
Abstract
Introduction
The purpose of this study was to describe how hip fractures differentially affect male and female patients regarding fracture pattern, hospital course, and postoperative course.
Materials and Methods
This retrospective case series was performed in a metropolitan healthcare system involving 2996 hip fracture patients >59 years old who underwent surgical management (eg, intramedullary nail, hemiarthroplasty, percutaneous pinning, etc.). Male patients were matched to female patients using 1:2 nearest neighbor matching on the basis of age and Charlson Comorbidity Index. Outcomes of interest included AO/OTA fracture classification, 30- and 90-day readmission, and 30-day and 1-year mortality rates.
Results
The cohort was predominantly female (64.5%). Female patients were more likely to sustain a type 31A fracture compared to males (P = .016). The average CCI was higher for males vs females (3.0 ± 2.5 vs 2.6 ± 2.3, P < .001). Males were more likely to be readmitted at 30 (P < .001) and 90 (P = .015) days after discharge. The 30-day mortality was higher for males vs females (6.6% vs 4.5%, P = .015). Approximately 19.9% of male patients vs 15.1% of females died within a year of surgery (P < .001). The average time to surgery was longer for males vs females (23.8 ± 18.8 vs 22.5 ± 21.9 h, P = .048). Males were more likely to die within a year if they underwent surgery >24 h after admission (P = .029).
Discussion
Hip fractures have different implications for male and female patients. With age, the incidence of IT fractures increased in females, while it decreased in males. On average, males with hip fractures are sicker than females, which likely contributes to the longer time to surgery as well as increased readmission and mortality rates seen in males.
Conclusions
Male and female hip fracture patients are not similar in baseline health status, fracture pattern, or postoperative morbidity and mortality. Orthogeriatricians and other providers that care for this patient population should be aware of these differences when implementing treatment strategies to optimize the recovery of their patients, and while educating patients and their families about postoperative expectations.
Introduction
Hip fractures are one of the most common injuries in the older adult population. In the United States there are approximately 325,000 hip fractures annually, with the majority of them occurring in females (66.7%). 1 They are associated with significant morbidity, mortality, and can have substantial effects on a patient’s quality of life.2-6 There are 3 major groups of hip fracture patterns based on anatomic location consisting of femoral neck, intertrochanteric (IT), and subtrochanteric hip fractures. IT fractures are the most common and account for approximately half of all hip fractures in the older adult population. 7 These fracture patterns can have implications related to treatment strategies, and potentially patient morbidity and mortality.
Previous literature has shown there are differences in mortality by patient sex in hip fracture patients, with males typically having more comorbidities and higher mortality rates compared to females.8-13 IT fractures have been demonstrated to be found more commonly in female patients compared to male patients, however these studies were conducted in populations outside the United States, or in small cohorts.14-16 Additionally, there is a paucity of literature describing readmission rates, and the effect of the duration of time to surgery on patient mortality by patient sex. Only one previous study has evaluated time to surgery by sex on patient mortality, however, this was only at 30 and 90 days postoperatively. 17
As healthcare providers that treat hip fractures seek to provide effective, high-quality care to their patients, it is imperative to understand how hip fracture care and outcomes may differ by patient sex. The purpose of this study was to further characterize how hip fractures differentially affect males and females regarding fracture pattern, hospital course, and postoperative course. Secondary aims include determining predictors of mortality for hip fracture patients according to biologic sex. The primary outcomes of this study included AO/OTA fracture classification, readmission, and 30-day and 1-year mortality rates. Secondary outcomes included time to surgery, hospital length of stay (LOS), and discharge destination.
Materials and Methods
This study was deemed exempt from review by the institutional review board due to its retrospective nature. All research was carried out according to the Declaration of Helsinki. Patient consent was not required for this retrospective review. A retrospective review of a metropolitan healthcare system’s electronic medical record was conducted. All surgically treated hip fractures from 2010-2022 were identified through the use of Current Procedural Terminology (CPT) codes. The following CPT codes were used: 27235, 27236, 27238, 27244, and 27245. Hip fractures were further classified based on anatomic location of the hip fracture using the AO/OTA Classification, which characterizes fractures in the intertrochanteric region as 31-A, 31-B and 31-C, and those in the diaphysis as type 32 (Figure 1). Patients receiving nonoperative treatment, revision procedures, concomitant procedures on the pelvis (ie, anterior column, posterior column ORIF etc.) excluding arthroplasty, and aged 59 and younger were excluded. Diagram of AO/OTA classification of hip fractures. (A) Type 31-A fracture pattern demonstrating simple fracture of the trochanteric region, including intertrochanteric fractures, greater trochanteric fractures, and lesser trochanteric fractures. (B) Type 31-B fracture pattern involving the femoral neck from the intertrochanteric line to the articular cartilage of the femoral head. (C) Type 31-C fracture pattern involving the femoral head.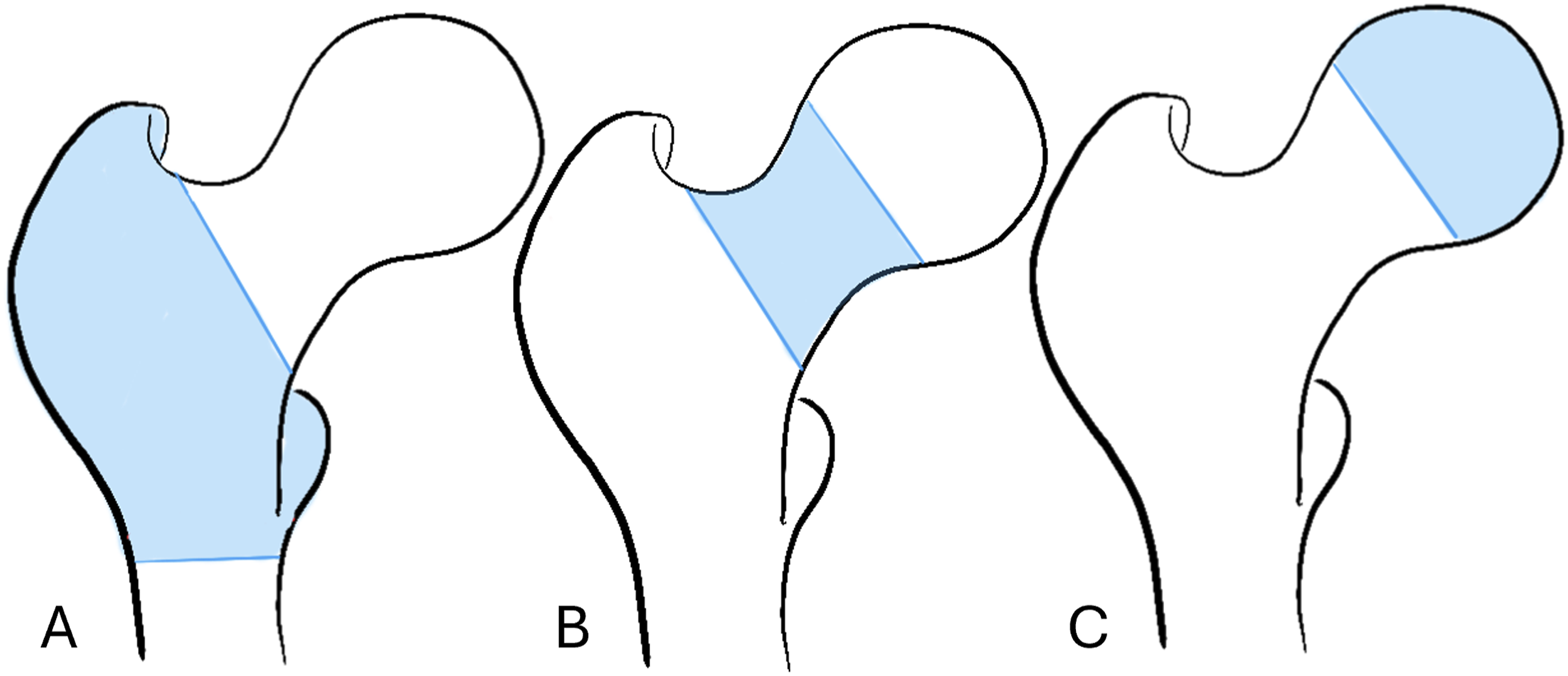
Evaluated baseline patient characteristics included: age, sex, body mass index (BMI), Charlson Comorbidity Index (CCI), and fracture pattern. Outcomes assessed included time to surgery, hospital LOS, discharge destination, readmission, and mortality.
Statistical Analysis
Data was analyzed using Intellectus Statistics (Clearwater, FL) and R (Indianapolis, IN). Male and female patients were matched using 1:2 nearest neighbor matching on the basis of CCI and age. A point-biserial correlation was first evaluated to determine what hip fracture variables correlated with sex. Chi-square test of independence and Fisher exact tests were used for categorical variables. Two-tailed independent t-tests were conducted as appropriate. Additionally, a logistic regression analysis was conducted to evaluate predictors of 1-year mortality. Variables included in this analysis were sex, BMI, age, CCI, hours to surgery, discharge destination, and fracture pattern. Significance was set to P ≤ .05.
Results
A total of 2996 patients were included for analysis. The majority of patients were female (n = 1,932, 64.5%). The average age at the time of admission was 80.7 ± 9.5 years old with a BMI of 24.1 ± 7.6, and a CCI score of 2.8 ± 2.4. The most common fracture pattern was 31B (n = 1562, 52.1%), followed by 31A (n = 1285, 42.9%). Most patients were treated with an intramedullary nail (n = 1592, 51.0%), followed by hemiarthroplasty (n = 1033, 34.5%). The 30-day and 1-year mortality rates were 5.2% (n = 157), and 16.8% (n = 508), while the 30-day readmission rate was 17.9% (n = 537). Patients with a longer hospital LOS, as well as with a discharge destination of a specialized nursing facility (SNF) were more likely to die within a year (P < .001).
Characteristics of Hip Fracture Patients by Sex.

Continuous data is reported as mean ± standard deviation. Categorical data reported as N/n (%).
aCOVID-19, coronavirus disease.
bBMI, body mass index.
cLOS, length of stay.
dSNF, skilled nursing facility.
eIncludes against medical advice, transfer to another hospital, hospice, or inpatient mortality.

Hip fracture patterns by age and patient sex.
Although the average hospital length of stay for males was not significantly different from females (P = .111), males were significantly more likely to be readmitted at 30 (P < .001) and between 30 and 90 (P = .015) days after discharge. There was no difference in proportion of males vs females that were discharged home (n = 185, 17.4% vs n = 294, 15.2%, P = .121). The 30-day and 1-year mortality rates were higher for males compared to females (30-day: 6.6% vs 4.5%, P = .015, respectively; 1-year: 19.9% vs 15.1%, P < .001, respectively). The average time to surgery was longer for males vs females (23.8 ± 18.8 vs 22.5 ± 21.9 h, P = .048), with approximately 33.7% of male patients proceeding to surgery 24 h or greater after admission vs 30.9% of females (P = .104) (Table 1). Males were significantly more likely to die within a year if they underwent surgery >24 h after admission (P = .029) (Figure 3). One-year mortality rates for patients who underwent surgery more than 24 h after presentation.
Predictors of 1-Year Mortality in Hip Fracture Patients.
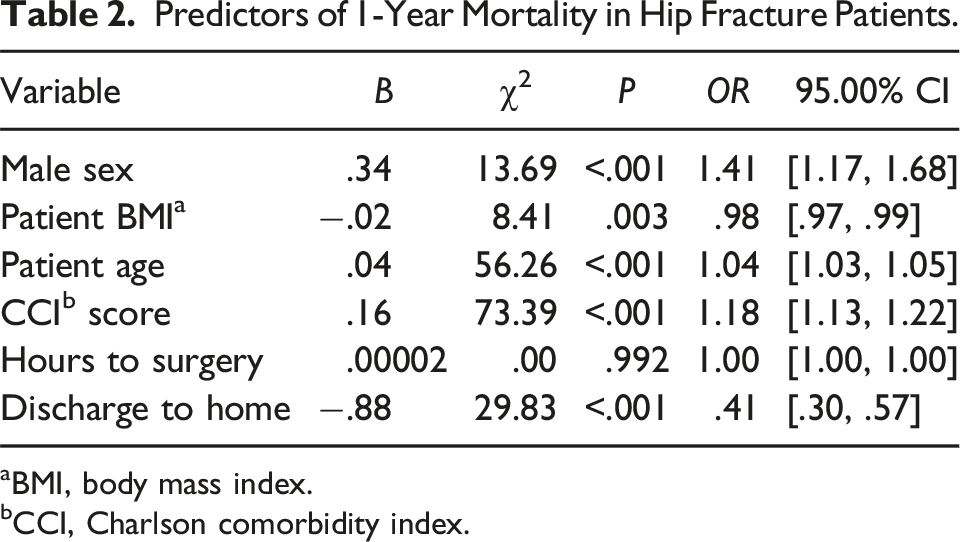
aBMI, body mass index.
bCCI, Charlson comorbidity index.
Discussion
Hip fractures are one of the most common injuries among the older adult population in the United States. Despite the commonality of this pathology, few studies have analyzed differences in the presentation and course of care of these patients stratified by sex. This study evaluated differences among hip fracture patients by sex, with particular emphasis on patterns, hospital course, and postoperative care up to 1-year follow-up. Although femoral neck fractures were the most common among males and females, females were more likely to present with an IT fracture compared to males (P = .003). Fracture pattern was not found to be associated with patient mortality (P > .113). 30-day and 1-year mortality rates were higher in males (30-day: 6.6% vs 4.5%, P = .015, respectively; 1-year: 19.9% vs 15.1%, P < .001, respectively). Despite LOS being equal between the groups (P = .106), the average time to surgery was 1.3 hours longer for males compared to females (P = .048), with approximately one third of patients proceeding to surgery after 24 h. Those male patients who underwent surgery more than 24 h after admission demonstrated a significantly higher 1-year mortality rate (P = .029). Male patients were more likely to be readmitted within 30 and 90 days (P < .001, P = .015, respectively) after discharge. In multivariate analysis, discharge destination, followed by patient sex were found to be the greatest predictors of 1-year mortality. Hip fractures will continue to be a common injury in the older adult population, making this information important to those involved in hip fracture care as they counsel, tailor treatment plans, and help establish the goals of care with their patients.
Hip fracture patterns have been shown to vary by patient sex.14-16 One study evaluated 2150 patients and found that for males and females, the proportion of IT fractures relative to femoral neck fractures increases with age. 14 When stratifying by gender, in females the trend is also true, but in males the proportion of IT fractures decreased with age relative to femoral neck fractures. 14 The same group extrapolated the study design to a national level in Canada and evaluated 102,842 hip fractures. 15 They found that the proportion of IT fractures relative to femoral neck fractures in females increased from 35% to 51% of hip fractures as patient age increased from the youngest (55-59 years) to oldest (84+) groups. In contrast, male hip fracture patterns remained constant when comparing age groups. 15 The current study similarly found IT hip fractures to increase with age in both groups. IT fractures were also shown to occur more often in female patients, and the proportion of IT fractures relative to femoral neck fractures increased by age group in females, however the proportion of IT fractures decreased in males. This has been postulated to be related to the higher prevalence of osteoporosis among females compared to males, with IT fractures being more associated with lower trabecular bone mass. 15 This has implications for hip fracture prevention and course of care.
A hip fracture patient’s hospital course has been shown to affect patient complication and mortality rates.17-20 Increased time to surgery has been associated with higher 30- and 90-day mortality rates, 17 specifically in male patients and those with more comorbidities. The current study also demonstrated that undergoing surgery greater than 24 h after presentation was associated with increased mortality as much as one year after surgery in male hip fracture patients. This delay in time to surgery may be due to time required for patient optimization due to the increased burden of comorbidities in males compared to females. Increased LOS has also been shown to be associated with increased 4-month mortality risk even after controlling for patient characteristics. 20 Although this study did not find a difference in overall LOS between sexes, this study did find longer LOS to be associated with higher 1-year mortality rate.
Male hip fracture patients have been shown to have more medical complications as well as higher mortality rates compared to female hip fracture patients.8-13 One study found a mortality rate of 16.5% for males and 9.4% for females at 1 year. 12 They found that males had higher ASA scores compared to women which is similar to the current study which shows males having higher CCI scores at baseline. 12 Type 1 and 2 diabetes mellitus have been shown to elevate risk of hip fractures in both males and females, with associated increased mortality. 21 Patients with diabetes have higher median CCI scores and are more likely to sustain intertrochanteric and subtrochanteric hip fractures.21,22 Males have also been shown to have worse cognition and be less physically active compared to female patients. 11 Additionally, pre-fracture ability to perform activities of daily living is associated with 1-year mortality in women while readmission within 6 months was associated with 1-year mortality in men. 23 Another study found that males were 2 times as likely to die in the first 2 years after hip fracture compared to females, which they mostly attributed to infections (pneumonia, influenza, and septicemia). 10 Other comorbidities such as respiratory disease, malignant neoplasm, and circulatory disease have been associated with the increased mortality rate in males also. 8 The current study found a significantly higher mortality rate among males, as well higher 30- and 90-day readmission rates. Thirty-day readmission was associated with higher 1-year mortality in women. The current study also found discharge destination and patient sex to be the largest predictors of 1-year mortality, while fracture pattern did not contribute. This may indicate that the relatively higher burden of comorbidities among male hip fracture patients may explain the large difference in mortality. Interestingly, more male patients have been shown to live with someone else and be more dependent on others to carry out activities of daily living compared to females, 12 further demonstrating the relatively worse baseline health found in male hip fracture patients. Patients and physicians should be particularly cognizant of the large differences in functional and medical-related concerns when treating male hip fracture patients.
Within our institution, the pathway for orthogeriatric patients involves the orthopaedic surgery team and the hospitalists that partner in patient admission and care delivery. Rather than one assigned team leading care, there is a collaborative approach between the orthopaedic surgeon, hospitalists, and advanced practitioners that specialize in inpatient orthopaedic care. All involved providers share responsibility for orders and patient care coordination throughout the hospital stay. Following discharge, patient care is coordinated by an orthogeriatric mobile outreach team consisting of 2 nurse practitioners and a physician’s assistant who do home visits for all follow-up care. As transitions from place to place can be disorienting and confusing for this population, the coordinated mobile outreach team provides reliable care without the need for travel and keeps patients in a more comfortable “home” setting. Additionally, all patients, regardless of age, that get evaluated for hip fracture undergo a bone health evaluation and consult with orthopaedic providers trained in bone health education and osteoporosis evaluation. We believe it is important for all providers that participate in patient care throughout the episode of care to understand and be able to educate patients regarding expected recovery, as well as associated morbidity and mortality. The results of this study provide a more complete understanding of postoperative care pathways and expectations for both patient and provider alike.
Hip fractures in older adults continue to be a public health concern around the world. Hip fracture prevention is critical for maintaining patients’ quality of life and reducing healthcare spending.6,24,25 This study highlights that prevention strategies could be adjusted based on patient sex, due to IT fractures more likely occurring in females, and femoral neck fractures more likely occurring in males. With IT fractures’ association with osteoporosis, 15 females may need additional attention surrounding bone health and osteoporosis, while males may require more time for patient education on fall prevention, exercises, improving balance, or home modifications. All patients regardless of sex can benefit from vitamin D supplementation which has been shown to reduce fall and fracture risk, however this has yet to be stratified by specific fracture pattern. 26 Although certain hip fractures were shown to be more common in each sex, physicians should determine what strategy is most appropriate for each individual patient. Future studies are needed to determine whether sex-specific hip fracture prevention protocols may provide additional benefits to patients.
Study Strengths and Limitations
This study had several strengths and weaknesses. The size of the study cohort allowed for an appropriate evaluation of the differences in the 1-year episode of care for male and female hip fracture patients. Additionally, matching male to female patients on the basis of CCI and age allowed for additional control of possible confounding variables. CCI is a well-validated tool and has been demonstrated to correlate with mortality in patients over 65 that sustain hip fractures.27-29 The 17% 1-year mortality presented within this study is consistent other literature regarding this patient population. Shin et al demonstrate an 18% 1-year mortality rate among operatively treated hip fracture patients in a recent large retrospective review from an academic level 1 trauma center for patients over 65 years of age. 30 Another recent study demonstrated a 16.6% 1-year mortality rate in a large prospective cohort analysis for hip fracture patients over 65, excluding pathologic and periprosthetic fractures. 31 According to the authors’ knowledge, this is the first study in the United States to evaluate for fracture pattern differences by patient sex. Due to the retrospective nature of this study, the results rely upon accurate documentation in the medical record. This study was conducted within a single healthcare system which may limit the generalizability of the results. Patient populations can widely vary across the United States, but we believe this study can be used to promote future discussions and evaluate for differences by patient sex on a national scale.
Conclusions
Hip fractures continue to be one of the most common and devastating injuries experienced by older adults. This study found that male patients were typically sicker, were more likely to take longer proceeding to surgery, and experienced higher 30-day and 1-year mortality rates compared to females. Male patients were more likely to be readmitted within 30 and 90 days as well. Overall, femoral neck fractures were the most common, however, as age increased, IT fracture incidence increased in females and decreased in males. Male and female hip fracture patients are not similar in baseline health status, fracture pattern, or postoperative morbidity and mortality. Orthogeriatricians and those that care for hip fracture patients should be aware of these differences when implementing treatment strategies in order to optimize the health and recovery of their patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Cunningham’s spouse is the CEO and founder of CODE Technology. Dr Cunningham is a member of the AAOS Health Care Systems and Patient-reported Outcome Measures Committees as well as the chair of the OTA Practice Management Committee. He is also a member of the editorial board for the Journal of Orthopaedic Business. Dr Switzer is committee member for AAOS and AOA. She is also on the editorial board for GOS&R, and a committee member for IGFS. For the remaining authors none were declared.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.