
Abstract
Objective
The presenting research aimed to assess the clinical results of hip pericapsular nerve group block (PENGB) combined with stellate ganglion block (SGB) on postoperative pain management and early rehabilitation in total hip arthroplasty (THA) patients.
Methods
There were 50 THA cases at our hospital inluded in the study. Twenty-five patients in the experimental group received general anesthesia combined with PENGB and SGB, while the remaining 25 patients in the control group received conventional general anesthesia. Mean arterial pressure and heart rate were recorded 30 min after the start of surgery and immediately postoperatively. The Numeric Rating Scale (NRS) scores for pain at rest and during movement were recorded at baseline (T0), 30 min (T1), 6 h (T2), 24 h (T3), and 48 h (T4) after the combined block was administered. The Athens Insomnia Scale (AIS) scores were recorded for 2 consecutive days postoperatively. Additionally, the number of analgesic pump presses, the time to first mobilization, patient satisfaction scores, and postoperative complications were documented.
Results
Compared with the control group, the experimental group exhibited more stable hemodynamics 30 min after the start of the operation and immediately postoperatively (P < 0.05). At T0, the 2 groups had no significant difference in NRS scores (P > 0.05). However, from T1 to T4, the experimental group had significantly lower NRS scores at rest and during movement, AIS scores for 2 consecutive days post-surgery, achieved earlier mobilization, shorter hospital stays, and reported higher overall satisfaction with hospitalization, all of which were statistically significant (P < 0.05). The postoperative complications rate of the 2 groups were similar (P > 0.05).
Conclusion
PENGB combined with SGB significantly enhances postoperative pain management, shortens hospital stay, and improves early rehabilitation outcomes in elderly patients undergoing total hip arthroplasty compared to conventional general anesthesia.
Keywords
Introduction
Total hip arthroplasty (THA) is one of the most significant medical advancements of the 20th century. In recent years, with the continuous advancements in surgical technology, THA has become a highly effective treatment for hip disorders in the elderly. For hip disorders resulting from infection, trauma, degenerative joint disease, or inflammation, THA can markedly alleviate pain, improve joint mobility, reduce swelling, and restore patients’ ability to perform daily activities and engage in normal physical function.1,2 This is particularly vital for the health and well-being of the elderly population.
Although THA effectively addresses underlying hip joint disorders, achieving optimal therapeutic outcomes remains challenging. Severe postoperative pain and delayed joint function recovery are primary factors that hinder success and significantly impact patients’ quality of life. 3 Elderly patients, in particular, are more susceptible to inadequate postoperative rehabilitation due to weakened muscle strength, limited baseline mobility, and comorbidities. These factors can exacerbate postoperative pain and impede timely, structured, and effective rehabilitation, leading to compromised therapeutic outcomes. 4 As a result, identifying more effective perioperative analgesic strategies and accelerating recovery are critical areas of ongoing clinical research.
To achieve these objectives, various medical interventions have been developed and implemented to alleviate postoperative pain and accelerate joint function recovery following THA. Pericapsular nerve group block (PENGB), a local analgesic technique, has gained recognition among clinicians in hip replacement surgery and has seen widespread use in recent years.5,6 This technique alleviates postoperative pain by blocking the nerve branches that innervate the hip capsule, without impairing the patient’s ability to turn independently, thereby facilitating early postoperative rehabilitation. Stellate ganglion block (SGB), another nerve block technique, primarily targets the autonomic nervous system.7,8 Its role in pain management and rehabilitation has garnered increasing attention in recent years. SGB positively influences pain, circulation, and endocrine function by regulating autonomic nervous system activity, which supports early postoperative recovery.
Although PENGB has been utilized in clinical practice, there are still relatively few studies that specifically analyze its efficacy in THA. Moreover, research examining the combined use of PENGB and SGB, and their synergistic effects on postoperative recovery in elderly THA patients, has not yet been reported. In response to this gap, our study aims to compare conventional general anesthesia with general anesthesia combined with PENGB and SGB in terms of postoperative pain, functional recovery, and quality of life. This will allow us to evaluate the effectiveness of the combined block technique and ultimately provide new therapeutic options and strategies for the rehabilitation of elderly patients following THA.
Methods
Inclusion, Exclusion, and Grouping of Patients
Patients diagnosed with hip disorders and requiring THA between January 2023 and September 2024 were included. A approval of Clinical Medicine Research Ethics Committee of our hospital, with ethics approval number Lunke [2023] No. 297.
Inclusion criteria: Patients requiring THA; aged 65 years or older; ASA grade II to III; no severe cardiovascular disease, severe respiratory disease, or liver and kidney dysfunction; a subjective willingness to accept PENGB combined with SGB for analgesia and adjunctive rehabilitation; signed the informed consent form for the procedure, agreed to be included in the study, and adhered to the research protocol.
Exclusion criteria: Patients with severe cardiovascular disease, severe respiratory disease, liver and kidney dysfunction; patients with multiple neurological disorders who are unable to cooperate; patients with severe coagulopathy or inflammation, edema, or infection at the puncture site; patients with related allergy history or severe intolerance.
The patients were numbered, and then selected using the random number table method. All patients were then randomly chosen for experimental group or control group (25 cases in each group). A double-blinding method was implemented to keep trial participants and investigators unaware of the assigned intervention during data collection and processing.
Anesthetic Drugs and Methods
Upon entering the anesthesia room, the patient’s basic vital signs were routinely monitored, along with invasive arterial blood pressure, BIS (45-55), and cerebral oxygen saturation (60-80%).
Anesthesia induction: Etomidate 200-600 µg/kg, sufentanil 0.1-2 µg/kg, rocuronium bromide at 2 times ED95, followed by the placement of an appropriate laryngeal mask. Anesthesia maintenance: Remifentanil 0.05-0.25 µg/(kgh), propofol 1.5-4.5 mg/(kgh), sevoflurane 1-2.5%, cisatracurium 0.06 mg/(kgh).
At the end of the surgery, the relevant anesthetic maintenance drugs were discontinued, and the patient was transferred to the recovery room with the laryngeal mask in place for a smooth transition. No anesthetic antagonists were administered, and the laryngeal mask was removed once the patient was fully awake.
PENGB and SGB Procedure
PENGB (Figure 1A) was performed under ultrasound guidance using a high-frequency linear probe (8-15 MHz) placed transversely at the midpoint between the ASIS and pubic symphysis. The needle was inserted at the lateral one-third–medial two-thirds junction of this line, targeting the fascial plane between the deep iliopsoas tendon and anterior hip capsule. The probe was positioned below the ASIS and adjusted to visualize the iliopsoas tendon in cross-section. Following hydrodissection confirmation, 15-20 mL of 0.25-0.375% ropivacaine was injected into the plane. Ultrasound Imaging Demonstrating the Procedures of PENGB and SGB. A: Ultrasound View During the PENGB Procedure, FA: Femoral Artery, ITP: Ilipsoas Tendon, AIIS: Anterior Inferior Iliac Spine, Asterisk: Needle tip; B: Ultrasound View During the SGB Procedure, SCM: Sternocleidomastoid Muscle, CA:Carotid Artery, CV:Jugular Vein, LC:Long Neck Muscle
SGB (Figure 1B) was performed via the classical anterior (paratracheal) approach. With the patient supine and neck extended, the C6 transverse process was identified at the lateral cricoid cartilage. After lateral displacement of the carotid artery, a needle was inserted between the trachea and carotid sheath to contact the C6 anterior tubercle, then withdrawn 1-2 mm. Ropivacaine (3-5 ml, 0.2-0.375%) was slowly injected over >1 min. Block efficacy was confirmed by Horner’s syndrome.
Postoperative Management
Immediately following the surgery, the patient was connected to the patient-controlled intravenous analgesia (PCIA) device, and the research team meticulously recorded the number of effective analgesia pump presses within the first 48 h. The analgesic formula consisted of sufentanil 2 µg/kg and tropisetron 6-8 mg. The protocol included no initial loading dose or background infusion; the self-controlled dose was set at 2 mL per administration, with a lockout time of 25 min. For temporary analgesic supplementation, flurbiprofen axetil 50 mg was administered as needed.
Drawing on clinical experience and a detailed evaluation of the effects of various anesthesia techniques, this study adopts a multidimensional approach—utilizing multiple outcome measures to comprehensively assess both short- and long-term effects. Specifically, the mean arterial pressure (MAP), together with the heart rate (HR), were documented 30 min after the commencement of surgery and immediately upon its completion. The Numeric Rating Scale (NRS) scores for pain at rest and during movement (turning) were recorded at several time points: before the nerve block (T0), 30 min after (T1), 6 hours after (T2), 24 h after (T3), and 48 h after (T4). NRS scores ranged from 0 (no pain) to 10 (unbearable pain). Additionally, the Athens Insomnia Scale (AIS) scores were recorded on the first and second days post-surgery (0-4 indicating no sleep disorder, 4-6 indicating suspected insomnia, and 6 or more indicating insomnia).
Time to first mobilization was recorded. Criteria included: (1) Independent Standing—SLR of the affected limb with quadriceps strength ≥Grade 4; (2) Pain Control—resting VAS ≤ 3, standing VAS ≤ 5, and no sharp pain or joint instability.
Ambulation Tolerance: Patients walked 3-5 meters with a walker. Ambulation was halted if VAS ≥ 7 or compensatory gait appeared. Hemodynamic criteria: HR increase ≤20%, SBP change <20 mmHg, no orthostatic symptoms.
Rehabilitation Protocol
Phase I (0-24 h): DVT prevention, joint mobilization via hourly ankle pumps, quadriceps sets (4 × 15/day), and bedside sitting (from 6 h, 3×/day).
Phase II (24-72 h): Mobilization training with twice-daily 30-min PT, active hip ROM (flexion 0-60°, abduction 0-30°), TDWB only.
Phase III (72 h-2 weeks): Functional recovery via 45-min daily PT, balance/stair training (step ≤ 10 cm), and progressive weight-bearing (+25%/week).
Additional Measures: Analgesic pump usage, patient satisfaction (scale 1-10), and postoperative complications were recorded.
Statistical Analysis
Based on the results of a preliminary experiment involving 20 cases (10 cases per group), the NRS scores at 6 h post-surgery were (3.10 ± 0.994) in the control group and (2.10 ± 0.738) in the experimental group. With an alpha (α) level of 0.05 and a power (1-β) of 90%, and accounting for a 20% lost visit rate, 9 the required sample size was calculated to be 25 for each group using PASS 15.0.
This study utilized the intention-to-treat (ITT) analysis, all data were analyzed by SPSS 26.0. Data conforming to a Gaussian distribution were expressed as mean ± standard deviation (±s), and inter-group comparisons were performed using the t-test. Continuous data that did not meet the Gaussian distribution criteria were presented as medians and quartiles [M(Q1, Q3)], with inter-group comparisons made using the Mann-Whitney U test. For intra-group comparisons, the Friedman M rank sum test of K related samples was employed. Interaction analysis was conducted using a generalized estimating equation for repeated measures. Binary data were expressed as counts or percentages, with inter-group comparisons conducted using either the chi-square test or Fisher’s exact test. All tests were two-sided, and a P-value < 0.05 was considered statistically significant.
Results
No Significant Differences Were Found Between the Two Groups in Baseline Characteristics
Comparison of Baseline Characteristics of Patients (n = 50)

“-” Fisher’s exact probability method is used. The P-values for the significance tests are all two-tailed.
The Heart Rate and Blood Pressure of the Experimental Group Were Significantly Lower in the Short Term After Surgery
Comparison of HR and MAP (n = 50)

Note: *: P < 0.05 (two-tailed test).
The Experimental Group Demonstrated Significantly Lower Pain Levels Within the First 2 days Postoperatively
Comparison of NRS Scores of Resting and Turning Over at Different Time Points (n = 50)
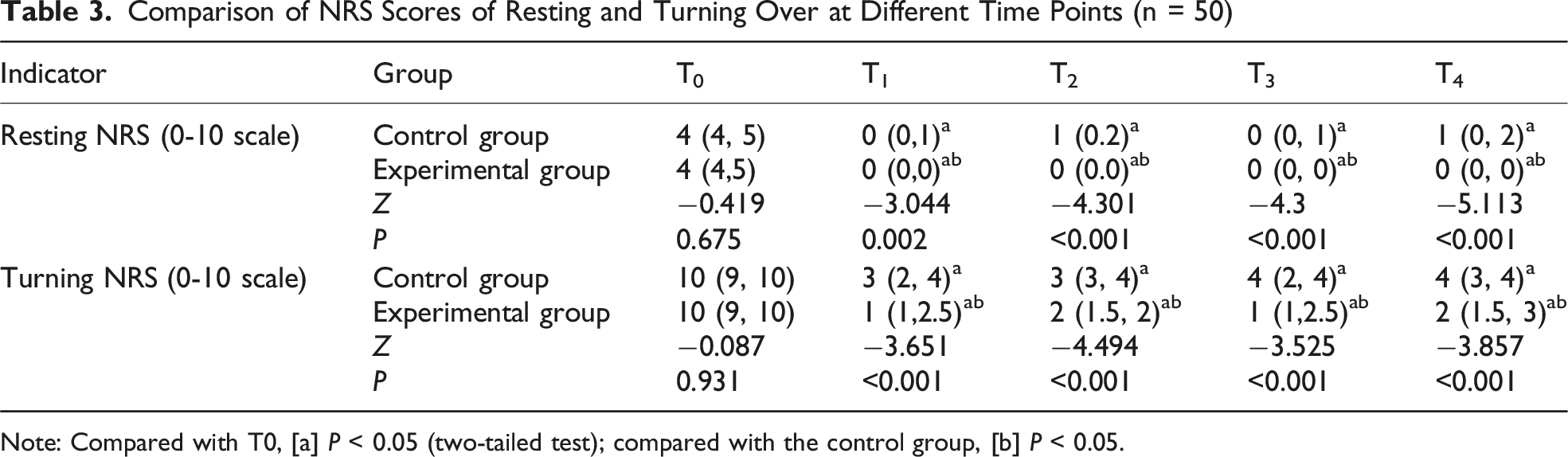
Note: Compared with T0, [a] P < 0.05 (two-tailed test); compared with the control group, [b] P < 0.05.

Comparison of NRS Scores Between the Two Groups at Different Postoperative Time Points in Resting and Turning States (n = 50, mean ± SD, **: P < 0.01, Two-Tailed Test; The Error Bars in the Figure Represent Standard Deviations). A: Resting state; B: Turning State
The Experimental Group had a Shorter Hospital Stay and Experienced a Faster Recovery of Postoperative Mobility and Daily Living Abilities
Comparison of Postoperative Rehabilitation and Patient Satisfaction (n = 50)

Note: The P-values for the significance tests are all two-tailed.
The Complication Rate in the Two Groups had No Significant Difference
Comparison of Postoperative Complications

Note: Fisher’s exact probability method. The P-values for the significance tests are all two-tailed.
Discussion
Effective postoperative pain relief, along with the recovery of motor function and daily living abilities, is crucial for optimizing the therapeutic outcomes of THA and remains a central focus of ongoing research.12,13 Numerous studies have demonstrated that effective pain management strategies can significantly accelerate postoperative functional recovery, potentially leading to improved therapeutic outcomes.14-17 Currently, no clinical studies have specifically examined the combined use of PENGB and SGB in the postoperative management of THA patients. This study employed a randomized controlled trial design to ensure the reliability and validity of the findings. Blinding of the medical staff involved in data collection and analysis further enhanced the study’s objectivity. The results demonstrate that, in elderly patients undergoing THA, the use of PENGB combined with SGB as an adjunct to general anesthesia significantly improves postoperative pain management and promotes early recovery compared with conventional general anesthesia. These findings offer new insights and approaches for the postoperative rehabilitation of elderly patients undergoing THA.
The study results demonstrated that the experimental group outperformed the control group across several key indicators. Firstly, circulatory stability was superior in the experimental group both 30 min post-surgery and at the end of surgery, suggesting that this combined block technique offers advantages in maintaining perioperative circulatory stability. Secondly, the NRS scores from T1 to T4, whether at rest or during movement, were consistently lower in the experimental group, highlighting more effective pain management. Moreover, compared with other published studies on PENGB in THA, the combined PENGB + SGB strategy used in our study also demonstrates unique advantages, as it is associated with milder postoperative pain within the first 48 h than that reported in patients who received PENGB alone. 18 Additionally, patients in the experimental group experienced less postoperative insomnia, an earlier first ambulation, shorter hospital stays, and higher overall satisfaction, all indicating a marked improvement in early rehabilitation outcomes. Although the incidence of postoperative complications did not differ significantly between the 2 groups, these positive rehabilitation outcomes substantially enhance patients’ postoperative quality of life and overall surgical experience.
Most elderly patients requiring THA due to hip trauma or degenerative conditions often present with multiple comorbidities. Managing severe postoperative pain is a significant challenge, as it can severely impact the physiological functions of these patients. Effective perioperative analgesia and adequate sleep are crucial for their rapid recovery. PENGB offers a targeted approach to alleviate postoperative pain19-21 by blocking the sensory nerve branches surrounding the hip capsule, allowing early postoperative rehabilitation and movement without compromising recovery. Its clinical benefits are well-documented.
SGB is a minimally invasive technique to modulate autonomic nervous system activity,22,23 stabilize the internal environment, and reduce inflammatory responses and pain perception.24,25 Additionally, SGB has been confirmed to dilate blood vessels, enhance perioperative cerebral blood flow in elderly patients, and decrease the incidence of perioperative cognitive dysfunction. It has also been used to treat cardiovascular conditions such as post-traumatic stress disorder, hypertension, angina, and refractory arrhythmias.26,27 By regulating sympathetic nerve function, SGB can mitigate postoperative issues like pain, tension, and anxiety, which often hinder normal sleep in elderly patients. 28
The combined application of PENGB and SGB forms a key component of multimodal analgesia, providing not only more effective pain control but also reducing postoperative tension and anxiety in the elderly. This approach accelerates patient recovery, shortens hospital stays, and ultimately offers significant economic benefits to society.
In elderly patients, effective pain management and rapid recovery following THA are of paramount importance. The PENGB specifically targets the surgical area, significantly reducing local pain perception, while the SGB modulates the autonomic nervous system, exerting broader effects on circulation and the endocrine system. Together, these techniques synergistically enhance the recovery of postoperative physiological function.
This dual nerve block technique not only reduces the dependency on analgesics and lowers the risk of opioid-related side effects but also expedites the recovery of physical function, facilitating earlier mobilization following THA. Postoperative pain often discourages elderly patients from moving, and extended bed rest significantly heightens the risk of complications, including urinary tract infections, pressure ulcers, muscle atrophy, deep vein thrombosis, pulmonary embolism, and pneumonia. 29 These complications not only jeopardize physical health but also detrimentally affect the patient’s quality of life and psychological well-being. Thus, meticulous postoperative pain management is essential for the swift and effective recovery of elderly patients, ensuring both their physical and mental well-being during the rehabilitation process. 30 It is also noteworthy that the synergistic mechanism between SGB and PENGB may involve multiple pathways, such as the attenuation of neuropathic pain via sympathetic inhibition or the improvement of sleep quality through autonomic modulation. These underlying mechanisms hold promise for future validation through biomarkers such as serum cortisol levels. Such investigations may provide a more comprehensive understanding of the synergistic effects and pave the way for further optimization of this combined therapeutic approach.
This study has several limitations. Despite rigorous sample size estimation, the cohort remains relatively small, potentially limiting statistical power. Future studies will expand both sample size and age range to improve generalizability. Additionally, this study focused on short-term postoperative outcomes following THA, without long-term follow-up; subsequent research will assess the sustained effects of combined PENGB and SGB. The potential synergistic mechanisms between the 2 blocks were not investigated and warrant further exploration. Lastly, the absence of any nerve block in the control group may affect the interpretability and robustness of the comparative findings.
Conclusion
The combination of hip joint capsule nerve block and stellate ganglion block as an adjunct to general anesthesia offers a novel and effective approach for pain management and early rehabilitation following total hip arthroplasty in the elderly. This technique significantly enhances perioperative quality of life by improving postoperative pain control, reducing hospital stay, and increasing overall patient satisfaction. As further clinical studies continue to develop, this promising approach is likely to become more widely adopted, emerging as a key strategy in pain management within clinical anesthesia practice, ultimately providing elderly patients with a safer and more comfortable rehabilitation experience.
Footnotes
Acknowledgement
All authors sincerely thank the Anhui Provincial Health Commission for their funding.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study is approved by the Ethics Committee of The First Affiliated Hospital of Bengbu Medical University ([2023] No. 297), Written informed consent was obtained.
Consent for Publication
Informed consent was obtained from all individual participants included in the study.
Author Contributions
Guarantor of integrity of the entire study: Di Liu, Congli Zhang, study concepts: Yunzhi Ling, study design: Wentao Dai, literature research: Nannan Song, experimental studies: Di Liu, data acquisition: Meijun Shen, data analysis: Di Liu.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding by Anhui Provincial Health Funding Project (based on the “imbalance of glycolysis and oxidative phosphorylation” to study on the protection mechanism of dexmedetomidine against ischemia and reperfusion injury of renal tubular epithelial cells) (No. AHWJ2022b024)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors declare that there are no conflicts of interest regarding the publication of this paper.
Data Availability Statement
The simulation experiment data used to support the findings of this study are available from the corresponding author upon request.