
Abstract
Introduction
A care conundrum for low-energy pelvic ring fracture patients in which they face financial burden after not qualifying for an inpatient stay of 3 days or more has been noted in the literature. The purpose of this study was to identify factors that lead to inpatient length of stay (IP LOS) ≥3 days in older adults with nonoperative pelvic ring fragility fractures and to highlight the challenging financial decision-making of those with IP LOS <3 days in the context of the Medicare 3-day rule.
Methods
This was a retrospective review of 322 patients aged ≥65 presenting from March 2016 and February 2019 to either of 2 emergency departments (EDs) after a ground-level fall resulting in a pelvic ring fracture. Patient demographic, IP LOS, and mortality data were extracted. Case management notes were analyzed to summarize financial decision-making for patients with IP LOS <3 days. Multivariate logistic regression analysis was conducted to identify factors that predicted IP LOS ≥3 days and mortality.
Results
IP LOS ≥3 days was associated with presentation to level I hospital (OR .30 [.19, 0.50]) and being single (OR 2.50 [1.10, 5.68]). 70.3% required a post-acute skilled nursing facility (SNF) stay. Of patients with LOS <3 days, 25.0% were financially responsible for their SNF stay, while 7.9% elected home care due to financial reasons. Overall 30-day, 90-day, and 1-year mortality were 2.5%, 8.1%, and 20.8%, respectively. For patients with LOS <3 days, returning to assisted living compared to discharging to a SNF increased 90-day mortality risk (HR 8.529, P = .0451). Having Medicare trended towards increased 90-day mortality risk compared to commercial insurance (HR 4.556, P = .0544).
Conclusion
The current system is failing older adult patients who sustain nonoperative low-energy pelvic ring fractures in terms of financial coverage of necessary post-acute treatment. This care conundrum has yet to be solved.
Introduction
Low-energy pelvic ring fractures include fractures to both the anterior and posterior pelvic rings. Anterior pelvic ring injuries include those of the superior and inferior rami and para-symphyseal region, while posterior ring fractures include those of the ilio-sacral region and sacrum. These injuries typically occur following a ground-level fall and are secondary to osteoporotic bone in the older population. Collectively, these injuries account for 7% of all low-energy fractures in the United States. 1 It is well documented that the prevalence of these fractures is increasing.2,3 Female gender, age greater than 65, fall tendency, and decreased bone density are well established risk factors for these injuries. 1 Because they are generally stable, low-energy pelvic ring fractures rarely receive operative treatment in the United States (US).4,5
Abernathy et al. summarized the global literature on low-energy pelvic ring fractures and reported that, while there is ample data regarding the care of these patients internationally, there is a paucity of literature describing this patient population and their treatment course through the US healthcare system. 6 An important aspect of the US healthcare system is financial coverage of therapies, including stays in a skilled nursing facility (SNF). According to the Centers of Medicare and Medicaid Services (CMS), skilled care is nursing and therapy care that can only be safely and effectively performed by, or under the supervision of, professionals or technical personnel. 7 For millions of Americans aged 65 years or older, primary coverage is through the federally-funded Medicare health insurance offered through CMS. During the time of this data collection, CMS had a 3-day rule that determined coverage of a SNF stay.8-10 In order to be eligible, a patient was required to spend 72 consecutive hours admitted as an inpatient to 1 or more hospitals and, specifically, not admitted under “observation status”. CMS defines “observation status” as outpatient services provided within the hospital. 10 This status is determined based on the level of care required by the patient, and if a previously healthy patient sustains a pelvic ring injury, this likely is not enough to require a full inpatient level of care. Other comorbidities and concomitant injuries may elevate a patient’s needs to those of inpatient status. If a patient is admitted under “observation status”, regardless of whether they spend more than 3 nights in a hospital, they would not qualify for financial coverage of a subsequent SNF stay. A patient’s admission status may change should they require more or less care throughout their hospitalization and is determined by the admitting physician. Generally, CMS advises that a patient be admitted as an inpatient if they are expected to need 2 midnights or more of medically necessary hospital care. If insurance companies, including Medicare, decide that a claim for an inpatient admission should have been an observation stay, they can deny the claim. This rule leaves low-energy pelvic fracture patients in a post-acute injury rehabilitation care conundrum, as these patients often do not qualify for inpatient admission, yet they cannot safely go home without significant assistance.
To the knowledge of the authors, there are no reports of the implication of this US care conundrum in the literature. The purpose of this study is to describe the characteristics of patients who sustain low-energy pelvic ring fractures treated nonoperatively and their treatment course through the US healthcare system including the financial burden of post-acute rehabilitative care felt by these patients. Secondary aims include understanding the mortality outcomes of these patients and identifying factors that lead to inpatient length of stay (IP LOS) ≥3 days. Identifying characteristics that make patients eligible for Medicare coverage of a post-acute SNF stay would help healthcare providers identify patients at risk of falling into this care conundrum and optimize shared decision-making as well as social and financial resource allocation.
Materials and Methods
This was a retrospective cohort study conducted following Institutional Review Board approval. The electronic medical record (EMR) was queried to identify patients aged 65 years or older who presented to the emergency department (ED) of either a level III suburban community hospital, or an urban level I safety net hospital that provides services to a socioeconomically disadvantaged population, between March 2016 and February 2019 after sustaining low-energy trauma, often a ground-level fall, and receiving a diagnosis of pelvic ring fracture. These dates were chosen to avoid any confounding effect of the COVID-19 pandemic (and changes in CMS policy) on the mortality and survival analysis for this cohort. The following ICD-10 codes were used to identify patients with a qualifying injury: S32.1 (Fracture of the sacrum), S32.3 (Fracture of the ilium), S32.5 (Fracture of pubis), S32.6 (Fracture of ischium), S32.8 (Fracture of other parts of the pelvis), and S32.9 (Fracture of unspecified parts of the lumbosacral spine and pelvis). Operatively treated fractures, fractures from a high-energy mechanism of injury, pathologic fractures, peri-prosthetic fractures, and isolated acetabular fractures were excluded. Patients who sustained concomitant injuries that required surgical treatment were also excluded. Mechanism of injury was determined by review of the ICD-10 codes associated with the hospital encounter and by manual chart review. A low-energy mechanism of injury was defined as a fall from standing height or equivalent, while high-energy mechanisms included motor vehicle accidents or a fall from height, among others.
Age at injury, sex, marital status, body mass index (BMI), race/ethnicity, date of injury, insurance type, overall length of stay, IP LOS, place of residence prior to injury, hospice status prior to and after injury, hospital discharge disposition, ambulatory function prior to injury, medical comorbidities, and case manager narratives regarding requirements for private pay were extracted from the EMR. Date of death was extracted from EMR and supplemented with state death records. Charlson Comorbidity Index (CCI) was calculated based off extracted comorbidities. 11 Marital status was grouped together to categorize patients who were living with a significant other at the time of injury and those living alone. Insurance plans were grouped based on governmental vs private source of funding, with governmental plans subsequently categorized into those with qualifying factors based on age vs based on income. Residence was categorized into independently owned residences (eg, homes, condos, etc), assisted living (AL) where communal services such as meals were provided (eg, senior living communities), and long-term care (LTC) facilities where individualized daily assistance was provided (eg, nursing home or memory care unit). Ambulation status was recorded as either independent, requiring an assistive device, or non-ambulatory.
Statistical analysis was conducted using SAS 9.4 (Cary, NC). Data was summarized using percentages, ranges, means, standard deviations, medians, and interquartile ranges where appropriate according to IP LOS. A multivariate logistic regression model (PROC GLIMMIX) was implemented to identify factors associated with IP LOS ≥3 days. Odds ratios and confidence intervals are presented. Ninety-day and 1-year survival analyses were performed using hazard ratios for patients IP LOS <3 days.
Results
A total of 515 encounters from 489 patients were identified, of which 322 and 320 patients were included in the study and final regression analysis, respectively (Figure 1). Patients were mostly female (82.3%) with a mean age of 84 ± 8.7. Most patients (93.8%) self-identified as White. Only 31.4% were married. The cohort was nearly evenly split between commercial and governmental insurance coverage. Prior to injury, under half of the patients were independently ambulating, while 58.1% either required an assistive device or were not ambulatory. Of the cohort, 57.1% lived in an independent home prior to the injury. Mean CCI was 2.5 ± 2.3, with 37.0% having documented cognitive deficits. Mean LOS and mean IP LOS were 3.3 ± 2.7 and 2.4 ± 3.0 days, respectively. Eighteen patients had a total LOS ≥3 days but an IP LOS <3 days. The majority of patients (70.2%) were discharged to a SNF following their hospital stay. The 30-day, 90-day, and 1-year mortality were 2.5%, 8.1%, and 20.8%, respectively (Table 1). Exclusions and final numbers included. BMI = Body Mass Index. Low-Energy Pelvic Ring Fracture Patients Aged 65 and Older (N = 322). Continuous variables reported as mean ± S.D. Categorical variables reported as N (%). aBMI = Body Mass Index. bCCI = Charlson Comorbidity Index. cLTC = Long-Term Care (eg, Nursing home, memory care, etc.). dLOS = Length of Stay. eSNF = Skilled Nursing Facility.

Patient Characteristics Based on Inpatient Length of Stay (N = 322).

Continuous variables reported as mean ± SD Categorical variables reported as N (%).
aResults of two-sample t test (significance set at P = .05).
bResults of chi-square test (significance set at P = .05).
cBMI = Body Mass Index.
dCCI = Charlson Comorbidity Index.
eLTC = Long-Term Care (eg, Nursing home, memory care, etc.).
fLOS = Length of Stay.
gSNF = Skilled Nursing Facility.
Factors That Predict Inpatient Stay of Three Days or More (N = 322).

Reference: Hospital B, Age 84.5, CCI 3.6, BMI 25.7, Male Sex, No Cognitive Dysfunction, Married, Commercial/Self-managed Insurance, Prior Home Residence, Uses Assistive Devices.
a= statistically significant (P < .0500).
c= approached significance (P = .0651).
bCCI = Charlson Comorbidity Index.
dBMI = Body Mass Index.
eLTC = Long-Term Care (eg, Nursing home, memory care, etc.).
For patients aged ≥65 with an IP LOS <3 and who were not discharged directly from the emergency department (n = 152), case manager narratives revealed that 43.4% of these patients had no documented counseling regarding the possibility of financial responsibility for a SNF stay. Only 53.3% of patients were informed of a potential financial burden for their care. Requested down payments and daily rates for SNF care ranged from $1000 to $6000 and from $250 to $500 per day, respectively. Of those who were informed of this potential financial cost, 46.9% were fully financially responsible for their post-acute SNF stay, 38.3% had additional resources (eg, Medicaid, supplemental insurance, VA coverage, previous qualifying stay within 30 days, etc.) to cover the cost of stay, and 14.8% chose other treatment due to these financial reasons (Figure 2). Only 14 of the 38 patients (36.8%) that elected to be financially responsible for the SNF stay had Medicare as their primary payer. Discharge and Financial Decision-Making of Low-Energy Pelvic Ring Fracture Patients after Case Management Encounter (n = 152). Red-colored boxes indicate instances where the current system may fail patients. IP LOS = Inpatient Length of Stay, SNF = Skilled Nursing Facility.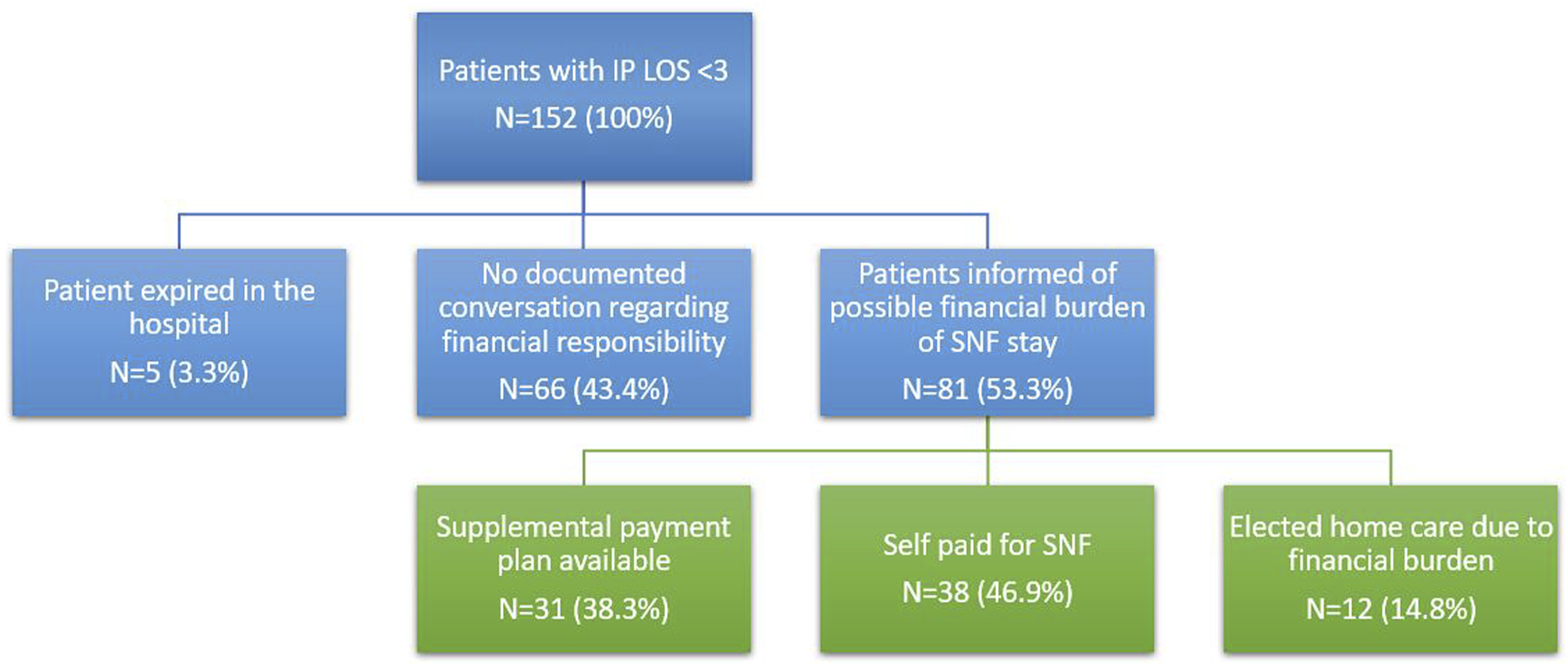
Hazard Ratios and Predictors of Mortality in Low-Energy Pelvic Ring Fracture Patients With an IP LOS a Under Three Days (N = 172).

Reference: Level I Hospital, Age 83.8, CCI 2.3, Discharge to SNF g , BMI 24.5, No Cognitive Dysfunction, Married, Commercial/Self-managed Insurance, Prior Home Residence.
c= statistically significant (P < .050).
d= approached significance (P = .054 for 90-Day Medicare, P = .051 for 365-Day Discharge to Assisted Living).
aIP LOS = Inpatient Length of Stay.
bCCI = Charlson Comorbidity Index.
eLTC = Long-Term Care (eg, Nursing home, memory care, etc.).
fBMI = Body Mass Index.
gSNF = Skilled Nursing Facility.
Discussion
This retrospective cohort study sheds light on the care conundrum that existed for older adult patients sustaining low-energy pelvic ring fractures due to the stipulations of the Medicare 3-day rule. Overall, the cohort had an average IP LOS of less than 3 days. This means that, under the Medicare three-night rule, a majority of the study patients would not receive financial coverage under Medicare alone regardless of whether they would benefit from a SNF stay. Review of case management notes regarding the topic of financial responsibility revealed that a quarter of patients in this scenario elected to pay out-of-pocket for their post-acute care, while over 7% elected another course of treatment due to financial hardship. These case management notes also reported that SNF facilities requested down payments of thousands of dollars and/or daily rates in the several hundreds of dollars for our patient cohort who were paying out-of-pocket for their care. These amounts far exceed the available discretionary funds for many Americans and places undue financial burden on patients and their families. 12
Equally as important was the lack of any documented conversation around the topic of possible financial burden to the patient for nearly half of the patients with IP LOS <3 days. While it is legally required for hospitals to provide a Medicare Outpatient Observation Notice (MOON) document outlining the possible financial responsibilities of an observation admission and possible post-acute SNF to all patients that are admitted under observation, 9 it is also important to document conversations surrounding this sensitive topic to demonstrate patient understanding and provide opportunities to improve holistic fracture patient care. This lack of documentation significantly limited our analysis surrounding this important topic.
Interestingly this financial burden was not felt only by patients with Medicare as their primary insurance payer. In this cohort, of the 38 patients who were ultimately financially responsible for their SNF cares, 2 thirds had some other insurance plan other than Medicare as their primary payer. This demonstrates how Medicare policies and this care conundrum can affect patients with private insurance plans as well. Medicare patients do not seem to be the only ones afflicted by this care conundrum.
In better understanding the patients who will necessitate a full IP LOS ≥3 days, it is reasonable that patients who had pre-existing cognitive deficits, higher CCI, and prior living arrangements in a LTC facility or hospice care would predict a longer inpatient hospitalization due to a need for the full use of the hospital’s resources. Our results did not demonstrate this, however, and the difference in IP LOS between the 2 centers was unexpected. Comparing patient populations at each hospital, there was no statistically significant difference in CCI to represent a cohort with increased number of comorbidities. However, the CCI does not appropriately weigh the severity of 1 or 2 comorbidities that may necessitate a longer IP LOS over a patient with multiple mild comorbidities. As the level I hospital serves a population that is more underserved and historically does not routinely receive recommended therapies, it is very possible that their comorbidities are much more severe than those seen within the wealthier, suburban community that the level III hospital serves.
Survival analysis for the cohort with IP LOS <3 days revealed that discharge disposition back to an assisted living when compared to SNF contributed to increased 90-day mortality and trended towards significantly increased 1-year mortality. This suggests that a SNF stay in the immediate post-injury stage may contribute to short-term, and potentially longer-term, patient survival. Interestingly, albeit no statistical significance, patients with Medicare insurance had a trend towards increased risk of death 90 days after injury. This could suggest that patients who are required to pay out-of-pocket for their SNF care elect less expensive and potentially lower-quality facilities. Future studies are needed to fully understand this finding.
Survival is not the only important outcome for this population. Older adult individuals may experience differing care goals from younger counterparts that may focus more on daily functioning and independence. 13 Areas of future study should include evaluating clinical outcomes of these patients such as ambulation status, independence with activities of daily living, and readmission rates. Large, multicenter studies could provide a better understanding of the differences in medical practice among trauma centers compared to community hospitals. Additionally, during the COVID-19 pandemic, there was a waiver to the three-night rule that allowed patients to receive SNF care without a qualifying IP admission. 14 It would be worthwhile to evaluate the financial coverage of treatment and clinical outcomes of the patients who sustained these fractures during this time period to better guide advocating efforts for future policy changes.
Policy changes on this topic are forthcoming The COVID-19 waivers were discontinued with the end of the public health emergency on May 11, 2023.15,16 A legislative bill introduced to the House in June 2021 titled “Improving Access to Medicare Coverage Act of 2021” could address this issue. This bill proposes that time admitted under observation status should count towards the 3-day rule coverage of post-acute care. 17 Should this bill be enacted, it may improve the care and satisfaction for some patients. For the cohort in this study, this bill would have impacted 18 patients who had long observation admissions. However, it would still leave the vast majority of patients who do not necessitate a 3-day hospitalization in a discharge conundrum. They could remain in the hospital on observation status, which continues to increase their healthcare spending while also occupying critical hospital beds in hospitals that are notoriously low-staffed and at full-capacity following the recent pandemic.18,19 In addition to this waste of resources, there are substantial risks for nosocomial infections by remaining in the hospital longer than necessary. Meaningful changes to the Medicare three-night rule can only occur with repeal of the 1965 statutory provision that mandates Medicare Part A coverage of post-hospitalization care only when a patient has been hospitalized for 3 days. 8
There are several limitations of this study. This is a retrospective study that can only assess for association, not causation. The study is only limited to 1 singular injury type (low-energy pelvic ring fractures) and was unable to assess for other injuries that may present a similar care conundrum. While we utilized a convenience sample in 2 centers in 2 different subsections of a large metropolitan area, this data may not be representative of the US population. The size of the final cohort may have left some of the statistical analyses underpowered. Post hoc analysis would be helpful to evaluate how many patients would be required to ensure statistical significance. Similarly, some patients lacked follow-up of 1 year or more. This affected the controlled survivorship models that censored these patients. The category choices for patient financial decision-making status in case manager narratives as well as baseline functional metrics (ie residential status and ambulation) were somewhat arbitrary and likely unable to granularly capture all aspects that contributed to these factors. Finally, this study is reliant on consistent coding across 2 hospitals within the studied healthcare system, thus there is a possibility that coding errors or inconsistencies exist that would skew the data. Manual chart review mitigated the limitations of both arbitrary categorization and coding inconsistencies for this study.
Conclusions
This is the first study to describe and evaluate the care conundrum imposed by the Medicare three-night rule on patients who sustain a low-energy fracture of the pelvic ring. Most of these patients did not require a three-night inpatient admission for this injury, yet many require post-acute SNF care. A quarter of the patients who did not qualify for a three-night stay were ultimately financially responsible for their SNF stay. Receiving SNF care compared to returning to a prior assisted living facility was suggestive of increased survival at 90 days post-injury, and having commercial insurance compared to Medicare trended towards increased survival in that same timeframe. Further studies are necessary to evaluate additional clinical outcomes, gauge patient satisfaction, direct policy advocacy, and compare costs both to patients and to Medicare.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lisa K. Schroder MBA is a paid consultant for Exactech, Inc. and Synthes. Julie A. Switzer MD is a committee member for the American Academy of Orthopaedic Surgeons (AAOS), the American Orthopaedic Associations (AOA), and the International Geriatric Fracture Society (IGFS). She is also on the editorial board of Geriatric Orthopaedic Surgery and Rehabilitation.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.