
Abstract
Purpose
Post-acute care (PAC) plays a key role in recovery following hip fractures. The aim of the study is to examine the factors affecting the achievement of the minimal important change (MIC) in older patients with hip fractures.
Methods
This retrospective cohort study included 228 patients who underwent surgical interventions for hip fractures and received subsequent PAC between 2020 and 2021. Data on demographics, medical history, and lifestyle habits were collected. Outcomes were measured using the Barthel Index, Numeric Rating Scale (NRS), and Harris Hip Score (HHS). Univariate and multivariate regression analyses were conducted to identify predictors of achieving the MIC.
Results
After treatment, significant improvements were observed in the Barthel Index (from 41.45 to 65.15, P < 0.001), NRS (from 5.03 to 2.52, P < 0.001), and HHS (from 29.35 to 63.68, P < 0.005). The MIC for the Barthel Index, NRS, and HHS were determined to be 6.20, 0.92, and 6.69, respectively. Dementia (odds ratio [OR] = 3.77, 95% confidence interval [CI] = 1.51-9.44, P = 0.005), age above 80 years (OR = 2.80, 95% CI = 1.15-6.84, P = 0.024), and heart failure (OR = 4.21, 95% CI = 1.34-13.23, P = 0.014) served as significant predictors of failure to achieve the MIC with the Barthel Index. For HHS, Diabetes mellitus was the only significant predictor of failure to achieve the MIC (OR = 4.32, 95% CI = 1.00-18.62, P = 0.050).
Conclusions
This study highlights major improvements in the Barthel Index, NRS, and HHS among older patients receiving PAC after hip fractures, along with a quantifiable MIC. Dementia is a robust predictor of failure to achieve the MIC with the Barthel Index, and advanced age, heart failure, and diabetes mellitus are key factors for optimizing recovery.
Introduction
Hip fractures in older adults pose substantial health concerns, with major implications for morbidity, mortality, and the health-care burden globally. 1 Managing these fractures is a complex process that extends beyond acute medical treatment, with the goals of restoring functional independence and improving quality of life.2,3 Post-acute care (PAC) plays an essential role in the recovery process, offering a continuum of care through services such as skilled nursing, inpatient rehabilitation, home health care, and long-term hospital care.4,5 These services are tailored to the diverse needs of older patients, aiming to enhance their functional recovery, prevent complications, and reduce their rehospitalization rate. Lee et al. reported that PAC significantly enhances physical function and quality of life in patients with hip fractures, 5 while Chiang et al. demonstrated that PAC reduces mortality and complications—including urinary tract infection, pressure sores, and pneumonia—in octogenarian and nonagenarian patients with fragility fractures. 6 Therefore, a robust PAC system is essential for offering structured support to facilitate the restoration of autonomy and functionality in older patients after acute medical treatment. 5
However, prior research has demonstrated that a range of risk factors significantly influence the prognosis of hip fractures among older adults.7,8 The risk factors include advanced age, the presence of comorbid conditions such as diabetes and cardiovascular disease, cognitive impairment, and the presence of a prefracture functional status. 9 Social determinants such as living alone or having a low socioeconomic status serve as barriers to recovery, and intrinsic factors such as nutritional status and psychological well-being influence the trajectories of recovery.10-12 However, the extent to which these previously identified risk factors influence the prognosis of hip fractures in older adults after receiving PAC has not yet been comprehensively elucidated in the existing literature.
In PAC, the minimal important change (MIC) is regarded as a pivotal benchmark; it represents the smallest change in a treatment outcome that a patient would identify as a vital improvement; thus, MIC help clinicians differentiate between meaningful changes and statistical noise. 13 The MIC of a patient’s self-reported outcome can be used as a measure of the minimum improvement achieved by this patient after hip fracture surgery. Generally, multiple factors influence the variability of postoperative care and rehabilitation, including the availability and quality of health-care services and patient characteristics. 14 Currently, a disparity exists in the recovery outcomes of post-hip fracture care, which is a recurring concern in orthopedic and geriatric medicine. In addition, the evidence supporting the risk factors associated with the outcomes of post-hip fracture surgery remains inconclusive. Optimal recovery is often hampered by systemic problems, such as limited access to specialized rehabilitation facilities, variations in care practices, and insufficient patient support systems.15,16
Despite the apparent benefits of PAC, its utilization and efficacy are influenced by socioeconomic factors, resource availability, and patient prefracture health status. Timely and adequate PAC considerably influences the likelihood of achieving the MIC and overall long-term outcomes after surgery.
The aim of this study is twofold: (1) to determine the proportion of patients achieving MIC in postoperative pain and hip function following PAC after hip fracture surgery, and (2) to identify both intrinsic and extrinsic factors associated with the attainment of MIC.
Method
Patient Selection
This manuscript was prepared in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. This retrospective cohort study was approved by the institutional review board (A-ER-113-115). Data were extracted from the PAC records, including patient records, of the National Cheng Kung University Hospital (NCKUH) between January 2020 and December 2021. The inclusion criteria were as follows: (1) having undergone a surgical intervention for hip fracture and (2) having completed a hospital-based PAC program. Hip fractures included femoral neck fractures (FNFs) and femoral intertrochanteric fractures (ITFs). Surgical interventions included hip hemiarthroplasty (HA) and open reduction and internal fixation (ORIF) with dynamic hip screws, cephalomedullary nails, or cannulated screws, which are routinely used to treat the aforementioned injuries. Corresponding surgical codes were obtained from the records of the NCKUH. The exclusion criterion was discontinuation of PAC for any reason, and the reasons for discontinuation were documented accordingly.
In Taiwan, the PAC system for hip fractures is a comprehensive program designed to support patients after discharge from acute-care hospitals. Within 3 weeks of discharge, these patients are enrolled in a hospital-based PAC program, and they participate in daily 50-minute sessions on weekdays that are led by a physical therapist. These sessions focus on post-surgical exercise and fall prevention, incorporating range-of-motion exercises, lower-extremity strengthening, mobility training, and balance training. To aid in the performance of activities of daily living, suitable assistive devices are recommended, and environmental assessments are conducted to mitigate the risk of falling. Patients also receive daily visits from physicians and continuous nursing care to ensure their close monitoring and to provide support throughout their recovery process. 5
Data Collection
Postoperative progress and rehabilitation were recorded after hip fracture surgery. Data were obtained to provide pretreatment and post-treatment perspectives, covering the time before and after receiving PAC. The outcomes of and relationships between different factors were evaluated from several aspects.
Comprehensive patient information was collected, including age, body height, body weight, and body mass index (BMI). For analytical purposes, patients aged above 80 years were classified as “oldest old”. 17 In addition to these metrics, sociodemographic details such as marital status and child caregiving responsibilities were precisely recorded. Marital status was precisely defined as follows: individuals who were married were classified as “married,” whereas those who were widowed or divorced were categorized as “unmarried.”
Overall, the types of fractures and their subsequent treatments were systematically classified. These classifications included femoral neck fracture status after hemiarthroplasty, femoral neck fracture status after ORIF, stable femoral intertrochanteric fracture status after ORIF, and unstable femoral intertrochanteric fracture status after ORIF. The criteria for unstable ITFs included fractures with reduced trochanteric involvement, reverse oblique fractures with posteromedial comminution, and lateral cortex fractures. 18
Lifestyle habits such as smoking and alcohol consumption were documented. A thorough medical history was obtained for each patient, detailing conditions such as coronary artery disease, heart failure, chronic obstructive pulmonary disease, peripheral vascular disease, cerebrovascular disease, dementia, peptic ulcers, liver cirrhosis, diabetes, chronic kidney disease (CKD), and hemiplegia. For the purposes of this study, peptic ulcers were defined as ulcers confirmed through gastrointestinal endoscopy, and CKD was defined based on a glomerular filtration rate of less than 60 mL/min/1.73 m2.
The outcome measures included the Barthel Index, Numeric Rating Scale (NRS), and Harris Hip Score (HHS).5The Barthel Index 19 was used as a primary tool to measure the performance of activities of daily living of patients. This index evaluates an individual’s ability to perform 10 basic activities: eating, bathing, grooming, dressing, bowel control, bladder control, toilet use, chair or bed transfer, mobility, and stair climbing. The total score ranges from 0 to 100, with 0 indicating total dependence and 100 indicating complete independence. The NRS 20 is a simple tool commonly used to evaluate the intensity of pain. Individuals rate their pain on a scale from 0 to 10, with 0 representing “no pain” and 10 representing “the worst pain imaginable.” The HHS 21 is a clinician-based outcome measure used to evaluate the outcomes of hip surgery, particularly hip replacement. The total score ranges from 0 to 100, with higher scores indicating more favorable hip function (90-100 indicating excellent function, 80-89 indicating good function, 70-79 indicating fair function, and <70 indicating poor function).
Statistical Analysis
A distribution-based technique was used to calculate the MIC in the absence of a credible anchor-based reference value22-24 After PAC, the degree of improvement achieved was measured using the Barthel Index and HHS. The MIC was defined as half of 1 standard deviation of the data. 25 Subsequently, patients were divided into 2 groups: those who reached the MIC and those who did not. A comparative analysis was conducted to examine the aforementioned factors in these 2 groups. Variables with statistical significance (P < 0.05) were entered into univariate logistic regression models, and the odds ratios (ORs) of these factors were calculated. In addition, a sensitivity analysis was conducted to assess whether the effects of key variables on PAC recovery were consistent across fracture types and surgical methods. Patients were stratified accordingly, and logistic regression was used within each subgroup to estimate ORs and 95% confidence intervals (CIs) for achieving improvement in the 3 outcome measures. All statistical analyses were conducted using IBM SPSS Statistics version 23.0 (IBM, Armonk, NY, USA), with P values <0.05 considered statistically significant.
Results
A total of 228 patients, with a mean age of 75.99 ± 11.13 years, were included in this study (Figure 1). These patients comprised 78 men (34.2%) and 150 women (65.8%), with a mean body weight of 57.19 ± 30.26 kg, a mean body height of 156.29 ± 8.27 cm. The mean BMI was 23.40 ± 12.98 kg/m2. As presented in Figure 2, patients exhibited significant improvements in their clinical outcomes after the PAC program. Their Barthel Index for activities of daily living increased from 41.45 ± 2.55 to 65.15 ± 13.23 (P < 0.001), with a mean increase of 23.71 ± 12.40. Their NRS for pain decreased from 5.03 ± 0.32 before treatment to 2.52 ± 1.84 after treatment (P < 0.001), with a mean decrease of 2.50 ± 1.84. In addition, their HHS for hip function increased from 29.35 ± 2.35 before treatment to 63.68 ± 13.73 after treatment (P < 0.001), with a mean increase of 34.33 ± 13.39 (Table 1). Patient Selection Flowchart Box Plots of the Barthel Index, Numeric Rating Scale, and Harris Hip Score before and after Post-acute Care. Boxes Indicate the Interquartile Range (25th–75th Percentile), the Line Inside Each Box Represents the Median, and Whiskers Show the Range Postoperative Clinical Outcomes and MIC Thresholds for Patients With Hip Fractures After PAC MIC, minimal important change; PAC, post-acute care.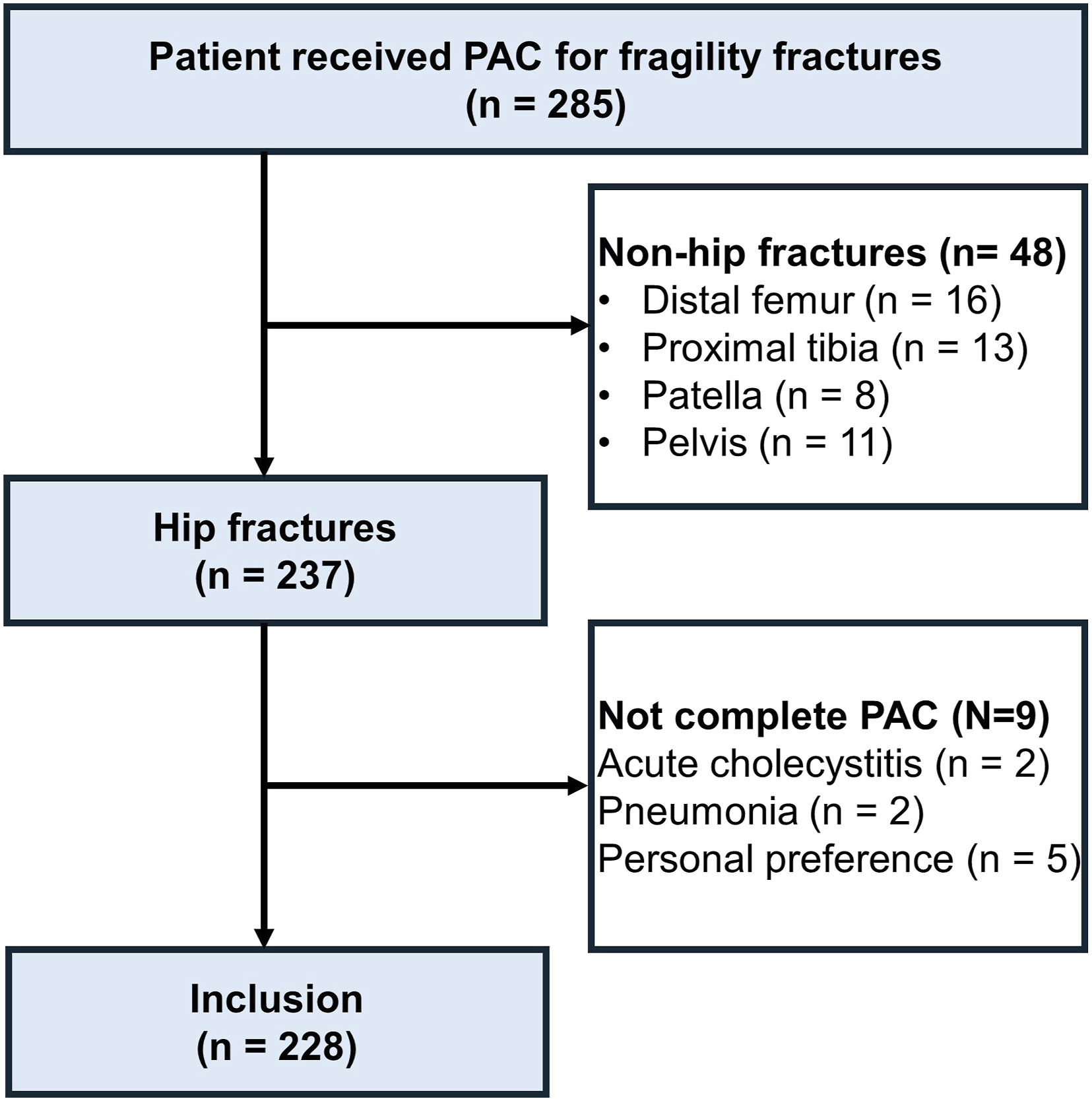


Comparison of Demographic Characteristics, Fracture Types, and Comorbidities in Patients Who Achieved the MIC and Those Who did Not

Data are presented as mean ± standard deviation. P-values were calculated using the Chi-square test for categorical variables and the Mann–Whitney U test for continuous variables (both two-tailed). The level of significance was set at P < 0.05. Bold font indicates statistical significance. BMI, body mass index; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CVD, cerebrovascular disease; DM, diabetes mellitus; FNF, femoral neck fracture; HA, hemiarthroplasty; ITF, intertrochanteric fracture; MIC, minimal important change; ORIF, open reduction internal fixation; PAC, post-acute care; PVD, peripheral vascular disease.
Odds Ratios of Significant Variables Predicting Patients’ Inability to Achieve the MIC With Univariate Logistic Regression

P-values were calculated using two-tailed logistic regression analysis. The level of significance was set at P < 0.05. Bold font indicates statistical significance. CI, confidence interval; MIC, minimal important change; OR, odds ratio.
Sensitivity Analysis of the Effects of Dementia and Diabetes Mellitus on the Odds of Failure to Achieve MIC Across Fracture Types and Surgical Methods

P-values were calculated using two-tailed logistic regression analysis. The level of significance was set at P < 0.05. Bold font indicates statistical significance. FNF, femoral neck fracture; HA, hemiarthroplasty; ITF, intertrochanteric fracture; MIC, minimal important change; ORIF, open reduction internal fixation.
Discussion
In this study, we discovered that PAC provided benefits to older patients with hip fractures by improving their overall functional outcomes, reducing their pain levels, and facilitating the recovery of hip function. Despite these positive outcomes, certain subgroups of patients did not experience significant clinical improvements. Specifically, patients belonging to the oldest old category, patients with heart failure, and patients with dementia were less likely than their counterparts to achieve the MIC for the Barthel Index after PAC. Similarly, patients with DM were less likely than their counterparts to achieve the MIC for the HHS.
Overall, our findings indicated that dementia significantly influenced the recovery outcomes of older patients with hip fractures. This finding is consistent with those of previous studies indicating that cognitive impairment substantially hinders rehabilitation as a result of difficulties in following rehabilitation protocols and decreased motivation for performing recovery activities.14,26 In addition, dementia is often correlated with other comorbidities and increased frailty, which can exacerbate postoperative complications and impede functional recovery.9,11 According to previous studies, patients with dementia are more likely than those without dementia to experience delayed mobilization and to require longer rehabilitation duration, which ultimately affect their functional outcomes.27-29 In addition, our results showed that dementia had a significant impact on patients with ITF but not on those with FNF. This finding is consistent with previous reports indicating that dementia patients undergoing HA demonstrated better one- and 2-year survival compared with those receiving ORIF. 30 This may be explained by the fact that full weight bearing is generally permitted earlier after HA than after ORIF, and patients with dementia often have greater difficulty adhering to postoperative weight-bearing restrictions.30,31 These patients typically require PAC services to offer structured support and specialized rehabilitation; thus, these services address some of the challenges posed by cognitive impairment. According to the literature, tailored PAC programs significantly improve patient outcomes by addressing the specific needs of patients with dementia, although the complexity of care required remains high.29,32
In this study, advanced age was significantly associated with failure to achieve the MIC in the Barthel Index.These findings are consistent with those of previous studies, indicating the low physiological resilience and high prevalence of comorbidities in older adults collectively hinder their postoperative recovery.1,2 Older patients often have slower healing and are more prone to complications such as infections or thromboembolic events, which can delay rehabilitation and functional recovery. In addition, comorbidities common in older adults may further hinder recovery, necessitating more intensive and prolonged rehabilitation.33,34 In contrast to previous studies, in this study, we observed that heart failure had a significant effect on the MIC for the Barthel Index. This discrepancy may be attributable to the complex interplay of multiple comorbidities and the overall health status of patients with heart failure. Although heart failure can cause fatigue and reduced exercise tolerance, its isolated effect may be masked by coexisting comorbidities and varying disease severity, leading to inconsistent results. 35 Some studies have suggested that the effective management of heart failure, including optimized medical therapy and close monitoring, can mitigate its effect on postoperative recovery, underscoring the importance of comprehensive care.36,37 However, advanced age and heart failure were associated with poor outcomes only in the Barthel Index, but not in the NRS or HHS, suggesting that these patients did not necessarily experience greater pain or worse joint-specific function. Therefore, tailored rehabilitation programs emphasizing activities of daily living—such as dressing, feeding, and mobility—together with cardiopulmonary conditioning, are essential to enhance overall functional independence in this population.
In this study, DM was identified as the only significant predictor of failure to achieve the MIC for the HHS, but not for the Barthel Index. This result indicates that DM has a negative effect on hip function. Despite these findings, the relationship between DM and functional outcomes after hip fractures remains unknown. Although DM is typically associated with increased mortality and high risks of cardiac complications and renal failure,38,39 multiple studies have indicated that patients with and without DM often achieve a similar degree of functional recovery.40,41 Overall, the severity and management of DM appear to be key factors affecting functional outcomes after hip fractures. Lee et al. 42 reported that patients with DM controlled by oral antidiabetic drugs did not have high complication or mortality rates, whereas those who required insulin had poor outcomes. Similarly, Ben-Joseph et al. 43 discovered that after hip fracture, patients with well-controlled DM exhibited a rehabilitation potential similar to that of individuals without diabetes despite having more comorbidities. Taken together, these findings indicate that the effective management of DM is more crucial than its mere identification, particularly for older individuals recovering from hip fractures.
Our findings indicated that factors such as sex, body weight, body height, marital status, and lifestyle habits (eg, smoking and alcohol consumption) did not have uniform significant effects on the achievement of the MIC for different outcome measures. This lack of a significant association for these variables may be due to several reasons. First, the effects of smoking and alcohol consumption may become more pronounced in the presence of other severe comorbidities, thereby mitigating their isolated effects in broad multivariate analyses. Second, the relatively small sample size for certain subgroups may limit the statistical power for detecting significant associations. Third, lifestyle factors such as smoking and alcohol consumption may have a delayed effect on recovery outcomes, which was presumably not fully captured within the follow-up period of this study. According to the literature, the long-term effects of smoking and alcohol consumption are more pronounced in terms of chronic disease progression than in terms of immediate postoperative outcomes, which may explain the lack of significant findings in our study.44,45 Therefore, although these factors must be considered in the broad context of patient health, their direct effect on short-term recovery after hip fracture surgery is unclear.
This study has several limitations. First, the MIC values were estimated using a distribution-based method because no established anchor-based reference was available. This methodological constraint may limit the clinical interpretability of the findings, as distribution-based thresholds reflect statistical variation rather than patients’ perceived meaningful improvement. Second, the retrospective study design may have introduced selection bias, as only patients with complete medical records were included. Moreover, the data were obtained from a single institution, which may limit the generalizability of the results to other settings. Third, although the overall sample size was moderate, the number of patients who failed to achieve the MIC was relatively small, which reduced the statistical power and precluded inclusion of multiple covariates in multivariate models. Consequently, only univariate analyses were performed, and the associations identified should be interpreted as exploratory rather than confirmatory, as they may be influenced by unmeasured confounding factors. Finally, some variables such as pain scores and activities of daily living were self-reported, which may have introduced measurement or reporting bias. In addition, the follow-up duration may have been insufficient to capture long-term functional recovery or delayed effects of certain prognostic factors.
Conclusion
Overall, this study highlights major improvements in the Barthel Index, NRS, and HHS among older patients receiving PAC after hip fracture surgery, along with a quantifiable MIC. Our findings indicate that dementia is a strong predictor of failure to achieve the MIC, and advanced age, heart failure, and DM are key factors for optimizing recovery. Taken together, these findings emphasize the need for personalized PAC strategies and the comprehensive management of comorbidities to improve functional recovery and quality of life in this vulnerable population.
Footnotes
Acknowledgments
We thank Medical Device R & D Core Laboratory, National Cheng Kung University Hospital, Tainan, Taiwan, Ms. Shing-Yun Chang BS, MSc and Ms. Ling-Yu Wang (Department of Orthopedic Surgery, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan) for assistance with this project.
Ethical Considerations
This study was approved by the institutional review board of National Cheng Kung University Hospital (A-ER-113-115).
Author Contributions
YC wrote the main manuscript text; FCK, CKH analyzed and interpreted the data; WRS approved the final version of the manuscript; HHL, GYL searched for relevant studies and abstracted the data; KLH designed the study and approved the final version of the manuscript. All authors reviewed the manuscript before submitting it.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.