
Abstract
Introduction:
The aim of this study was to compare the effectiveness of 2 interventions in prompting patients to obtain osteoporosis follow-up after a fracture. Our hypothesis was that a phone call plus letter would yield greater response toward osteoporosis evaluation versus a letter alone to patients after sustaining a fragility fracture.
Materials and Methods:
Prospective study randomized 141 patients age 50 years and older with a fragility fracture into 3 groups for comparison. Group 1 (letter only) patients received a letter 3 months after their diagnosis of fracture indicating their risk for osteoporosis and urging them to follow-up for evaluation. Group 2 (phone call plus letter) patients were contacted via phone 3 months after their diagnosis of fracture. A letter followed the phone call. Group 3 (control) patients were neither contacted via phone nor sent a letter. All groups were contacted via phone 6 months after their initial visit to determine if they followed up for evaluation.
Results:
In group 1, 23 (52.27%) of 44 had follow-up, and 21 (47.73%) of 44 did not follow-up. In group 2, 30 (62.5%) of 48 had follow-up, and 18 (37.50%) of 48 did not follow-up. In group 3, 6 (12.24%) of 49 had some sort of follow-up, and 43 (87.76%) of 49 did not have any follow-up. A statistical significance was achieved between group 3 (control) and both groups 1 and 2 with regard to follow-up (P < .0001). The results did not show a statistically significant difference between Groups 1 and 2, however, there was a trend toward improved response with a phone call plus letter (P = .321).
Conclusion:
A more personalized approach with a phone call plus follow-up letter to patients increased osteoporosis follow-up care by an additional 10%, however, this was not a statistically significant difference from just sending out a letter alone.
Keywords
Background and Significance
Osteoporosis is a prominent disease throughout the world affecting the quality of life and health of at least 10 million people in the United States alone. 1 Furthermore, it is speculated that 34 million people across many backgrounds and ethnicities in the United States are at risk for the disease. 2,3 Osteoporosis is characterized by progressive deterioration of bone microarchitecture, which leads to low bone mineral density and weakened bone at increased risk for fracture. A fragility (or osteoporotic) fracture is a fracture sustained from a low-energy mechanism during normal activities of daily living, such as a fall from standing height or without obvious trauma. Patients with a fragility fracture have a much higher rate of morbidity and mortality than their counterparts without such fractures. 4 –7 Such fractures can be prevented via primary or secondary prevention of osteoporosis. Primary prevention of osteoporosis is defined by protecting healthy patients against developing the disease, whereas secondary prevention of osteoporosis screens and treats patients either at high risk for developing the disease or diagnosed with an earlier stage of osteoporosis. Research has shown that when treatment for osteoporosis is initiated after sustaining a fragility fracture, the risk of future fractures is decreased by as much as 50%. 8 Prevention of future fracture after sustaining a fragility fracture is known as tertiary prevention of osteoporosis.
Unfortunately, osteoporosis is overshadowed in an era of chronic illnesses, and a medical care gap exists between physicians and patients. Fewer than 12% of postmenopausal women have a diagnosis of osteoporosis before their index fracture. 9 By their first presentation with the disease, they typically have already become symptomatic with a fragility fracture. A strikingly low rate (<15%) of patients with a fragility fracture seek and receive treatment for osteoporosis. 10 –12 A recent retrospective study by Balasubramanian et al revealed that treatment rates are continuing to decline. 13 This low rate is multifactorial and due in part to various barriers such as the lack of physician recognition of their role to encourage patient follow-up, lack of patient knowledge, the potential cost of workup and treatment, and the presence of multiple patient comorbidities. A growing body of literature supports the initiation of an osteoporosis intervention program to encourage patient follow-up and treatment. A variety of osteoporosis programs have been proposed and they all reveal significant efficacy as compared to no intervention at all. For example, our prior study showed a 60% response rate compared to 15% without any intervention (P < .0001). 14
Much of the literature examines only one osteoporosis intervention program at a time, however, and research that compares the effectiveness of differing osteoporosis intervention is limited. The purpose of the present study was to address this lack of data and to determine if the type of intervention makes a difference in an effort to close the existing care gap. Our aim was to compare the effectiveness of two interventions in prompting patients to obtain osteoporosis follow-up after a fracture. We hypothesized that a follow-up phone call plus letter would yield greater response toward osteoporosis evaluation versus a letter alone.
Methods
This was a prospective study that was reviewed by our institutional review board (IRB) committee and qualified for exemption. The study was given a nonresearch determination by our IRB, so informed consents were not necessary. Patients aged 50 years or older with a fracture were identified upon arrival to our emergency department (ED) from December 1, 2011, to May 14, 2013. In total, 1191 billing records were compiled and patients were tagged with an International Classification of Diseases, Ninth Revision (ICD-9) diagnostic code at the time of discharge from the ED. The billing department determined the code based on the documentation in the electronic medical record. Study patients were then identified based on specific ICD-9 fracture codes that initially suggested a fragility fracture diagnosis. Hospital encounter screening identified the patients linked to these codes, and patient information was downloaded in monthly increments by an individual in the hospital’s financial department. The data were autopopulated into our “Orthopaedic Osteoporosis Registry/Database.” We used Filemaker Pro for our database application. Manual chart reviews were performed on each patient chart to determine how their fracture occurred to confirm if indeed it was a fragility fracture (ie, fall from standing height). Patients were excluded if their mechanism of injury was not consistent with the definition of a fragility fracture such as those fractures resulting from high-energy traumas, falls from higher than standing height, and motor vehicle accidents. Patients with polytrauma were exempted even if the injuries sustained were from low-energy forces. Patients were also excluded if they were dead, repeated in the database (ie, multiple ED visits for fractures), or had fracture treatment at another institution. Finally, patients currently treated for osteoporosis or individuals unable to be contacted for various reasons (phone disconnected/out of service, patient admitted to nursing home, or having dementia) were also excluded. Upon completion of chart review, 1050 patients were excluded from the study for the reasons listed previously.
One hundred forty-one participants were eligible for the study after exclusion, as their mechanisms of injury fit the definition of a fragility fracture and they each have neither been diagnosed with nor treated for osteoporosis. The following fracture codes were identified: (10) pathologic fracture-vertebrae 733.13; (2) pathologic fracture femoral neck 733.14; (10) dorsal vertebra 805.2; (10) lumbar vertebra 805.4; (5) sacrum/coccyx 805.6; (3) vertebral fracture not otherwise specified (NOS) 805.8; (6) proximal humerus 812; (16) Colles fracture 813.41; (27) distal radius 813.42; (2) distal ulna 813.43; (10) distal radius with ulna 813.44; (2) femur, midcervical neck 820.02; (2) femur, base of cervical neck 820.03; (8) femur, transcervical 820.09; (1) trochanteric NOS 820.2; (12) intertrochanteric 820.21; (1) subtrochanteric 820.22; and (14) femoral neck NOS 820.8 (Table 1). We did not include in our research if our participants sustained a fragility fracture prior to their current fracture because this was not the focus of our study, and any patient with prior osteoporosis evaluation and treatment were excluded from our study.
ICD-9 Fragility Fracture Codes Assigned to Study Patients and Controls.

Abbreviations: ICD-9, International Classification of Diseases, Ninth Revision; NOS, not otherwise specified; group 1, letter only; group 2, phone call plus letter; group 3, control.
The 141 participants were randomized into 3 groups for comparison. In the first group (letter only), letters were sent out to each participant 3 months after their initial visit indicating their risk for osteoporosis and urging them to follow-up with their primary care physician (PCP) or at our hospital system. Patients were contacted 6 months after their initial visit to determine whether they followed up with osteoporosis evaluation. In the second group (phone call plus letter), each participant was contacted via phone 3 months after their initial visit and informed that they could be at risk for osteoporosis and urged to follow-up with their PCP or at our hospital system. A letter followed the phone call. Patients were contacted 6 months after their initial visit to determine whether they followed up with osteoporosis evaluation. In the third group (control), participants were neither contacted via phone nor sent a letter indicating their risk for osteoporosis. They were contacted 6 months after their initial visit to determine whether they followed up on their own.
Results
In the control group, 6 (12.24%) of 49 had some sort of follow-up care for osteoporosis following discharge from the ED, and 43 (87.76%) of 49 patients did not have any follow-up. In the letter-only group, 23 (52.27%) of 44 received follow-up for osteoporosis evaluation, and 21 (47.73%) of 44 did not follow-up further for osteoporosis management. Reasons for not following up included too busy (4.76%), other health issues (23.81%), just did not do anything (33.33%), did not understand letter (9.52%), and did not feel they had osteoporosis (28.57%). In the phone call plus letter group, 30 (62.5%) of 48 received follow-up care for osteoporosis, and 18 (37.50%) of 48 did not follow-up for further care. Reasons for not following up included too busy (27.78%), other health issues (27.78%), just did not do anything (22.22%), did not understand letter (11.11%), and did not feel they had osteoporosis (11.11%). Our results showed a trend toward improved response with a phone call plus letter, but statistical significance was not achieved (Figures 1 and 2).

Percentage of patients who followed up for osteoporosis workup.
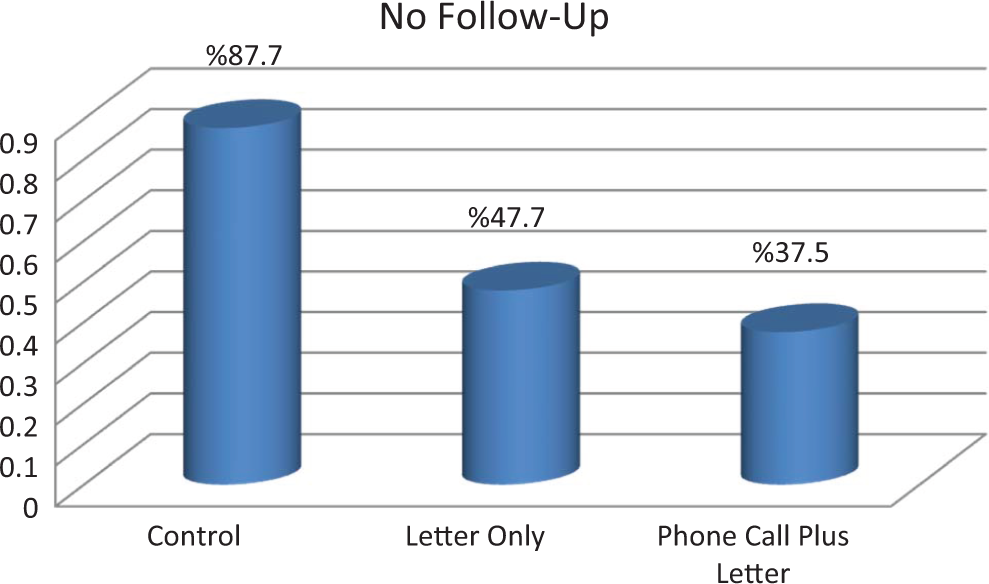
Percentage of patients who did not follow-up for osteoporosis workup.
Discussion and Conclusion
Approximately 1.5 million people sustain fragility fractures in the United States annually, costing an estimated 18 billion dollars. 15 These numbers are expected to expand with the rapidly aging population. Current literature demonstrates a low rate of follow-up care received by patients experiencing fragility fractures without intervention, despite the large burden it places on both patient health and the health care system. 1,12,16 –19 Patients who experience a fragility fracture increase their risk of future fracture 1.5- to 9.5-fold. 4 It is quite evident that an osteoporosis intervention program for patients presenting with a fragility fracture is effective in improving the rate of patient follow-up. The targeted outcome of these programs is multifactorial. The primary outcome is to enhance the continuum of care for high-risk patients or to improve patient follow-up and physician-to-physician communication so that appropriate workup and diagnosis of osteoporosis are not missed. Other projected outcomes include improving osteoporosis treatment rates, reducing morbidity and mortality, and decreasing the annual cost burden of fragility fractures. A wide variety of intervention programs has demonstrated effectiveness in improving the continuum of care, with the rate of patient follow-up significantly greater with an intervention program in place compared to no program. 8,10,14,16,20 –26
Despite the expanding data on single program efficacy, the most successful method of intervention has yet to be determined and studies that compare more than 1 intervention program are limited. Our present study contributes to the sparse data of comparing intervention programs. We chose our patient population based on recommendations from the National Osteoporosis Foundation, which states that all individuals aged 50 years or older experiencing fragility fractures should be evaluated and treated for osteoporosis. 27 The results of our study showed statistical significance between the control group (12.24%) and both the letter-only group (52.27%) and the phone call plus letter group (62.5%) with regard to follow-up (P < .0001). The results did not show a statistical difference between the letter-only (52.27%) and the phone call plus letter (62.5%) groups (P = .321). Because the results trended toward a better response with the phone call plus letter, there is a possibility that future studies with a larger sample size may reveal a significant difference. Alternatively, these results reveal that programs as simple as sending out a letter to at-risk patients targeted with a fragility fracture improve patient follow-up, which would be easy to implement in most hospital systems.
A good intervention program should be cost effective, have little to no margin for error, and be feasible for multiple hospital systems with varying infrastructure. Although there are many proposed interventions that are effective in improving patient follow-up, some may not be reproducible in several hospital systems secondary to the program’s complex design or the lack of hospital resources. Multiple studies have shown efficacy in simply sending out standardized letters to patients at risk. 14,20,28 Our previous study showed success with a simple automated letter. 14 Methods that lack automation may be too time consuming and cumbersome, and patient identification for program inclusion is at greater risk of being overlooked secondary to human error. Some programs advocate for an osteoporosis care coordinator. 16,21 –23 Sander et al created a program utilizing a dedicated care coordinator and analyzed both cost effectiveness and avoidance of subsequent hip fractures as compared with no care coordinator. Their analysis revealed that a medical center that hires an osteoporosis coordinator who manages 500 patients with fragility fractures each year could reduce the number of subsequent hip fractures from 34 to 31 in the first year, resulting in a net hospital cost savings of C$ 59,160 (Canadian dollars in the year 2015 values). They determined a 90% probability that hiring a coordinator costs less than C$ 30,214 per hip fracture avoided and that greater savings are anticipated after the first year. 21
A growing body of evidence has shown that involvement of the orthopedic surgeon in osteoporosis care significantly improves patient follow-up and compliance. 1,10,24,29,30 The orthopedic surgeon is often the first and possibly the only physician involved in the patient’s care for their fragility fracture. An opportunity for patient education and osteoporosis intervention can potentially be missed in these situations. A prospective randomized trial by Miki et al determined that early and continued management of osteoporosis treatment by the orthopedic team in patients with a hip fracture resulted in 58% pharmacologic treatment at 6 months, which is compared to only 29% of patients who were to follow-up with their PCP (P = .04). 24 Similarly, another prospective randomized study by Rozental et al compared 2 different interventions: group 1 consisted of osteoporosis screening initiated by the orthopedic physician via ordering a bone mineral density test and sending the results to the patient’s PCP. Group 2 consisted of the orthopedic surgeon sending a letter to the patient’s PCP describing the guidelines for osteoporosis evaluation and treatment. The results revealed that the patients randomized to group 1 had 2 to 3 times greater rates of bone mineral density testing (93% compared with 30%, P < .001), discussion of osteoporosis with their PCP (89% compared with 35%, P < .001), and initiation of osteoporosis therapy (74% compared with 26%, P < .001) compared with patients randomized to group 2. 29 Programs such as the Own the Bone project 8,10 and the Healthy Bones Program 15 have been initiated to enhance the rate of counseling by the orthopedic surgeon to patients with fragility fractures.
It is important to note that the outcome of patient follow-up for osteoporosis testing does not always equate successful treatment. A prospective study by Hawker et al implemented an intervention program in an outpatient setting that consisted of educating patients with fragility fractures of their osteoporosis risk and encouraging them to follow-up with their PCP. A standardized letter was also sent out to each patient’s PCP. The results revealed that patients who received the intervention were more likely to follow-up with their PCP (adjusted odds ratio [OR]: 1.85, P = .02) and to be recommended for bone density screening (adjusted OR: 5.22, P < .0001) but were not more likely to receive a treatment recommendation (adjusted OR: 2.07, P = .07). 20 The previously mentioned study by Edwards et al found that if actual treatment was initiated early, the outcome of treatment care initiation at 6 months was more than 2 times greater than with delayed patient follow-up. 10 However, there is evidence that education alone prior to patient discharge does demonstrate effectiveness and improved rates of treatment. Patients prepared with questions to ask their PCP were twice as likely to receive osteoporosis treatment as those without questions (42% vs 19%, respectively). 26
As with any study, the present study does have some limitations. This study consists of a relatively small sample size, and the cohort comparison between the letter group and phone call plus letter group is underpowered. Additionally, a potential limitation to this study is that we did not specify if each fragility fracture was the patient’s first one or if they have sustained prior fragility fractures. We felt that this information extended beyond the scope of our study as our focus was on determining whether or not our patient followed up for evaluation after diagnosis of their current fragility fracture, and any patient with prior osteoporosis workup and treatment were excluded from the study.
The present study further supports the notion that osteoporosis intervention programs enhance the continuum of care for high-risk patients, which could ultimately decrease the morbidity, mortality, and financial impact of the disease on society. We have shown that contacting the patient whether with a letter or also a phone call does improve follow-up care for osteoporosis management following a fragility fracture diagnosis requiring an ED visit. We also showed that a more personalized approach with a phone call to the patient increased osteoporosis follow-up care by an additional 10%, however, this was not a statistically significant difference from just sending out a letter alone. Future studies may look at sending out a letter first and then placing a phone call to see if this reveals any significant findings.
Footnotes
Acknowledgments
Special thank you to Ananya Das for her exceptional work and dedication to this project.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E. J. Fox is a consultant for Amgen and Eli Lilly, and his wife is an employee at GSK. A. D. Armstrong is a consultant for Zimmer.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.