with aflibercept, treatments were discontinued by ophthalmology with subsequent progression of the patient’s macular degeneration.
Given the severity of the patient’s macular degeneration and high likelihood of blindness without treatment, the patient was referred for urgent evaluation to determine whether she had an allergy to anti-VEGF therapies, including the most recently used medication, aflibercept, as well as previously used bevacizumab and ranibizumab, in an attempt to find a medication that could be used to preserve her eyesight.
Physical Examination
At the time of consultation, the physical examination was unremarkable. She was without urticaria or angioedema.
Laboratory and Other Diagnostic Findings
Procedure and medication records for each retinal injection procedure were reviewed. All medications used in the procedure, including the anti-VEGF therapy (aflibercept), topical anesthetics (tetracaine and proparacaine hydrochloride), and antiseptic (povidine) were evaluated via skin prick test and intradermal testing. She was additionally tested for the 2 other anti-VEGF therapies (ranibizumab and bevacizumab). For skin prick testing, aflibercept, bevacizumab, ranibizumab, tetracaine, and proparacaine hydrochloride were assayed at a 1:10 dilution and full strength. Full strength povidine was used for the skin prick testing. Intradermal testing for aflibercept, bevacizumab, ranibizumab, and povidine was completed at the following concentrations: 1:1000 dilution, 1:100 dilution, and 1:10 dilution. For tetracaine and proparacaine hydrochloride, intradermal testing was assayed at the following concentrations: 1:1000 dilution, 1:100 dilution, 1:10 dilution, and full strength. Skin prick and intradermal testing were assessed after 15 min. A test dose, consisting of a full therapeutic dose, was given if the skin testing was negative for aflibercept, ranibizumab, and bevacizumab. Allergy evaluation results are included in Table 1.
Results of Skin Prick and Intradermal Testing and Test Dose Medications Considered as Potential Causes for the Drug Hypersensitivity Reaction.
Differential Diagnosis
The patient was referred specifically to determine whether she had an allergy to anti-VEGF medications. Although this concern was considered in the differential, it is imperative that all medications used in a procedure be included in the evaluation of a postprocedural allergic reaction as the culprit medication may be a secondary drug used. The differential diagnoses considered for this patient included immunoglobulin E (IgE)-mediated hypersensitivity to anti-VEGF medications, local anesthetics, and antiseptics; adverse reaction to local anesthetics or preservatives; contact dermatitis (delayed type IV hypersensitivity reaction) to anti-VEGF medications, local anesthetics, and antiseptics; and chronic idiopathic urticaria with angioedema. Skin testing (prick and intradermal) and administration of test doses are necessary for the evaluation of medication type I immediate hypersensitivity reactions. The patient’s history of rash (“whelps”) and swelling after medication exposure support a type I hypersensitivity reaction although the timeframe to the development of rash is delayed for a typical type I hypersensitivity reaction. Contact dermatitis was considered given the delayed appearance of the rash with some features of a sunburned appearance and dryness; however, the reported “whelps” are not characteristic of contact dermatitis. The patient’s history did not support chronic idiopathic urticaria with angioedema.
Conclusion
The patient’s skin prick and intradermal testing with appropriate controls were negative to aflibercept, ranibizumab, bevacizumab, and povidine. Intradermal testing was positive to tetracaine and proparacaine hydrochloride. The patient tolerated test dose challenges to aflibercept, ranibizumab, and bevacizumab. The patient underwent skin prick and intradermal testing to the amide anesthetic, preservative-free lidocaine at a subsequent appointment. Lidocaine was chosen as it was the only amide anesthetic available in a topical ophthalmic preparation. Skin testing was negative, and the patient tolerated a subsequent graded challenge to preservative-free lidocaine (0.1 cc of 1:10 dilution, 0.1 cc of full strength, 0.5 cc of full strength, and 1.0 cc of full strength).
Final Diagnosis
Based on the allergy evaluation, the patient was diagnosed with IgE-mediated type 1 hypersensitivity to ester-type local anesthetics. She successfully resumed and continues to receive anti-VEGF therapy with aflibercept and an amide local anesthetic for the treatment of macular degeneration. The patient’s immediate reaction on skin prick testing confirmed an allergy to ester-type local anesthetics. Patch testing was not performed to assess for a type IV hypersensitivity reaction. In retrospect, this would have been useful to validate or exclude contact dermatitis as a contributor to her rash.
Discussion
The use of biologics to treat a variety of disease has entered the arena of all fields of medicine. This patient was referred for concern that her allergic reaction was secondary to a biologic used to treat macular degeneration. Hypersensitivity reactions to these medications are rare events but important to consider. One notable case report for hypersensitivity to anti-VEGF agents described a patient who developed dyspnea, dysphagia, and throat swelling after intravitreal injection with bevacizumab and then throat tightness and coughing with subsequent challenge to ranibizumab. 1 The patient’s IgE-mediated hypersensitivity to anti-VEGF agents was confirmed with positive allergy testing to bevacizumab and ranibizumab. 1 Aflibercept was tolerated in this patient. This was thought to be secondary to the “fully human” origin of aflibercept compared to humanized monoclonal antibodies, bevacizumab, and ranibizumab. 1 Nagai et al. report a case of a patient who developed a maculopapular rash 10 hr after injection with aflibercept and was presumed to have a type IV hypersensitivity reaction to this biologic. 2 In addition, a case report detailed a series of patients who were found to have type IV hypersensitivity reactions after intravitreal injections; however, these reactions were most commonly found to be secondary to phenylephrine used during the procedures and not the anti-VEGF medications. 3 A practicing allergist needs to remain aware of hypersensitivity reactions to biologics but also consider other medications used in each procedure so as to not overlook other possible culprits.
This patient’s history and allergy evaluation results support a diagnosis of an IgE-mediated type 1 allergy to ester-type local anesthetics. IgE-mediated hypersensitivity to local anesthetics is rare.4–6 A recent literature review by Bhole et al. reviewing 23 case series noted that 29 of the total 2978 patients had true IgE-mediated allergy to local anesthetics, which corresponds with a <1% prevalence of local anesthetic allergy.6–8 A retrospective observational study of patients seen at hospital clinics in France for immediate hypersensitivity reactions also found local anesthetic allergy to be rare with a local anesthetic as the causal agent for a reaction in only 0.4% of patients studied. 9 In addition, the literature notes that the majority of adverse reactions to local anesthetics are secondary to nonallergic factors, including anxiety, vasovagal reactions, or toxic reactions.4,5 Toxic reactions from local anesthetics occur when an excess of the medication is given which adversely affects both the cardiovascular and central nervous systems. 10 Toxic concentrations can lead to adverse reactions such as tremors, seizures, bradycardia, and vasodilation with the potential for cardiac arrest. 10 It is, therefore, important to consider both adverse and toxic reactions when evaluating a patient for local anesthetic allergy. Delayed type IV hypersensitivity reactions such as eczema are common and should also be considered. 5 A study by Warshaw et al. sought to determine the frequency and pattern of positive allergy patch-test reactions to topical anesthetics and found that of the 344 patients patch tested 3.4% had an allergic reaction to at least one anesthetic. 11 This study additionally found that the most common culprits for positive testing included benzocaine (50%), dibucaine (27.9%), lidocaine (19.2%), tetracaine (11.1%), and prilocaine (2.3%). Moreover, 79% of patients reacted to both an amide and ester anesthetic, but there was little cross-reactivity based on the structure of the medication. 11
While local anesthetic allergy is rare, the use of local anesthetics is common in ophthalmology, dentistry, obstetrics, and for minor procedures and surgeries. 7 These medications are vital as they allow for procedures to be completed in a manner that is both comfortable and safe for patients. Local anesthetics typically used are of either the amide or the ester group. The common anesthetic agents used clinically in the amide group include lidocaine, prilocaine, mepivacaine, bupivacaine, ropivacaine, and articaine, while the ester group contains proparacaine, chloroprocaine, procaine, and tetracaine.5,12 The ester group of anesthetics break down to para-aminobenzoic acid, which is known to be allergenic and therefore a portion of patients listed with ester anesthetic allergy potentially are allergic to this by product.7,10,13 Dr Gaul reported 2 cases of patients who were found to be positive on patch testing to p-aminobenzoic acid and local anesthetic agents. 13 One limitation of this report is that the cross-reactivity was based on patch testing and not IgE-mediated skin prick testing. Of note, the ester anesthetics can cross-react with others in the same group but do not tend to cross-react with amide anesthetics.7,8,13
Case reports have illustrated the variability in cross-reactivity among amide anesthetics. A 39-year-old man developed an immediate type I hypersensitivity reaction characterized by urticaria and angioedema after the administration of mepivacaine. He was later found to have strong positive skin test (both prick and intradermal) results to mepivacaine, lidocaine, and ropivacaine, all of which are amide anesthetics. 14 In another case, a 35-year-old woman developed hives and pruritus after mepivacaine administration. She notably had positive skin tests to mepivacaine and ropivacaine but tolerated lidocaine and bupivacaine. 15 These 2 cases illustrate the variability in cross-reactivity among amide anesthetics; therefore, testing for different medications within the amide group can be useful.
When amide anesthetics were introduced, there was a notable decrease in allergic reactions and currently most local anesthesia uses amides. 7 However, the amide anesthetics that are contained in multiuse vials contain the preservative methylparaben which has a similar structure to para-aminobenzoic acid and can be responsible for allergic reactions. 10 Patients who are allergic to ester local anesthetics can typically tolerate preservative-free amide local anesthetics, and therefore, if a patient is found to have a true hypersensitivity reaction to ester anesthetics, they should be assessed for the use of a preservative-free local amide anesthetic instead. 10
This patient successfully resumed anti-VEGF therapy with aflibercept and an amide local anesthetic for her macular degeneration. It is important for patients to receive a complete allergy evaluation after an allergic reaction following a procedure that includes multiple medications to determine which medication is responsible for the reaction. This case highlights the importance of a thorough allergy evaluation of all medications used during procedures to determine the causative agent of a reaction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the following NIH Grant number T-32 5T32-AI007062-39 (to RSK).
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.