
Abstract
Introduction
Pain management modalities after proximal femoral fracture are variable and have been studied extensively. Regional anesthesia, specifically femoral nerve (FNB) and fascia iliaca compartment blocks (FICB), can be used to provide analgesia preoperatively.
Methods
Systematic searches of all related literature were conducted in the Medline, Embase, and Cochrane Central Register of Controlled Trials databases. Randomized controlled trials (RCTs) of proximal femoral fractures were included. The pain scores at different time points, opioid requirement in 24 h, mean arterial pressure, time for spinal anesthesia, patient satisfaction, and incidence of side effects between the 2 groups were extracted throughout the study.
Results
Fifteen RCTs including 1240 patients met the inclusion criteria. The present meta-analysis indicated that compared with FNB, FICB could decrease the visual analog scale (VAS) scores at 4 h after surgery (P < .05). The incidence of side effects (nausea, vomiting, and sedation) was lower in the FNB group (P < .05). Compared to the FICB, no significant difference was found at any other observed time point. Additionally, no difference was found in opioid requirement at 24 h, mean arterial pressure, time for spinal anesthesia, or patient satisfaction (P > .05).
Conclusions
FICB demonstrates a reduction in VAS score at 4 while FNB decreases the risk of several adverse events. More high-quality RCTs are necessary for proper comparison of the efficacy and safety of FNB and FICB.
Introduction
Proximal femoral fractures are painful injuries that are difficult to manage in the geriatric population. 1 Improvements in surgical technique and the introduction of care pathways for hip fracture have improved outcomes including pain management. Despite these advances, challenges remain in achieving adequate analgesia in elderly hip fracture patients. Pain associated with immobility may lead to the development of postoperative complications such as hypostatic pneumonia or deep venous thrombosis. These complications increase healthcare costs and prolong hospital stay. 2 Under such circumstances, early provision of analgesia, even before surgical intervention, is a priority. 3
Considering the various adverse effects of opioid analgesics, peripheral nerve blocks have grown in popularity for pain management in patients with proximal femoral fractures. 3 The hip joint receives innervation from branches of the lumbar and sacral plexuses. 4 The femoral and obturator nerves innervate the anterior and anterolateral capsules, whereas the lateral femoral cutaneous nerve provides cutaneous innervation. The articular branches of the femoral nerve innervate the hip joint. Thus, the femoral nerve is a significant contributor to the development of postoperative pain following a proximal femoral fracture. 5 Compared with the obturator nerve block, branches of the sciatic and lateral femoral cutaneous nerve blocks, femoral nerve block (FNB), and fascia iliaca block (FICB) are attractive perioperative pain management techniques owing to their ability to block the extensive sensory nerves. 6 They have been proven to lower the rate of complications and improve pain control in this setting. 7
Some studies have been conducted to evaluate the effects of FNBs and FICB perioperatively.8-10 Although the FNB and FICB are 2 commonly utilized pain management techniques for proximal femur fractures, the differences in outcomes between these 2 nerve block procedures have not yet been investigated. Hence, the present meta-analysis aimed to compare these 2 procedures.
Methods
This meta-analysis of published literature was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (Figure 1). No ethical approval was obtained for this study.
11
All literatures were identified by electronically searching the Medline (1966–present), Embase (1966–present), and Cochrane Central Register of Controlled Trials databases. The following keywords were combined with Medical Subject Headings terms to improve the accuracy of the search results: “pain management, postoperative pain, hip fracture, proximal femoral fracture, femoral nerve blocks, and fascia iliaca compartment blocks.” The search included randomized controlled trials (RCTs) published up to April 2021. The PRISMA Flow Diagram showing the process of selecting eligible studies.
Inclusion Criteria
RCTs, studies conducted in older adults (age ≥60 years) with proximal femoral fractures, studies that evaluated FNB and FICB, and studies that reported at least one of the following outcomes were eligible for inclusion: cumulative consumption of morphine, visual analog scale (VAS) score, time to spinal anesthesia (SA), mean arterial pressure, patient satisfaction, and adverse effects.
Exclusion Criteria
Patients who had bone neoplasms, severe osteoporosis, infection, metal sensitivity, or mental health illness were excluded from the study.
Selection Criteria
The eligibility assessment was performed independently by 2 reviewers. Disagreements between reviewers were settled by discussion; if consensus was not reached, the third reviewer made the final decision as the adjudicator. The risk of bias was assessed using the Cochrane Collaboration tool, and the quality of the RCTs was evaluated using funnel plots. 12
Data Extraction
Data from the included studies were independently pooled by 2 authors. The following data were extracted and analyzed: first author’s name, publication year, number of patients, type of anesthesia, types of narcotic drugs and methods of administration, pain assessment methods, and adverse reactions. In studies with unclear or incomplete data, attempts were made to contact the authors to request for the missing data.
Statistical Analysis
RevMan5.3 (The Cochrane Collaboration, Oxford, United Kingdom) was used to analyze the pooled data. Using the chi-square test, heterogeneity was based on the P and I2 values. P > .10 and I2 < 50% indicated the absence of significant heterogeneity. A fixed-effects model was used for data analysis. A random-effects model was used when a significant heterogeneity was observed. For continuous data such as VAS scores and narcotic consumption, the mean difference (MD) and 95% confidence intervals (CIs) were pooled to determine the results. The relative risk with the corresponding 95% CIs was calculated for dichotomous data, such as vomiting, nausea, and other side effects. A P value of < .05 was considered significant.
Results
Literature Search
A total of 673 potential records were identified using an electronic search, including 291 duplicate articles. After assessing the titles and reading the abstracts, 368 articles were considered irrelevant and excluded; thus, only 15 studies eventually fulfilled the eligibility criteria.13-24 The 15 RCTs included 614 patients who underwent FNB and 626 patients who underwent FICB. The publication period ranged from 2010 to 2020.
Study Characteristics
Characteristics of All Included Studies.

Risk of Bias Assessment
The Cochrane Collaboration tool was used to evaluate the risk of bias in all included RCTs. A quality assessment of the methodology is shown in Figure 2. A high risk of bias was not found in any of the included studies. The bias risk of all trials.
Outcomes for Meta-analysis
Postoperative VAS scores at different time points. Details regarding the postoperative VAS scores at different time points (2 min, 20 min, 2 h, 4 h, 24 h at rest, 24 h at movement, 48 h at rest, and 48 h at movement) were available for 13 trials.14-26 Significant heterogeneity was found (P<.05) in the VAS scores at 2 h, 4 h, 24 h at rest, 24 h at movement, and 48 h at rest. Compared with FNB, FICB decreased the VAS score at 4 h after surgery (MD = .83, 95% CI: .41-1.24, P = .00). No significant difference was found between FNB and FICB at the rest of the time points postoperatively (2 mins, 20 mins, 2 h, 24 h at rest, 24 h at movement, 48 h at rest, and 48 h at movement) (MD = .08, 95% CI: −.12 to .28, P = .46) (MD = −.24, 95% CI: −.54 to .07, P = .13) (MD = −.05, 95% CI:−.82 to .73, P = .90) (MD = −.08, 95% CI: −.51 to .35, P = .71) (MD = −.16, 95% CI: −1.04 to .72, P = .72) (MD = −.26, 95% CI: −.59 to .07, P = .13) (MD = −.25, 95% CI: −.60 to .11, P = .17; Figure 3). Forest plot of postoperative VAS scores at different time points (2 mins, 20 mins, 2 h, 4 h, 24 h at rest, 24 h at movement, 48 h at rest, and 48 h at movement).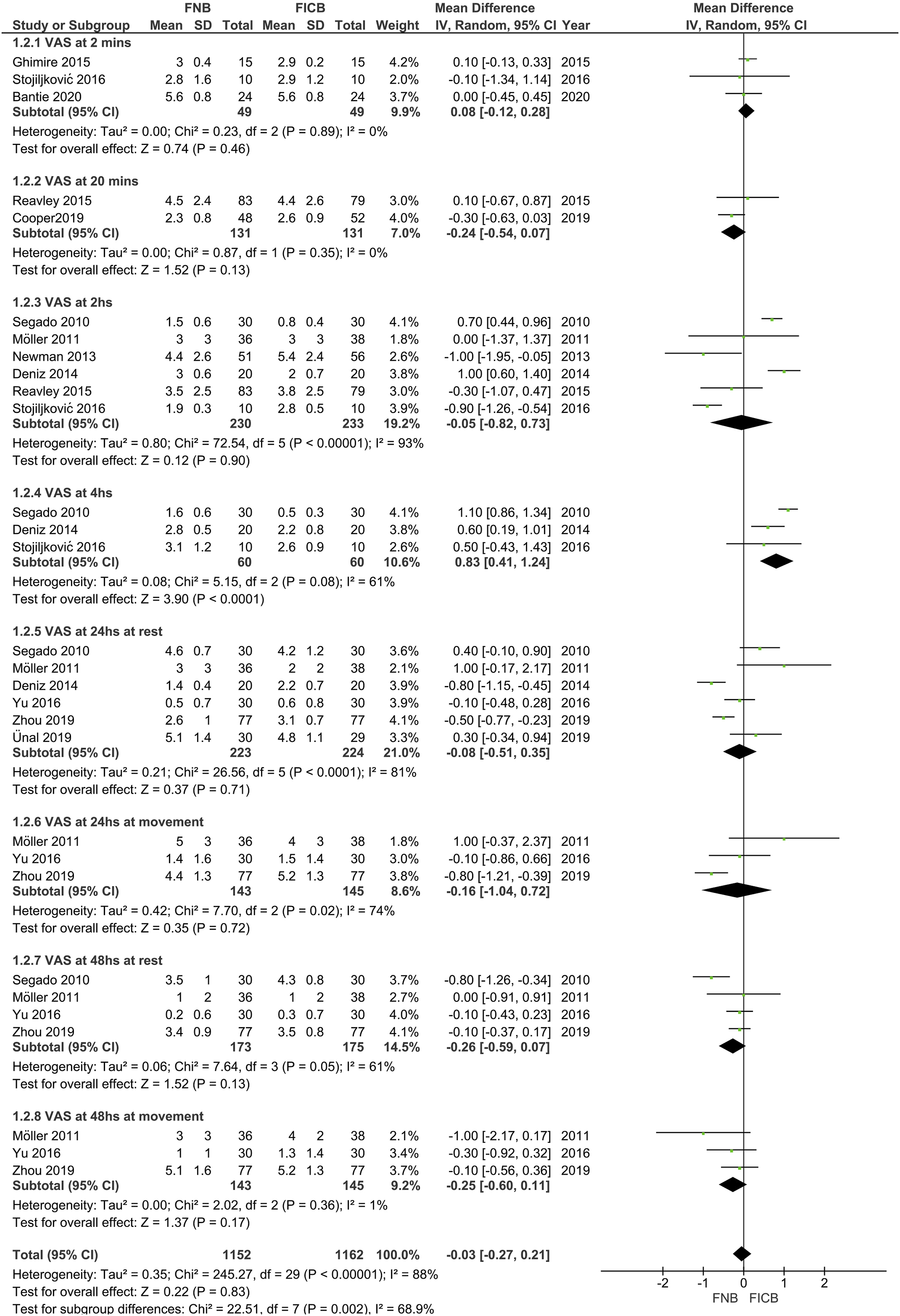
Narcotic requirements at 24 h. Three trials reported the details of narcotic consumption.19,22,24 Significant heterogeneity was found (P < .05); the pooled results from the meta-analysis showed no significant difference in the FNB groups compared with that in the FICB group in terms of reducing narcotic consumption at 24 h (MD = .45, 95% CI: −.30 to 1.20, P = .24; Figure 4). Forest plot of narcotic consumption at 24 h between the 2 groups.
Spinal anesthesia time. Three trials evaluated the time (s) for SA in the 2 groups.13,14,20 Significant heterogeneity was found (P < .05); a random model was performed. Compared with the FICB group, no significant difference in SA time was found in the FNB group (MD = −9.13, 95% CI: −61.28, 43.03, P = .73; Figure 5). Forest plot of time for spinal anesthesia between the 2 groups.
Mean arterial pressure (mmHg). Two trials compared the mean arterial pressure between the 2 groups.15,18 No significant heterogeneity was found (P > .05); hence, a fixed-model was developed. Compared with the FICB group, no significant difference was found in the mean arterial pressure in the FNB group (MD = −1.11, 95% CI: −5.00, 2.79, P = .58; Figure 6). Forest plot of mean arterial pressure (mmHg) between the 2 groups.
Patient satisfaction with the treatment. Details regarding patient’s satisfaction with the treatment were available in 6 trials.13,17,20,24-26 No significant heterogeneity was found (P > .05); hence, a fixed-model was developed. Results showed no significant difference between the 2 groups (relative rate: 1.00, 95% CI: .86-1.17, P = .99; Figure 7). Forest plot of patient’s satisfaction to treatment between the 2 groups.
Adverse effects (nausea, vomiting, and sedation). Two studies reported the incidence rate of nausea and vomiting,15,18 while 3 studies reported the incidence rate of sedation.14,21,26 Significant heterogeneity was not found in all included studies; therefore, a fixed-model was used (P > .05). Compared with FICB, FNB significantly reduced the incidence rates of nausea, vomiting, and sedation (relative rate: .30, 95% CI: .12-.79, P = .01) (relative risk: .13, 95% CI: .02-.71, P = .02) (relative risk: .40, 95% CI: .20-.81, P = .01; Figure 8). Forest plot of adverse effects (nausea, vomiting, and sedation) between the 2 groups.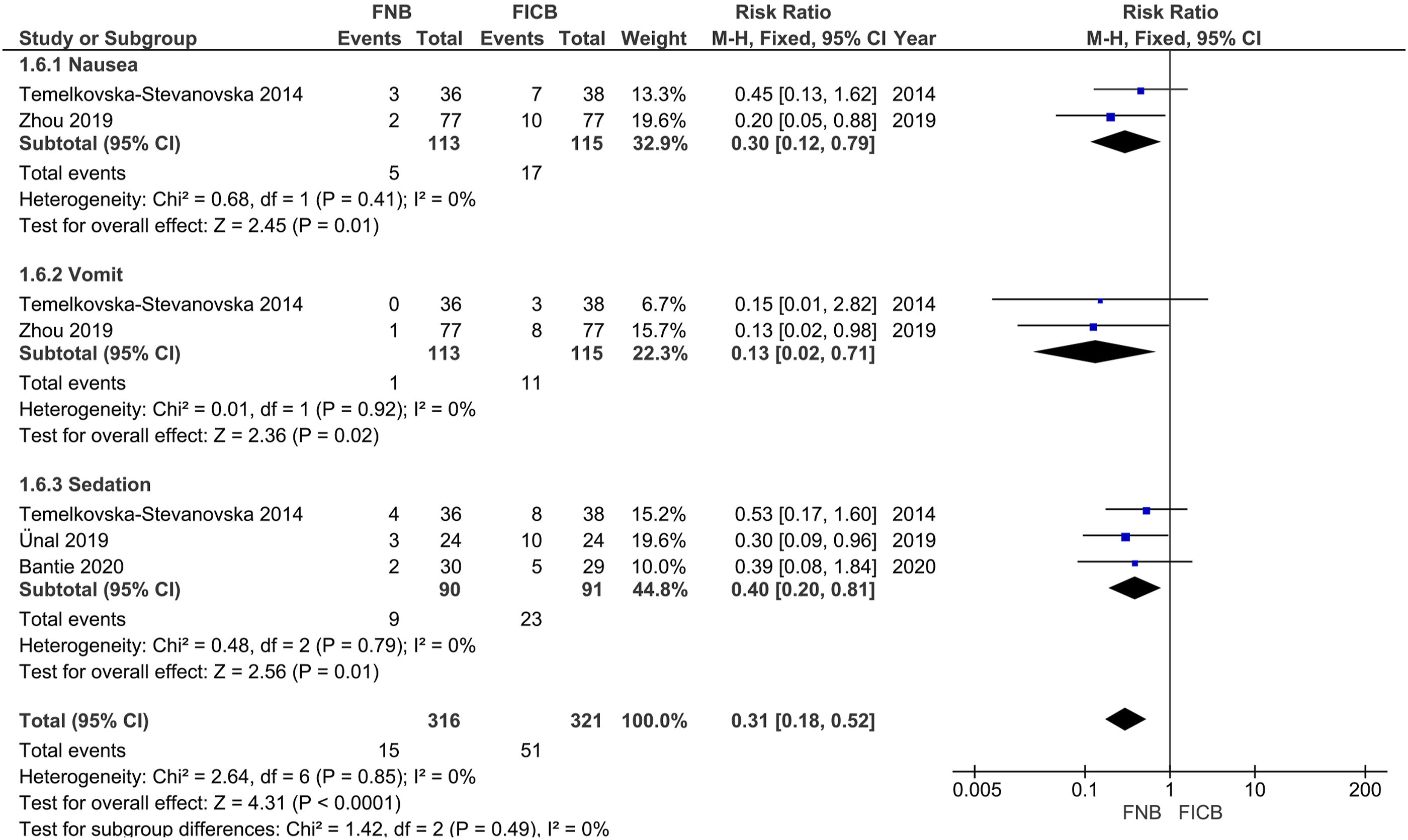
Discussion
This meta-analysis increases our understanding of the regional nerve blocks used in the management of proximal femoral fractures. Results demonstrated that the FICB produced better postoperative analgesia at 4 h. However, the FNB group exhibited lesser nausea, vomiting, and sedation. Minimizing the side effects of anesthesia and opioids improves patient’s satisfaction and accelerates recovery. 27 The FNB group showed a reduction in the side effects, which was consistent with the results of previous studies.3,28,29
The benefits of block analgesia vs non-block analgesia were clearly demonstrated. It decreases postoperative morbidity, improves surgical results, facilitates rehabilitation, and shortens the postoperative recovery time. Although the VAS scores demonstrated superior analgesia at 4 h in the FICB group, no significant difference was found at the other time intervals. This finding could be explained by the similarity between the 2 nerve block procedures. An FNB, when performed using a high volume of local anesthetic, may also produce local anesthetic spread that reaches the obturator and lateral femoral cutaneous nerves. In addition, the hip occasionally receives nerve supply from the sciatic and superior gluteal nerves. These nerves were not affected by FNB, which explains the lower reduction in pain in the group. Regardless, adequate pain management has been associated with reduced therapeutic costs and shorter hospital lengths of stay. 30
Peripheral nerve blocks are an integral part of the opioid-sparing strategy employed by the United Kingdom’s National Institute for Health and Care. They are considered good options, especially when the use of multimodal analgesia, such as oral analgesic or non-pharmacologic intervention, is contraindicated or predicted to be ineffective. 31 The use of FNB and FICB reduced the consumption of opioids; however, no significant difference was found between the 2 groups. This finding is consistent with those of previous studies.32,33
Time for SA, mean arterial pressure, and patient satisfaction were the common indices in the postoperative period used to compare the efficacy between FNB and FICB. Better pain relief and better positioning during FNB and FICB were reflected in the time required to perform the SA. As shown in Figure 5, the time required to perform SA with FICB was the same as that for FNB in the present study. Similarly, the mean arterial pressure recorded during surgery was a good indicator of the effects of both FNB and FICB on cardiovascular stability. As shown in Figures 6–7, both methods showed efficacy in these outcomes. Again, this finding supports those of previous research.33,34
This meta-analysis was the first to assess the differences between FNB and FICB in the treatment of proximal femoral fractures. To strengthen the data, observational or retrospective studies were not included. RCTs are the gold standard for all research; however, heterogeneity was still observed in this study. This study has several limitations. First, perioperative surgical characteristics, such as duration of surgery and intraoperative complications, were not considered. Second, multiple non-opioid drugs, such as acetaminophen, paracetamol, and non-steroidal anti-inflammatory drugs, are used in anesthesia/analgesia, whose action is not only limited to nerve blockade. This may limit the ability to distinguish between block types using these interventions. Third, the placement of block or timing of block placement varied among the included trials: the ultrasound-guided placement was applied in less than half of the trials,13,15,17,19,22,26 and the timing of placement was only recorded in 4 trials.13,14,20,22 Ultrasound guidance is a superior technique for visualizing the anatomical structures during the administration of nerve blocks and can be used to confirm the correct placement of FNB and FICB. These inconsistencies may have complicated the results. Moreover, a wide range of local anesthetic medication doses was used, from 5 mL to 50 mL, among the trials. Lastly, almost all of the included studies were performed by anesthetists, which skewed the focus toward anesthetic outcomes. Some valuable information, such as the operative approach, has not been reported in many trials. These missing data could possibly have an effect on the degree of postoperative surgical pain and should be considered in future studies.
Conclusion
This meta-analysis of RCT studies revealed that FNB was effective in reducing the side effects (nausea, vomiting, and sedation), and FICB was more advantageous in reducing the VAS scores at 4 h postoperatively. No significant difference was found in the VAS scores at the rest of the time points, narcotic requirement in 24 h, time for SA, mean artery pressure, and patient satisfaction between the FNB and FICB groups. More high-quality RCTs are necessary for proper comparison of the efficacy and safety of FNB and FICB.
Footnotes
Authors' Contributions
X.D.L and C.H. conducted the literature search and determined the studies for exclusion and inclusion. X.D.L and C.H. extracted data from the included studies, performed the meta-analysis, and drafted the manuscript. X.D.L and W.L.Y. conceived the idea of the study, designed the study, and critically revised the manuscript for important intellectual content. All authors reviewed the paper and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by 1. Tianjin Enterprise Postdoctoral Innovation Project Funding (No.TJQYBSH2018020), 2. Scientific and Technological Talent Cultivation Project of Tianjin Municipal Health Commission (No. RC20112), Science and Technology Foundation of Tianjin Health Bureau (ZC20052).