
Abstract
Background
Patellofemoral arthroplasty (PFA) is a surgical option for patients older than 40 years old who are affected by patellofemoral osteoarthritis. Regarding the complications of PFAs, few studies have investigated periprosthetic fractures. The purpose of this literature review was to highlight a previously overlooked complication of primary prosthetic surgery of the patellofemoral joint.
Methods
Three literature databases were searched for studies published between 2000 to 2020 using relevant keywords. A total of 4,942 articles were originally identified. After excluding duplicates and analysing the titles and abstracts, 20 studies were considered. From these, data regarding the number of cases, clinical outcomes and complications were extracted.
Results
Among the 20 selected articles, only one described periprosthetic fractures as a complication of PFAs. Herein, we also report an illustrative case of an unknown fracture complication. No cases in the literature were found that described the type of complications experienced by our patient during the postoperative period.
Conclusions
This review confirms the lack of data about clinical outcomes and fracture complications of PFAs. In primary prosthetic surgery of the patellofemoral joint, patient selection and close consideration of demographic factors (such as BMI and age) and intraoperative factors (such as patellar thickness and size of the trochlear component) play a key role in optimising pre-operative planning to avoid intraoperative periprosthetic fractures.
Keywords
Introduction
Patellofemoral arthroplasty (PFA) is a type of partial knee replacement that is especially used to treat severe isolated patellofemoral osteoarthritis (PFOA). According to Iwano classification, PFOA can be divided into stages based on the severity of osteoarthritic changes. Stage III and IV represent the ideal phases in which a PFA can be implanted.1,2
Idiopathic PFOA represents 49% of all PFA cases, while the remaining PFAs are carried out because of patellar instability, chondrocalcinosis, fractures or dislocations. Trochlear dysplasia also plays a key role in the pathogenetic process. 2
Therapeutic options used for isolated PFOA, include nonoperative (intra-articular injections, physiotherapy and taping) and operative treatments. The available operative treatments are: the arthroscopic debridement of articular cartilage, the chondroplasty with the use of osteochondral allografts, the resection-arthroplasty, the lateral facetectomy, the extensor mechanism alignment and lateral release and the prosthetic surgery. 3
In prosthetic surgery, especially in primary surgery of the patellofemoral joint, patients are chosen according to recruitment criteria. PFA is reserved for patients with severe and painful PFOA in which conservative treatment has failed. For patients to be eligible for PFA, the function of the joint and the extensor apparatus must be preserved without any sign of tibio-femoral osteoarthritis or injuries to the capsular ligaments and meniscus. 4
This implant replaces the joint surface of the patella and femoral trochlea but maintains the physiologic tibiofemoral joint.
The introduction of biomaterials and design innovations has allowed the evolution of PFAs, from generations I to III. Starting with the vitallium prosthesis, introduced by McKeever in 1955, new prosthesis have been developed using metal alloys, such as chromium-cobalt, titanium and oxininium, combined with polyethylene.5,6
Three generations of prosthesis design have been described in the literature. In generation I, the femoral trochlea is resurfaced without changing its native anatomy; in generation II, the femoral surface is cut as in total knee arthroplasty (TKA); generation III is similar to II, but a larger portion of the anatomy is maintained, with a lower risk of patellar impingement.7,8
According to literature, the first and the second generation implants showed a higher reoperation, complication and revision rate compared to TKA. 9
The introduction of the third-generation PFA and the improvement in surgical techniques and patient selection has led to better clinical outcomes.
Although third-generation implants have shown encouraging results in terms of functional outcomes, compared with TKA, a higher risk of early postoperative complications and a higher rate of surgical revision has been described.9-11
This review of the current literature aimed to investigate the rarity of periprosthetic fractures as complications of PFA. To support the literature, we also report a significant case of a 63-year-old woman who underwent bilateral PFA and experienced different complications in each limb: patellar and femur fracture on the left side and a supracondylar fracture of the femur on the right side. This is the first description of a new complication characterised by simultaneous fractures of the patella and the distal femur in each limb.
Materials and Methods
Because of the rarity of the case reported herein, this article begins with a review of the literature focusing on periprosthetic fracture after primary prosthetic surgery of the patellofemoral joint.
The preferred reporting items for systematic reviews and metanalyses (PRISMA) guidelines were followed. 12
Literature and Database Searches
Two researchers (C.B. and G.V.) independently searched three databases – PubMed, the Cochrane Library, and Google Scholar – for the keywords “patellofemoral arthroplasty”, “clinical outcomes” and “periprosthetic fracture”. A third researcher (G.M.) independently verified the number of articles identified to avoid potential discrepancies.
Literature Selection
The inclusion criteria were: • Human studies that considered different postoperative complications, particularly those related to periprosthetic fractures in PFA; • Studies written in English.
The Exclusion Criteria Were: • Articles published before 2000 or after the end of 2020; • Cadaveric and biomechanical studies; • Studies that did not report complications.
Data Extraction
Several articles were excluded after reviewing the titles and abstracts. From the remaining articles, data regarding possible complications of primary prosthetic surgery of the patellofemoral (PF) joint were extracted.
The following data were extracted (when reported): authors and year of publication, type of study and level of evidence, number of patients enrolled and timing of complications, number of prostheses implanted, mean patient age, type of complication and percentage of observations.
In addition, an illustrative case study of a woman with a bilateral PFA who suffered from post-surgery fractures in each limb is reported herein.
Results
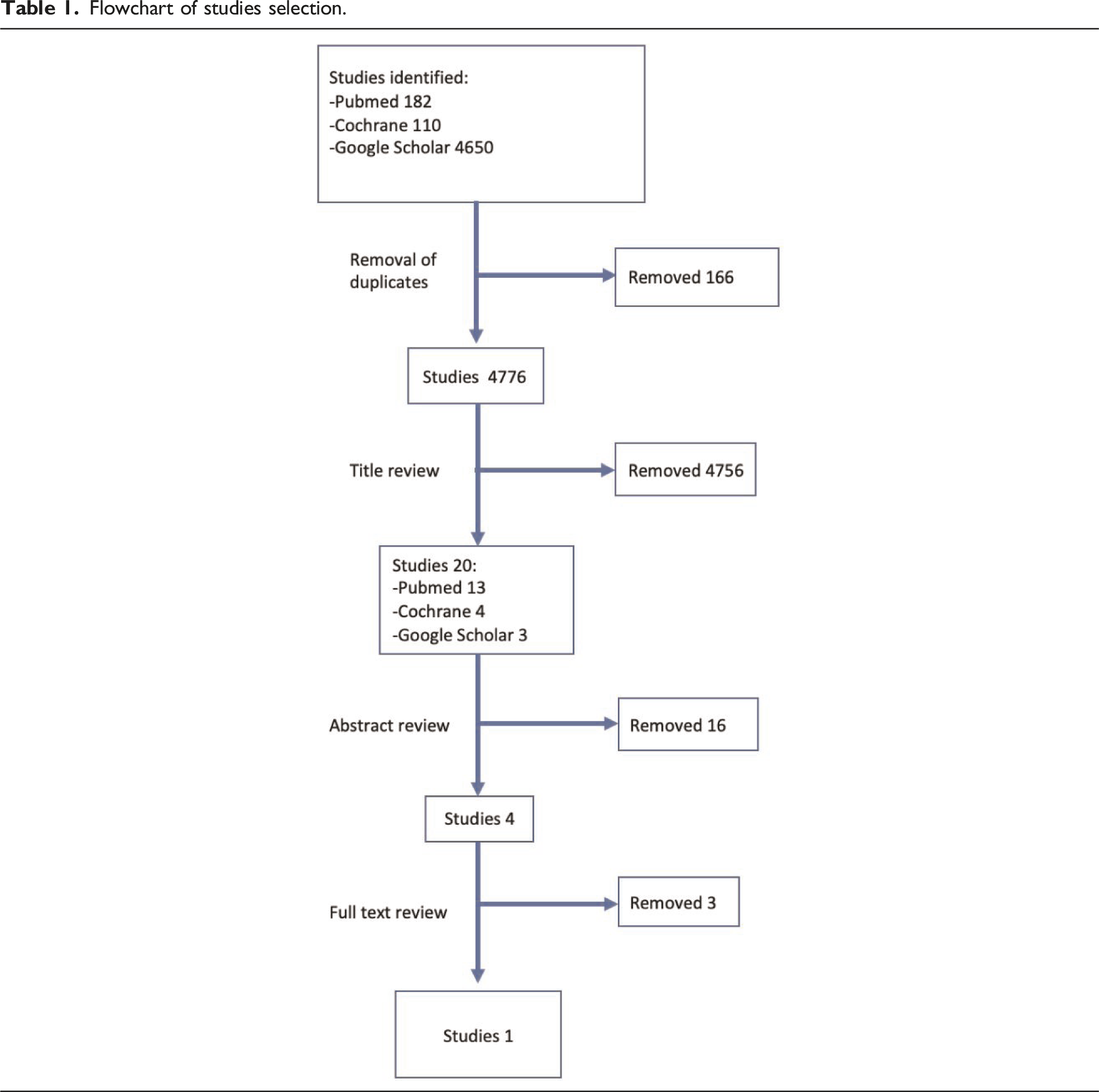
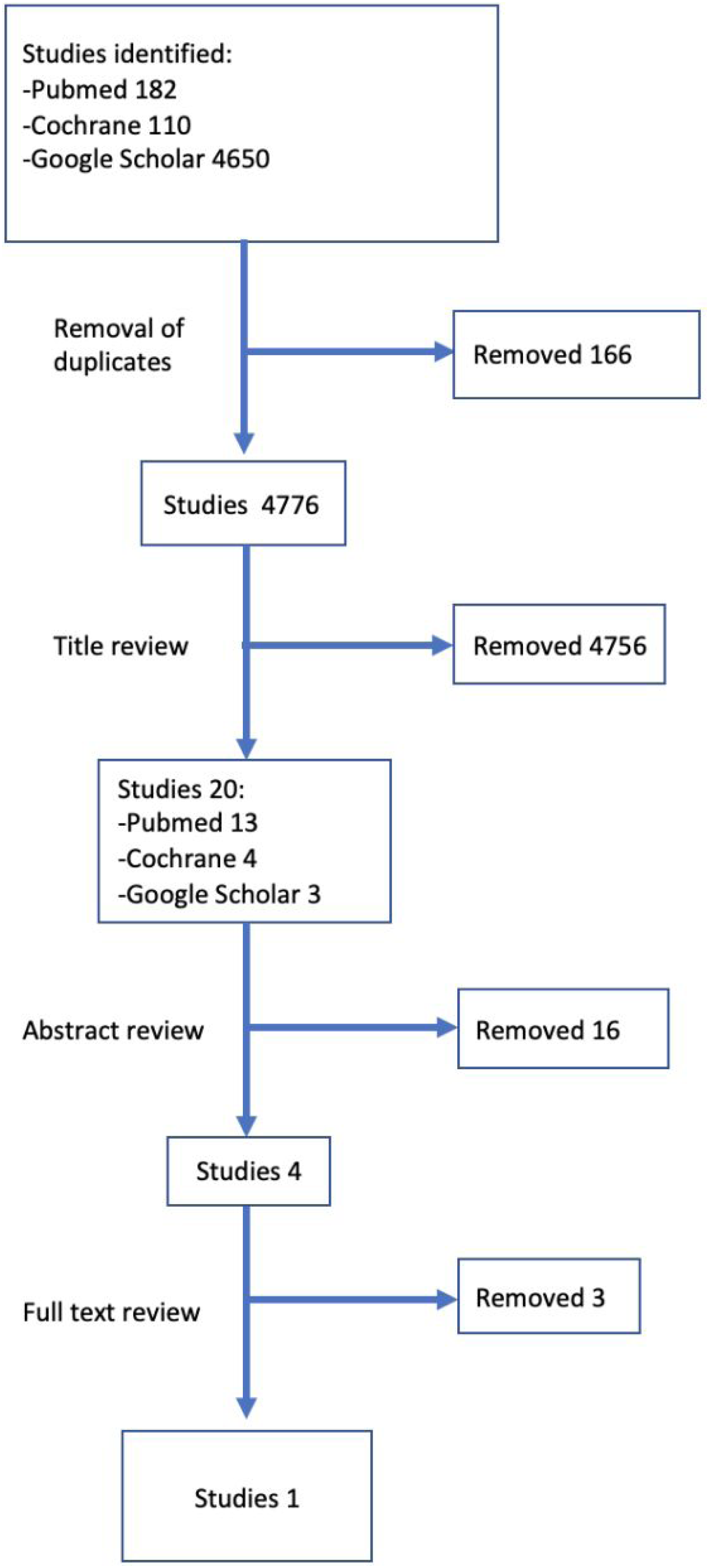
A total of 4,942 articles were identified in the following databases: PubMed (182), Cochrane (110) and Google Scholar (4,650).
These articles had been published before 2000 or after the end of 2020, a time period in which the use and the role of PFA has been more questioned.
Flowchart of studies selection.
PFA post-operative complications of the 20 articles selected. AbbreviationsOA, osteoarthritis.

Articles screened and assessed for eligibility.

Three of these articles (the studies by Ahearn et al., Williams et al. and Leadbetter et al., published in 2016, 2013 and 2008, respectively) were removed after a detailed analysis of the complications reported.
The study by Ahearn et al. 21 was discarded because the breakage of only the femoral component (without a periprosthetic fracture) was observed after a low-energy trauma.
The article by Williams et al. 17 was removed for a similar reason. In that study, the patellar fracture resulted from a fall and not from the surgical procedure.
Finally, injury of the patellar tendon after a fall in the postoperative period was described in Leadbetter et al. 24 ; thus, this study was also removed from further consideration.
Therefore, the only remaining study examined in detail was King et al. 14
This was a retrospective study that described the clinical outcomes and complications (including fractures) of 77 primary PFAs (AVON Patello-Femoral Joint Replacement System, Stryker, Mahwah, New Jersey) implanted in 59 patients.
Illustrative Case
A clinical case of a 65 years old woman is shown. After clinical evaluation for anterior knee pain the patient was operated for bilateral PFAs (AVON Patello-Femoral Joint Replacement System, Stryker, Mahwah, New Jersey) (Figures 1, 2 and 3). X-rays before surgery. Post-operative right knee X-ray where it is possible to verify the supracondylar fracture already. Post-operative left knee X-rays.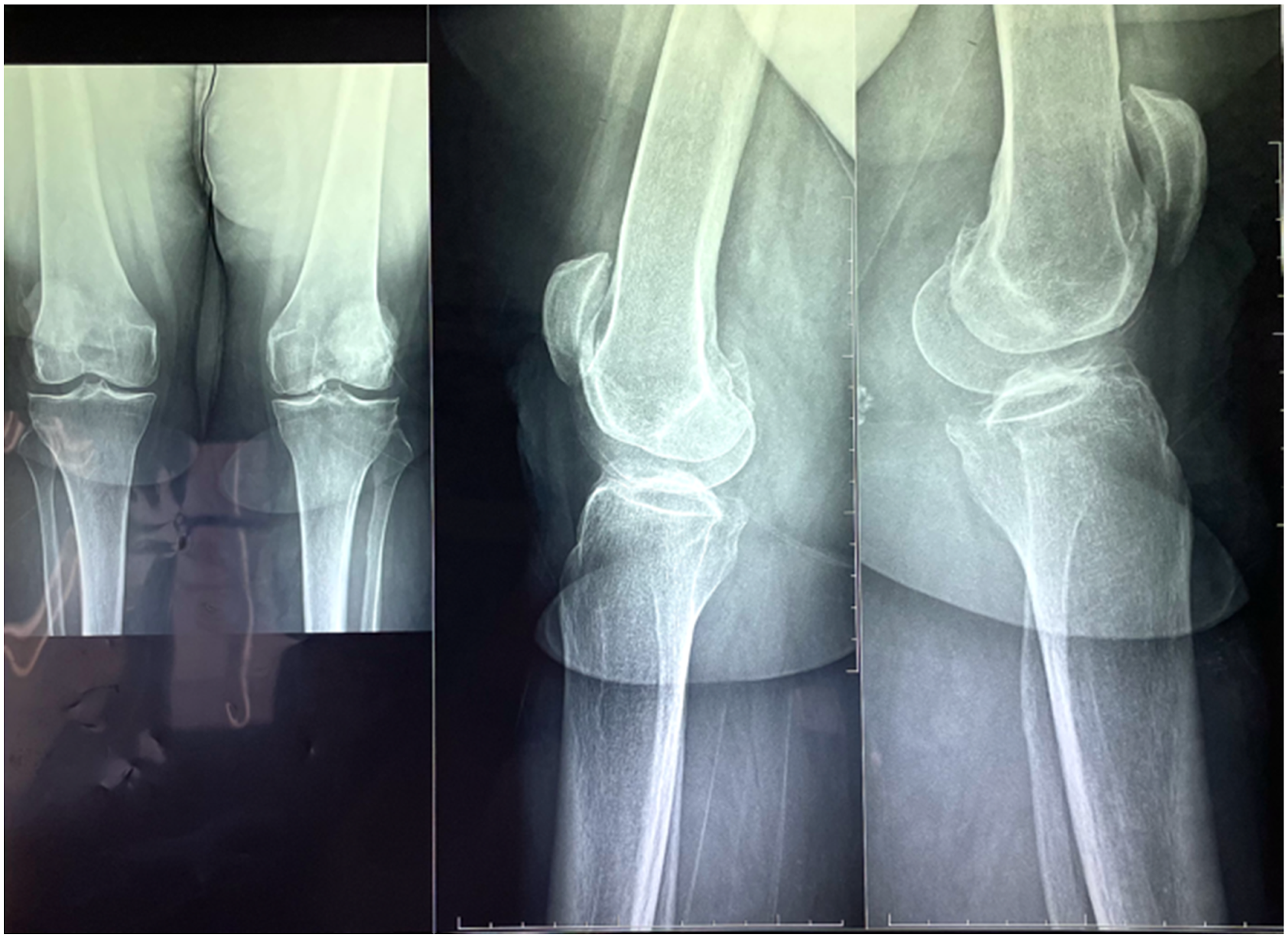


On the first postoperative day, the patient suddenly experienced worsening pain and functional impotence during passive immobilization of each lower limb. The patient was discharged on the third postoperative day with indication to rehabilitation and gradual partial weight bearing. Two weeks later, for the worsening of the clinical symptoms the patient ask for a second opinion in our Hospital and the X-rays of both knee showing a bilateral periprosthetic fracture (Figure 4). Right knee and Left knee X-rays before surgery.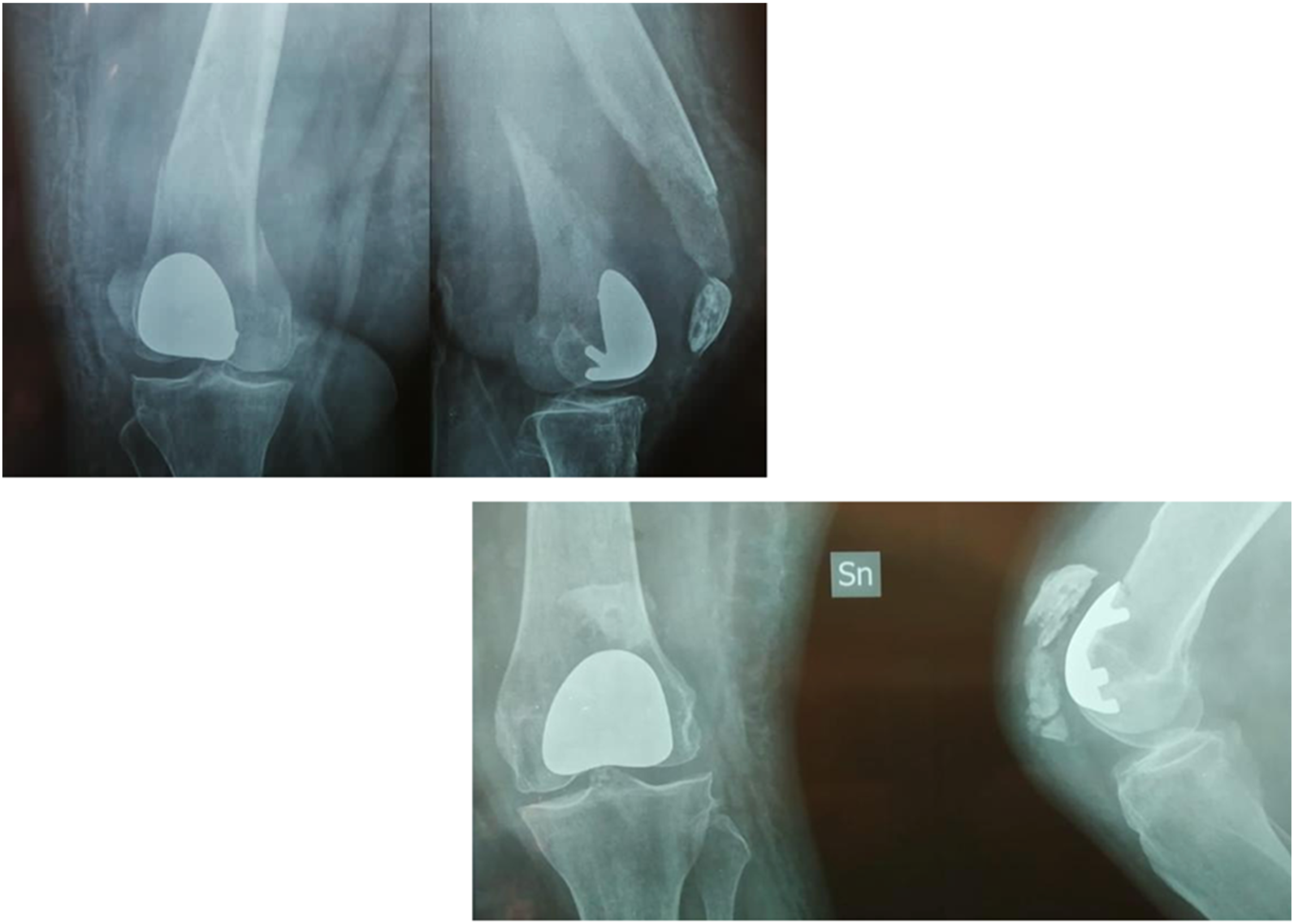
The supracondylar fracture of the right knee is a specific complication described in the literature as a consequence of the femoral notching in TKA. Harish et al 28 divided the femoral cut into four grades according to its depth. For this patient, the cut was classified as a grade III/IV according to Gujarathi.
In the left knee, the X-ray analysis led to a diagnosis of both a patellar fracture (a complication described as a consequence of PFA/TKA 29 ) and an infraction of the anterior cortical of the left femur.
The supracondylar fracture of the right side was treated with open reduction and internal fixation with lag screws and a neutralization dedicated locked plate (Figure 5). Intra-operative photos and post-operative right knee X-rays.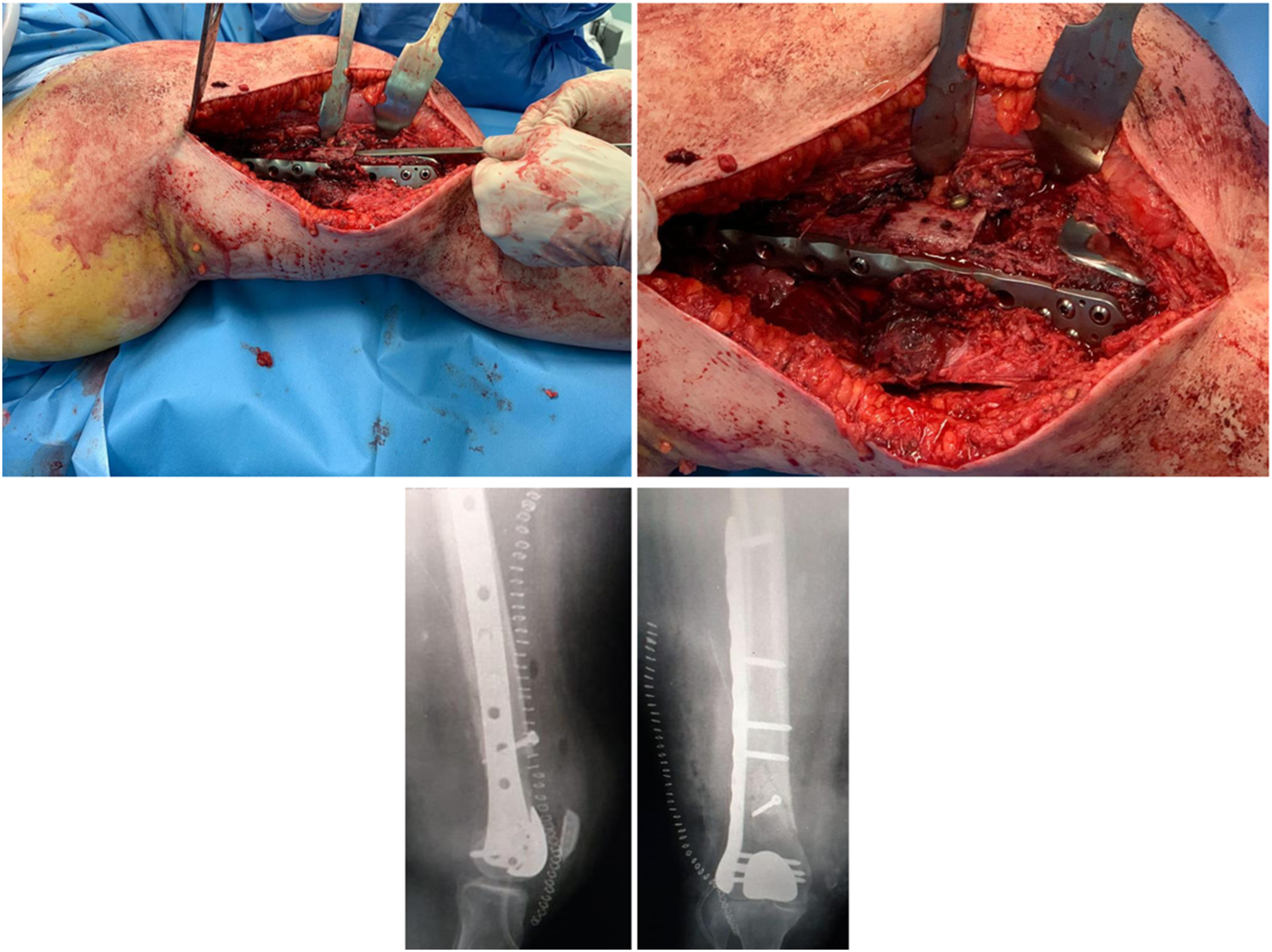
Unlike supracondylar fractures in TKAs, 30 the design of PFAs does not allow for retrograde nail osteosynthesis.
Two weeks after the first surgical procedure, an osteosynthesis of the patellar fracture on the left side with two cerclages, in accordance with Weber, and a suture of the medial and lateral retinaculum of the knee with Cracow’s technique to prevent patellar maltracking during the postoperative period
31
(Figure 6). Intra-operative left knee photo.
Weight bearing as tolerated was allowed from day one post op and the patient started an aggressive rehabilitation program for the recovery of the full range of motion of both knees.
The radiographic and clinical follow up after 3 months showed complete recovery of the patient (Figure 7). Post-operative right and left knee X-rays.
Discussion
The evolution from the first PTA, introduced by McKeever in 1955, 32 to third-generation anatomic prosthetic implants has led to improved clinical and functional outcomes. However, the survival rate of implants over the medium to long term in patients who undergo revision surgery has been disappointing. 33
Postoperative complications such as pain, patellar maltracking, and injuries of the quadriceps and patellar tendon are the primary cause of revision surgery within 30 days after the first surgical procedure. 34
Moreover, bleeding is also responsible for a high percentage of revision surgeries (11.7%) within 30 days. 13
Owing to the lack of cases described in the literature, here we have focused on the periprosthetic fractures as a postoperative complication after primary prosthetic surgery of the PF joint.
In this review, the article by King et al. was the only study to account for patellar fracture after PFA surgery. King et al. 14 reported a rate of patellar fractures of 9.1% (referring to the number of patients recruited). This incidence is higher than that observed for TKA surgery, which is thought to range from 0.5% and 3.6%.35,36
Demographic and intraoperative factors might affect the onset of patellar periprosthetic fractures. King et al. accounted for BMI and age as demographic factors. In addition, they considered the thickness of the patellar prosthesis, the thickness of the residual patella, the size of bone resection of the trochlear component, and the lateral release of the retinaculum as intraoperative factors.
Studies have been published that treated only demographic factors as risk factors for periprosthetic fractures. Among them are the recent study by Rezzadeh et al 13 in which the authors concluded that some types of complications are related to age. The study by King et al 14 found a relationship between patellar fracture, age and BMI. There have also been studies on the differences between men and women in patellofemoral osteoarthritis and operative management. Male sex has been associated with a high incidence of DVT (which has been well documented) and longer operation time. By contrast, female sex is related to a higher risk for bleeding requiring transfusion.13,37
King et al. 14 the only study selected in the current review, confirms that demographic factors can be risk factors if they associated with intraoperative factors.
Regarding intraoperative factors, King et al. 14 report that the thickness of the residual patella, patellar resection, and the residual thickness compared to the pre-operative patellar dimensions are factors that may lead to a higher risk of periprosthetic fracture. In fact, as previously reported regarding TKA surgery, a reduced post-operative patellar thickness (compared with the pre-operative thickness) results in a higher risk of periprosthetic fracture due to greater patellar fragility.38-41
Similarly, a large femoral component compared to the shape of the trochlea may result in a higher risk of periprosthetic fracture.
Unlike other studies, King. et al. 14 emphasised that there is no statistically significant correlation between patellar tendon release and the incidence of periprosthetic fracture.36,42,43
There is a general lack of studies about periprosthetic fractures of the femur after a PFA. From the experience of the illustrative case reported in this review and in line with the considerations regarding TKA, we can relate periprosthetic fractures of the femur to notching of the anterior femoral cortex and to osteoporosis.
Studies have demonstrated that a femoral notch creates a weakened area of the anterior femoral cortex, favouring the production of a fracture. 28 However, the link between femoral notching during surgery and periprosthetic fracture is controversial. 44 No studies demonstrate that femoral notch is the cause of femoral periprosthetic fracture in PFA.
The incidence of supracondylar fracture following a total knee replacement (TKR) in the early postoperative period in a notched femur varies from 0.5 to 52%. 45
Lesh et al., 2000 46 studied the effect of femoral notching of the distal anterior cortex and found a reduction of bending strength and torsional strength that could lead to a risk of periprosthetic fracture. Other factors that contribute to the pathogenesis of supracondylar fracture after a TKR are the difference in elastic modulus between the femoral cortex and the metal components, stress shielding, and postoperative hypo-vascularity. In fact, these factors can cause inadequate osseous remodelling.
One strength of this review is that the PRISMA methodology was applied to search keywords in various databases.
A weakness is the limited number of selected studies (only 20) after reviewing titles and abstracts, and only one was considered for its full text.
Another limitation is the small number of patients enrolled, and the level of evidence of the selected articles is low. However, this aspect is owing to the low rate of observations of periprosthetic fractures in primary prosthetic surgery of the PF joint.
Conclusion
The presence of a supracondylar fracture is not well described in the literature as a complication of PFA, but it has been described as a consequence of a femoral cut in TKA.
Similarly, patellar fracture as an intraoperative complication has been reported by only one study (King et al (2015) 14 ).
The lack of data about fracture complications of PFAs was confirmed after analyzing the selected studies.
In the primary prosthetic surgery of PFA, the correct surgery indication, careful patient selection, and the close analysis of demographic and intraoperative factors are crucial. We also emphasize the importance of intraoperative factors (i.e. patellar thickness, the size of bone resection, and the size of the trochlear component) in optimal preoperative planning to avoid intraoperative fracture complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.