
Abstract
Introduction
Hip fractures can be divided into intracapsular(ICF) and extracapsular(ECF) fractures. Preoperative pain management of hip fractures is important and complex. Fascia Iliaca Compartment Block(FICB) is proven effective in reducing pain. The effectiveness may vary depending on the location of the hip fracture, given the complex nerve innervation of the hip joint. To our knowledge, the difference in effect of pre-operative FICB across the various types of hip fractures has not yet been investigated. This study compared pre-operative pain management with FICB in ICF and ECF patients.
Methods
This retrospective, single center cohort study included patients(>50 years) with ICF or ECF and preoperative FICB. Numeric Rating Scale(NRS) scores at 2 time points after FICB were compared, adjusting for baseline NRS, potential confounding by prehospital opioid use and time interval between FICB and NRS-score. Also preoperative opioids use 24 hours after FICB was compared.
Results
183 patients were included; 94 ICF and 89 ECF patients. Both groups had comparable demographics(age and gender) and baseline characteristics, except for pre-injury home opioid use, which was significantly higher in the ECF patient group. NRS score before FICB-administration was 4.610(SD1.634; ICF) and 4.870(SD1.746;ECF P = 0.302) and did not differ between groups. NRS scores decreased significantly after FICB, with no significant difference between the groups: ICF: 2.900(SD1.522) and 2.360(SD1.574) and ECF 2.920(SD1.817;P = 0.834) and 2.960(SD1.938;P = 0.093) for the first and second NRS scores after FICB respectively. There was no confounding or effect modification. Opioid use in the first 24hrs after FICB was not significantly different in both groups.
Conclusion
There was no statistically significant difference in preoperative pain relief provided by FICB in patients with intracapsular or extracapsular hip fractures. The FICB had great value as a regional pain block at the emergency department for both types of frail hip fracture patients.
Keywords
Introduction
Hip Fractures
Hip fractures are common fractures worldwide. 1 They can be classified as either intracapsular (femoral neck) or extracapsular (intertrochanteric, pertrochanteric and subtrochanteric) fractures. 2 Hip fractures are associated with high morbidity and mortality, particularly in elderly and frail patients. 1 Operative treatment is generally recommended for most hip fracture patients. 3 Optimal preoperative pain management is key, as uncontrolled pain from a hip fracture can lead to delirium, increased postoperative complications and reduced quality of life.4,5
Pain Management
Preoperative pain management can be challenging due to preexisting comorbidities, increasingly common polypharmacy and physiological changes from the aging process. 6 Oral or intramuscular/intravenous analgesics (eg, paracetamol, NSAIDs and/or opioids) are generally used in hip fracture patients in the emergency department. These medications, and particularly opioids, have well-known side effects like nausea, confusion and oligoanalgesia which are particularly common in elderly patients.3,7,8
Surgery often has to be postponed due to the use of anticoagulants, comorbidities (eg, malnutrition and anemia), and/or the unavailability of emergency operation rooms.9-11 Pain management with regional anesthesia is an effective treatment for pain relief in patients awaiting surgery. Fascia Iliaca Compartment Block (FICB) and Femoral Nerve block (FN) have been shown to be effective in reducing pain and opioid consumption in patients with hip fracture during the perioperative stage.12-17 Other forms of regional analgesia such as pericapsular nerve blocks (PENG) have been described as alternative pain blocks in hip fracture patients. 2 Previous studies reported that perioperative nerve blocks are more effective than morphine in reducing pain in hip fracture patients.18,19
Nerve Innervation of the Hip
The innervation of the hip joint is complex. The anterior capsule of the hip joint is innervated by the sensory nerve branches of the femoral and obturator nerves. The posterior joint capsule is innervated by the sciatic and superior gluteal nerves, especially by mechanoreceptors.20-22 The overlying structures of the hip joint receive sensory innervation from the lateral femoral cutaneous nerve (LFCN). The femoral nerve and the LFCN are located under the iliac fascia.14,20-23 To date, studies have focused on the effectiveness of pain blocks in reducing pain in patients with hip fractures with all fracture types grouped together. However, because sensory innervation varies at different regions of the hip and nerve blocks target on different neural pathways, the effectiveness of regional nerve blocks may vary between different fracture types, (eg, intra- or extracapsular hip fractures).
Fascia Iliaca Compartment Block (FICB)
The FICB is a regional anesthesia technique that targets the femoral, lateral femoral cutaneous and obturator nerves by injecting local anesthetic beneath the fascia iliaca. This is a safe and effective analgesic technique in the perioperative management of geriatric patients which results in a clinically significant reduction in pain scores.12,24 The FICB is 1 of the most common used pain block at the emergency department for treatment of hip fractures. 24 Integration of FICB into geriatric hip fracture protocols is strongly recommended by the American Academy of Orthopaedic Surgeons (AAOS). 25 The Dutch guidelines also strongly recommend to consider the use of nerve blocks for preoperative pain management. 26 When administering a FICB, a volume of levobupivacaine is deposited underneath the iliac fascia to reach the femoral nerve, the LFCN and obturator nerve. The FICB thereby blocks the nerve innervation in the hip, the anterior and lateral thigh and partially in the knee.27-29 The success of the FICB depends on the technique, volume of local anesthetic and anatomical variability. 30 The FICB has an onset of action of ≤15 min and can be effective for up to 17 h after placement. 30
Recent studies have proven the effectiveness of FICB in perioperative pain management of all hip fracture types.12-17 Studies investigating the effectiveness of a pain block do not differentiate between types and locations of hip fractures (intracapsular vs extracapsular). Given the sensory innervation pathways of the anterior hip joint capsule FICB may be more effective in managing preoperatively pain relief in patients with intracapsular fractures compared to extracapsular fractures. Therefore, the primary aim of this retrospective study was to compare the effect of FICB on pain relief in patients with intracapsular and extracapsular hip fractures, measured by a Numeric Rating Scale (NRS). 31 In addition, the effectiveness of FICB was assessed by the use of preoperative opioids after FICB in both fracture types.
Materials and Methods
Study Design and Study Population
The data of this retrospective, patient cohort study was collected from the medical records of all consecutive hip fracture patients who received a FICB at the Isala Hospital between January 2019 and December 2021. Patients eligible for inclusion were: >50 years old with radiographically confirmed hip fractures, administration of preoperative FICB and the pain score (NRS) available both before and after the FICB. Exclusion criteria included the following: pathological hip fracture, allergy to opioids or local anesthetics, conservative treatment of the hip fracture, other traumatic injury related to the hip fracture and history of surgery on the ipsilateral hip. The exclusion criteria of the FICB as protocolled by the Dutch Association of Emergency Department Doctors (NVSHA) were based on the contraindications. The absolute contraindications were local skin infection and allergies to local anesthetics. Relative contraindications were non-cooperative patient, risk of compartment syndrome, the use of anticoagulant, INR (International Normalized Ratio) > 4.5 and/or conditions associated with reduced coagulation activity. Enrolled patients were divided into 2 groups according to the type of fracture; intracapsular or extracapsular fractures.
The local medical ethical committee approved the study protocol (study number 20220316) and informed consent was waived.
Fascia Iliaca Compartment Block (FICB)
All patients had received a FICB at the emergency department as standard preoperative hip fracture pain management. Informed consent about the procedure, including possible side-effects and complications was provided by the administering doctor at the emergency department. The FICB is a nationally protocolized procedure by the Dutch Association of Emergency Department Doctors (NVSHA). The procedure was performed by an emergency doctor (in training) with the patient in supine position. A linear ultrasound probe 10-18 MHz was used to identify the location of FICB administration. After visualization of the iliac fascia, a sterile echogenic needle was placed just below the iliac fascia and 3 cm lateral of the femoral nerve. After a negative aspiration, 1-2 mL of levobupivacaine was injected to confirm the desired position. If the correct plane was confirmed, 2 mg/kg levobupivacaine of 2.5 mg/mL was administered with a minimal volume of 40 mL and maximal dose of 150 mg. Under visualization of the injection of the anesthetic, every 5 mL aspiration was perfomed. 32 FICB with levobupivacaine has an onset of action of ≤15 min and can be effective up to 17 h after placement of a peripheral nerve block. 30 Standard procedure was to obtain and document NRS scores at 30 min and 8 h after FICB but in practice, these time points widely varied.
Outcome Measures and Data Collection
CTcue software (version 4.4.0.), an electronic medical record search engine (https://www.ctcue.com/) was used to identify and chart review eligible patients. Clinical data was collected from the electronic medical record. Demographics included age and gender. Baseline characteristics included fracture side, ASA (American Society of Anesthesiologists) score and use of opioids at home. Prehospital use of opioids was recorded as positive when patients had used any type of opioid prior to the hip fracture. Three preoperative NRS scores ranging from 0 to 10 (a higher score indicating more severe pain) were collected from the patient’s electronic medical record and all time points were registered. The first NRS score was prior to administering the FICB, the second NRS score was the first available score after FICB and the third NRS score was the second available NRS score after FICB. The type of hip fracture was then classified as either intracapsular (femoral neck) or extracapsular (intertrochanteric, pertrochanteric and subtrochanteric). Opioid use in the hospital after FICB was in predefined time frames: 0-6 h, 6-12 h and 12-24 h preoperatively. Lastly, a random sample including about a quarter of the patients from both groups, was made to calculate opioid doses into Morphine Milligram Equivalents (MME) and the total preoperative opioid use in MME was calculated.
Statistical Analysis
For the sample size calculation, a difference of 0.5 points in NRS score after FICB between the 2 fracture groups was considered clinically relevant. This was based on the expert opinion of the investigators. The expected standard deviation (SD) of approximately 1 was based on a study of Zou et al comparing the femoral obturator nerve block (FONB) with the Fascia Iliaca Compartment Block (FICB) in patients with hip fractures using comparable statistical analysis. 33 Eighty-seven patients per group were required for a 5% significance level and 90% power. With a margin of error, we planned to include 97 participants per group, randomly selected from the data collected.
Continuous data are reported as mean with SD when normally distributed. If not normally distributed, the median and interquartile range (IQR) are reported. A Shapiro-Wilk test was used to test for normal distribution of data. Categorical data are presented as absolute numbers and percentages. Baseline characteristics of the 2 fracture groups were compared using a Fisher (Freeman Halton) exact test for categorical data and Student’s t-test or Mann-Whitney U test for continuous data. Differences in NRS score between the 2 fracture groups were analyzed by a linear autoregression analysis with correction for baseline NRS score. Potential confounding by time and prior opioid use at home and effect modification by gender was tested. Differences in opioid use between patients from both groups post FICB and pre-surgery (0-6 h, 6-12 h, 12-24 h) was analyzed by a Fisher (Freeman Halton) exact test. Differences in total opioid doses (in MME) pre-operatively between both groups (as calculated for a quarter of the patients in both groups) was analyzed by a Mann-Whitney U test. Statistical significance was determined using two-tailed tests with a threshold of P < 0.005. A complete case analysis was performed using IBM SPSS Statistics version 28.0.0.0 (190). The manuscript was prepared according to the structure of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Guidelines.
Results
Of all patients presenting with a hip fracture between January 2019 and December 2021 at Isala hospital Zwolle, 183 met the eligibility criteria and were included in this study: 94 patients in the ICF group and 89 patients in the ECF group.
Demographics and Baseline Characteristics of Patients With an Intracapsular or Extracapsular Hip Fracture (ICF and ECF, Respectively) Who had Received FICB Preoperatively

aTwo-tailed tests with a threshold of P < 0.005.
bMann-Whitney U test.
cFisher (Freeman Halton) exact test.
NRS Score Before FICB, and First and Second NRS Scores Obtained After FICB

aTwo-tailed tests with a threshold of P < 0.005.
bLinear autoregression analysis.
cN = 83.
dN = 79.
Opioid Use After FICB Administration in Patients With Intracapsular or Extracapsular Hip Fracture
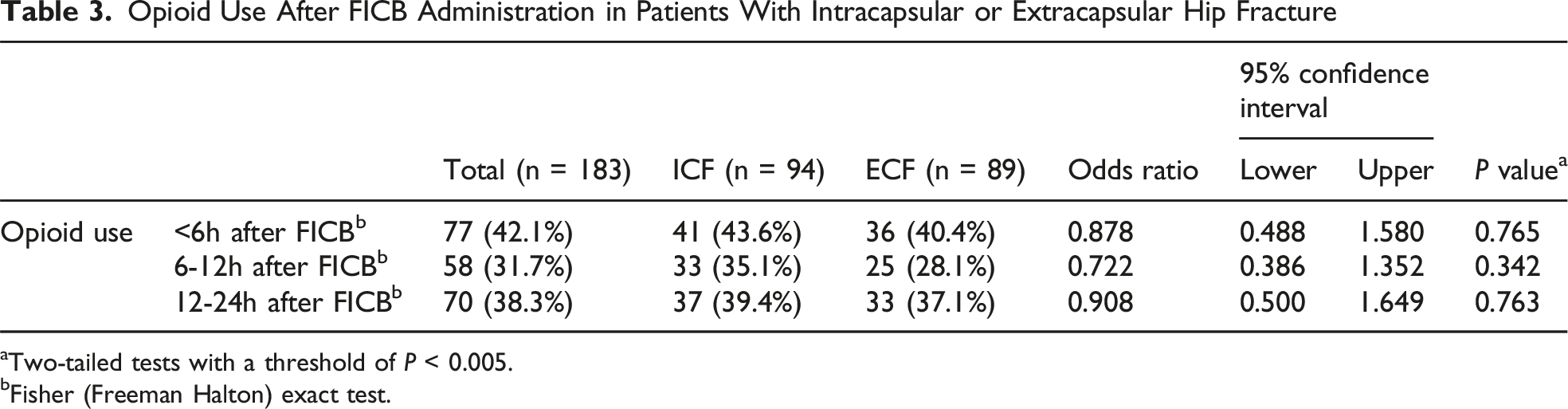
aTwo-tailed tests with a threshold of P < 0.005.
bFisher (Freeman Halton) exact test.

The difference in preoperative opioid use, measured in morphine milligram equivalents (MME), among the fracture type groups
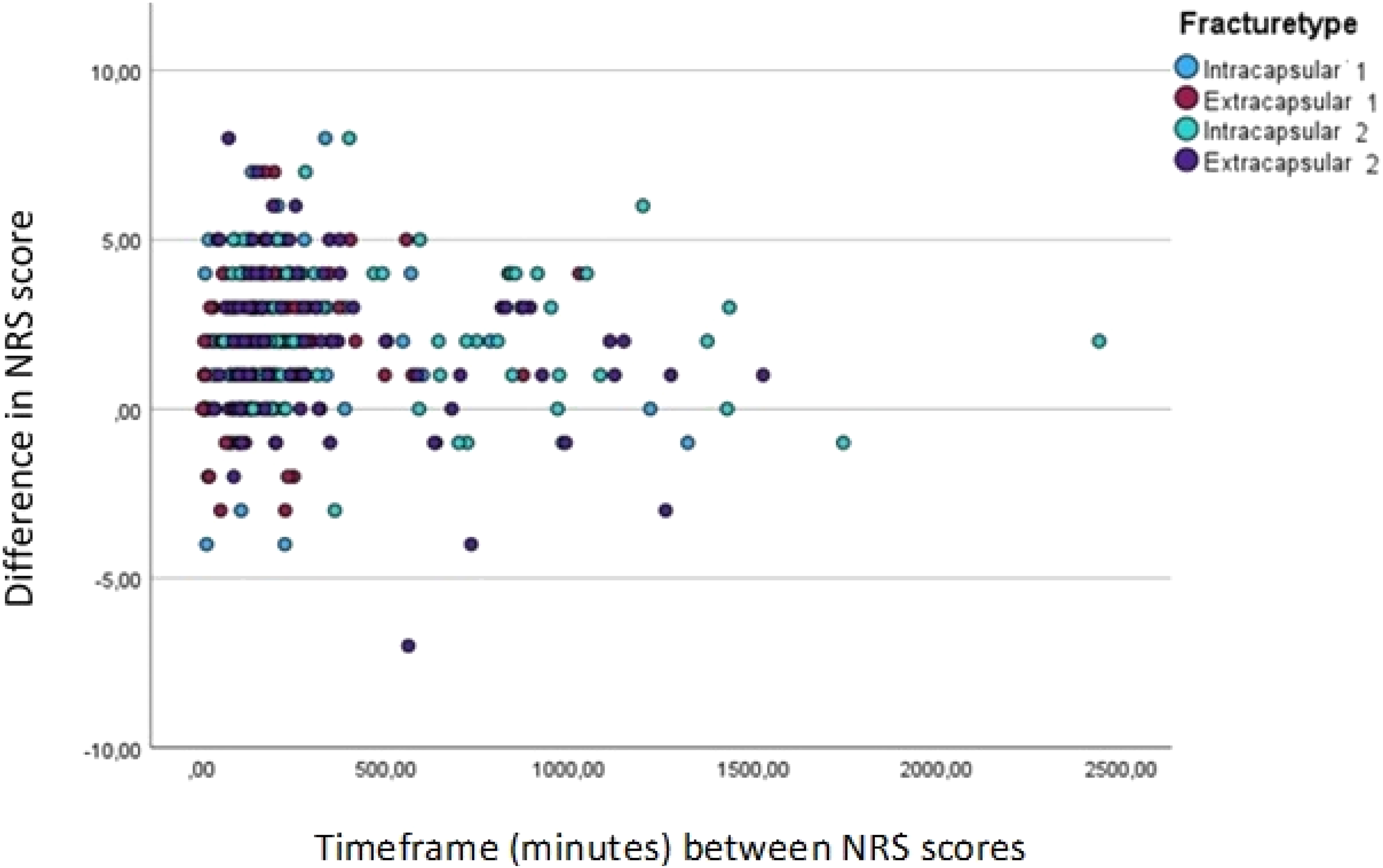
Timeframe of NRS scores after FICB administration
Discussion
This retrospective study compared the effectiveness of FICB in reducing pre-operative pain, as measured by NRS scores, in patients with intracapsular and extracapsular hip fractures. Clinical significant reduction of the preoperative NRS scores after FICB administration was shown in both hip fracture groups. No statistically significant difference in pain reduction between the 2 hip fracture groups was found. Opioid usage after FICB was also not significantly different between the 2 groups.
Several studies have recently evaluated locoregional pain management in patients with hip fractures. Aprato et al 20 investigated FICB vs intra-articular hip injection as preoperative pain management for intracapsular hip fractures, with the intra-articular injection group reporting significantly lower pain scores during mobilizing than the FICB group. No significant differences were found between the 2 groups at rest. Recently, Yin et al compared the outcomes of PENG and FICB in perioperative hip surgery in a systematic review. They reported no difference in pain scores within the first 24 hours between the PENG and FICB group. 34 To our knowledge, no previous study has compared the effect of pre-operative pain relief with a specific peripheral nerve block between patients with different hip fracture locations. It is known that the sensory innervation of the hip joint varies at different locations of the hip.2,14,20-23 Therefore, the type of peripheral nerve block may contribute to the effectiveness for pain relief in ICF or ECF patients based on the innervation of the hip.
Noteworthy in this study is a difference in pre-existing opioid use between the 2 fracture groups. The ECF group used significantly more opioids at home than the ICF group. After administration of FICB, there was no significant difference in number of opioid intakes between the fracture groups. This may indicate that the ECF group was frailer before the moment of trauma, which may have contributed to the (extracapsular) fracture type. The pre-existing opioid use may also have influenced the pain experience in this group. The opioids after administration of FICB were prescribed according to standard hospital protocolized pain management. This may have led to a higher amount of opioid intake than if a strictly on demand patient based opioid use schedule was followed. Data of the sample of patients in both groups show however that there was no difference in the total opioid usage (in MME) pre-operatively. Future studies should include patient based opioid use, especially for frail hip fracture patients.
The FICB is primarily utilized to provide analgesia to the hip region, the anterior and lateral aspects of the thigh, and partially to the knee. However, it does not typically anesthetize the posterior thigh and may inconsistently cover the medial thigh.27-30 The success of lateral femoral cutaneous nerve (LFCN) blockade with FICB is variable and influenced by several factors, including the specific technique employed (eg, landmark-based vs ultrasound-guided), the volume of local anesthetic used, and individual anatomical differences. 35 Those facts may contribute to some higher VAS scores after FICB in our population. However, we expect this to have occurred in both fracture groups, and therefore it is unlikely to have introduced significant bias.
The major strength of this study is that it is the first study to compare the effectiveness of pre-operative FICB in the 2 distinct fracture groups. Compared to similar studies, this study had a large number of patients in both fracture groups.20,33,34 Furthermore, this study only used pain scores prior to surgery to examine the effect of FICB on pain relief in both intra- and extracapsular hip fracture patients in the pre-operative period. Several studies have compared pain scores before and after surgery, which may lead to biased results due to the analgesic effect of surgery itself.14,33
This study exclusively included patients who received a FICB, and no comparative analysis with other peripheral nerve block techniques was conducted. Future studies may investigate the degree of effectiveness of FICB compared to other peripheral nerve blocks, such as the use of the PENG (peripheral nerve block) and FONB (Femoral Obturator Nerve Block), on the NRS score in ICF and ECF patients.
A possible limitation was the retrospective character of this study. Therefore, a wide distribution of time intervals between the NRS score before and after FICB administration was found. However, there was still no significant difference in pain relief between the 2 fracture groups when we corrected for time interval between NRS score before and after FICB in our autoregression analysis.
Conclusion
The fascia Iliaca Compartment Block (FICB) is an effective pre-operative treatment for pain relief in both intracapsular and extracapsular hip fractures. No statistically significant difference in pain reduction or opioid use was seen between the 2 different fracture types in our patients. With the knowledge and experience that the FICB is relatively easy to administer in frail patients, the FICB has great value as a regional pain block at the emergency department for both types of hip fracture patients.
Footnotes
Ethical Approval
This study was approved by the Isala Research Ethics Committee (approval no. 20220316) on March 16 2022. This is an IRB-approved retrospective study, all patient information was de-identified and patient consent was not required. Patient data will not be shared with third parties.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and analyzed during the current study are available in the Mendeley repository 36 .