
Abstract
Introduction
Hip hemiarthroplasty is commonly performed for displaced femoral neck fractures in older adults, with implants placed either cemented or uncemented. While cemented fixation offers immediate stability, uncemented fixation reduces operative time and pulmonary complications. Large single-center analyses comparing these techniques remain limited, and this study aims to assess this.
Methods
We conducted a retrospective case-control study of 634 adult patients undergoing hip hemiarthroplasty at a single Level 1 trauma center from 2019 to 2025. Patients were classified by cemented (n=403) or uncemented (n=231) fixation and further stratified by surgical approach (anterolateral vs posterior). Outcomes included length of stay, postoperative complications, return to baseline mobility (Koval score), discharge destination, and postoperative mortality within 1 year. Statistical analyses were conducted to evaluate predictive factors with independent-samples t-tests, Mann-Whitney U tests, Chi-square tests, and logistic regression utilized where appropriate.
Results
Baseline demographics and preoperative mobility were similar between cohorts. Cemented hips with anterolateral approaches had the lowest rates of dislocation (1.3%, p=0.036) and revision surgery (1.7%, p=0.024), but this did not remain significant after statistical correction (p=0.228, p=156). Functional recovery was comparable across groups. Cemented fixation independently predicted discharge home (OR 2.17, p=0.002). There were no significant differences in length of stay, postoperative pain, periprosthetic fracture, infection, readmission, or mortality within 1 year.
Conclusions
In this large single-center cohort, cemented hip hemiarthroplasty, particularly with an anterolateral approach, was associated with reduced dislocation and revision rates and increased likelihood of discharge home. These findings support consideration of cemented fixation with an anterolateral approach in appropriately selected patients to optimize postoperative outcomes and quality of life. Further multicenter prospective studies are warranted to confirm these results and refine surgical decision-making for femoral neck fractures.
Introduction
Hip hemiarthroplasty is commonly used to treat displaced fractures of the femoral neck in older patients with lower functional demands or significant comorbidities.1-3 This approach reduces reoperation rates compared to open reduction internal fixation (ORIF). The literature reports reoperation rates of 7–14% for hemiarthroplasty versus 39–44% for ORIF.4-6 In this procedure, the prosthesis can either be cemented in place or inserted uncemented depending on surgeon discretion. In a cemented hemiarthroplasty, strong support is established immediately and has been linked to early mobility, reduced pain, and lower incidence of periprosthetic fracture.7-11 In an uncemented hemiarthroplasty, the implant is designed to fit tightly into the bone, and over time, allow for bony ingrowth and durable femoral fixation. This method reduces surgical duration by approximately 7–8 minutes on average and has been associated with a decreased incidence of pulmonary embolism and other cement related complications.12-14 However, this method has been linked to higher incidence of periprosthetic fracture and revision surgery.8,9,15-17 Therefore, careful consideration on a case-by-case basis is required to determine which method would be best for a particular patient.
Comparisons between these two methods has been the topic of many large cohort studies, but many have been multicenter studies or analyses of entire health systems.8,9,15 While these methods grant robust sample sizes, the inclusion of various sites comes with an inherent loss of granularity. Therefore, a large single site comparison between cemented and uncemented hip hemiarthroplasty for femoral neck fractures would be a meaningful addition to the current base of knowledge. Currently, large single center studies tend to handle cohorts under 500 patients.18-21 With this analysis, we hope to analyze the effects of hip hemiarthroplasty cementation on patient outcomes using a sample that exceeds this count. This study aims to compare the functional and quality of life outcomes between cemented and uncemented hemiarthroplasty and to determine if cementation is a predictive factor for post-operative complications and discharge destination. This study also includes a subgroup analysis of surgical approach to determine the optimal approach and fixation combination. We hypothesize that cemented fixation with an anterolateral approach will best reduce complications. We intend findings to help guide pre-operative planning and post-operative care for these patients.
Materials and Methods
Study Design and Patient Population
A case-control retrospective review was conducted in adult patients diagnosed with a femoral neck fracture. Included patients underwent hip hemiarthroplasty at a single Level 1, tertiary referral trauma center between January 1, 2019 and July 20, 2025. Institutional Review Board approval was obtained, and patients were identified in the institution’s trauma database using CPT codes (CPT 27236) and secondarily verified with direct chart review and radiographic verification. Exclusion criteria included patients younger than 18 years of age and those that underwent open reduction internal fixation (ORIF), total hip arthroplasty, or proximal femur replacement. The total cohort included 634 patients who underwent hip hemiarthroplasty for treatment of their femoral neck fracture.
Collected Variables
Patients were placed into case cohorts based on documentation in the electronic medical record (EMR) of cemented arthroplasty utilizing standard cementation technique or uncemented arthroplasty using triple taper collared stems. Choice of implant was decided by surgeon discretion. Koval scoring has been previously used in studies assessing mobility in older adults, and so each patient was assigned a Koval score to assess both baseline and maximum post-operative mobility. 22 This was determined using either official post-operative outpatient assessments by the primary surgeon or, if available, records from other specialties such as primary care or physical therapy. Other data points such as baseline demographics, primary surgeon, surgical approach, length of stay, post-operative complications, and discharge destination were sourced from the EMR.
Statistical Analysis
Data was analyzed using IBM SPSS Statistics Version 27 (IBM Corp., Armonk, NY). Continuous variables were assessed for normality using the Shapiro-Wilk test. Normally distributed variables were compared between groups using independent-samples t-tests, while non-normally distributed variables were compared using Mann-Whitney U tests. Categorical variables were compared using Chi-square tests to determine difference in descriptive data between cohorts. Logistic regression was used on outcomes that were statistically different between cohorts to quantify the predictive value of a given variable for patient outcomes. For outcomes with multiple pairwise group comparisons, Bonferroni correction was applied. The above process was replicated for sub-analyses of anterolateral and posterior approach surgeries.
Post hoc power analyses were performed for all primary outcomes using the observed effect sizes, sample sizes, and α = 0.05.
Results
Patient Characteristics
Patient Demographics and Surgical Approach
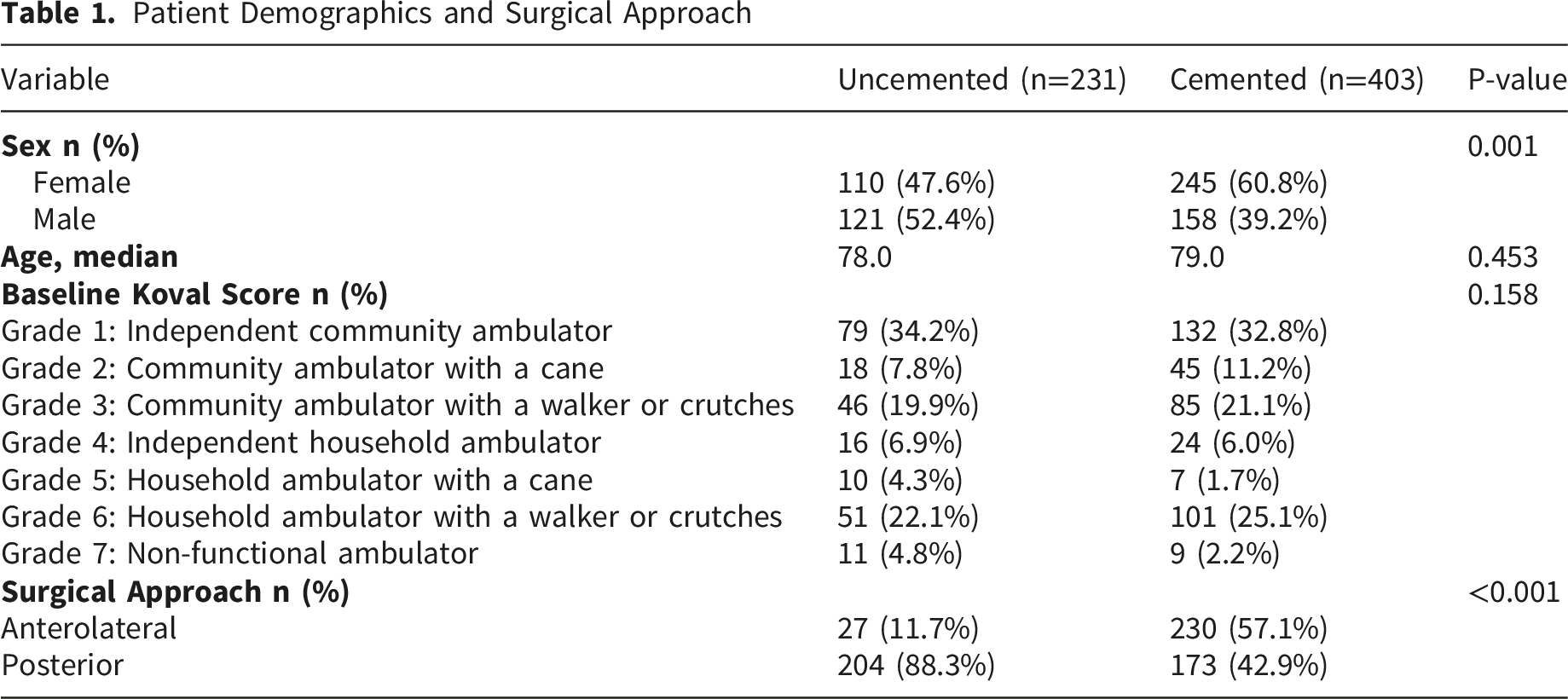
There was a total of 48 individuals identified as primary surgeons. The difference among them regarding cementation choice was statistically significant (p<0.001) with many surgeons demonstrating a clear preference for one arthroplasty method over the other. Of note, arthroplasty fellowship trained surgeons showed a preference for cementation (80.6% of their cases, p=0.29), but since arthroplasty trained surgeons only performed 36 cases (5.7% of the total), this should be interpreted with caution.
Group Comparisons
Overall Outcome Comparisons

For the sub-analyses, length of stay was significantly shorter by about 2 days in the anterolateral cemented hips as opposed to uncemented (p=0.015). Upon logistic regression, anterolateral approach was found to be predictive of shorter hospital stays (p<0.001). There were also proportionally more infections in the anterolateral uncemented sub-group (P = 0.040), but logistic regression found that this association was not significantly predictive (P = 0.056).
As for the posterior approach sub-cohort, there were significantly less revision surgeries in the cemented group (P = 0.04), and cementation was confirmed to be predictive upon linear regression (P = 0.05).
Surgical Approach Sub-Analysis

Logistic Regressions

Discharge Destinations

Discussion
These results show that there are significant post-operative differences between cemented and uncemented hip hemiarthroplasty. For this cohort, cementing had no effect on length of stay, post-operative pain, or the return to previous mobility and the general speed at which it is reached. This indicates that the functional outcomes are similar regardless of cement usage which is consistent with established literature. 9 As for post-operative complications, cemented arthroplasty was 61.5% less likely to dislocate and 69.2% less likely to require a revision. This was, however, likely a function of the surgical approach. When taking this into account, dislocation and need for revision occurred at significantly lower rates in anterolateral cemented hips than any of the other surgery types (Table 2). However, smaller subgroup cohorts limited our confidence in these results after statistical correction. While these findings did not hold up under a higher bar of scrutiny, they display a data trend that possibly sheds light on important considerations for patient care. For older patients, who make up the majority of these injuries, these risk reductions have a great impact on regaining mobility post-operatively, which this study associates with being approximately 73% less likely to die within 1 year after surgery.
As for the complications of surgical site infection and all-cause mortality within 1 year, there was no difference detected between the cohorts. This is consistent with recent literature. Generally, there has been no detectable difference between infection rates, although some studies have found small increases in infection for uncemented patients that is attributed to their increased rate of reoperation.9,11,15 As for 1 year survival, there have been some studies which detect no difference, while some have detected a small survival benefit from cemented arthroplasty.8-10,18 While this survival benefit was not detected in this study, these results add to the discourse on this topic.
Of note, this study failed to detect a difference in post-operative periprosthetic fracture and readmission related to the affected hip. Previous studies have found that uncemented stems have both a significantly higher periprosthetic fracture rate and an associated increased readmission rate to address these injuries.8,9,15 It is unknown exactly why this was not the case in this cohort. It is possible that it may be related to surgeon specific factors, specifically performing uncemented stem fixation in osteoporotic bone, which is quite different than elective total hip population. It was noted that some surgeons in this cohort had a significant preference for or against the usage of cement. Therefore, this institution may have been utilizing uncemented prosthetics in patients that otherwise would have been cemented at the institutions that hosted previous studies. Ultimately, this study population demonstrated a much lower periprosthetic fracture incidence than prior studies with uncemented fixation, which is notable. Typically, uncemented arthroplasty is considered ideal for patients that are more at-risk for specific complications, especially those with cardiorespiratory comorbidities. These patients benefit from the reduced time under anesthesia, reduced chance of PE, and the reduced chance for bone cement implantation syndrome.8,12-14 If patients that are healthier and less injury prone than the average uncemented patient were included in that cohort, then the rate of post-operative fracture would be diluted. Although this cannot be determined with the current data available, it offers an explanation that takes into account the observed surgeon trends. There may also be a degree of limited power in this study to detect a difference in periprosthetic fracture rate. Post-hoc testing revealed an achieved power of 16.5%. While not incredibly low, this may speak to the smaller difference in fracture risk between these cohorts as opposed to those of other studies. Future studies utilizing data from more years at this institution could demonstrate if this is the case.
As for discharge destination, it is unsurprising that a nursing facility is the most popular for each cohort. The incidence rate of femoral neck fractures is markedly higher in nursing home residents with rates up to 8.7–9.4 times greater in long-stay institutions compared to the community at-large. 23 Therefore, a return to the facility from which they presented is predictable. However, cemented hips are shown to be more likely to be discharged home than their uncemented counterparts in this cohort. The reason for this is unclear with the data available, but it may be due to the more rigid fixation giving surgeons more confidence in the patient’s mobility recovery in a home environment. Also, individuals may be sent home because they have strong family support or other avenues of at-home assistance. Returning to recover in one’s home brings much value to a patient as studies have highlighted that long-term healthcare facility stays are associated with a decline in quality-of-life metrics.24,25 As with all surgical intervention, post-operative life quality should be taken into account when determining if a patient should receive a cemented stem.
There are limitations to this study. Firstly, as a retrospective study, there was no control on how the data was collected, and so there was no uniformity in how different physicians document post-operative outcomes. Therefore, many variables such as cement technique and capsular repair were not controlled. Secondly, we noted individual bias for one method over the other. This means that the surgical skill and preferences of a surgeon are mostly represented in one cohort over the other, and it is unclear as to how much of the results of one cohort can be attributed to the particular aspects of its surgeons. It is notable that the cemented cohort was significantly more female than the uncemented cohort, and this may be a confounding factor. The degree of a patient’s osteoporosis may be an influence, but the lack of consistency in documentation for this comorbidity reflects another limitation due to the retrospective nature of the study. The distribution of surgical approach was also highly skewed between fixation populations which likely has a confounding effect. Also, patients with more recent surgeries did not have an entire year of follow-up as of the writing of this manuscript. Therefore, there is some limitation to outcome data in these cases. As a single institutional analysis, there may be unique patient population or institutional factors that impact the results. Future study should address these limitations with a prospective arm that can better control for surgical approach, implant choice, cementation method preferences, and osteoporotic severity as well as expand the observed outcomes with objective analyses of gait and muscle strength recovery.
Conclusion
In this large single-center analysis of 634 patients undergoing hip hemiarthroplasty for femoral neck fracture, cemented fixation was associated with significantly lower rates of postoperative dislocation and revision surgery compared to uncemented fixation and predicted discharge home. The effects of cement fixation on patient outcome appear to be impacted by surgical approach, as it would appear anterolateral approaches correlated with these positive findings of cement fixation. These findings suggest that, in appropriately selected patients, cemented hemiarthroplasty with an anterolateral approach can offer an advantage in reducing complications and facilitating a return to independent living. Given the observed distribution of fixation choice among surgeons, further investigation into method selection patterns, patient comorbidity profiles, and long-term functional outcomes is warranted. Regardless, it is imperative that surgeons always consider the overall health of their patient and their patient’s goals of care before deciding on which method of arthroplasty to use.
Footnotes
Ethical Considerations
This study was reviewed and approved by the local Institutional Review Board (IRB ID #202507192) with waiver of consent. Consent was waived due to the retrospective, deidentified nature of the analysis.
Author Contributions
Dr. Berkes was the primary investigator for this project. Mr. Rust contributed data collection, analysis, and manuscript preparation. Dr. Obey, Dr. Wilson, and Dr. McAndrew contributed to manuscript composition and edits prior to submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Marschall Berkes, MD, received teaching honorarium from AO North America and consulting fees from Smith and Nephew. Christopher McAndrew, MD, received institutional support from Zimmer Biomet and teaching honorarium from AOTrauma North America. The remaining authors have no interests to declare that are relevant to the content of this article.
Data Availability Statement
Protected patient data from Barnes-Jewish Hospital/Washington University School of Medicine was utilized and is thus not publicly available.