
Abstract
Background
In cementless hip arthroplasty, the femoral component should obtain firm fixation within the endosteal bone and achieve adequate reconstruction of hip joint biomechanics simultaneously. Previous anatomical studies described age-related changes of the proximal femoral canal, such as canal widening, which theoretically necessitates the use of larger stem sizes in elderly patients. This study examines a potential association between patients’ age at surgery and the implant size of a cementless femoral component.
Material and methods
A total of 13,423 primary hip arthroplasties with a single cementless stem registered in the Dutch Arthroplasty Register (LROI) were included. Patient characteristics (ie patients’ age, sex, height and weight at time of surgery) and femoral component size were derived. A one-way ANCOVA was used to compare the mean stem size between age groups, and multivariable linear regression analysis was used in order to investigate to which extent ageing impacted stem size.
Results
Each subsequent age- group (ten-year intervals) had a significantly larger mean stem size than the prior age- group. Multivariable linear regression analysis revealed that age is positively correlated with stem size and that this correlation is more prominent in females than in males (beta = .046, P < .001 and beta = .028, P < .001 respectively).
Interpretation
Implant size is positively correlated with age, in particular in females and independently from investigated anthropometric characteristics. The present study endorses that the femoral canal morphology is related to patients’ characteristics such as age and sex. The morphology will subsequently influence implant sizing and therefore may have biomechanical and clinical implications.
Introduction
Implant fixation in hip arthroplasty can be achieved with or without the use of bone cement. Over the last few decades, cementless femoral component fixation has gained popularity at the expense of cemented fixation,1-4 but is associated with a higher incidence of implant-related complications such as periprosthetic fractures, loosening and subsidence in elderly patients.1,2,5-8 The higher incidence of periprosthetic fractures in elderly patients treated with cementless stems is multi-factorial, but may partly be explained by anatomical changes in the proximal femur during the ageing process.
Anatomical studies have revealed several age-related changes such as progressive thinning of cortical bone, femoral canal widening and a transformation of a ‘champagne-flute’ appearance to a more ‘stovepipe’ shaped canal9-14 (Figure 1). These changes were found to be most prominent in females. Thinner cortices make the proximal femur more fragile and thus prone to (periprosthetic) fractures, while the morphology of the proximal femoral canal influences the stability of fixation and the reconstruction of hip joint biomechanics in cementless stem fixation.15,16 Therefore, age-related widening and shape changes of the femoral canal may result in an increased mismatch between implant and femur morphology. Schematic overview of the variations in proximal femoral canal morphology that are associated with subject’s age.9-14 A Thick cortices and a narrow shaft combined lead to a ‘champagne flute’ shaped canal. This appearance is associated with young age and is described with a high canal flare index
11
or as a Dorr type A femur.
14
B Cortical bone thickness and the meta-diaphyseal flare are generally decreasing during the ageing process (lower canal flare index
11
or a Dorr type B femur
14
), C Thin cortices and a widened shaft result in a ‘stovepipe’ like appearance. This morphology is associated with elder age and described with a low canal flare index
11
or as a Dorr type C femur.
14
(Reprint from Boymans,
40
with author’s permission).
In daily clinical practice, implantation of a cementless stem in a widened femoral canal might necessitate the use of a larger sized implant in order to achieve adequate primary fixation. Clinically, changes in femoral canal morphology and stem sizing might impact: (i) the implant stiffness, which is higher when using a larger sized stem and associated with increased stress shielding-related complications,17-19 (ii) the reconstruction of hip joint biomechanics 16 and (iii) the clinical success.15,20,21 Knowledge on age-related femoral canal changes currently consists of anatomical investigations performed on radiographs, computerized tomography scans, and three-dimensional models.9-14 However, whether and to what extent age-related changes in femoral canal morphology are related to the sizing of cementless femoral components in the clinical situation is currently unknown.
Therefore, this study aims to investigate the association between patients’ age at surgery and the implant size of a single frequently implanted cementless femoral component. We hypothesize that older age is accompanied with larger sized implants, independently from other anthropometric characteristics (ie patients’ height and weight), and that this correlation is more pronounced in females.
Materials and Methods
The data for the present study were derived from the Dutch Arthroplasty Register (LROI). The LROI is a nationwide population-based registry that has been collecting information on joint arthroplasties in the Netherlands since 2007. 22 The LROI was started by the Dutch Orthopaedic Association (NOV) and covers 100% of the centers performing arthroplasty surgery in the Netherlands. 22 A completeness of 98% of all procedures is described for hip arthroplasty. 22
A single femoral component design was studied because this ensures comparability between sizes and excludes the influence of differences between implant designs. All primary hemi- and total hip arthroplasties between 2007 and 2017 with the cementless Corail stem (DePuy Ltd, Leeds, United Kingdom) (Figure 2) were included in this study. This stem was chosen because it is among the most frequently implanted cementless stems in Europe.4,23,24 Photograph of the cementless fully coated Corail stem (DePuy Ltd, Leeds, United Kingdom). (Image derived from CORAIL Hip System Design Rationale brochure by DePuy Synthes.)
The implant is a fully hydroxy-apatite (HA) coated stem of titanium alloy with a wedge taper, a trapezoid cross section proximally and a quadrangular cross section distally. The cementless stem is available in 12 sizes (6 to 20) and three different offset options per size. The ‘standard offset’ and ‘high offset’ stems have a caput-collum-diaphyseal (CCD) angle of 135°, while the ‘coxa vara’ stem has a CCD-angle of 125°. The coxa vara stem is collared, the high offset stem is collarless, and the standard stem is available with and without collar. All primary hemi- and total hip arthroplasties with this cementless stem were included regardless of stem type (offset and CCD-angle), acetabular component, bearing surface, or the indication for the procedure; since these parameters will not considerably influence canal morphology or implant size. In revision surgery on the other hand, canal morphology and stem size may be manipulated and therefore revisions with the stem of interest were not part of this study.
Data of interest for the present study consisted of: (i) patient characteristics (ie patients’ age, sex, height and weight at time of surgery) and (ii) the size of the femoral component. In order to study the effect of age on stem size in subjects with mature proximal femur bone morphology, patients aged <18 years were excluded from all analyses. If one of the patient characteristics of interest or the implant size was missing, the subject was excluded as well.
A one-way ANCOVA was used to determine statistically significant associations between age groups and stem size, controlling for patients’ characteristics. Categories were made based on patients’ age (ie ≤50, 51 to 60, 61 to 70, 71 to 80 and >80 years), sex (male/female), weight (ie ≤65, 66 to 75, 76 to 85, 86 to 95 and >95 kg) and height (ie ≤155, 156 to 160, 161 to 165, 166 to 170, 171 to 175, 176 to 180 and >180 cm). The Bonferroni’s post hoc test was subsequently used to assess the differences between particular means. Per category of age, sex, weight and height; the frequency of implantation of small, medium and large stem sizes (size 6 to 10, 11 to 14, and 15 to 20 respectively) were noted as well. A multivariable linear regression analysis was conducted in order to investigate to which extent each patient characteristic was associated with the implant size. Stem size was considered a continuous variable in our analyses. All statistical analyses were performed in SPSS v23 (IBM Statistics, Illinois) and a P-value <.05 was considered statistically significant.
Results
A total of 27,018 hip arthroplasties with the cementless stem of interest were registered between 2007 and 2017 in the LROI. After assessment of the database, a total of 13,423 patients (49.7%) were considered eligible for full quantitative analyses (Figure 3). Of the excluded cases, 99.4% were excluded because only the BMI value was available instead of separate values for the patient’s weight and height. At time of surgery, the mean age was 68.3 (SD: ± 9.8, range: 18 to 102) years, the mean weight was 79.7 (SD: ± 15.4, range: 33 to 188) kilograms, and the mean height 171.0. (SD: ± 9.1, range: 138 to 204) centimetres. The median implant was size 12 (range: 6 to 20). Flow chart of patient selection based on eligibility criteria.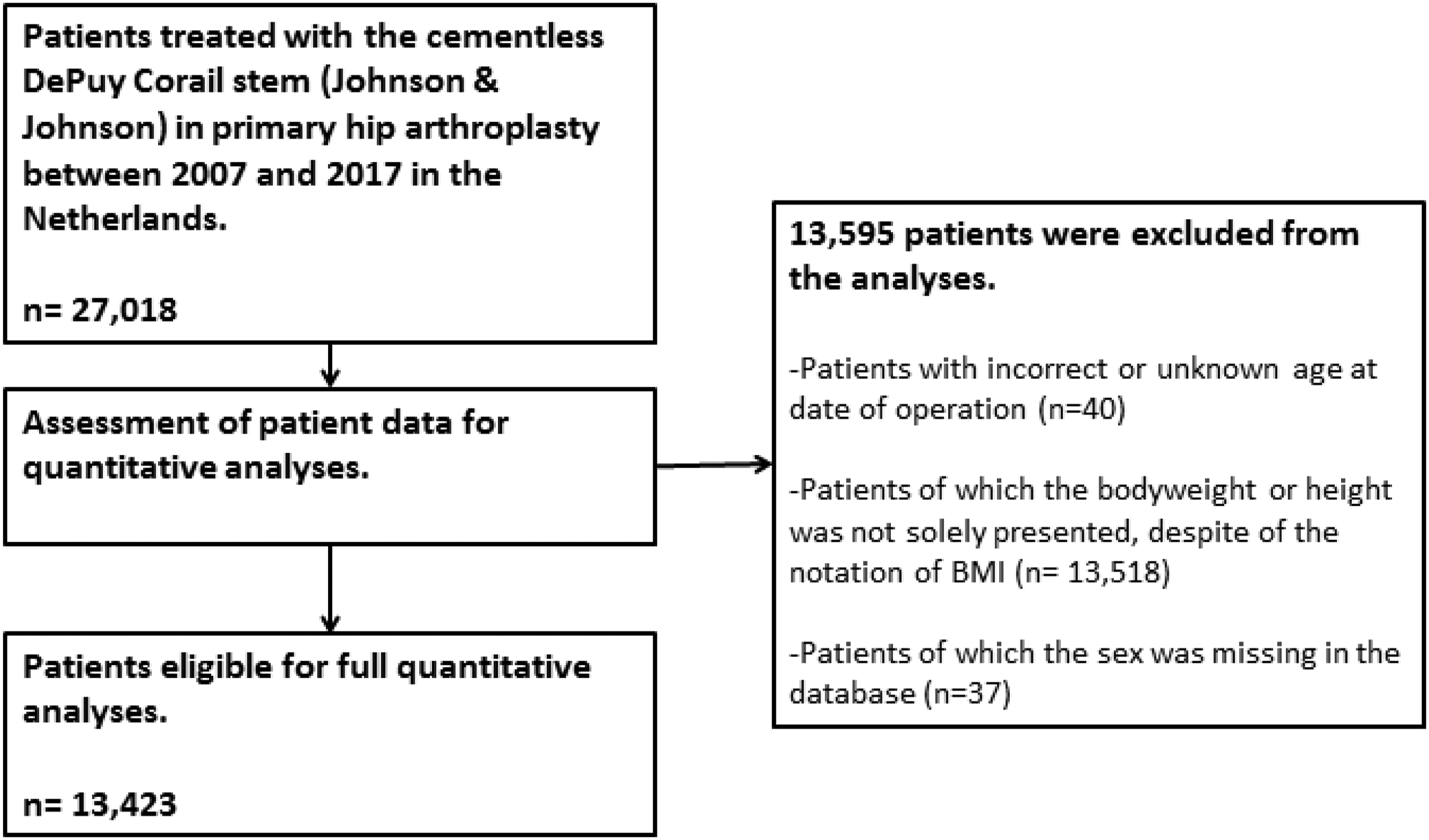
The mean size, standard deviation, range, and frequency of implantation (%) of small (ie 6 to 10), medium (ie 11 to 14), and large sizes (ie 15 to 20) per group of sex, age, weight, and height.

All percentages were rounded to whole numbers.
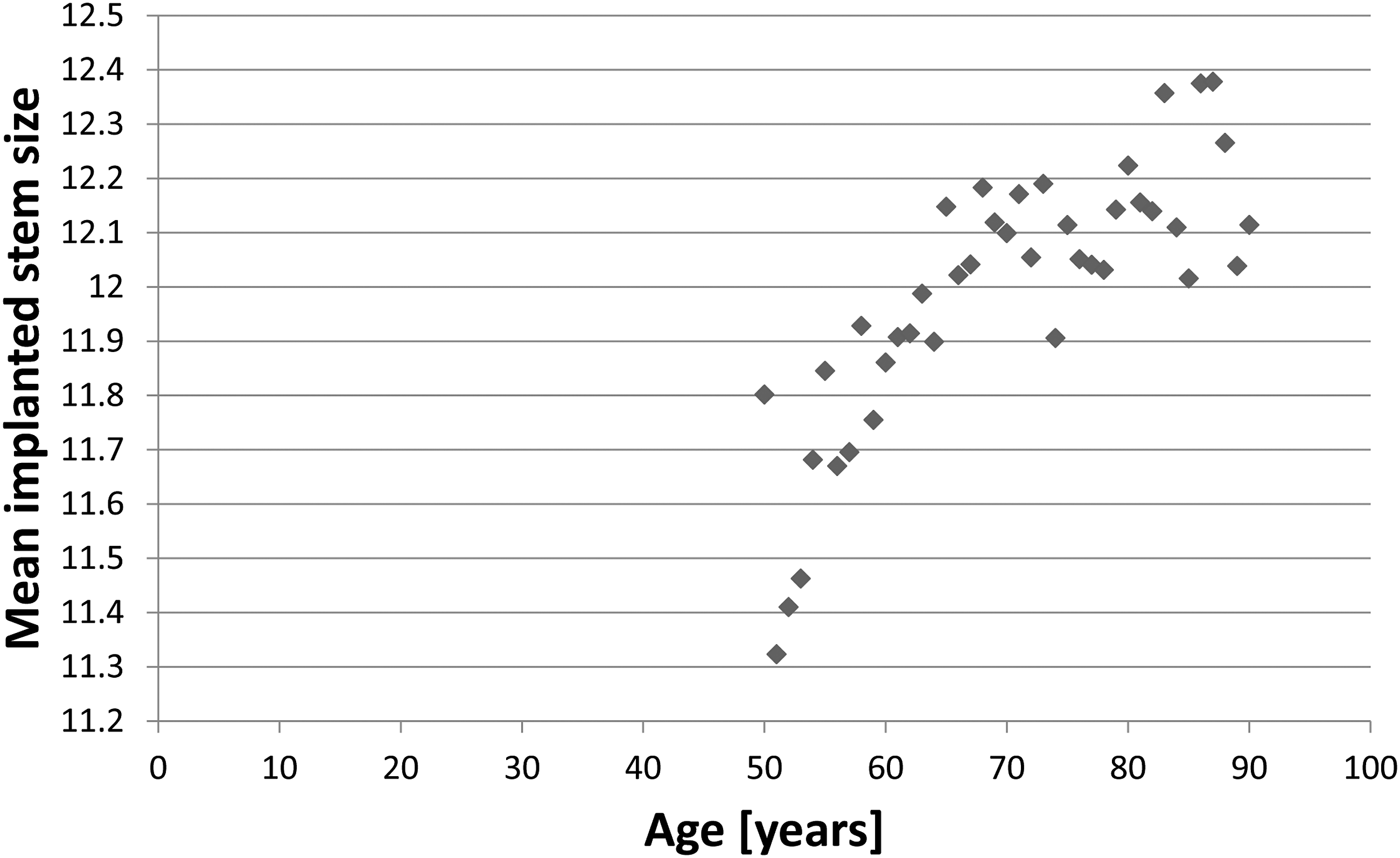
A positive association between age and mean implanted stem size was visually observed in the data (Figure 4). Accordingly, multivariable linear regression analysis revealed that age (beta =.046, P < .001), height (beta =.080, P < .001) and weight (beta =.003, P =.01) significantly predicted the implanted stem size in females. In males, only age (beta =.028, P < .001) and height (beta =.095, P < .001) were significant predictors of the implanted stem size, while weight was not (beta =.000, P =.880). Therefore, the following formulas could be reconstructed in order to predict the implanted stem size based on the anthropometric characteristics examined: A plot of the average stem size per age of patients aged 50 to 90 years, which represents 95.5% (12,813 cases) of the total cohort.

These findings imply that the positive association between patients’ age and implanted stem size is stronger in females. Based on the inverse beta of the predictor age alone, it was found that for a difference of one stem size, the average difference of age was 21.7 years in females and 35.7 years in males, in case height and weight were equal.
Discussion
In this study we demonstrated that patients’ age at surgery is positively correlated with the implanted stem size. The association between age and implanted stem size was statistically significant, independent from patient’s height and weight, and appeared to be more pronounced in females. The age-related widening of the proximal femoral canal is described to be more profound in females,9,12-14 which is in accordance with our finding of a stronger association between size and patient’s age in females.
The association between age and femoral component size is of clinical importance in cementless hip arthroplasty when considering (i) implant stiffness, (ii) the reconstruction of the femoral head center (FHC), and (iii) the implant design of the cementless femoral component. Regarding implant stiffness, a larger sized implant is accompanied with higher implant stiffness, which in turn, is correlated with higher levels of stress shielding.18,19 The main risks of this size-related stress-shielding are thigh pain, implant loosening, and periprosthetic fractures, particularly in the often fragile femora of (very) elderly patients.15,18,19,25 It should be noted that based on our findings, the more vulnerable elderly femora with wider canals and thinner cortices receive the larger sized and therefore stiffer implants. In order to achieve adequate fixation in the femoral canal, cementless stems are generally broader than cemented stems because of the absence of a cement mantle. Therefore, the age-related femoral canal widening and the subsequent larger stem in the eldest age groups may be an extra argument for cemented fixation in this age group. Because of the smaller diameter of the cemented stems and the Young’s modulus of cement, stress shielding will be reduced with cemented stems, especially in the fragile elderly patient with a widened femoral shaft.
Implant sizing directly affects the reconstruction of the femoral head center (FHC). Accurate FHC reconstruction is a keystone in hip arthroplasty since the FHC location will determine leg length and mediolateral offset. Our findings show that age-related changes in femoral canal morphology lead to the implantation of a larger sized femoral implant. Application of our formula on two hypothetical female cases reveals that on average, a 94-year old female would be treated with a Corail stem 2 sizes larger compared to a 50-year old female, if weight and height would be comparable. Simultaneously, for external morphology, it has been described that the femoral neck and head shift in a relative varus position during the ageing process.10,26,27 Since no clear proportional relationship between the size and shape of young and old femora exists,9,12,27-29 difficulties might occur in achieving adequate fixation and correct reconstruction of hip joint biomechanics with one cementless implant design.30,31 Boese et al. studied the ability of the Corail stem to reconstruct the FHC and found that reconstruction was poor in cases with a combination of low mediolateral offset and height, in coxa vara and in coxa valga. 32 Careful and accurate preoperative templating should be used in order to optimize the preservation of hip biomechanics after cementless hip arthroplasty and could help to identify potentially complex cases for any specific implant system.33,34
The implant design of the femoral component should be compatible with the native proximal femur morphology of an individual patient so that fixation occurs in association with optimal reconstruction of the FHC. During ageing, the meta-diaphyseal taper of the proximal femoral canal decreases. In other words, young subjects generally have a so-called ‘champagne flute’ shaped femur (referred to as a high canal flare index 11 or a Dorr A type femur), 14 and the shape generally shifts towards a more ‘stovepipe’ appearance during the ageing process (decreasing canal flare index 11 or towards a Dorr type C femur). 14 In cementless hip arthroplasty, a decreased meta-diaphyseal taper has been associated with a higher incidence of periprosthetic fractures.15,35 On the other hand, Brumat et al. showed that an increased taper is associated with excessive leg lengthening in cementless metaphyseal fixating stems. 16 Interestingly, no effect of canal morphology on postoperative leg lengthening was shown in cementless diaphyseal fixating or cemented stems. 16
Previous studies related the size of the Corail stem to the risk of revision.20,21 Jameson et al. analysed 35,386 primary THAs with the cementless Corail stem recorded in the National Joint Registry for England and Wales. 20 They found a significantly increased risk of revision of small stem sizes (8 to 10) compared to midsized stems (11 to 13), while larger stems had comparable revision rates as midsized stems. 20 Accordingly, Hoskins et al. analysed 41,265 primary THAs with the cementless Corail stem recorded by the Australian Joint Replacement Registry, and found that the smaller sizes (8 and 9) had significantly more revisions compared to larger sizes (10 to 20). 21 Hoskins et al. provided two potential explanations for the high incidence of implant failure in the small sizes of the cementless Corail stem 21 : (i) the small sizes are simply undersized and incorrectly implanted in varus, resulting in aseptic loosening, or (ii) these cases have a too narrow femur at isthmus level, resulting in distal fixation of the implant instead of metaphyseal loading. For patients with this kind of femoral canal morphology it was suggested to perform distal reaming or to consider another stem design. These findings emphasize the importance of considering both canal morphology and stem design when choosing the optimal (cementless) implant for an individual patient. Overall it seems to be very difficult to design a stem that matches the different morphology changes of the femur.
Major strengths of our analyses are the large population-based study population of 13,423 subjects with complete records and the focus on a single cementless stem that is currently among the most popular stems in several national joint registries.4,23,24 To our knowledge only one previously published study has investigated the association between anthropometrical characteristics and implant size of a cementless femoral component in total hip arthroplasty. 36 De Clerico et al. assessed the impact of patients’ sex, age, weight and height on the stem size of the AncaFit stem (Wright Medical Technology, Arlington, TN, USA) in 2329 subjects from the Emilia-Romagna region (Italy) with the use of the Register of Orthopaedic Prosthetic Implants (RIPO). Comparable to our findings, they found that sex, age and height, but not weight, were associated with stem size of the AncaFit stem. 36 However, a shortcoming of this study was data missing in their included cases. In their analyses, for 9.7% of all subjects height was missing, and for 7.1% weight, which led to an unbalanced model. Finally, although the authors stated that the AncaFit stem was the most commonly used stem in the RIPO database, this implant is not among the popular cementless stems in other arthroplasty registries.4,23,24
The present study is not without limitations. Firstly, due to the observational nature of this database, some selection bias regarding age might have occurred. A total of 1285 (10%) subjects were aged >80 years in our population. It is extensively described that cementless fixation in very elderly subjects could lead to more implant-related complications compared to cemented fixation and is therefore not recommended in this age group.1,2,7,8,37 As a consequence, a substantial part of the elderly patients will be treated with a cemented stem in daily practice. Therefore, there is a high probability that especially elderly patients with an obvious wide femoral canal and thin cortices did not receive the studied cementless stem. While on the other hand, elderly subjects with a femur morphology comparable to younger subjects (ie narrow shaft and thick cortices) may still have received a cementless component. This selection may have led to an underestimation of the effect of patients’ age on implanted stem size in our results.
Secondly, procedural factors such as the surgical approach and the used broaching technique may have influenced implant positioning and sizing.38,39 Our analyses were performed on a large quantity of subjects, who were treated in centres across the country and thus operated by a substantial number of surgeons. This potentially leads to a fair amount of variety in the techniques used. To which extent these factors influenced the selected implant size and our results is hard to estimate. However, we assume that this effect was equalized over both sexes and all height, weight and age groups; and therefore did not influence our conclusions.
Thirdly, in order to ensure comparability between sizes, a single cementless stem design was chosen. The findings of this study are therefore not generalizable to all cementless stem designs. The way ageing relates to the implanted stem size for different stem designs might be a topic for future research since the location of primary fixation within the proximal femur canal differs between stem designs.16,31
Finally, some data were missing in the database (Figure 3). Especially patients’ height and weight were frequently not included and substituted for a BMI value. Since we aimed for input completeness, the database entries which only provided a BMI value instead of also reporting patients’ height and weight prevented us from including a substantial part of the total population (13,518 subjects) in our analyses. This limitation is caused by the policy on filling in the inclusion forms and did not influence the conclusions of our analyses. In case multivariable linear regression analysis was performed on all 27,018 patients, comparable results were found.
Conclusion
The present study is the largest study that investigates the association between anthropometric characteristics and implanted stem size of a single cementless stem in hip arthroplasty. Based on the analysis of 13,423 procedures, we conclude that age-related anatomical changes in femoral canal morphology are represented by the implanted stem size of this frequently used cementless femoral component. Implant size was positively correlated with age, in particular in females and independently from height and weight. In the selection of the optimal cementless femoral implant for a specific patient, the sizing, design, and Young’s modulus should be compatible with the patient’s femur as much as possible. The present study emphasizes that the femur morphology is related to patient’s characteristics such as sex and age, which will subsequently influence implant sizing.
Footnotes
Author Contributions
HV: study idea, study design, data analyses, interpretation and reflection, writing the manuscript TB: study design, data analyses, interpretation and reflection, reviewing the manuscriptLS: data collection, data interpretation and reflection, reviewing the manuscriptIH: study design, data analyses, interpretation and reflection, reviewing the manuscript
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.