
Abstract
Background
The functional outcome in patients with preexisting osteoarthritis after surgically treated trochanteric fracture is not yet fully elucidated. As the global population ages, the coexinsting of degenerative joint osteoarthritis and fragility fractures is increasing. Consequently, it is imperative to provide affected patients with information regarding the anticipated clinical outcomes. The objective of this study is to examine the impact of preexisting hip osteoarthritis in elderly patients on the clinical outcome following trochanteric fracture fixation.
Methods
In this retrospective single-center study elderly patients aged ≥70 years who underwent intramedullary nailing between January 2016 and March 2023 have been analysed. The severity of hip osteoarthritis was stratified into two categories: grade 0-II and grade III-IV, according to the Kellgren-Lawrence classification system. Radiological signs of consolidation were ascertained. A comprehensive evaluation of the patients’ demographics and patient-reported outcome measures (Oxford Hip Score, WOMAC-score, and SF-36-score) was conducted, followed by a thorough statistical analysis, with a significance set at P < 0.05.
Results
21 patients with 23 affected hips were included (mean age 81 ± 7.5 years; 81% female) with a mean follow-up duration of 15.1 ± 13.8 months. Patients with advanced OA (KL III-IV) reported significantly lower Oxford Hip Scores (33.3 ± 6.3 vs 43.1 ± 6.7; P = 0.003), and higher total WOMAC and WOMAC pain scores (P = 0.016 and P = 0.003).
Conclusion
The severity of pre-existing osteoarthritis of the hip in patients with intertrochanteric fractures is a significant risk factor, potentially leading to a diminished quality of life postoperatively. Further studies are necessary to provide therapeutic guidance.
Keywords
Introduction
Background
Intertrochanteric femoral fractures (IFF) represent the most common subtype of hip fractures, 1 particulary among the elderly population. With increasing life expectancy and a growing proportion of older individulas worldwide, the incidence of these fractures continues to rise.2,3 Typically caused by low-energy trauma, IFFs are associated with significant morbidity, including substantial physical limitations and a potential loss of independence.1,3 Intramedullary nailing is widely regarded as the gold standard treatment for IFFs, particulary in unstable fracture patterns, 4 due to its ability to provide stable fixation with favorable biomechanical properties. The Trochanteric Fixation Nail Advanced (TFNATM) system has been widely evaluated and is associated with high-qualitiy fracture reduction, accurate implant positioning, and a postoperative complication rate of approximately 20%. 5 In the present study, the TFNATM implant was also the primary fixation method utilized.
These considerations are especially relevant for patients with advanced hip osteoarthritis (OA), in whom joint preservation remains a critical concern – particularly the preservation of the greater trochanter, which is essential for potential future total hip arthroplasty. Patients with pre-existing OA often experience pain and functional limitations, which may be further exacerbated by an IFF, potentially leading to poorer outcomes and increased disability. In such patients, intramedullary nailing is generally preferred over primary arthroplasty due to shorter operation times, reduced blood loss, fewer complications, lower mortality rate, overall reduced healthcare costs.6-8 Given the rising prevalence of OA, it is increasingly important to provide patients with realistic expectations regarding their postoperative quality of life following fracture fixation. Despite the clinical relevance of this issue, 9 current literature on the influence of pre-existing advanced hip OA on specific outcomes such as pain, function, mobility, and overall quality of life following intramedullary fixation remains scarce.7,10-12 The aim of this study was to investigate the impact of pre-existing advanced hip osteoarthritis on both clinical and patient-reported outcomes following intertrochanteric fracture fixation in elderly patients, with the goal of informing clinical decision-making and improving patient expectations.
Objectives
The study investigates the hypothesis that patients with pre-existing OA of the hip who sustain intertrochanteric femoral fractures may experience a reduced quality of life following endomedullary nailing compared to patients without pre-existing OA.
The primary objective is to evaluate the impact of advanced pre-existing hip OA (Kellgren-Lawrence Grad III/IV) on patient-reported outcome measures (PROMs) following endomedullary nailing of intertrochanteric femoral fractures.
Secondary objectives include a comparison of the PROMs of patients with advanced pre-existing OA (Kellgren-Lawrence III/IV) and those with mild or no OA (Kellgren-Lawrence 0-II) as well as to analyze the relationship between PROMs and patient-specific factors such as age, sex, and baseline OA severity.
Primary and Secondary Endpoints
The primary endpoint is the postoperative quality of life in patients with intertrochanteric fractures and pre-existing hip osteoarthritis treated with intramedullary nailing. Quality of life will be assessed using three validated questionnaires: the WOMAC score, the Oxford Hip Score, and the SF-36 score.
Patient responses to these standardized questionnaires will serve as the basis for evaluating the hypothesis and identifying potential influencing factors. Variables expected to influence the primary endpoint include severity of osteoarthritis (Kellgren-Lawrence grade 0-II vs III-IV), patient age and sex.
Methods
In this study the STROBE guidelines have been followed when preparing the manuscript. 13
Study Design
This retrospective, observational, single-center study included patients who were ≥70 years at the time of surgery, had sustained intertrochanteric hip fractures and underwent femoral intramedullary fixation between January 2016 and March 2024. Eligible patients were stratified into two groups based on the radiolographically determined severity of pre-existing osteoarthritis (OA) according to the Kellgren–Lawrence classification (KLC): • Group 1: No/mild OA (KLC grades 0, I, and II) • Group 2: Advanced/severe OA (KLC grades III and IV)
Participants were invited to complete three validated patient-reported outcome measures (PROMs): the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), the Short Form-36 (SF-36), and the Oxford Hip Score (OHS). Questionnaire results were compared between the two groups to assess the potential impact of osteoarthritis severity on postoperative quality of life.
Setting and Participants
A mandatory follow-up period of at least three months was implemented, incorporating both clinical and radiological evaluations, including assessment of fracture consolidation. A complete set of standardized radiographs (pre- and postoperative anteroposterior and lateral views) was available for each patient. Written informed consent was obtained from all participants.
Exclusion criteria encompasses individuals with documented diagnosis of cognitive impairment in patients’ history (precluding comprehension and completing of PROMs), atypical or pathological fractures in conjunction with concomitant pelvic fracture and any documented intra- or postoperative complications (eg, wound infection, migration of blade, implant failure). Withdrawal or absence of general or study-specific informed consent were excluded from the study aswell. Patients who have been prior treated with an arthroplasty have been excluded as well.
Following the institutional database and application of inclusion and exclusion criteria, 66 out of an initial 647 screened patients were eligible for final analysis. Of the original cohort, a total of approximately 42% had to be excluded due to pre-existing cognitive impairment, constituting the largest subgroup among excluded individuals. The overall dramatic decrease is due to a combination of stringent exclustion criteria based on patients characteristics, complications, follow-up data availability, and patients willingness to participate in questionnaires. Each exclusion step significantly reduced the sample size, ultimately leading to a study population of only 21 patients. The inclusion process is illustrated in Figure 1. Inclusion Process of 21 Patients
Surgical Procedure
All patients underwent surgical treatment with either a short Proximal Femoral Nail Antirotation (PFNA, DepuySynthes, Zuchwil, Switzerland) nail or the Trochanteric Fixation Nail Advanced (TFNA, DePuy Synthes, Zuchwil, Switzerland) system. Surgeries were performed under either general or spinal anesthesia with patients positioned supine on a traction table. Intraoperative fracture reduction and implant positioning were guided and documented using fluoroscopy. Postoperative care encompassed full weight-bearing as tolerated for all cases included in the study.
Radiographic Assessment
Preoperative anteroposterior pelvic radiographs were evaluated for the degree of osteoarthritis using the Kellgren–Lawrence classification system via the institution’s Picture Archiving and Communication System (PACS, Deep Unity, DH Healthcare GmbH, Bonn, Germany). Patients were again stratified based on OA severity into: • Group 1: KLC grades 0, I, or II • Group 2: KLC grades III or IV
This grouping was chosen because clinical and radiographic characteristics tend to correlate with disease severity, and such stratification allows for clearer analysis of the impact of OA severity on postoperative outcomes (Figure 2). Examples for the Kellgren and Lawrence Classification at the Hip Joint: Grade 0/I-IV
The present study was approved by the local ethics committee, and informed patient consent was obtained.
Patient Reported Outcome Measures
Patients meeting inclusion criteria were asked to participate in a final analysis by means of completing three questionnaires. These questionnaires were the Western Ontario and McMaster Universities Osteoarthritis (WOMAC) score, the Oxford Hip Score (OHS), and the Short Form 36 (SF-36) score.14-17
The WOMAC-Score evaluates pain, stiffness and physical function in patients with osteoarthritis. The OHS assesses pain and functional ability in daily activies. It consists of 12 items, each scored from 4 to 1, with a maximum score of 48. Higher scores indicate better outcomes. 15 The SF-36 score is a multidimensional measure of health- related quality of life, covering eight domains across 36 items: physical functioning (10 items), role limitaions due to physical health (4 items), role limitations due to emotional problems (3 items), energy/fatigue (4 items), emotional well-being (5 items), social functioning (2 items), pain (2 items), and general health perceptions (5 items). 18 Scores for each domain range from 0 to 100 and are compiled as a percentage. Higher scores reflecting a more favorable health state. 19
All three questionnaires are validated patient-reported outcome measures widely used in clinical research to assess pain, function, and quality of life in patients with hip osteoarthritis and related condition. The WOMAC score has been validated as a reliable and sensitive tool for measuring pain, stiffness, and physical function in patients with OA, demonstrating high internal consistency and construct validity. 20 The Oxford Hip Score has also undergone validation, showing strong reliability, validity, and responsiveness in evaluations hip-specific outcomes following surgical interventions. 21 Similarly, the SF-36 is a valdidated generic helath survey with well-established reliability and validity for assessing overall helath-related quality of life across diverse patient populations, including those with musculoskeletal conditions. 18
Variables
The independent variables include the severity of osteoarthritis (classification grade 0-II or III-IV according to KLC) and demographic factors such as age and gender. The dependent variables indluce patients-reported outcome measures, notably the Oxford Hip Score and the WOMAC Score, with a particulary focus on the pain subcategory. Additionally, radiological indicators of fracture consolidation and the duration of follow-up are considered as outcome parameter.
Bias
Potential bias in this study include selection bias, inherent to the retrospective singe-center design, which may limit the representativeness and external validity of the results. Retrospective data collection could lead to information bias and potentially incomplete or inaccurate data, particulary for patient-reported outcome measuers. Assessment bias is also a concern, as OA severity grading and radiological examinations may involve subject interpretation by the authors. The limited sample size of 21 patients further inceases the risk of statistical imprecision and reduces the generalizability of the results. Furthermore, residual confounding factors such as comorbidities or variations in rehabilitation protocols may not have been adequately controlled and thus influence the observed associations.
Statistical Analysis
The collected data were then subjected to analysis using descriptive statistics. The Shapiro–Wilk test was employed to evaluate the normality of the distribution. For the purpose of comparing the continuous variables across the various groups, the independent Student’s t-test (for normal distribution) and the Mann–Whitney U test (for non-normal distribution) were employed. The chi-square test or Fisher’s exact test (if n < 5) were used for categorical variables. For comparison of three groups, ANOVA (normal distribution) or the Kruksal-Wallis test (non-normal distribution) were used. The assessment of bivariate correlations was conducted by employing the Pearson correlation coefficient (r). Multivariate analyses were performed to assess associations between patient age at surgery and genderm, and Patient reported outcome measures .All statistical analyses were performed in SPSS for Mac (version 23.0; SPSS Inc., Chicago, IL). A significance level of P 0.05 was established for the statistical tests.
Results
Descriptive Data
For the purpose of final analysis, a total of 21 patients with 23 affected hip (mean age 81 ± 7.5, range 70-96 years) were included in the study, with the majority of the sample being female (81%). Accoring to the Kellgren-Lawrence classification, 14 cases were assigned to Group 1 (grades 0-II) and 9 cases to group 2 (grades III-IV). The average follow-up period was 15.1 ± 13.8 months. None of these patients required postoperative revision surgery or reported about a subsequent conversion to an arthroplasty or another surgery of the affected side.
Main Results
Patients’ Demographics Subdivided into Kellgren and Lawrence Classification

No. = number; Yrs. = years.
aGrade of OA was graded from I (mild) to IV (severe) according to the Kellgren Lawrence classification.
bData are presented as mean ± standard deviation. The level of significance was set at P > 0.05.
OA-Grade Specific Results of Affected Hips (Mean ± SD)
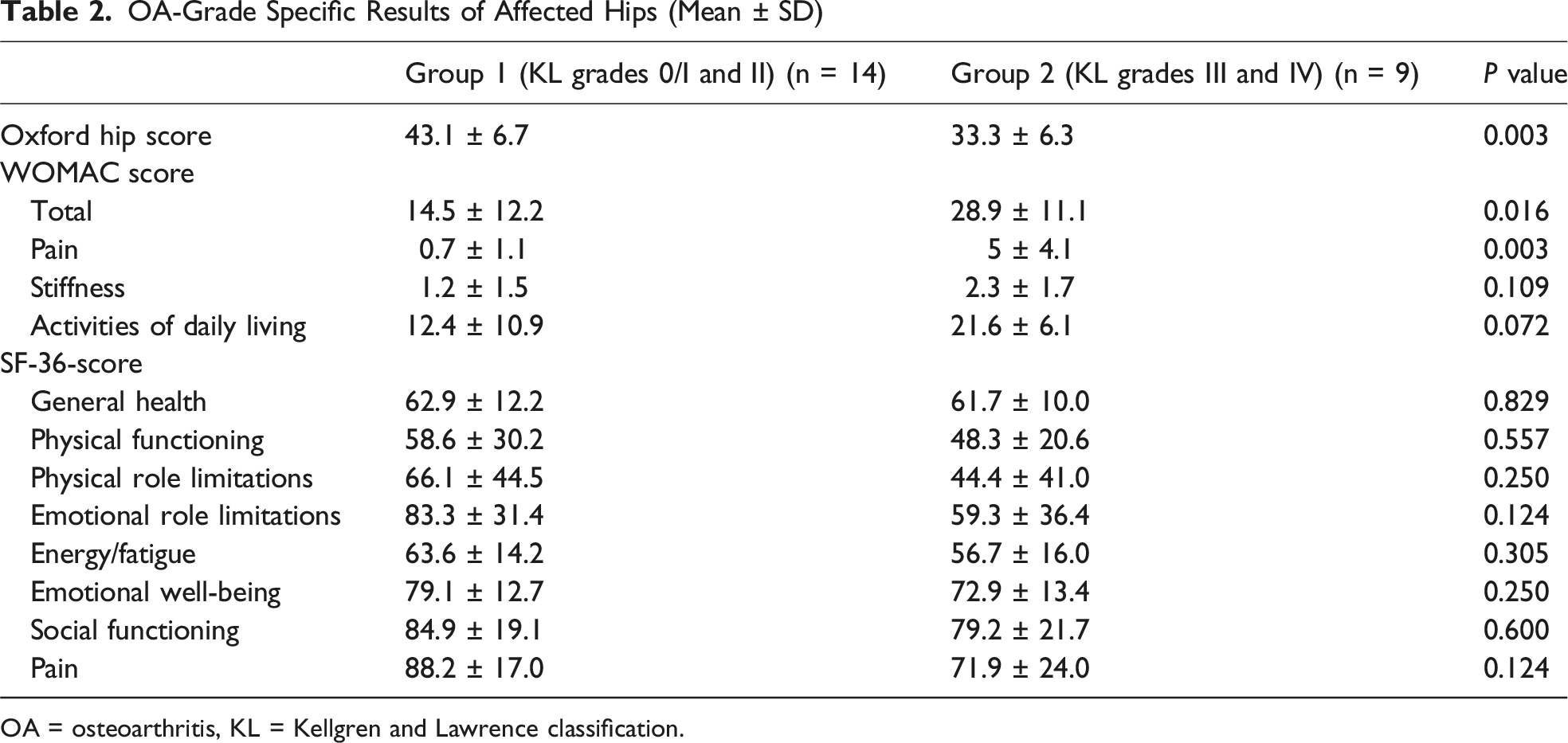
OA = osteoarthritis, KL = Kellgren and Lawrence classification.
Discussion
Key Results
In this study the subjective postoperative outcome of intertrochanteric fractures in elderly patients according to the grade of preexisting osteoarthritis of the hip was examined.
While many studies have analyzed different treatment options of intertrochanteric fractures with hip arthroplasty22-24 or have investigated/intra- vs extramedullary fixation25-28 in unstable fractures, osteoporosis and osteoarthritis, studies still show that internal fixation remains the gold standard.29,30 However, the effect of preexisting osteoarthritis on the quality of life has not yet been analysed in depth and there is little evidence concerning recommendations regarding optimal postoperative strategies.
The results of this study demonstrate that the severity of pre-existing hip osteoarthritis, as classified by the KLC, has a significant impact on the postoperative quality of life of elderly patients treated with intramedullary nailing for IFF. Patients with advanced osteoarthritis (KL grades III-IV) showed significantly worse outcomes in both hip-specific and general health-related quality of life parameters compared to patients with mild or no osteoarthritis (KL grades 0-II). Notably, the OHS was significantly lower in patients with advanced osteoarthritis, indicating poorer hip function and higher symptom burden. Furthermore, the WOMAC score and its subscale for pain were markedly elevated in this group, highlighting the discomfort and mechanical joint limitations that appear to persist even after successful fracture fixation. Importantly, the Activities of Daily Living subscale and SF-36 did not differ significantly. Therefore the SF-36 may data underscore the burden of severe osteoarthritis. These findings suggest that advanced osteoarthritis impairs physical mobility which also has far-reaching effects on psychosocial well-being and participation in daily life.
From a clinical perspective, these findings are particularly relevant. Although intramedullary nailing is an effective method for stabilizing trochanteric fractures, its ability to restore function and relieve symptoms may be limited in advanced osteoarthritis. This underscores the importance of comprehensive preoperative assessment and patient counseling. Elderly patients with severe osteoarthritis should be informed that fracture fixation alone may not sufficiently improve their overall quality of life and that additional treatment strategies—including rehabilitation or even staged arthroplasty—must be considered.
In summary, the severity of pre-existing hip osteoarthritis is a relevant prognostic factor for postoperative outcome after trochanteric fracture fixation. These findings underscore the need for individualized treatment planning and can support shared decision-making between patients and physicians. Further prospective studies are needed to refine treatment approaches for this complex and growing patient population.
Strenghts and Limitations
This study offers several notable strengths. First, by exclusively including patients with radiologically confirmed fracture consolidation, we eliminated a major confounding factor—delayed or nonunion—that can independently influence the postoperative course. Second, the exclusion of patients with cognitive impairment ensured the reliability and validity of patient-reported outcome measures (PROMs), such as the Oxford Hip Score, WOMAC, and SF-36. Third, the use of a comprehensive, multidimensional assessment framework allowed us to capture not only hip-specific function and pain, but also broader aspects of health-related quality of life, including emotional and social functioning. This approach allows for a more holistic understanding of postoperative recovery and patient well-being.
However, several limitations must be considered. Most notably, the small sample size of the study limited the ability to draw definitive conclusions. Due to the advanced age of the initial cohort, increased mortality rates and cognitive impairment were observed during the inclusion process, ultimately leading to a drastic reduction in sample size (Figure 1). The relatively small sample size (n = 21 patients, 23 hips) reduces statistical power and may limit generalizability to broader patient populations. Despite the limited number of patients included in the study, the distribution between the two groups (KLC 1 & 2, KLC 3 & 4) was overall balanced. The retrospective design carries potential selection and information bias, and the single-center design may limit the external validity of the results. Although we controlled for cognitive status and confirmed fracture healing, we did not consider fracture morphology beyond basic classification. Complex fracture patterns—such as inverse fractures or those with severe dislocation—were not analyzed separately, although they may also influence functional outcomes. Finally, potential confounders such as comorbidities, baseline mobility, and adherence to rehabilitation protocols were not systematically controlled and should be considered in future prospective studies.
Interpretation
To our knowledge the existing publications up to date on this relevant topic are limited7,10,11 and each of them have different attempts of analysing this topic.
Consistent with our results, Boese et al 10 demonstrated a significant negative association between radiological OA severity and postoperative outcome in a large prospective cohort (n = 188). They observed that higher Kellgren-Lawrence (KL) grades correlated with lower Harris Hip Scores (HHS) and lower Barthel Index values both 6 and 12 months postoperatively. Importantly, these associations remained statistically significant even after adjusting for confounding variables such as age, ASA score, and cognitive function. This supports the argument that OA severity independently influences recovery potential.
Our study aligns with Boese et al 10 and shows that patients with OA grades III–IV (KL) experience significantly greater functional limitations postoperatively. However, our study involves multidimensional outcome instruments—including the Oxford Hip Score, WOMAC, and SF-36—to assess pain, stiffness, and broader quality of life measures. This comprehensive approach allows for a more detailed assessment of the impact of osteoarthritis on domains beyond physical function, including emotional well-being and social participation. For example, we found significantly worse SF-36 scores in patients with severe osteoarthritis in the domains of physical and emotional role functioning and social interaction—dimensions not captured by either the HHS or the Barthel Index.
Garcia et al 7 similarly reported that patients with advanced radiographic osteoarthritis had reduced functional recovery after internal fixation. However, their study focused primarily on the HHS and EQ-5D, thus providing a narrower view of patient well-being. Although their conclusions regarding the impact of osteoarthritis on physical function are consistent with ours, the extent of patient-reported outcomes in our study provides a more detailed picture of the lived experience after surgery.
In contrast, Fidan et al 11 reported less pronounced differences in outcomes between osteoarthritis severities. Although they found a lower HHS score in patients with severe osteoarthritis, they reported no significant differences in pain scores, EQ-5D general health status, or Barthel Index scores. This discrepancy can be attributed to several factors. First, the study was not limited to patients with confirmed fracture consolidation, so nonunion or delayed fracture healing may have confounded outcome measurements. Second, they did not exclude patients with cognitive impairment, which may have limited the reliability of self-reported measures. Third, the follow-up duration and rehabilitation protocols may have varied and influenced recovery trajectories.
Our study mitigates these limitations by including only patients with radiologically consolidated fractures and excluding individuals with relevant cognitive deficits. This ensures the validity and interpretability of patient-reported outcomes. Furthermore, our relatively long and variable follow-up period (average 460 days) captures both early and late outcomes, thus providing a more comprehensive overview of the postoperative course. In summary, these results support the interpretation that pre-existing osteoarthritis is not merely a radiological background finding but a clinically significant factor that independently limits postoperative function and quality of life. They also suggest that osteosynthesis alone may not adequately address the symptomatic and functional needs of patients with advanced osteoarthritis. This underscores the need for careful preoperative assessment and improved postoperative rehabilitation strategies or even consideration of early secondary arthroplasty for this vulnerable group.
Generalisability
The generalisability of the present study is subject to certain limitations. First, this is a retrospective, single-center analysis with a relatively small sample size (n = 21 patients, 23 hips), the results may not be directly transferable to broader populations. Second, given that the elderly population are often unable to attend follow-up appointments due to disabling medical conditions, dementia and death, the study is more hypothesis-generating in nature than confirmatory. Consequently, no power analysis was conducted. The limited sample size reduces the statistical power of analyses. The small cohort underscores the need for cautious interpretation of the findings and suggests that results should be validated in larger, prospective studies.
Third, there are potential confounders such as comorbidities, pre-fracture mobility, or socioeconomic status were not systematically controlled, which could influence patient-reported outcomes. Nevertheless, the study provides valuable insights into a growing.
Conclusion
The severity of pre-existing osteoarthritis of the hip in patients with trochanteric fractures is a significant risk factor, potentially leading to a diminished quality of life postoperatively. Further studies are necessary to provide therapeutic guidance for this complex and growing patient population.
Footnotes
Ethical Approval
The study was obtained by the local ethical committee and all procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was given by all the patients. Ethics approval was given by the local ethics committee (KEK Zürich, Switzerland, BASEC-Nr. 2023-01679).
Consent for Publication
Informed consent for publication was provided by all participants. All patients who have been included in the study signed the informed consent, the participant information sheet as well as the questionnaires. Only data from patients who have given their fully written permission for pseudonymized use have been utilized.
Author Contributions
S.W. and M.K. conceptualized and designed the study as well as collected and curated the data. M.W. performed data analysis. All authors interpreted the results. S.W. and M.K. wrote the manuscript. M.D. and M.W. critically revised the manuscript. All authors approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.