
Abstract
Introduction:
This study investigates the management of hip fractures in a German maximum care hospital and compares these data to evidence-based standard and practice in 180 hospitals participating in the UK National Hip Fracture Database (NHFD) and 16 hospitals participating in the Irish Hip Fracture Database (IHFD). This is the first study directly comparing the management of hip fractures between 3 separate health-care systems within Europe.
Methods:
Electronic medical data were collected retrospectively describing the care pathway of elderly patients with a hip fracture admitted to a large trauma unit in the south of Germany “University Hospital Freiburg” (UHF). The audit evaluated demographics, postoperative outcome, and the adherence to the 6 “Blue Book” standards of care. These data were directly compared with the data from the UK NHFD and the IHFD acquired from 180 and 16 hospitals, respectively.
Results:
At 36 hours, 95.8% of patients had received surgery in UHF, compared to 71.5% in the NHFD and 58% of patients in the IHFD. The rate of in-hospital mortality was 4.7% compared to 7.1% in the NHFD and 5% in the IHFD. The mean average acute length of stay was 13.4 days compared to 16.4 days in the NHFD and 20 days in the IHFD. Reoperation rates are 3.3% compared to 1% in the NHFD and 1.1% in the IHFD; 50.5% of patients were discharged on bone protection medication, compared to 47% in the IHFD and 79.3% in the UK NHFD.
Discussion:
Despite uniformly acknowledged evidence-based treatment guidelines, the management of hip fractures remains heterogeneous within Europe.
Conclusion:
These data show that different areas of the hip fracture care pathway in Germany, England, and Ireland, respectively, show room for improvement in light of the growing socioeconomic burden these countries are expected to face.
Introduction
Hip fractures of the elderly patients present an ever-increasing social and economic burden within Europe. Due to demographic changes, this burden is predicted to increase strongly in the future decades. 1 On an individual patient level, hip fractures are associated with a high rate of mortality. 2 The reduced mobility and the long in-hospital stay can be a serious setback and exacerbate comorbidities in a geriatric patient. 3 Due to these factors, European countries, as well as other developed nations, are in need of continual development of effective strategies for preventing and managing hip fractures in the elderly patient population. A valuable part of this process is critically evaluating the care pathway on a regular basis and drawing from the experience of other developed nations.
Hip fracture management in the United Kingdom and Ireland has transformed since the publication of the “Care of Patients with Fragility Fracture ‘Blue Book’” by the British Orthopaedic Association and British Geriatric Society in 2007. 4 This publication highlights the following 6 evidence-based standards to improve patient outcome: admission to orthopedic ward within 4 hours of presentation, surgery within 48 hours of admission, prevention of the development of new pressure ulcers, routine preoperative orthogeriatric (OG) assessment, assessment for the need for therapy to prevent future osteoporotic fractures, and specialist falls assessment. The National Hip Fracture Database (NHFD) in the United Kingdom bases its data set on the Blue Book standards and transparently and continually audits the care and outcome of senior patients with hip fracture since 2008. 5 The NHFD has expanded to base its audit on further 6 quality standards published by the National Institute for Health and Care Excellence (NICE) in 2011. 6 The Irish Hip fracture Database (IHFD) was established in 2012, modeled on the NHFD, and continues to measure individual hospitals compliance against the 6 Blue Book standards. 7 A further change in the structure of the management of hip fractures in the United Kingdom and Ireland has been a push toward integrating OG models of care as well as fracture liaison services (FLSs). So far these measures have been shown to reduce fracture rerates, 8 in-hospital mortality, length of stay (LOS), and in consequence improve cost-effectiveness. 9,10
In Germany, 608 hospitals were registered as trauma units in 2015. 11 Altogether 30 trauma units participate in a hip fracture auditing program (AltersTraumaRegister DGU) since 2016 which uses a similar data set to the NHFD and are obliged to offer an OG model of care. 12 Hospitals manage patients with hip fracture according to the clinical guidelines of the “Deutsche Gesellschaft für Unfallchirurgie” (DGU). 13 Additionally, the management of trochanteric fractures is centrally controlled in each German state by a quality assurance office and is subject to strict regulations with regard to time to surgery, postoperative mobilization, and the rate of complications. Some individual hospitals have recently begun offering an FLS to ensure continuity of osteoporosis therapy. Currently, 2 trauma units in Germany offer an FLS using the recognized “Capture the Fracture” model of the International Osteoporosis Foundation. 14
To the best of our knowledge, currently no analysis exists comparing similar data sets between hospitals in separate European countries. This study aims to compare the management of hip fractures between the NHFD, the IHFD, and the trauma unit of a German maximum care facility.
Methods
Study Population
Electronic medical data were collected between January 1, 2012, and December 31, 2016, which includes all admissions and discharges to the emergency department (ED) as well as direct admissions to a trauma and orthopedic ward in the “University Hospital Freiburg” (UHF). As a large maximum care facility, this hospital admits patients from the entire Southern Baden Area of Germany. International Classification of Diseases, Tenth Revision, German Modification diagnoses included were S72.0—fractures of the femoral neck, S72.1—pertrochanteric fractures, and S72.2—subtrochanteric fractures. Periprosthetic fractures were not included in the search. For the purpose of comparing groups, we excluded 153 patients younger than 60 years and 141 patients with terminal malignancies or pathological fractures from this population (955 patients). Furthermore, 25 patients were excluded with a fracture older than 7 days. Therefore, we collected the data of 636 patients (66.6% of the initial selection).
Variables
For the purpose of comparing groups, we firstly evaluated demographic and clinical variables. These variables included age at surgery, sex, source of admission, type of surgery performed, and type of anesthesia. Secondly, we evaluated the adherence to the 6 standards of care published in the Blue Book in the United Kingdom, which consists of time to admission to orthopedics ward, time to surgery, incidence of a new pressure ulcer, OG assessment, discharge on bone protection medication, and specialist falls assessment. Additionally, we evaluated the time to surgery, the rate of in-hospital mortality, and rates of reoperation within 30 days. Data were entered into Microsoft excel. In order to assess the accuracy of the data, 10% of the electronic medical records included in the audit were randomly selected by the study researcher. No errors in transcription were detected in this selection. Subsequently, we directly compared all the acquired variables with NHFD 5 and the IHFD 7 each collected between January 1, 2015, and December 31, 2015.
Statistical Analysis
The results were analyzed using the software IBM SPSS Statistics 25.0. The χ2 test was used to establish a relationship between the groups UHF, NHFD, and IHFD. The maximum value for a statistical difference was set at α = .05.
Results
Patient Demographics and Source of Admission
Sixty-seven percent of patients were female, compared to 70% in the IHFD and 71.6% in the NHFD; 43.2% of patients admitted were younger than 80 years, compared to 41% in the NHFD and 41% in the IHFD (Table 1). Sixty-nine percent of patients were admitted from home, compared to 83% in the IHFD. Seventeen percent of the patients were transferred from other acute hospitals, compared to 9% in the IHFD (Table 2). There were no comparable data describing the source of admission in the NHFD 2015 report. 5
Patient Demographics.

Abbreviations: IHFD, Irish Hip Fracture Database; NHFD, National Hip Fracture Database; UHF, University Hospital Freiburg.
Source of Admission.

Abbreviations: IHFD, Irish Hip Fracture Database; UHF, University Hospital Freiburg.
Fracture Classification, Type of Surgery, and Anesthesia
The fracture classification varied between the NHFD, IHFD, and UHF. In the UHF collective, 50% of the hip fractures sustained were classified as trochanteric fractures. The most common hip fracture in the NHFD and the IHFD was classified as displaced intracapsular neck fractures, with 49.1% and 37%, respectively (Table 3). The type of surgery also varied between data sets. A dynamic hip screw (DHS) was used for 82% of the undisplaced intracapsular neck fractures in the UHF, compared to only 24% in the IHFD, where the most common procedure performed was cemented hemiarthroplasty with 68% (Figure 1). For displaced intracapsular fractures, 27% of patients received a total hip replacement (THR) compared to 26.9% in the NHFD and 5% in the IHFD. The preferred procedure for displaced intracapsular neck fractures in the IHFD seemed to be a hemiarthroplasty with 89% (Figure 2). Intramedullary (IM) nailing was the preferred option for treating intertrochanteric fractures with 76%, compared to 38% in the IHFD. Twenty-three percent of patients with trochanteric fractures received a DHS, compared to 79.8% in the NHFD (Figure 3). One hundred percent of patients with a subtrochanteric fracture received an IM-nail compared to 79% in the NHFD and 82% in the IHFD. With regard to the proportion of cemented arthroplasties, 90.7% of all arthroplasties were cemented, compared to 83.6% in the NHFD and 70% in the IHFD. Almost all of the patients (99.8%) received surgical treatment under general anesthetic, whereas 44.9% of patients in the NHFD and 74% in the IHFD underwent spinal anesthesia (Figure 4).
Fracture Classification.

Abbreviations: IHFD, Irish Hip Fracture Database; NHFD, National Hip Fracture Database; UHF, University Hospital Freiburg.
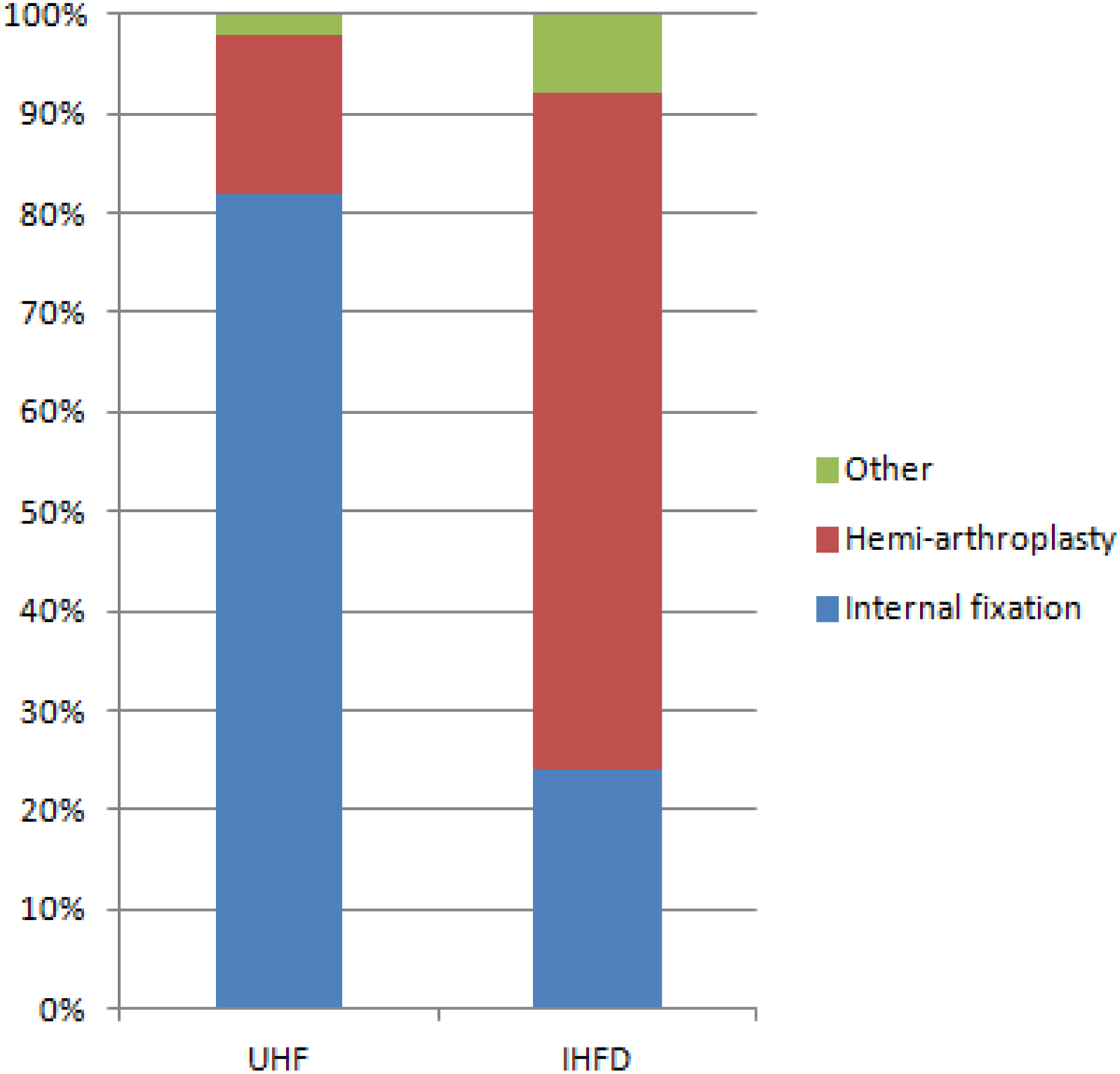
Proportion of hemiarthroplasty and internal fixation in undisplaced intracapsular fractures.

Proportion of THR in displaced intracapsular fractures. THR indicates total hip replacement.
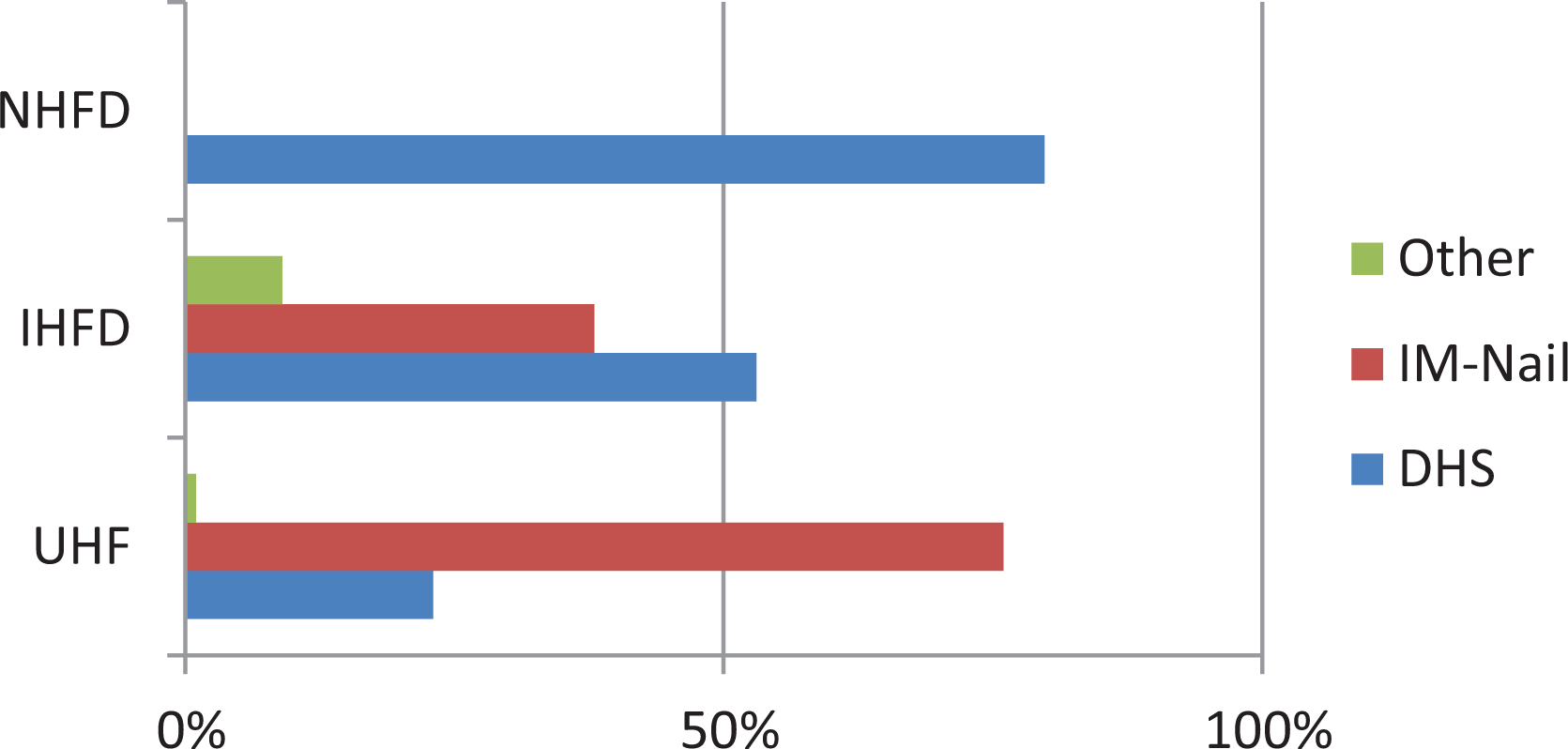
Proportion of DHS and IM-nailing for intertrochanteric fractures (no data reported on procedures apart from DHS for intertrochanteric fractures in the NHFD. 5 ). DHS, dynamic hip screw; IM, intramedullary; NHFD, National Hip Fracture Database.
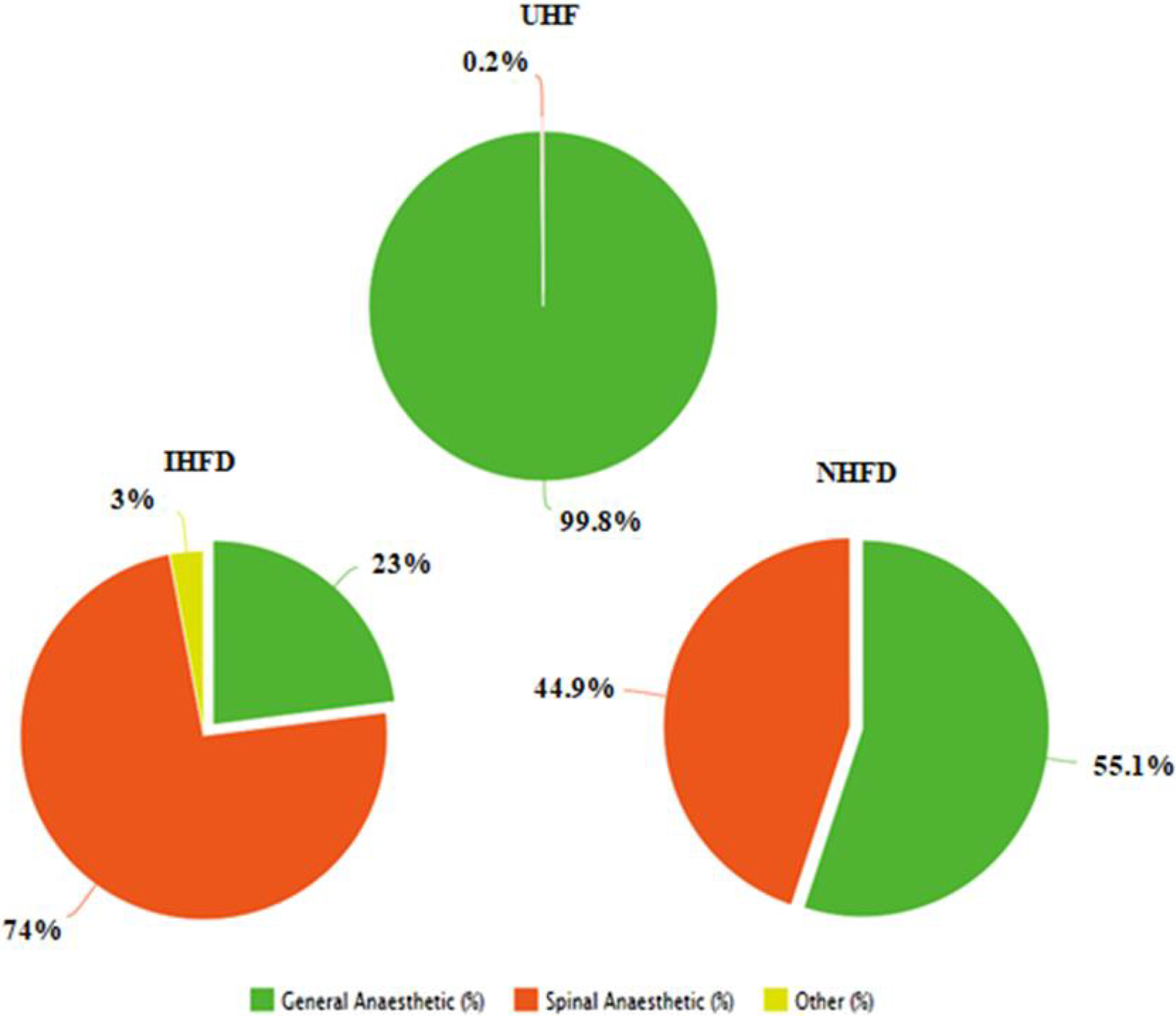
Anesthesia.
Adherence to the 6 Blue Book Standards
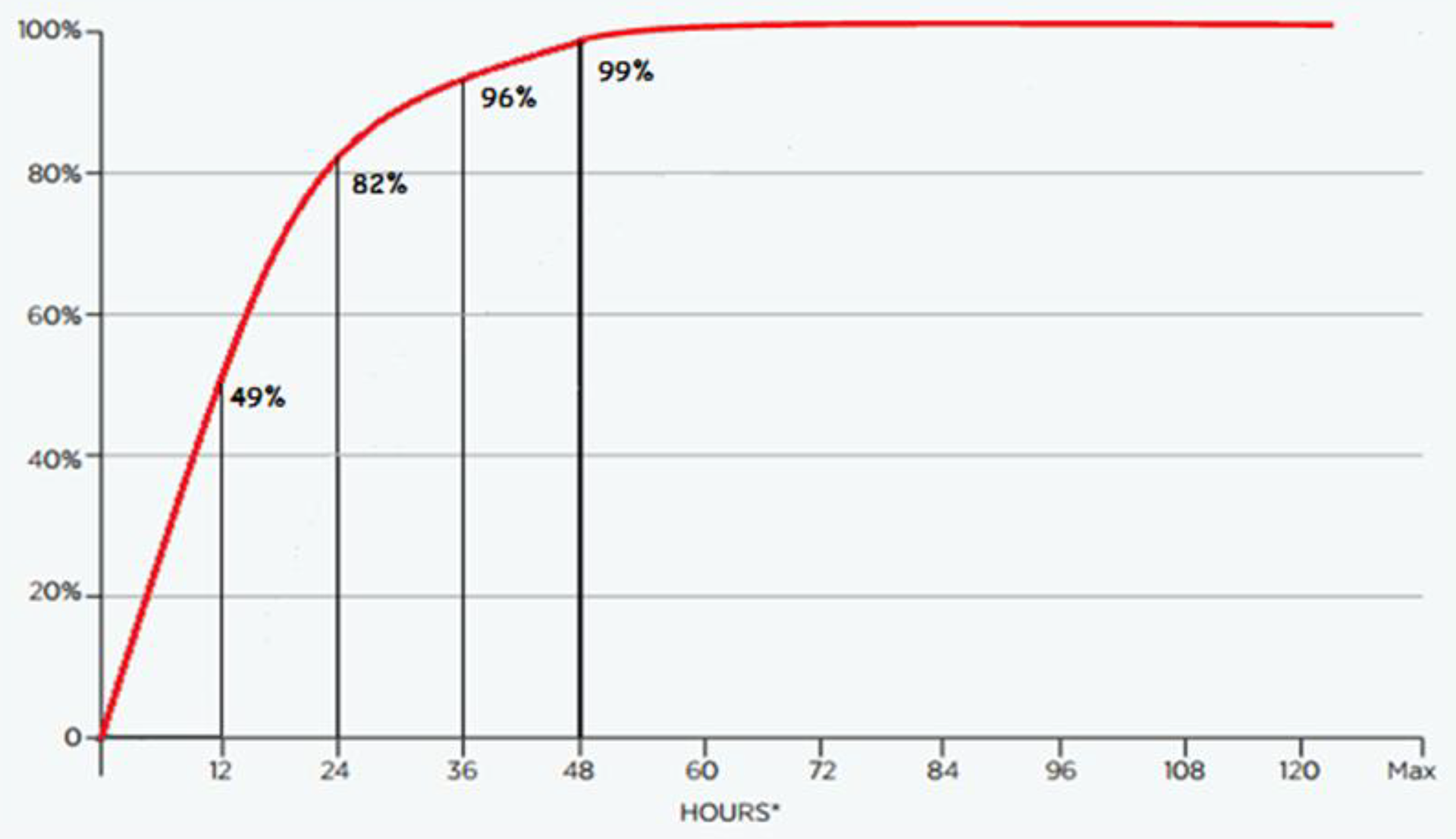
In the UHF audit, 60.5% of patients were admitted to the orthopedic ward within 4 hours, compared to 43.9% and 10% in the NHFD and IHFD, respectively. Ninety-eight percent of the patients were admitted via the ED, compared to 89% in the IHFD. 7 In the UHF audit, none of the patients were managed nonoperatively, compared to 4% in the IHFD 7 up to 10.5% of patients in the United Kingdom. 5 Almost half (49%) of the patients in the UHF audit received surgery within 12 hours. After 24 hours, 82% of patients had received surgical treatment, compared to 40% in the IHFD (Figures 5 and 6). After 36 hours, 95.8% of patients had received surgery, compared to 71.5% in the NHFD and 58% of patients in the IHFD; 98.9% of patients in the UHF received surgery within 48 hours of being admitted compared to 74% in the IHFD (Table 4). Out-of-hours surgical treatment is much more frequent in the UHF where 26% of patients received surgical treatment between 18:00 and 08:00; 97.1% of patients in the NHFD underwent surgery between 8:00 and 20:00. 5 In the IHFD, 72% of 74% of patients surgically treated within 48 hours underwent surgery between 8:00 and 17:59; 1.8% of 7 patients developed a new pressure ulcer, compared to 5.1% and 4% in the NHFD and IHFD, respectively (P = .451). None of the patients in the UHF were recorded to have been preoperatively assessed by a geriatrician, compared to 85.3% in the NHFD and 15% in the IHFD; 50.5% of patients were discharged on bone protection medication, compared to 68% in the IHFD and 79.3% in the NHFD. One hundred percent of patients received specialist falls assessment postoperatively in the UHF, compared to 97% in the NHFD and 48% in the IHFD (Table 4).

Cumulative time to surgery IHFD 7 percentages (n = 2812)*. IHFD indicates Irish Hip Fracture Database. *Excluding “not known” cases and patients not medically fit.
Cumulative time to surgery UHF percentages (n = 524)*. *Excluding “not known” cases and patients not medically fit. UHF indicates University Hospital Freiburg.
Adherence to the 6 “Blue Book” Standards.

Abbreviations: NHFD, National Hip Fracture Database; UHF, University Hospital Freiburg.
aExcluding patients not medically fit.
bOr referred for a dual-energy X-ray absorptiometry scan or bone clinic, or already were on appropriate medication.
Outcome Measures and LOS
The mean average acute LOS was calculated as 13.4 days in the UHF (n = 587). This compares to a mean average LOS of 16.4 in the NHFD (n = 64,864) 5 and 20 days in the IHFD (n = 2962). 7 The measures of outcome are summarized in Table 5.
Reoperation Rate Within 30 Days and In-Hospital Mortality Rate.

Abbreviations: IHFD, Irish Hip Fracture Database; NHFD, National Hip Fracture Database; UHF, University Hospital Freiburg.
aNHFD casemix-adjusted 30-day mortality rate.
Discussion
The 6 evidence-based Blue Book standards are included in the treatment standards recommended by the DGU for patients with hip fractures in German hospitals. 4,13 Our study has identified many differences in the care pathway of hip fractures between the United Kingdom, Ireland, and Germany despite these similar treatment guidelines. Regarding the data, the treatment pathway in the UHF collective of patients appears significantly faster. More than twice as many patients receive surgery within 24 hours (82%), compared to 40% of patients in the IHFD, and 95.8% of patients receive surgery within 36 hours, compared to 71.5% of patients in the NHFD. This difference can be explained by the requirement of external quality assurance for 95% of patients with hip fracture to be surgically treated within 24 hours (likewise 95% of all patients under oral anticoagulation therapies are to be surgically treated within 48 hours). For this reason, out-of-hours surgical treatment is practiced more commonly in the UHF where almost a quarter of patients receive surgery between 18:00 and 08:00. Shorter acute in-hospital LOS of 13.4 days may lead to fewer patients developing a new pressure ulcer in the UHF. None of the patients in the UHF collective receive routine preoperative OG assessment, which seems to reflect the lack of services in this hospital. Geriatric assessment seems more common in the United Kingdom where many units report daily OG ward round on weekdays. Altogether, 85.3% of patients in the NHFD are preoperatively assessed. In Ireland, OG assessment was only present in varying degrees in 2015 (15%), with only 1 OG locum consultant in the whole country 7 ; 50.5% of patients in the UHF are discharged on bone protection medication; however, it is unsure how many patients attend follow-up appointments with the general practitioner, receive appropriate outpatient bone assessment, or discontinue the recommended medication. Similar to the NHFD where 97% receive specialist falls assessment, 100% of the patients in the UHF audit receive this service postoperatively by a trained physiotherapist.
Patient demographics are similar between all data sets (67% of patients are female compared to 71.6% in the NHFD and 70% in the IHFD). Age distribution seems to be similar between the UHF and NHFD with a slightly younger patient population (43.2% younger than 80 years compared to 41% and 41% in the NHFD and the IHFD, respectively). Interestingly, half of all hip fractures in the UHF collective are classified as trochanteric fractures. However, in the NHFD, the most commonly sustained hip fracture seems to be displaced intracapsular neck fractures (49.1%), similar to the IHFD (37%). This difference might be explained by the significantly higher proportion of patients (17%) being transferred from other acute hospitals to the UHF because the patient is too sick for a district hospital or has multiple comorbidities. Some epidemiological studies have shown a higher proportion of trochanteric fractures in sicker patients. 15,16
Regarding the type of surgery, internal fixation is the surgery of choice (82%) for nondisplaced intracapsular fractures in the patient collective of the UHF, compared to the IHFD where the surgery of choice seems to be hemiarthroplasty (89%). A recent meta-analysis has shown an increased risk of mortality associated with hemiarthroplasty for undisplaced femoral neck fractures; therefore, it is not recommended as primary treatment. 17 Similar to the NHFD, more than a quarter (27% in the UHF compared to 26.9% in the NHFD) of patients are deemed eligible for a THR after an intracapsular displaced neck fracture. In the IHFD, 89% of displaced intracapsular fractures are treated with hemiarthroplasty and only 5% of patients received a THR, although studies have suggested the long-term results to be superior for THR in fit, independent patients with displaced intracapsular fractures. 18 Most intertrochanteric fractures (89%) in the UHF are treated with an IM-nail (PFNa; Depuy/Synthes), compared to the NHFD and the IHFD where 79.8% and 53% are treated with a DHS, respectively. Recent studies have shown IM-nailing to be associated with less blood loss and fewer complications in patients with intertrochanteric fractures; however, more research is needed due to heterogeneity of the skills of surgeons and different types of pertrochanteric fractures. 19 Intramedullary-nailing produces the best outcomes for patients with subtrochanteric fractures. All of the patients (n = 33) with subtrochanteric fractures in the UHF are treated with an IM-nail, compared to 82% in the IHFD and 79% in the NHFD. The exceptionally high rate (99.8%) of general anesthetic use in the UHF collective would suggest that the choice of anesthesia is driven by the preference of the department, rather than informed patient choice, which is the approach recommended by NICE. 6 This contrasts starkly to the IHFD where 74% of patients receive spinal anesthesia during surgical treatment. The significant difference in in-hospital mortality (7.1% in the NHFD, 5% in the IHFD, and 4.7% in the UHF; P = .003) suggests that delays in time to surgery and performing surgery exclusively during working hours may negatively affect patient outcome.
Considering the retrospective nature of our study, the data show several limitations. However, the main strength of this study is that it offers a direct comparison of the care pathways between 3 different European health-care systems. Considering the fact that some information was not consistently recorded in the electronic medical data for each individual patient in the audit, the sample size is less than the total sample size (n = 636) in the comparisons of source of admission, time to surgery, LOS, reoperation rates, and adherence to 5 Blue Book standards. Patients who were not medically fit to undergo surgery were not included in the NHFD, IHFD, and the UHF audit. Therefore, we were not able to determine the quantity of patients who were not medically fit for surgical intervention in our audit compared to the national registries. Additionally, the extent to which the findings in our collective can be compared to other German trauma units is uncertain, considering the fact that each hospital individually manages patients with hip fracture using the DGU guidelines 13 with or without an auditing program. The University Hospital of Freiburg is categorized as a maximum care hospital. Given that trauma units in Germany are divided into different care levels, it is conceivable that the quality of care at our trauma unit is not capable of being generalized to the whole of Germany.
Our study shows that in the UHF, the speed of surgical treatment appears to stand at a relatively high level (95.3% of patients receive surgical treatment within 36 hours). However, despite overwhelming evidence in the literature supporting OG models of care, none of the patients in the UHF collective received routine preoperative OG assessment, and the continuity of osteoporosis therapy remains questionable. Similar to other developed nations such as Japan, 20 there is a possibility of a gap in osteoporosis treatment after discharge. The “AltersTraumaRegister DGU” is a beginning in implementing an OG model of care in Germany similar to the United Kingdom and Ireland and shows potential to further optimize standard of care in individual hospitals by auditing patient outcome. Considering the relative population density, it is surprising that only 2 units in Germany have an FLS in place to ensure continuity of osteoporosis therapy compared to 4 units in Ireland. 14
Studies conducted within the United Kingdom as well as other countries have shown that continual nation-wide transparent auditing has been a catalyst to improve the quality of the care pathway for many elderly patients with hip fractures. 21,22 The speed of surgical care in the NHFD and IHFD has improved since implementing the auditing program; however, this study suggests there still remains room for further improvement. Pressure sores, infections, hospital stay, treatment cost, depression, and mortality are all directly related to delays in presentation and surgery. 22,23 In addition, OG assessment remains low in Ireland compared to the United Kingdom, with only 15% of patients receiving routine preoperative assessment.
Conclusion
Our study suggests there is potential for optimization and standardization of hip fracture management within Europe. Considering simplicity of data collection and given that many European countries are already participating in similar data collection programs, 24 -26 we see the possibility of developing an Europe-wide transparent database in the future. This could open up the possibility of including the United Kingdom and Irish experience into the care in Germany (and other participating countries) and vice versa. As a result, this could be a valuable tool for continually improving the acute care pathway as well as the long-term treatment of elderly patients with hip fractures, in accordance with the growing socioeconomic burden of hip fractures European countries are expected to face in the future. 1,27
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The article processing charge was funded by the German Research Foundation (DFG) and the University of Freiburg in the funding programme Open Access Publishing.