
Abstract
Background
Poor pain control and opioid use are risk factors for perioperative neurocognitive disorders (PND). The peripheral nerve block (PNB) can reduce pain and opioid consumption. This systematic review aimed to investigate the effects of PNB on PND in older patients with hip fractures.
Methods
The PubMed, Cochrane Central Registers of Controlled Trial, Embase and ClinicalTrials.gov databases were searched from inception until November 19, 2021 for all randomized controlled trials (RCTs) comparing PNB with analgesics. The quality of the selected studies was assessed according to Version 2 of the Cochrane tool for assessing the risk of bias in RCTs. The primary outcome was the incidence of PND. Secondary outcomes included pain intensity and the incidence of postoperative nausea and vomiting. Subgroup analyses were based on population characteristics, type and infusion method of local anesthetics, and type of PNB.
Results
Eight RCTs comprising 1015 older patients with hip fractures were included. Compared with analgesics, PNB did not reduce the incidence of PND in the elderly hip fracture population comprising patients with intact cognition and those with pre-existing dementia or cognitive impairment (risk ratio [RR] = .67; 95% confidence interval [CI] = .42 to 1.08; P = .10; I2 = 64%). However, PNB reduced the incidence of PND in older patients with intact cognition (RR = .61; 95% CI = .41 to .91; P = .02; I2 = 0%). Fascia iliaca compartment block, bupivacaine, and continuous infusion of local anesthetics were found to reduce the incidence of PND.
Conclusions
PNB effectively reduced PND in older patients with hip fractures and intact cognition. When the study population included patients with intact cognition and those with pre-existing dementia or cognitive impairment, PNB showed no reduction in the incidence of PND. These conclusions should be confirmed with larger, higher-quality RCTs.
Background
Hip fractures is the most frequent indication for emergency orthopedic surgery in people over 50 years.1,2 With an expected increase in the elderly population, the incidence of hip fractures is also expected to be the highest in people aged above 65 years. 3 Perioperative neurocognitive disorders (PND) are the most common perioperative complications of hip fractures, namely cognitive decline diagnosed preoperatively (known as neurocognitive disorder), any acute event (postoperative delirium), and cognitive decline diagnosed within 30 days after the procedure (delayed neurocognitive recovery) or within 12 months postoperatively (postoperative neurocognitive disorder). 4 PND prolong the length of hospital stay, increase the incidence of postoperative complications and mortality, 5 and are associated with the development of dementia later in life. 6 There are many risk factors for PND, including advanced age, pre-existing cognitive impairment, American Society of Anesthesiologists (ASA) grade 3 or 4, 7 pain intensity, and opioid use.
Hip fractures cause moderate-to-severe pain. 8 The analgesic effect of peripheral nerve block (PNB) has been shown in previous studies.9–11 Compared to opioids and nonsteroidal anti-inflammatory drugs (NSAID), PNB provides precise analgesia, improves patient mobility, and reduces the risk of systemic adverse effects.12–15
According to a Cochrane systematic review, 16 in adult patients with hip fractures and intact cognition, PNB reduced movement-related pain within 30 min after block placement and decreased the risk of acute confusion. However, most patients with hip fractures are elderly, and half of the patients with hip fractures are diagnosed with pre-existing dementia at >70 years. 17 The effects of PNB on PND in older patients with hip fractures and pre-existing dementia or cognitive impairment are unknown.
Therefore, this systematic review and meta-analysis aimed to determine the effects of PNB on PND, pain relief, and complications in older patients with hip fractures, including patients with intact cognition and those with pre-existing dementia or cognitive impairment, by comparing PNB with other analgesics.
Methods
This review was performed according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines. 18 The protocol for the present meta-analysis was registered before data extraction in the Prospective Register of Systematic Reviews database.
Search Strategy
Electronic databases were searched to identify relevant studies. A systematic search of PubMed, Cochrane Central Registers of Controlled Trial, Embase, and ClinicalTrials.gov were performed from database inception until 19 November 2021 without restrictions on language or publication type. The non-English studies were translated by an online translator. The search was conducted using Medical Subject Headings (MeSH) and the following free text keywords: hip fractures (MeSH), trochanter fractures, subtrochanteric fractures, intertrochanteric fractures, anesthesia conduction (MeSH), nerve block, femoral block, fascia iliaca compartment block, and FICB. The search strategy is provided in the supplementary file.
Study Selection
Two investigators independently reviewed the titles and abstracts to exclude irrelevant studies. The inclusion/exclusion of studies was determined by consensus or discussion with a third review author. Randomized controlled trials (RCTs) were eligible if they met the following criteria for inclusion: (1) patients: elderly patients (≥65 years) with hip fractures, including those involving the femoral head, femoral neck, trochanters, intertrochanteric or subtrochanteric region, (2) intervention: peripheral nerve block of any type performed from the time of injury to the time of discharge, (3) comparison: analgesics of any type (opioids, NSAID, and paracetamol), (4) outcomes: at least one type of PND outcome was assessed using any scale. We excluded (1) studies of patients with polytrauma or those requiring additional surgery apart from hip surgery and (2) ongoing trials or unpublished research.
The primary outcome of this review was PND incidence. The secondary outcomes included pain intensity at various time intervals, assessed using any scale, and incidence of postoperative nausea and vomiting (PONV).
Data Extraction
Two investigators independently extracted the data using a standardized data extraction table. Disagreements were resolved by discussion until consensus was reached or by consulting a third author. The following data were extracted from each eligible study: (1) first author’s name, (2) year of publication, (3) country, (4) study design, (5) patient characteristics (sample size, age, and sex), (6) types of PNB and local anesthetic, (7) intervention period of PNB, (8) the dosage of local anesthetic, (9) injection method of local anesthetic, and (10) outcomes.
Study Quality Assessment
Two investigators independently assessed the quality of the selected studies according to Version 2 of the Cochrane tool for assessing the risk of bias in randomized trials. 19 Disagreements on the risk of bias were adjudicated by a third author. Items were classified under three categories: low, unclear, and high risk of bias. The following characteristics were evaluated: random sequence generation (selection bias); allocation concealment (selection bias); blinding of participants and personnel (performance bias); incomplete outcome data (attrition bias); and selective reporting (reporting bias). All bias results from these questions were graphed and assessed using Review Manager 5.4.1 (Review Manager [RevMan], Version 5.4.1, Cochrane Collaboration, 2020).
Statistical Analysis
Statistical analysis of the pooled data was performed using Review Manager version 5.4.1 (RevMan, Version 5.4.1, Cochrane Collaboration, 2020), and the random-effects model was used to analyze continuous and dichotomous outcomes. Weighted mean difference (WMD) with a 95% confidence interval (CI) was calculated for continuous outcomes, and risk ratio (RR) with a 95% CI was calculated for dichotomous outcomes. P < .05 was regarded as statistically significant. Heterogeneity between studies was quantified using the I2 statistic, and significant heterogeneity was deemed present for I2 >50% and P < .1. Subgroup analyses were performed to investigate the heterogeneous control interventions. Subgroup analysis was based on the population characteristics of studies (older patients with hip fractures with intact cognition vs older patients with hip fractures including those with intact cognition and those with pre-existing dementia or cognitive impairment), types of PNB (fascia iliaca compartment block [FICB] vs femoral nerve block [FB]), PNB infusion methods (single injection vs continuous infusion), and types of local anesthetic (ropivacaine vs bupivacaine). Publication bias was assessed using funnel plots. In addition, the sensitivity analysis were performed to investigate the influence of individual studies on the pooled results by excluding differences in PND types and two perioperative period phases in which local anesthetics were administered.
Results
Study Selection
The database search yielded 1911 studies. A total of 1213 abstracts were screened after removing duplicates. After screening, 91 potentially relevant studies were included and 72 were excluded because they were considered irrelevant for this review. Nine studies20–28 did not fulfil the inclusion criteria, and data from two studies29,30 could not be extracted. Eight studies31–38 comprising 1015 older patients with hip fractures were included in this systematic review and meta-analysis. The included studies were published between 2007 and 2021. PNB was administered to 512 older patients, whereas 503 older patients received analgesics for hip fractures. The trial selection process was illustrated in Figure 1. The flowchart for study screening and selection process according to the PRISMA guidelines.
Study Characteristics
Study Characteristics of all Studies Included in this Systematic Review.

BIS, bispectral index; FB, femoral nerve block; FICB, fascia iliaca compartment block; IM, intramuscular; IV, intravenous; NSAID, nonsteroidal anti-inflammatory drugs; PNB, peripheral nerve block; RCT, randomised controlled trial; SC, subcutaneous; VAS, visual analogue scale.
Risk of Bias Within Studies
We assessed the risk of bias in each study using Version 2 of the Cochrane tool for assessing the risk of bias in RCTs (Figure 2 and 3). One study
36
had a high risk of performance bias. Five studies31–33,35,38 did not clearly describe the blinding processes for participants and personnel, and we considered these studies to have an unclear risk of bias. Four studies31,32,35,37 had unclear descriptions of allocation concealment, three studies32,33,35 had unclear descriptions of blinding of outcome assessment, and two studies32,35 did not provide a clear description of random sequence generation. These studies were deemed to have an unclear risk of bias. All studies reported satisfactory outcome data and were considered to have a low risk of attrition. Proportions of studies with categories for risk of bias. Summary for the risk of bias in each study.

Synthesis of Results
To obtain sufficient data points for a meta-analysis, only the following measurements were included: PND, PONV, and the analgesic effects at the 4 hours, 12 hours, 24 hours, and 48 hours after surgery. Funnel plots were not used to detect publication bias because only eight studies were included in this systematic review.
Primary Outcome
Compared to analgesics, PNB did not significantly affect the incidence of PND in older patients with hip fractures (RR = .67; 95% CI = .42 to 1.08; P = .10; I2 = 64%) (Figure 4). The sensitivity analyses revealed stable results (Table 2). Exclusion of the study
34
that reported data on the incidence of cognitive decline and two studies35,37 in which local anesthetics were administered continuously during two phases of the perioperative period did not alter the results. Heterogeneity of the above results was evident from the I2 values (>50%). Forest plot of the incidence of perioperative neurocognitive disorders. Sensitivity Analysis for PND Outcome. PND, perioperative neurocognitive disorders.

Subgroup Analysis of PND Outcome.

PND, perioperative neurocognitive disorders; FICB, fascia iliaca compartment block; FB, femoral nerve block.
Secondary Outcomes
Comparison of Analgesic Effect at Various Time Intervals Between the PNB and Control Groups.
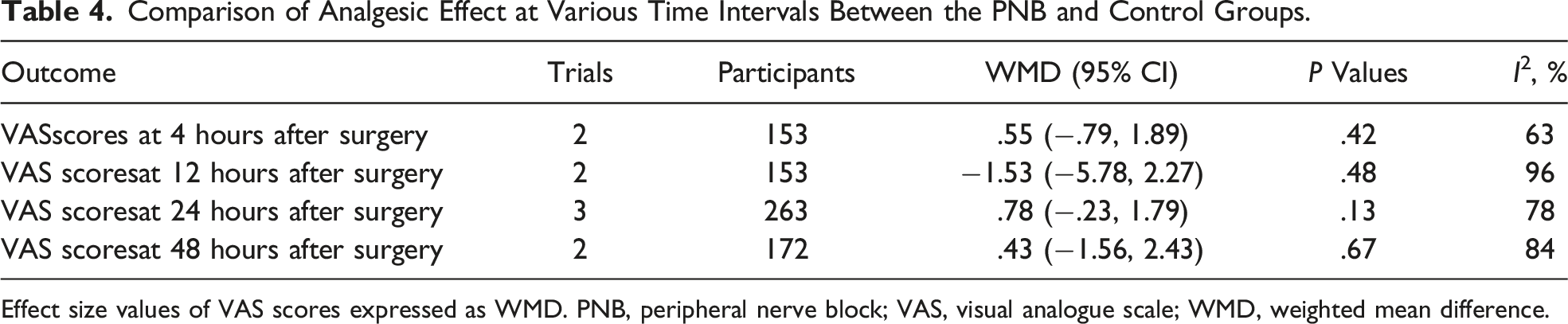
Effect size values of VAS scores expressed as WMD. PNB, peripheral nerve block; VAS, visual analogue scale; WMD, weighted mean difference.

Forest plot of the incidence of postoperative nausea and vomiting.
Discussion
Our study showed that PNB reduced PND in elderly patients with hip fractures and intact cognition. However, there was no significant difference between PNB and analgesics with regards to reducing the incidence of PND in the elderly population with hip fractures. The incidences of PONV and pain reduction did not differ significantly between the PNB groups and analgesics groups.
This systematic review differs from a recent systematic review 16 in that it included RCTs involving patients with pre-existing dementia or cognitive impairment. The populations of studies which exclude patients with pre-existing dementia or cognitive impairment might not reflect routine clinical practice. An increase in the proportion of elderly patients with hip fractures will also result in an increase in the proportion of patients with hip fractures with pre-existing dementia or cognitive impairment. In this review, three studies included patients with intact cognition and those with pre-existing dementia or cognitive impairment. Subgroup analyses of these three studies, which included 515 patients, showed that PNB did not reduce the incidence of PND. Compared to patients with intact cognition, when these patients have hip fractures, there is a high probability that their analgesic treatment will be inadequate. 39 A previous study showed that only 24% of the patients with dementia or cognitive impairment received appropriate pain treatment. 40 One reason is the presence of difficulties in communication with such patients who are unable to express the need for pain relief accurately and promptly. 41 Another reason is when using analgesics, medical personnel have difficulty assessing the level of pain in those with dementia or cognitive impairment. 40 Accordingly, improved methods are required to objectively assess pain levels in these patients. In addition, more high-quality studies related to pre-existing dementia or cognitive impairment are required.
Our results showed that PNB reduced the incidence of PND in the elderly patients with hip fractures and intact cognition. This was consistent with the results of other studies involving such patients. 16 PNB influenced PND, which was associated with reduced pain on movement, reduced opioid consumption and early mobilization.42–44 However, in this review, we did not find any analgesic advantage of PNB over analgesics. This was probably because of the variable time intervals for reporting VAS scores and the clinical heterogeneity between studies. Only the data of 2-3 studies were included in the meta-analysis, and the samples sizes were not sufficient enough to allow definitive conclusions on the analgesic effect of PNB.
The association of injection methods of local anesthetic with their analgesic effect is controversial. This review showed that continuous infusion of local anesthetic reduced the incidence of PND in elderly patients as compared with the single injection. A possible explanation for the decline in the incidence of PND may be that continuous infusion of local anesthetic offers increased pain control, decreased opioid consumption, and reduced PONV.45,46 Concerns regarding continuous infusion were primarily related to complications. However, in the studies included in this review, only one study 37 observed local hematomas associated with nerve block. Three local hematomas were reported in this study of 102 FICB procedures, resulting in an incidence of 2.9%, which was similar to the 1.7% reported in a previous review. 12
The most optimal PNB modality for hip fractures is undetermined. 47 In terms of anatomy, hip innervation includes the lateral cutaneous nerve of the thigh, femoral nerve, and obturator nerve. The fascia iliaca compartment is the space under the fascia iliaca, where the femoral, obturator, and lateral cutaneous nerves are located, with the injection site being far from the nerves or blood vessels. Although FB is recognized as an effective method, 48 FICB has a wider range of blockade than FB alone and provides a better analgesic effect.29,43 In particular, FICB can simultaneously block the lateral cutaneous nerve of the thigh and femoral nerves more effectively. 49 Additionally, there are different types of hip fractures. Surgical treatment involves either internal fixation of the fracture or total or partial replacement of the joint with arthroplasty. A study 15 showed that FICB had an advanced analgesic effect in patients with femoral neck fractures, but no obvious analgesic effect in patients with intertrochanteric fractures. This result suggests that fracture location might affect the efficacy of FICB or FB. Further homogeneous studies are required to confirm this conclusion.
In addition, the administration of ropivacaine does not show the same advantage as bupivacaine in reducing the incidence of PND in elderly patients with hip fractures. Ropivacaine produces a less potent motor blockade but an equally effective sensory block to dose-equivalent bupivacaine. 50 In this review, the concentration of bupivacaine reported in three studies were .25%, and that of ropivacaine reported in four studies were .125%–.25%. As the efficacy of a local anesthetic was closely related to its concentration, 51 the differences in drug concentrations might explain the negative results in the ropivacaine group.
Further, PONV is a known side effect of opioids. In three studies that reported PONV data, only one control group used morphine, whereas the other groups used non-opioid analgesics. The incidences of PONV were low in the PNB and control groups, with no significant differences between the groups.
This meta-analysis has some limitations. First, only eight trials met the inclusion criteria, and only two included more than 100 patients. Many trials had an unclear risk of bias; therefore, the possibility of bias in this systematic review cannot be ignored. Second, there was a risk of publication bias because of the limited number of trials. Third, there existed heterogeneity within some subgroups, and the lack of standardization of PNB treatment protocols limited our findings. Analgesic efficacy and PONV outcomes were also characterized by a high degree of heterogeneity. This could be attributable to the small number of included studies, lack of a standardized time interval for the assessment of analgesic effects, and paucity of complication data, which limited the interpretation and applicability of the results. These limitations should be addressed by larger, higher-quality RCTs.
Conclusion
The result of this systematic review and meta-analysis demonstrated that PNB was advantageous in reducing PND in older patients with hip fractures and intact cognition. FICB, bupivacaine, and continuous infusion of local anesthetic were beneficial for reducing PND in elderly patients with hip fractures and intact cognition or pre-existing dementia or impairment.
In both groups of patients, there were no differences between PNB and analgesics in terms of reducing PND, pain, and PONV. In addition, there were insufficient evidence to draw conclusions regarding the efficacy of FB, ropivacaine, and the single injection of local anesthetic in reducing PND.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
PROSPERO Registration Number
CRD42022310852