
Abstract
Background
Goal-oriented patientcare is a key element in qualityhealthcare. Medical-caregiver’s (MC) are expected to generate a shared decision-making process with patients regarding goals and expected health-outcomes. Hip-fracture patients (HFP) are usually older-adults with multiple health-conditions, necessitating that agreed-upon goals regarding the rehabilitation process, take these conditions into consideration. This topic has yet to be investigated by pairing and comparing the perception of expected outcomes and therapeutic goals of multidisciplinary MCs and their HF patient’s. Our aim was to assess in a quantitative method whether HFPs and their multidisciplinary MCs agree upon target health-outcomes and their most important goals as they are reflected in the SF12 questionnaire.
Methods
This was a cross-sectional, multi-center, study of HFPs and their MCs. Patients and MCs were asked to rate their top three most important goals for rehabilitation from the SF12 eight subscales: physical functioning, physical role limitation, bodily pain, general health, vitality, social functioning, emotional role limitation and mental health, and indicate their expected outcome. Descriptive statistics and mixed effect logistic-regression were used to compare concordance of the ratings. Agreement between patients and MCs was assessed using interclass coefficients (ICCs).
Results
A total of 378 ratings were collected from 52 patients, 12 nurses, 12 physicians and 6 paramedical personnel. Each patient had between 3 and 9 raters. Patients considered physical functioning and physical role limitation more important than did MCs. Physicians and nurses emphasized the importance of bodily pain while patients referred to it as relatively less significant. The total ICC was low (2%) indicating poor agreement between MCs and patients. With the exception of physical-functioning, MCs predicted a less optimistic outcome in all of the SF12's subscales in comparison to HFPs.
Conclusion
Effective intervention in HFPs requires constructive communication between MCs and patients. The study suggests that caregivers have an insufficient understanding of the expectations of HFPs. More effective communication channels are required in order to better understand HFPs’ needs and expectations.
Keywords
Introduction
Hospital admission rates of hip fracture (HF) patients have grown substantially in the past decade. 1 HFs in older adults are associated with poor outcomes, high costs and a lengthy rehabilitation process.2,3 Rehabilitation following HF has been geared toward reducing the impact of long-term disability, 4 improving the patients’ quality of life 5 and decreasing the risk of mortality. 6
Patients with HFs are usually older adults who often have multiple underlying conditions.7,8 Thus, defining the expected rehabilitative outcomes, 9 setting agreed-upon goals that take these complications into consideration is necessary. 10 Patients in rehabilitation following a HF maintain that setting goals helps facilitate recovery 11 ; In fact, achieving those goals has been categorized as the third and final stage of recovery after a HF and termed “gaining ground,” ie regaining control and independence. 12
Pre-operative patient expectations and the MC’s attitude regarding their patient’s expected outcomes have been associated with outcomes and patient satisfaction.13–16 Fulfillment of pre-orthopedic surgery expectations, such as reduction in pain or improved physical functionality, is usually associated with high patient-satisfaction and improved functionality.17,18 Thus, optimizing pre-operative expectations communication between patients and their MCs is a key element of quality-rehabilitative orthopedic care.
Qualitative studies have demonstrated that communication between MCs and HF patients is not always optimal and that MCs were unable to identify the patient’s needs.19,20 Although the MCs agreed that patients should be individually informed regarding their expected outcomes, they stressed that this information is not communicated to the patients and that the patients’ needs are not always heard.20,21 Additionally, orthopedic patients and their physicians had different outcome expectations from surgery.21,22 A Cross sectional study and a systematic review have shown that agreement between MCs and patients on treatment goals, and expected outcomes are associated with better health-outcomes, improved patient care, self-efficacy and self-management.23,24
Our aim was to investigate whether HF patients and their MCs agree upon target health-outcomes and their most important goals by using quantitative paired comparisons of the MC’s and their patient’s perception of the expected outcomes and goals.
Materials and Methods
Study Design and Setting
This cross-sectional study of HF patients and MCs took place in December 2021- June 2022, within two large tertiary medical academic health centers.
Participants
Patients over 60 years of age who were hospitalized with HF and who understood Hebrew and could sign an informed-consent form, were eligible to participate in the study. The patients were recruited when they were hospitalized in the Department of Orthopedics or Rehabilitation, 1–7 days after surgery. Medical, nursing and paramedical personnel (physiotherapy, occupational-therapy, social workers and clinical pharmacist), from the two medical centers, who work with HF patients on a daily basis were recruited to the study.
Variables
Data regarding patients’ demographic and medical history were gleaned from the electronic medical files, including age, sex, co-morbidities, fracture type, surgical approach, functional status, family support, and residence (home/nursing home) before the fracture. Retrospective data regarding pre-fracture mental component score (MCS) was collected with the Short Form 36 (SF36) questionnaire. Data regarding demographics and length of professional experience of MCs were obtained through questionnaires.
Questionnaires
Reuben & Jennings 25 proposed using patient reported outcome measures (PROs) for goal-setting and outcome evaluation. Kremenchutzky & Walt 26 and Ysrraelit et al. 27 have used this method while utilizing the Short Form 12 (SF12) questionnaire to examine and compare the perception of postoperative outcomes and quality of life among patients and their physicians. The SF12 questionnaire, is a shorter version of the SF36, that has been found suitable for measurement of PROs in patients rehabilitating from a HF.28,29 It consists of 12 questions in eight topics: physical functioning, physical role limitation, bodily pain, general health, vitality, social functioning, emotional role limitation and mental health. Interpretation of the results can be obtained from a calculation of each topic and a summarization of several topics that generate a physical component score (PCS) and the MCS. 30
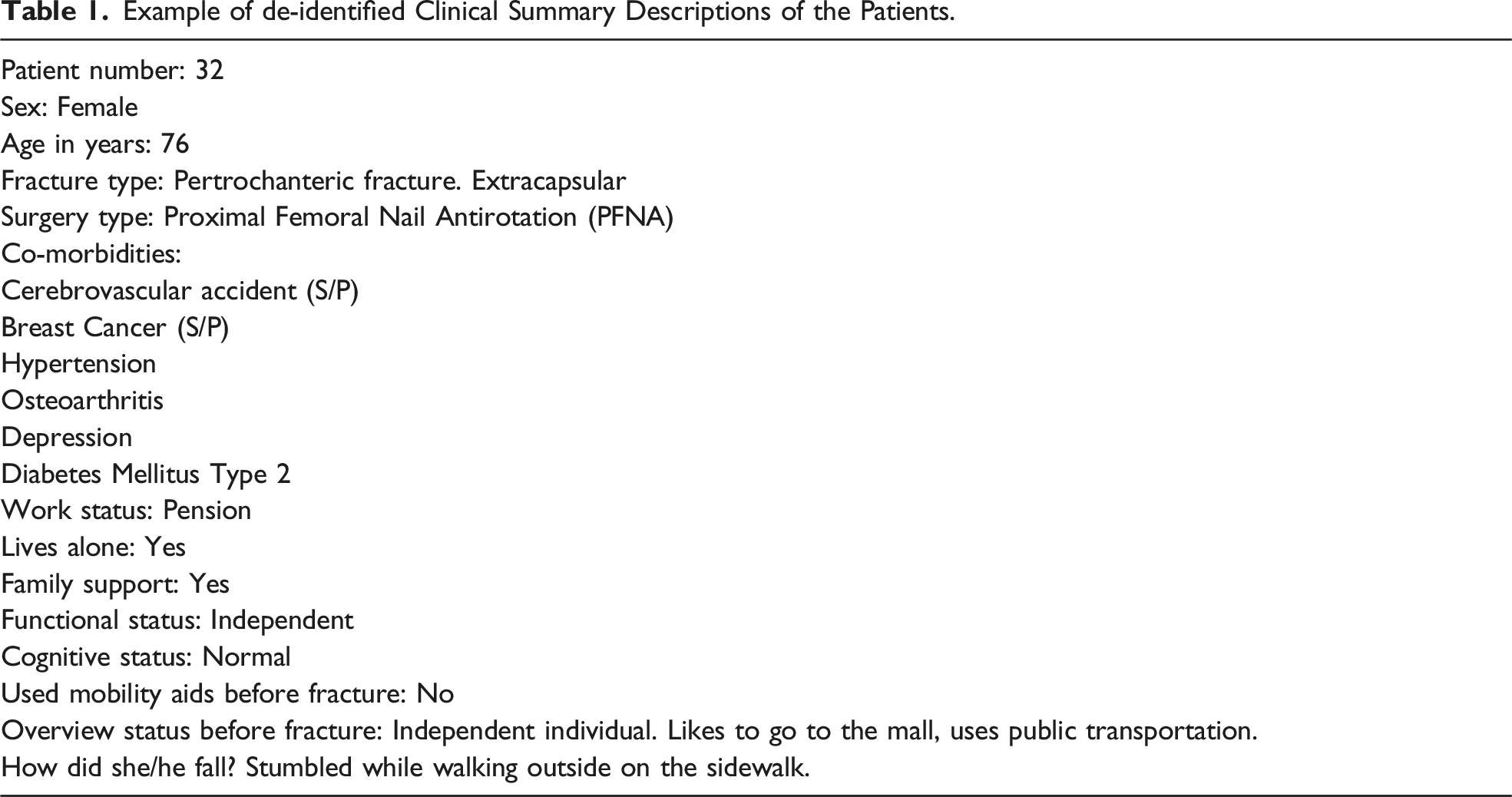
Example of de-identified Clinical Summary Descriptions of the Patients.
Data Measurement
Two main objectives were measured: 1. Expected outcomes: Patients (for themselves) and MCs (for their patients) were asked to answer the SF12 as they expect they would be 3 months after the fracture. SF12 data were scaled so possible scores ranged from 0 (poor health) to 100 (excellent health) for the eight domains. PCS and MCS were also calculated according to the RAND Corporation web site and the oblique (correlated) factor solution that is recommended for orthopedic patients.
31
2. Most important health goals: Validated translations of the SF12
32
health domains were detailed correlating with the eight subscales of the SF12. Patients were asked to rank their top three most important goals for rehabilitation from the list of the eight health domains; the MCs were asked to do the same for their patients. To avoid potential bias, both MCs and patients were masked as to the other’s responses.
Statistical Analysis
Descriptive statistics were used to outline the patients’ and MC’s demographics, medical history (for patients), and profession and length of experience (for the MCs). Proportions were measured to describe the three most important health domains of patients and MCs. Mixed effect logistic regression was utilized for comparison of concordance of the health domain ratings among patients vs MCs, in which the random effect was the patient, with a range of 3–9 raters.
In the univariable analysis step, mixed effect linear regression models were conducted to assess differences in concordance by clinical characteristics (fracture type, age, sex, professional experience) of expected outcomes and most important health goals. In the multivariable analysis step, age was added to the models and a sensitivity analysis that examined the effect of pre-fracture MCS on the outcomes.
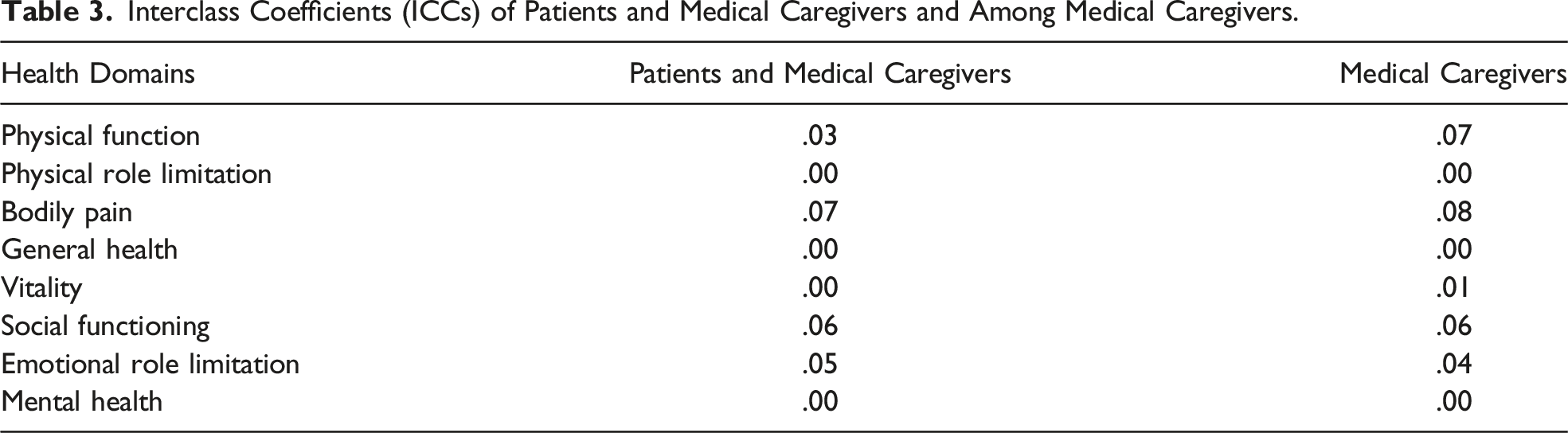
General agreement between patients and MCs and between MCs was assessed using interclass coefficients (ICCs) calculated from a two-way analysis of variance. The ICCs provided a measure of the degree of agreement between MCs and patients at an individual level. The maximum ICC is 1.00, reflecting 100% agreement. It is generally accepted in these kinds of assessments that ICC values of <.40, .41–.60, .61–.80 and .81–1.00 mean poor to fair, moderate, good or excellent agreement, respectively. 33
Analysis was performed using IBM SPSS for windows version 27 (IBM, Armonk, USA), and Stata version 15.0 (StataCorp. LP, College station, TX, USA).
Study Size
Sample size requirements were performed using Winpepi 11.65. Assuming an ICC of .7 with four raters: patient, physician, nurse and paramedical personnel; a significantly higher than .4 ICC; a risk level of 95%; and power of 80%, the study needed at least 44 ratings in each cluster. To enhance power eliminated inter-variance within professions this study used mixed raters and at least two raters from each MCs profession.
Ethics Approval and Consent of Participate
The study was approved by the ethics committees of the two medical centers. All participants provided written informed consent forms before enrolling in the study.
Results
A total of fifty-two patients, 12 nurses, 12 physicians and six paramedical personnel from two medical centers, participated in the study. Each patient had a range of 3–9 raters, a median of seven ratings per patient, ideally two raters from each sector to moderate the influence of possible extreme raters, for a total of 378 ratings in 52 groups (see Figure 1 for description of rating process). Clinical and demographic data of patients and MCs are presented in Table 2. The majority of the patients were female and over 80 years of age. Most of the patients had an extracapsular fracture (69%). All patients had undergone repair surgery, 39 of them had proximal femoral nail anti-rotation (PFNA), 11 had partial hip replacement and two had undergone total hip replacement. Prior to the fracture 56% of the patients walked independently and the remainder used a cane or a walker. About 94% of them lived at home and 5% still worked. Description of rating process. Participants’ Characteristics.

No significant differences in concordance of ratings of expected outcomes were found by sex, professional experience and fracture type. Age was found to be associated with ratings and accordingly was added in the multivariable analysis.
Comparison of Most Important SF12 Health Domains
As shown in Figure 2, the highest rated health domains were physical function and physical role limitation. Patients rated these goals as most important more frequently in comparison to the MCs. MCs and specifically physicians and nurses emphasized the importance of bodily pain while patients referred to it as relatively less significant. The paramedical personnel had the highest ratings for vitality, social functioning and mental-health in comparison to the patient’s and the other MCs professions. However, the differences were found to be statistically significant only for social functioning. The sensitivity analysis modified the difference in ratings of patients and their MCs in physical function, physical role limitation and mental health (P > .05) but strengthened the differences in general health and emotional role limitation (P < .05). Comparison of the three most important goals for patients; as rated by the medical caregivers and stratified to nurses, physicians and paramedical personnel.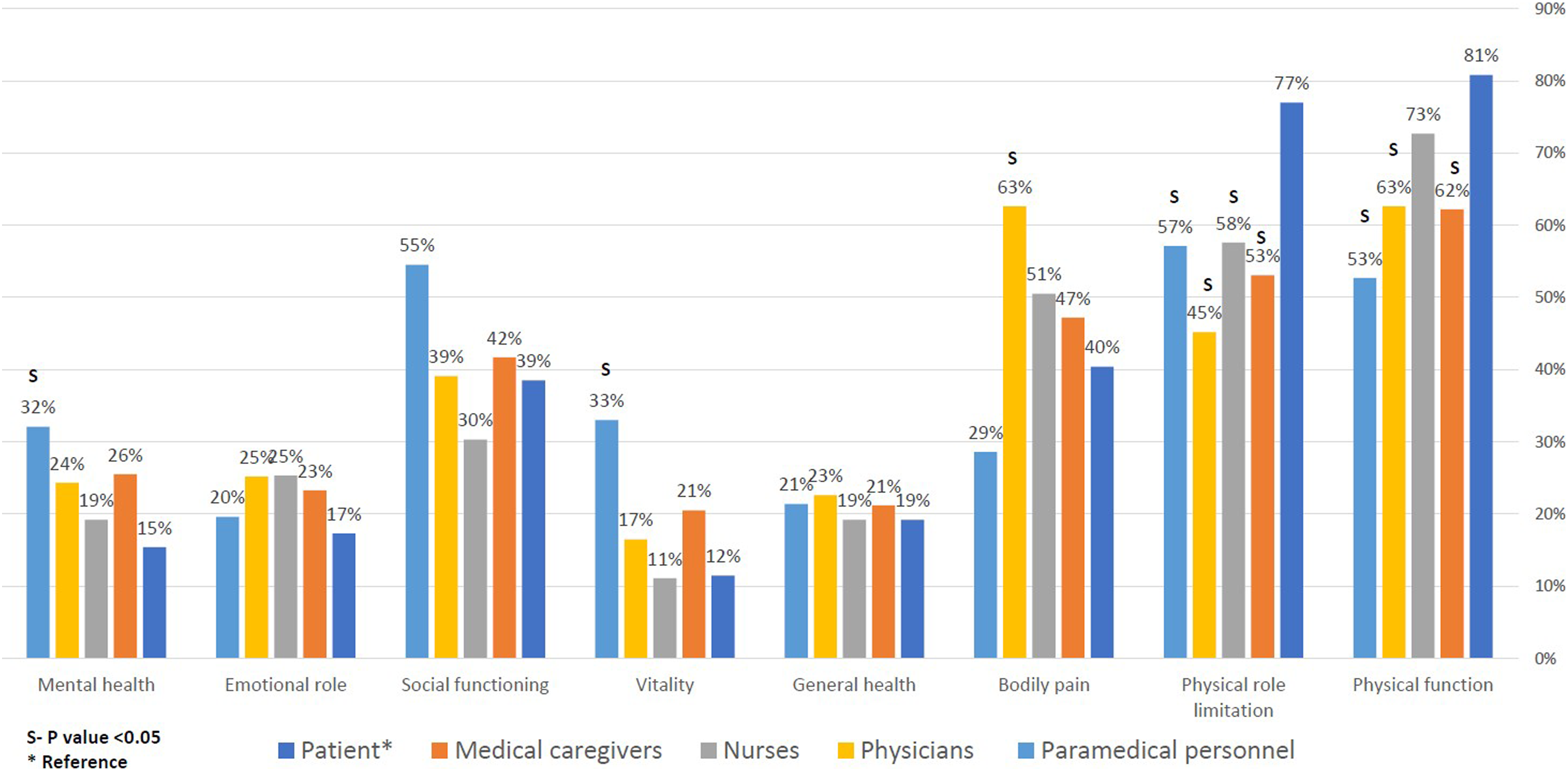
Expected Health Outcomes
Interclass Coefficients (ICCs) of Patients and Medical Caregivers and Among Medical Caregivers.
Comparison of Patient’s Mean Expected Outcomes, Adjusted to Age, as They Were Rated Using the SF12 by Patientss, the Medical Caregivers and Stratified to Nurses, Physicians and Paramedical Personnel.

S- Statistically significant, P value <.05 Mixed effect logistic regression, * Reference. PCS, physical component score; MCS, mental component score.
Discussion
This study examined agreement between the MCs and their patients regarding expected health outcomes after HF, as assessed by the SF12 questionnaire. The measures demonstrated a lack of concordance in the expected health outcomes of patients and their caregivers. Generally, patients rated their expected health outcomes as potentially better than did the MCs, though within the MCs there were differences in the ratings among physicians, nurses and paramedical personnel. Overall, physicians’ rates tended to be more closely aligned to the patients’ ratings, nurses tended to rate furthest from the patients and paramedical personnel were usually somewhere in the middle. Disagreement among MCs regarding medical goals has been documented before. 34 HF patients stressed the importance of ensuring all the MCs are “on the same page” regarding the therapeutic goals. 35 Further research should explore the meanings and implications of these differences within medical personnel groups.
Similar to our study, other16,36–39, orthopedic studies have found that patients have high outcome expectations. A qualitative study of HF patients reports that patients are confident that the current situation was just a “sudden interruption” in their daily life and that they will return to their previous routines and functionality within a few weeks.16,37 Aoude 38 found that patients undergoing spinal surgery were more optimistic than surgeons regarding their expected outcomes, such as regaining independence, general health and pain-management. A possible explanation for these differences is that patients are influenced by their previous experiences40,41 and MCs are influenced by their clinical experience and knowledge. 42
Research is divided regarding the management of patient’s pre-orthopedic surgery expectations. Coole 36 and Hoorntje 43 suggest that MCs should modify patients’ expectations so they won't be disappointed with the surgical outcomes and have higher satisfaction. Southwell 44 and Swarup 9 argue that an optimistic point of view can improve a patient’s post-op functionality.
To further understand the concordance among patients and caregivers of goals most important to HF patients, the second aim of the study was to compare agreement of the three most important health domains. The results yielded a mixed picture: although there was consensus among patients and MCs regarding the importance of the physical function and physical role limitation goals, there were differences in the frequency of the ratings. Furthermore, on an individual level there was no agreement between patients and MCs. This indicates that although there was concordance between MCs and patients about the importance of physical role limitation and physical function goals following HF, they failed to identify these goals on an individual level.
The third most frequently rated health domain was bodily-pain. Interestingly, nurses and physicians rated this goal as important to recovery following HF more frequently than did patients, indicating that clinicians overestimated the centrality of pain in post-HF patients. This phenomenon has been reported previously in orthopedic patients. 16 A possible reason for this is that patients underestimate the intensity and duration of pain in the postoperative course. Or alternatively, because patients expected the major trauma of having a HF to be painful, they did not rate it as frequently. 45
Qualitative studies of HF patients and their MCs also reported that MCs were unable to identify the patient’s needs.21,46 MCs recognized that although many times they think they know what HF patients’ needs are, they do not verify this with the patients themselves. The staff acknowledged that the treatment was targeted mainly to physical aspects of recovery as opposed to additional areas that require treatment such as mental and social capacities. 19 Some MCs even stated that they are in need for a change of mindset to better understand what HF patients experience. 47 In fact, HF patients also stress the importance of better communication with MCs regarding their needs and expected outcomes. In a cross-sectional study 78% of HF patients and 92% of their caregivers rated the importance of MCs hearing their wishes as “very important”. 47 These findings our mirrored by Asplin 35 qualitative study where HF patients emphasized the need of “being seen” by the MCs.
This study underlines the need to improve communication and systematic joint decision assessment of goals and expected outcomes for HF patients and enhance patient centered care. This issue is especially important due to the aging of the population worldwide, the surge of HF, the expected increase in patient involvement in their own rehabilitation and the growing use of patients of non-peer reviewed information on the internet as a source for medical-guidance that may alter their expectations.48-50 Others have shown that goal-setting by MCs in HF patients is often not based on fixed objective parameters that are evidence-based. 50 PROs enable a comprehensive assessment of the patient’s health status and can be used to establish joint decisions in goal setting. The initiation of a discussion with the patient regarding goals and expected outcomes in the rehabilitation process can improve the patient satisfaction, therapeutic alliance and treatment.
Strengths and Limitations
This study has several strengths that were not seen in previous studies. Others19,20,47 have published qualitative studies that evaluate patient or staff members perception of the expected outcomes following a HF. In this study the methodology was more robust, and included quantitative paired comparisons of the MCs and their patient’s perception of the expected outcomes and goals. The evaluation of the goals and the predicted outcomes were undertaken in a masked procedure, meaning that patients and MCs did not know the responses of others, thus enabling an unbiased approach where they were not influenced by others’ opinions. Others 51 have criticized the lack of representation of actual medical decision makers in similar studies. In this study, the MCs were recruited from the departments where the patients were hospitalized, hence are involved in their decision-making on a daily basis.
Using more than one rater per patient and from different healthcare professions enabled a greater variance in the answers, thus diminishing the possibility of bias by an extreme rater and enhancing the power. Others28,52 have stressed the importance of a multidisciplinary team approach when caring for HF patients, accordingly we included MCs from a wide range of healthcare sectors. The use of different professions from within the MCs, was not demonstrated in other studies that primarily focused on the physician’s perception, enabled a richer understanding of the communication between HF patients and the various caregivers. The use of de-identified clinical summary descriptions of real patients and the opportunity to pair the ratings of the different groups, allowed a more in-depth analysis that could compare the specific ratings of the different groups. However, the use of de-identified clinical summary descriptions can also be perceived as a limitation as judgment may have been limited because it was not based on not real-life interaction rather on the, clinical, social, and personal characteristics that were brought in the descriptions. Performing the sensitivity analysis with the pre-fracture MCS aimed to partially solve this limitation. Patients and MCs were recruited from two medical centers, and from acute and rehabilitation health care settings, thus presenting a diverse sample that enhances the ability for generalization. A possible limitation is that participants were all Hebrew speakers. We recommend that future research explore the relevance of our findings in different cultures and other languages. Another possible limitation is that the SF12 traditionally measures outcomes rather than predicting them. We chose to use this measure because it was found to be suitable for PROs measures in HF patients and hence illustrates the heterogenic expected outcomes of this population. Finally, the study was performed during the COVID-19 pandemic, which may have influenced patients and medical staff expected outcomes and goals.
Conclusions
Patient centered care requires effective communication between MCs and patients regarding expected outcomes and goals of treatment on an individual basis. The present study suggests that caregivers have an insufficient understanding of “what matters most” 53 to HF patients. More effective communication should be initiated to better understand the HF patients’ needs. Tools such as PROs can help better outline patients’ goals and needs. They can enhance communications in order to coordinate goals of care and meet realistic expectations on the part of patients and caregivers.
Footnotes
Acknowledgments
We thank the patients and the medical caregivers from the Orthopedic and Rehabilitation departments in Hadassah medical center and Sheba medical center for participating in the study.
Author Contributions
Study concept and design: HS, AI, ML, EZ, OP, and OO. Acquisition of data: HS, WA, AI, and EZ. Analysis and interpretation of data: HS, AI, EZ, WA, ML, and OP. Drafting of the manuscript: HS, AI, DJ, OO, ML, EZ, and WA. Critical revision of the manuscript for important intellectual content: HS, AI, ML, EZ, OO, and OP.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the ethics committees of the two medical centers (#SMC-7933-20 and #HMO-0691-21). All participants provided written informed consent forms before enrolling in the study.