
Abstract
Objective
To provide pooled evidence on the association between central sarcopenia and risk of mortality and/or complications among geriatric patients with moderate to severe trauma.
Methods
We conducted a systematic search in PubMed, EMBASE, and Scopus databases for relevant observational studies documenting the association of central sarcopenia with the risk of mortality and/or complications in geriatric patients with moderate to severe trauma. The studies reported computerized tomography (CT) based assessments of the psoas muscle cross-sectional area. We used a random effects model for the analysis and reported effect sizes as pooled odds ratios (ORs) or hazards ratios (HRs) along with 95% confidence intervals.
Results
We analyzed data from 13 studies and found an association between the presence of psoas muscle size reduction and the risk of in-hospital mortality (OR, 1.47; 95% CI, 1.13, 1.90). In addition, we found increased risk of mortality within 24 months of follow-up in patients with sarcopenia (HR, 2.40; 95% CI, 1.11-5.17). We found each unit increase in psoas muscle cross-sectional area to be significantly associated with reduced risk of mortality within 24 months of follow-up (HR, .92; 95% CI, .90-.95). Patients with sarcopenia also had an increased risk of complications (OR, 1.69; 95% CI, 1.08-2.63).
Conclusion
Central sarcopenia, assessed using psoas muscle morphology, among geriatric patients with moderate to severe trauma appears to be significantly associated with increased risks of mortality and complications.
Keywords
Introduction
Improvements in medical care and living environments have enhanced human longevity 1 and resulted in an increased elderly population global burden due to the negative effects of ageing on physical and mental health.1,2 Individuals of Europe, USA and Asia older than 70 have become the fastest growing population in those areas. 3 According to estimates, around 20% of the global population will be comprised of adults aged 60 years and above by the year 2050. 4
There is also an increase in the number of elderly patients presenting to trauma centers,5-8 and the Global Burden of Disease study (2019) found that death rates fell considerably among older adults between 1990 and 2019. 3 Interestingly, during the same period, the mortality rates due to falls increased. 3 Traumatic injury events in elderly individuals are associated with increased risk of complications and mortality.8,9 Studies on elderly populations have shed light into the concept of frailty as a potential driver of adverse outcomes in individuals with underlying diseases such as kidney disease, malignancy, and cardiovascular disease.10-13 Frailty is diagnosed in individuals with difficulties executing activities of daily living, reduced ambulation, unexplained weight loss, and presence of weakness, as indicated by diminished grip strength and a general feeling of exhaustion. 14 An assessment of frailty based on these parameters is often challenging in trauma patients, and, the association of sarcopenia with outcomes in such patients has been difficult to study. Attempts at identifying a reliable proxy for frailty without the need for active participation of the patient and useful in trauma patients (ie, central sarcopenia detection using radiography) have been made.
Central sarcopenia, as determined by psoas muscle morphology, has been associated with poor disease outcomes.15-18 Sarcopenia in the psoas muscle is typically measured through imaging modalities such as CT or MRI at the L3-L4 vertebral level. 19 The assessment involves determining the cross-sectional area or volume of the muscle. To classify individuals as having sarcopenia, age-specific cut-off values are employed, often based on percentile comparisons with reference populations. Sarcopenia in the psoas muscle can also be assessed by normalizing the cross-sectional area (CSA) for height. By dividing the psoas muscle CSA by a person's height, researchers can obtain a more standardized measure that accounts for individual variations in body size. However, it's crucial to note that exact methodologies and cut-off values may vary across studies, and adherence to standardized protocols is essential for accurate and meaningful comparisons of sarcopenia prevalence and severity in this muscle group.
Studies have attempted to document the association between central sarcopenia and trauma patient outcomes among the elderly, but their findings have not been systematically synthesized to derive meaningful lessons for clinical practice. Thus, we designed a meta-analysis to include findings from all relevant studies and assess whether sarcopenia measured by psoas muscle morphology is significantly associated with adverse outcomes in geriatric trauma patients.
Methods
Selection of Studies
We conducted a systematic review in PubMed, EMBASE and Scopus databases to identify relevant studies published in English until the 15th of March 2023. Online Supplementary Table 1 presents our search strategy in each of these databases. We registered our protocol at PROSPERO (registration number CRD42023411973) and followed the standard PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines to conduct this review. 20
Selection of Studies and Data Extraction
We included studies that used psoas muscle morphology as a marker for sarcopenia assessment. The studies should have utilized standardized protocols or validated methods for sarcopenia assessment. Studies using imaging modalities (e.g., computed tomography (CT), magnetic resonance imaging (MRI), ultrasound) to assess psoas muscle cross-sectional area, volume, or density were eligible to be included. We were interested in studies documenting the association of sarcopenia with risk of mortality and/or complications in geriatric patients with moderate to severe trauma. We did not select studies that specifically focused on hip trauma/fractures because a systematic review on this issue has recently been published. 21 However, to the best of our knowledge, the evidence in elderly patients with general trauma and more than one organ system affected have not been synthetized. Observational cohort, case-control or cross-sectional studies were eligible for inclusion. We did not exclude any studies on the basis of their criteria for reporting sarcopenia.
After obtaining the search results from all databases, we removed the duplicates. Two study authors independently screened the titles and abstracts of the remaining unique studies. After screening the titles and abstracts, we retrieved full texts and reviewed them independently to obtain the final set of selected studies and extract their data using a pre-tested sheet. All disagreements or discrepancies related to any of the steps mentioned above were resolved by discussions between two authors and/or a third senior author.
Statistical Analysis and Quality Assessment
We conducted all analyses using STATA 16 software (TX, USA). We expressed pooled effect sizes as odds ratios (ORs) or hazards ratio (HRs) along with 95% confidence intervals. We decided a priori to use a random effects model for the analysis as the included studies differed in characteristics such as the mean age and genders of participants, the study settings, and the methods for assessing and defining sarcopenia. We anticipated that these differences might lead to substantial heterogeneity in the reported findings. To assess publication biases, we used Egger’s test, and we visually inspected funnel plot symmetries. 22 Finally, we used the Newcastle-Ottawa scale to assess the risk of bias. 23
Results
We retrieved 1104 studies through the search strategy from the three databases. We removed 217 duplicates and screened the titles and abstracts of 887 studies for relevance. This step led to further exclusion of 834 studies. We reviewed the full text of the remaining 53 studies and excluded another 40 (Figure 1) to include a total of 13 studies in our analysis.24-36 Selection process of studies included in the review.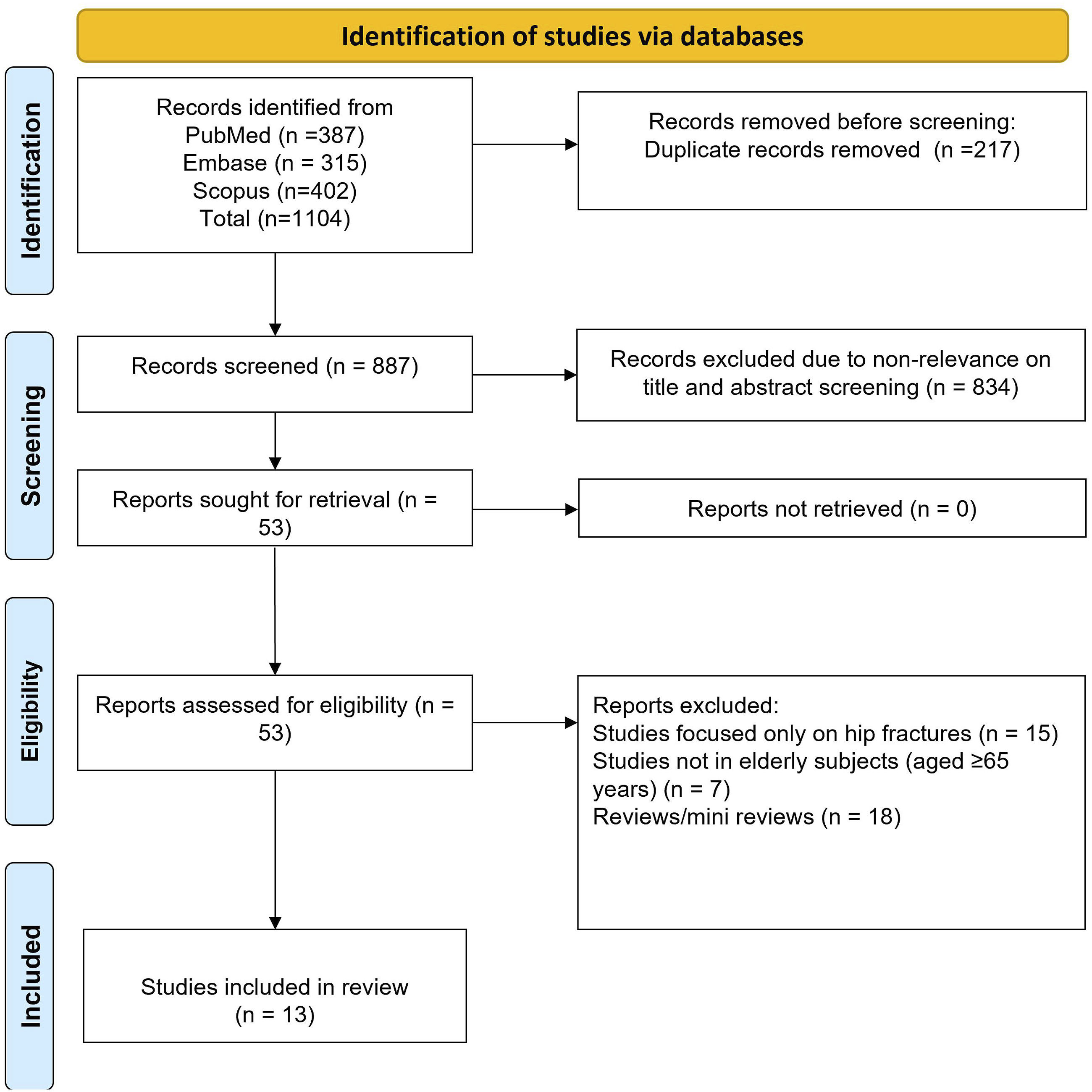
Summary of the Studies Included in the Meta-Analysis.

Mortality Outcome
We found that trauma patients with sarcopenia had an increased risk of in-hospital mortality (OR, 1.47; 95% CI, 1.13, 1.90; n = 7; I
2
= 20.3%) (Figure 2). There was no evidence of publication bias, either on visual inspection of the funnel plot or on Egger’s test results (P > .05) (Online Supplementary Figure 1). In addition, we examined the association between unit increase in lean psoas muscle cross-sectional area and risk of in-hospital mortality, but we found no statistically significant association (OR, .92; 95% CI, .78, 1.09; n = 2; I
2
= 94.0%) (Online Supplementary Figure 2). Risks of in-hospital mortality among elderly patients with trauma and associated sarcopenia and those without sarcopenia.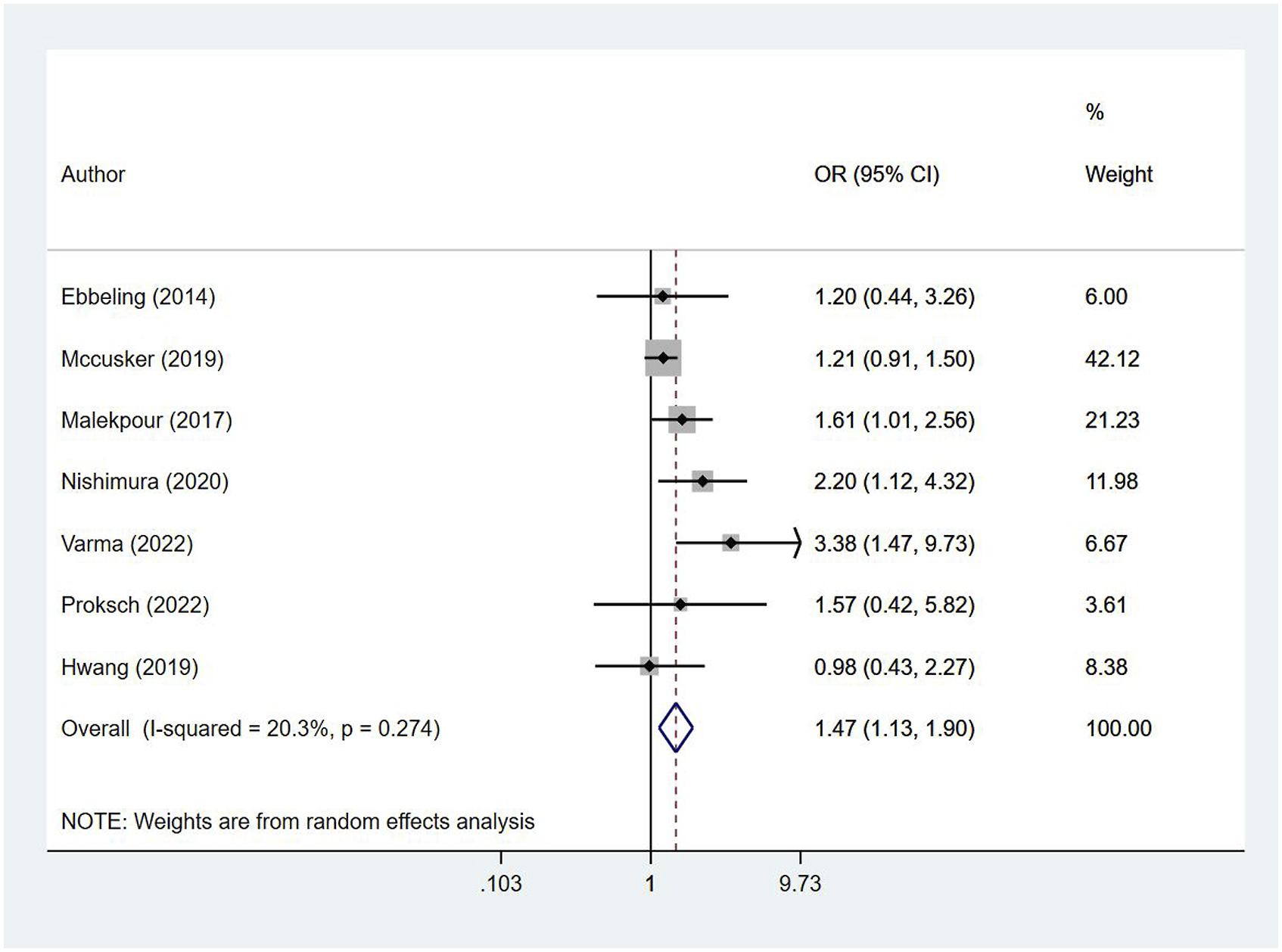
We also found an increased risk of mortality within 24 months of follow-up after hospital discharge in elderly patients who had sarcopenia using a pooled analysis (HR, 2.40; 95% CI, 1.11, 5.17; n = 5; I
2
= 74.6%) (Figure 3). We did not note any evidence of publication bias (Egger’s P value >.05) (Online Supplementary Figure 3). We found that each unit increase in psoas muscle cross-sectional area was significantly associated with a reduced risk of mortality within 24 months of follow-up after hospital discharge (HR, .92; 95% CI, .90, .95; n = 3; I
2
= 23.0%) (Online Supplementary Figure 4). Risks of mortality within 24 months of follow-up after hospital discharge among elderly patients with sarcopenia and those without sarcopenia.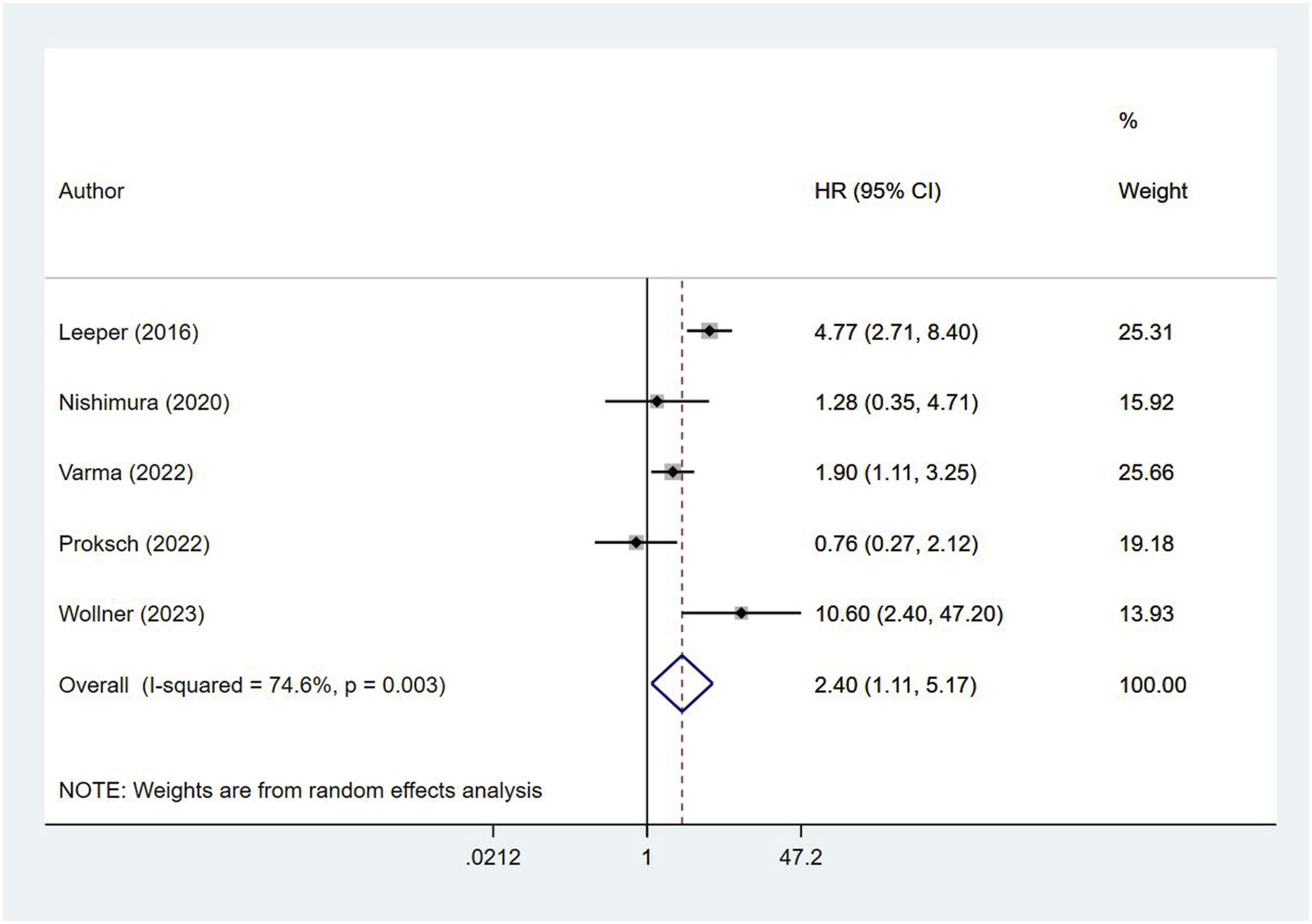
Morbidities and Complications
Elderly patients with sarcopenia had a higher risk of complications than those without sarcopenia (OR, 1.69; 95% CI, 1.08, 2.63; n = 5; I
2
= 79.2%) (Figure 4). The reported complications were mainly respiratory-related (pneumonia, pulmonary embolism), thromboembolism, hemorrhage, sepsis, urinary tract infections, myocardial infarction, heart failure, and acute kidney injury (Table 1). We found no evidence of publication bias, either upon visual inspection of the funnel plot or on Egger’s test (P > .05) (Online Supplementary Figure 5). Risks of complications among elderly patients with trauma and associated sarcopenia and those without sarcopenia.
Discussion
Our meta-analysis results indicate that central sarcopenia is associated with an increased risk of mortality, both short term (in-hospital) and long term (within 24 months of hospital discharge) in elderly patients with moderate to severe trauma. In addition, the risk of complications was also high in the elderly trauma patients with sarcopenia. Our findings suggest that sarcopenia, as assessed by a single radiological measurement, may be a reliable predictor of frailty and trauma outcomes in elderly patients and that it may be useful as a standalone measure to avoid using a plethora of biochemical and physical assessment variables. Our findings are similar to those in the review by Chiang et al, in which the authors showed that older adults with hip fracture and associated sarcopenia have a poorer postoperative functional recovery than those without sarcopenia. 21
Dealing with patients trauma is challenging due in part to the substantial variation in the types, severity, extent, and distribution of their injuries, all of which can make decision-making and prognoses difficult. Assessing sarcopenia on the basis of psoas muscle area measurements in trauma patients has practical advantages. For example, radiological examinations, including CT scans that show psoas characteristics, are often needed during the initial evaluation,37,38 and these objective assessments can be performed even in immobilized patients with trauma. Central sarcopenia has been used for predicting outcomes in several patient groups, and a reduced psoas muscle cross-sectional area has been associated with poor outcomes in patients with pancreatic and gastric cancer, pathological fractures, elective abdominal aneurysm repair, and hepatic transplantation.39-43 We propose that combining an objective assessment of central sarcopenia with a clinical frailty score may result in an accurate multi-dimensional frailty assessment. This, may facilitate clinical decision-making and prognostication. Moreover, such an approach may aid in identification of patients that require multi-disciplinary interventions and those that require conservative monitoring, discharge planning, and continued follow-up.
We found that patients with sarcopenia, according to the radiological psoas size measurement, had increased risks of complications related to infections, sepsis, and thromboembolism compared to patients without sarcopenia. Previous evidence indicates that frailty is associated with abnormalities in both innate and adaptive immunity that affect immune responses44-46 and may explain the patients’ increased risk of infectious complications. In addition, elderly individuals with sarcopenia and frailty may not recover their mobility early and may need prolonged use of indwelling urinary catheters, leading to increased risks of kidney infections. Delayed mobilization may also be a predisposing factor for thromboembolism. 47
The studies considered in this review did not include subjects with congenital/developmental neuro muscular disorders or systemic muscle wasting diseases in whom pre-existing sarcopenia may be expected. However, it is important to note that adjusting for expected pre-existing sarcopenia requires careful consideration. Since sarcopenia may already be present due to the underlying condition, it's essential to differentiate between disease-related muscle wasting and age-related sarcopenia. One of the ways to do so is to utilize age-specific reference standards for muscle measurements. This allows us to compare the subjects muscle characteristics with what would be expected for individuals of the same age, helping to separate disease-related changes from normal age-related changes. Another way could be to assess muscle quality, such as muscle density or fat infiltration, through imaging techniques like CT or MRI. This is because muscle quality can differ between disease-related and age-related muscle changes.
We are aware of the limitations of our meta-analysis. First, most analyzed studies were retrospective in design and unadjusted confounders may have had an impact on our results. Second, we found considerable heterogeneity (>50%) for the outcomes in the studies included; possibly be due to methodological differences among them (different cut-offs for sarcopenia definition, and different treatments and assessment time points for outcomes). Therefore, these differences need to be considered before generalizing our findings in other contexts. Third, we used “overall complications” as an outcome and did not focus on individual complication risks. While this approach may be questioned, we think presenting data on complications as an aggregate is appropriate as it reflects the overall patient condition and host response to trauma. Fourth, all the studies included were conducted in high income settings, particularly in the USA. This limits the external generalizability of the findings, which may not be applicable to low- and middle-income settings. Fifth, the sarcopenia diagnoses in the studies were based on the psoas muscle cross-sectional area assessed bilaterally and, in some studies, this measurement was normalized for height. However, most studies failed to consider the quality of the psoas muscle. Muscle quality is an important index of functionality that has a role in contributing to an individual’s fitness. It's also important to note that muscle mass and muscle strength are positively correlated, but they are not one and the same. Generally, individuals with larger muscle mass tend to have greater muscle strength. However, the relationship between muscle mass and muscle strength can be influenced by various factors. These factors include neural adaptations, muscle fiber type, neuromuscular coordination, and muscle quality (which includes factors like fat infiltration and fibrosis within the muscle). Finally, only some included studies were adjusted for comorbidities while exploring the association between sarcopenia and outcomes in the elderly trauma patients. The presence of comorbidities in this high-risk age group may have influenced the observed association.
Conclusion
On the basis of our findings, central sarcopenia is associated with increased risks of mortality and complications in elderly patients with moderate to severe trauma. Individuals with sarcopenia, according to CT-based assessments, should be kept under careful supervision and follow-up. Heterogeneity in the cut-offs used to define sarcopenia may reduce the validity of our findings; however, this highlights the need for global scale standard cut-offs. Future prospectively conducted studies should conclusively establish any causal associations between the presence of comorbidities, sarcopenia, and adverse trauma outcomes in elderly patients.
Supplemental Material
Supplemental Material - Psoas Muscle Morphology as a Sarcopenia Marker to Predict Outcomes of Geriatric Trauma Patients: A Systematic Review and Meta-analysis
Supplemental Material for Psoas Muscle Morphology as a Sarcopenia Marker to Predict Outcomes of Geriatric Trauma Patients: A Systematic Review and Meta-analysis by Yang Wang, Lei Li, Qinmei Pan1, Ying Zhong, and Xinmei Zou in Geriatric Orthopaedic Surgery & Rehabilitation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.